Embed Size (px)
Citation preview

Multidisciplinary treatment approach in severe Molar Incisor Hypomineralization: - A Case Report
The term Molar Incisor Hypomineralization (MIH) was introduced first in 2001, defined as development enamel disorder characterized by hypomineralization of systemic origin of first permanent molars, often associated with permanent incisors.1 MIH, also referred to as "hypo mineralized” PFMs2, "idiopathic enamel hypomineralization, "3,4 “demineralized” PFMs,5
"nonfluoride hypomineralization, "6,7and "cheese molars, "8.9 the disturbed function of ameloblast cells causes all these conditions during the transitional and maturational stages of amelogenesis. 3,10
Clinically, the hypomineralization can be seen as an abnormality in the translucency of enamel (opacity), which can be of different colors depending upon the severity of MIH and often undergo post-eruptive enamel breakdown due to soft and porous enamel.11 The etiology is multifactorial, which includes neonatal problems, sickness during early childhood, or medically compromised children.12,13,14,15,16,17,18 The treatment approach of MIH consists of early diagnosis, caries risk management, remineralization therapy for prevention of decay and caries, restorations.19,20 Depending upon the occasion, molar restoration could be composite restoration, metal inlays, and crowns, whereas anterior teeth are restored using veneers or esthetic fillings.20
This case report presents the multidisciplinary approach to a patient with MIH on borderline skeletal class III malocclusion to achieve satisfactory esthetics and prevent further trauma to upper teeth.
Case report
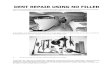
A 16-year-old male reported with a chief complaint of irregularly placed lower front teeth and the inability to utilize the front teeth to bite correctly with no relevant associated medical history. There was a history of root canal treatment in 11 & 21. Clinical frontal examination revealed a comparatively symmetrical face with mesomorphic facial form, no incisal display at rest. (Fig 1) Clinical profile examination revealed a straight profile with anterior facial divergence, normally positioned chin, acute nasolabial angle, retrognathic maxilla, orthognathic mandible with retrusive lower lips, low mandibular plane angle (Fig 1). Intra-oral examination revealed good oral health with apparently symmetrical arches, multiple rotations. The inter-arch relationship showed a reverse overjet of 0.5mm and overbite of 9 mm each. Class I molar and canine relationship existed in maximum intercuspation on both sides. The mandibular midline was shifted to left by 1.5 mm. There was severe attrition in anterior maxillary teeth (Fig 1).
Functional examination revealed no tenderness of temporomandibular joint, the patient was an oronasal breather, with normal mastication and deglutition and mouth opening within a healthy range. Cephalometric examination revealed a Skeletal Class III skeletal pattern with the retrognathic maxilla and orthognathic mandible with horizontal growth pattern, maxillary incisors were proclined, and mandibular incisors were upright. Soft tissue profile showed an acute nasolabial angle, deep mentolabial sulcus, retruded lower lip (Fig 2). The Orthopantomogram revealed no temporomandibular irregularities/ pathology, unerupted third molars. The crown-root ratios were normal, with good alveolar bone levels (Fig 2).

Fig 1: Pretreatment photographs
Fig 2: Pretreatment x rays: Lateral Cephalogram and Orthopantomogram

PROBLEM LIST AND TREATMENT OBJECTIVES
Problem list Included Reverse smile arc, Skeletal Class III jaw bases, and supra erupted lower anterior teeth, attrition of upper incisors, anterior crossbite, overclosure of the mandible, the increased curve of Spee. Revised treatment objectives were set after the patient refused to underwent Orthognathic surgery. These included restoration of smile arc to consonant form, the intrusion of lower incisors to correct deep bite and to level curve of Spee
TREATMENT PROGRESS
The patient was explained about treatment limitations and started with fixed orthodontic braces in the lower arch first. Preadjusted Edgewise bracket system 022” X 028” was used. One lower incisor (31) was extracted due to tooth size arch length discrepancy. Remaining lower incisors were intruded with archwire (Fig 3, 4). After leveling and alignment of the lower arch, the Upper arch was started.
Figure 3 intraoral photographs with treatment progress
Figure 4: Mid-stage radiographs
After the intrusion of upper and lower incisors, upper incisors were prepared for crown placements, and temporary crowns were given according to Subharti Protocol 21. Treatment was further continued

and finished with temporary crowns over 11 and 21 (Fig 5, 6). At the end of treatment, we were able o achieve Consonant Smile Curve, satisfactory overjet, overbite and good interdigitations (Fig 7,8,9)
Figure 5 intraoral photographs with treatment progress
Figure 6: Mid-stage radiographs
Figure 7. Intraoral photographs showing treatment progress

Figure 8: Post-treatment extraoral photographs
Figure 9: Post-treatment intraoral photographs
Fig 10: Post-treatment x rays: Lateral Cephalogram and Orthopantomogram

Discussion: - Treatment approaches of MIH consists of early diagnosis; caries risk management, remineralization therapy for prevention of decay and caries, restorations 19,20. Teeth beyond restoration need extraction and space closure by orthodontic means. The case in our case report was very challenging due to the amount of severe attrition and reverse overjet and reverses deep bite along with skeletal Class III jaw discrepancy. An ideal treatment plan was a mandibular surgical setback, which was refused by the patient. The next option (Single mandibular incisor extraction) was a viable alternative, keeping in mind the severity of negative overjet and deep bite. We were able to intrude lower incisors below the occlusal plane and able to give positive overjet, which was the primary objective concerned to smile aesthetics of the patient. Later on, the upper incisor position was finalized by temporary crowns as a significant amount of tooth structure was lost due to attrition21. Temporary crowns acted as a guide for final vertical positioning and intended inclination of upper incisors. Upper incisors were monitored through the treatment as they were RCT Treated, and there could be increased root resorption increased in these teeth.
REFERENCES
1. Weerheijm KL, Jalevik B, Alalusua S. Molar-incisor hypomineralization. Caries Res 2001;35:390-391
2. Jalevik B, Noren JG. Enamel hypomineralization of permanent first molars: A morphological study and survey of possible aetiological factors. Int J Paediatr Dent 2000; 10:278-289.
3. Fearne J, Anderson P, Davis GR. 3D X-ray microscopic study of the extent of variations in enamel density in first permanent molars with idiopathic enamel hypomineralization. Br Dent J 2004; 196:634-638.
4. Koch G, Hallonsten AL, Ludvigsson N, Hansson BO, Holst A, Ullbro C. Epidemiologic study of idiopathic enamel hypomineralization in permanent teeth of Swedish children. Community Dent Oral Epidemiol 1987;15:279-285
5. Croll TP. Creating the appearance of white enamel demineralization with bonded resins. J Esthet Dent 1991; 3:30-33.
6. Holtta P, Kiviranta H, Leppaniemi A, Vartiainen T, Lukinmaa PL, Alaluusua S. Developmental dental defects in children who reside by a river polluted by dioxins and furans. Arch Environ Health, 2001; 56:522- 528.
7. Leppaniemi A, Lukinmaa PL, Alaluusua S. Nonfluoridehypomineralizations in the permanent first molars and their impact on the treatment need. Caries Res 2001; 35:36-40.
8. vanAmerongen WE, Kreulen CM. Cheese molars: A pilot study of the etiology of hypocalcifications in first permanent molars. J Dent Child 1995; 62:266-269.
9. Weerheijm KL, Groen HJ, Beentjes VE, Poorterman JH. Prevalence of cheese molars in 11-year-old Dutch children. J Dent Child 2001; 68:259-262.
10. Wright JT, Hall K, Yamauchi M. The protein composition of normal and developmentally defective enamel. Ciba Found Symp 1997;205:85-99, 106 (discussion)
11. Weerheijm KL. Molar Incisor Hypomineralisation (MIH). Eur J Paediatr Dent 2003; 4(3):114-20.
12. Beentjes VE, Weerheijm KL, Groen HJ. Factors involved in the aetiology of molar-incisor hypomineralisation (MIH). Eur J Paediatr Dent. 2002 Mar; 3(1):9-13.
13. Crombie F, Manton D, Kilpatrick N. Aetiology of molar-incisor hypomineralisation: a critical review. Int J Paediatr Dent. 2009 Mar;19(2):73-83

14. Hong L, Levy SM, Warren JJ, Dawson DV, Bergus GR, Wefel JS. Association of amoxicillin use during early childhood with developmental tooth enamel defects. Arch Pediatr Adolesc Med. 2005 Oct;159(10):943-948
15. Kabaktchieva R. Study on Dental dysplasia and alternatives for primary and secondary prevention, Ph.D. Thesis,1989, Sofia, 148 and supplement (in Bulgarian)
16. Laisi S, Ess A, Sahlberg C, Arvio P, Lukinmaa PL, Alaluusua S. Amoxicillin may cause molar incisor hypomineralisation. J Dent Res. 2009 Feb;88(2):132-136.
17. Lygidakis NA, Dimou G, Marinou D. Molar-Incisor-Hypomineralisation (MIH). A retrospective clinical study in Greek children. II. Possible medical aetiological factors. Eur Arch Paediatr Dent. 2008 Dec; 9(4):207-17
18. Whatling R, Fearne JM. Molar incisor hypomineralisation: a study of aetiological factors in a group of UK children. Int J Paediatr Dent. 2008 May;18(3):155-162.
19. Willmott NS, Bryan RA, Duggal MS. Molar-incisor-hypomineralisation: a literature review. Eur Arch Paediatr Dent. 2008 Dec; 9(4):172-9.
20. William V, Messer LB, Burrow MF. Molar incisor hypomineralization: review and recommendations for clinical management. Pediatr Dent 28(3):224-32.
21. Arora R, Raj S, Verma RK, Raghav P, Rohilla S. The Subharti protocol for interdisciplinary management of non-vital teeth. Int J Orthod Rehabil 2016;7:108-11