Embed Size (px)
Citation preview
1
January 2014
.
Improving Procurement Practices in Developing Country Health Programs
FINAL REPORT
Leslie Arney and Prashant Yadav, With significant inputs from
Roger Miller and Taylor Wilkerson
2
About WDI
The William Davidson Institute (WDI) is a non-‐profit research and educational institute at the University of Michigan that promotes actionable business and public policy approaches to address the challenges and opportunities within emerging market economies. More specifically, the WDI Healthcare Research Initiative produces independent, multi-‐disciplinary research and business knowledge to help increase access to essential medicines, vaccines and other health technologies in developing countries.
Recommended Citation
Arney L. & Yadav P. 2014. Improving Procurement Practices in Developing Country Health Programs.
Acknowledgements
Taylor Wilkerson LMI Roger Miller LMI Bonface Fundafunda Zambia Drug Supply Budget Line Joycelyn Azeez Head of Procurement Unit, Ghana MOH Rosalie Faniyo Deloitte Consulting LLP, Mozambique CMAM Damian Beil University of Michigan Ross School of Business Ravi Anupindi University of Michigan Ross School of Business

3
4
Table of Contents
1. ABBREVIATIONS & ACRONYMS.................................................Error! Bookmark not defined.
2. INTRODUCTION .................................................................................................................. 6
3. METHODOLOGY.................................................................................................................. 7
4. U.S. GOVERNMENT PUBLIC PROCUREMENT OF HEALTH COMMODITIES ............................. 7 4.1 Pricing Arrangements................................................................................................................. 8 4.2 Prime Vendor Program .............................................................................................................. 9 4.3 Provision for Flexible Contracting.....................................................Error! Bookmark not defined.
5. PUBLIC PROCUREMENT IN DEVELOPING COUNTRIES .........................................................10 5.1 Legislative Reform ................................................................................................................... 10 5.2 Country Procurement Assessment Reports (CPAR)...........................Error! Bookmark not defined. 5.3 Public Procurement of Health Commodities............................................................................. 10
5.3A Case Studies of Sub-‐Saharan Africa ...........................................................................................11 5.3B Key Observations .......................................................................................................................13
6. SYNTHESIS OF FINDINGS....................................................................................................14
7. FRAMEWORK AGREEMENTS ..............................................................................................14 7.1 Case Studies of Framework Agreements in Health Commodity Procurement ........................... 17
7.1A Chile...........................................................................................................................................17 7.1B Mexico .......................................................................................................................................17 7.1C United Nations System ..............................................................................................................17 7.1D Global Fund to Fight AIDS, Tuberculosis and Malaria ...............................................................18
7.2 Legislative Provision for Framework Agreements in Sub-‐Saharan Africa................................... 19 7.3 Current Use of Framework Agreements in Select Countries of Sub-‐Saharan Africa ................... 19 7.4 Barriers to Use of Framework Agreements............................................................................... 20
8. CONCLUSIONS ...................................................................................................................21
9. RECOMMENDATIONS ........................................................................................................22
REFERENCES ..........................................................................................................................23

5
6
2. INTRODUCTION Despite significant progress made by many countries toward meeting the Millennium Development Goals, there has been little improvement in access to essential medicines in developing countries (1). The mean availability of essential medicines is lowest in the World Health Organization (WHO) Africa Region, followed by the WHO South East Asia Region, the regions which account for all but two of the least-‐developed countries of the world (2,3). Although different national procurement models exist across developing countries, the provision of essential medicines to many of these populations relies heavily on public monies, international funding mechanisms and donor agencies (4). However, the mean availability of select medicines is consistently lower in the public sector than in the private sector across all WHO regions (2). The public entities largely responsible for the procurement of essential medicines often lack the technical capacity to efficiently and strategically carry out the procurement process; inadequate planning and forecasting and the use of archaic methods of procurement contribute to high drug costs and commodity insecurity (4). The need for maximum efficiency and increased value-‐for-‐money in the public procurement of health commodities cannot be overstated in these resource-‐limited environments. An important outcome of the Paris Declaration on Aid Effectiveness was a renewed focus on strengthening national procurement systems, including a commitment by donors to increase the use of country systems and procedures (5,6). Although the private sector is often used as a benchmark for efficiency, public sector procuring entities face unique challenges and constraints, such as heightened public scrutiny. There is a need for transparency and corruption prevention in the use of public monies, and many view the institutionalization of additional controls and checks and balances as limiting to the agility and responsiveness of procurement practices. Similarly, the procurement of health commodities is different from the procurement of non-‐health products; as the demand for medicines and health supplies reflect changes in population health and environmental conditions, there exists a great need for flexibility and responsiveness in procurement and contracting. We examine various public sector procurement systems of health commodities for alternative, more strategic practices that may be suitable for global health supply chains. We first look to procurement systems of select departments of the U.S. Federal Government which procure large volumes of pharmaceuticals. We then explore the public procurement systems of select developing countries of sub-‐Saharan Africa, and assess the use and challenges to use of such alternative practices within these settings. The aim of our study is to illustrate how transparency and flexibility in procurement may be achieved simultaneously to improve commodity security, even by national government/public procuring entities operating under strict public scrutiny.

7
3. METHODOLOGY We conducted semi-‐structured literature reviews of the procurement systems and methods used by the large public procurers of medicines and health products of the U.S. Federal Government, as well as of the public procurement systems of select countries of sub-‐Saharan Africa. Much of the relevant literature on these topics is not included in peer-‐reviewed journals, but is grey literature in the form of presentations, websites, reports, government-‐issued assessments and legislative documents. Discussions with experienced colleagues at LMI contributed greatly to our working knowledge of the procurement processes of the U.S. Federal Government. Additional country-‐specific information was gained through interview or correspondence with persons involved in public procurement in select countries of sub-‐Saharan Africa.
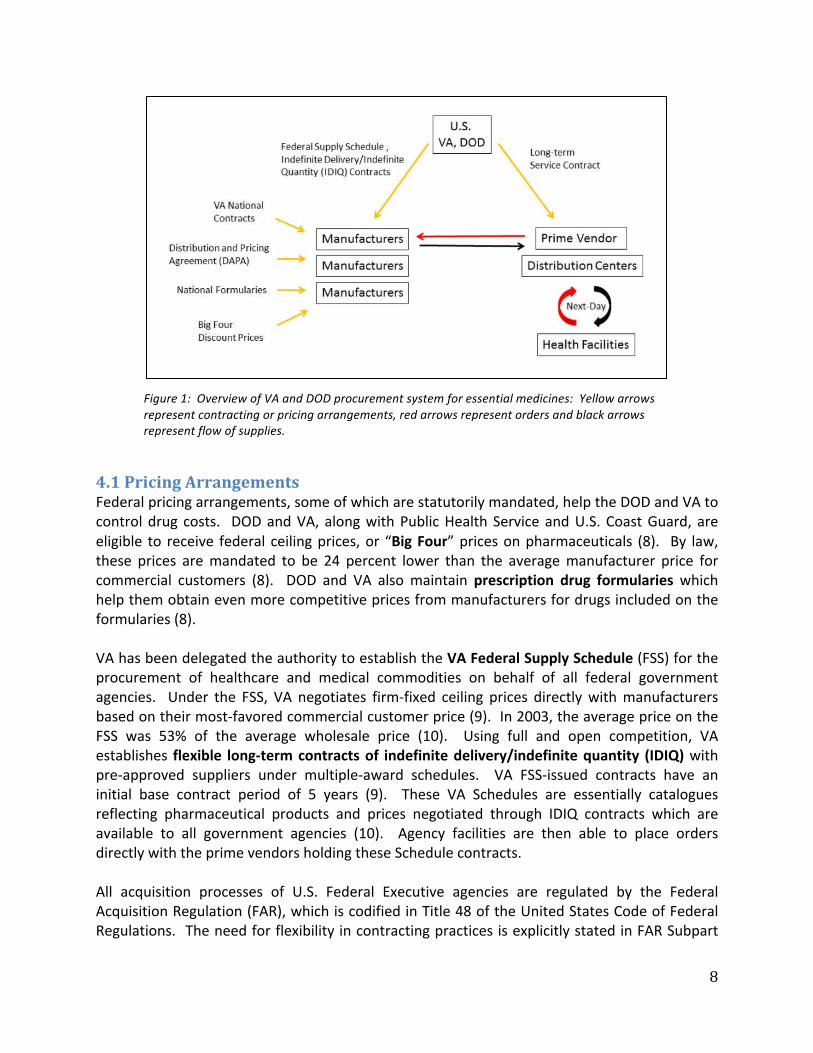
4. U.S. GOVERNMENT PUBLIC PROCUREMENT OF HEALTH COMMODITIES The U.S. health system is comprised of both public and private sector facilities and financing. Although most health care provision occurs through the private sector, the government plays a significant role in the provision of health care to the military, veterans and underserved populations, and manages the financing and reimbursement for health care for the elderly, poor, and persons living with certain disabilities through Medicare and Medicaid. The U.S. Federal government provides health coverage to veterans and the military through the Department of Veteran’s Affairs (VA) and the Department of Defense (DOD), both of which are heavily involved in the procurement of pharmaceuticals. In 2012, the VA provided prescription drug coverage to 8.8 million eligible veterans, with prescription drug spending totaling approximately $4.2 billion (7). During the same year, the DOD provided prescription drug coverage to 9.7 million active-‐duty and retired military personnel and their dependents, with spending totaling $7.6 billion (7). The provision of pharmaceuticals to a combined 18.5 million beneficiaries necessitates these departments to use strategic methods to control drug costs and ensure supply security (7). The VA and DOD procurement systems can be generally characterized by the use of centralized negotiation and contract management and decentralized procurement authority. The key components of the VA and DOD systems include various federal pricing arrangements, direct negotiation of flexible contracts with manufacturers and a direct purchase and distribution approach facilitated by prime vendor programs. A simplified diagram of the VA and DOD procurement systems for essential medicines is shown in Figure 1.
8
Figure 1: Overview of VA and DOD procurement system for essential medicines: Yellow arrows represent contracting or pricing arrangements, red arrows represent orders and black arrows represent flow of supplies.
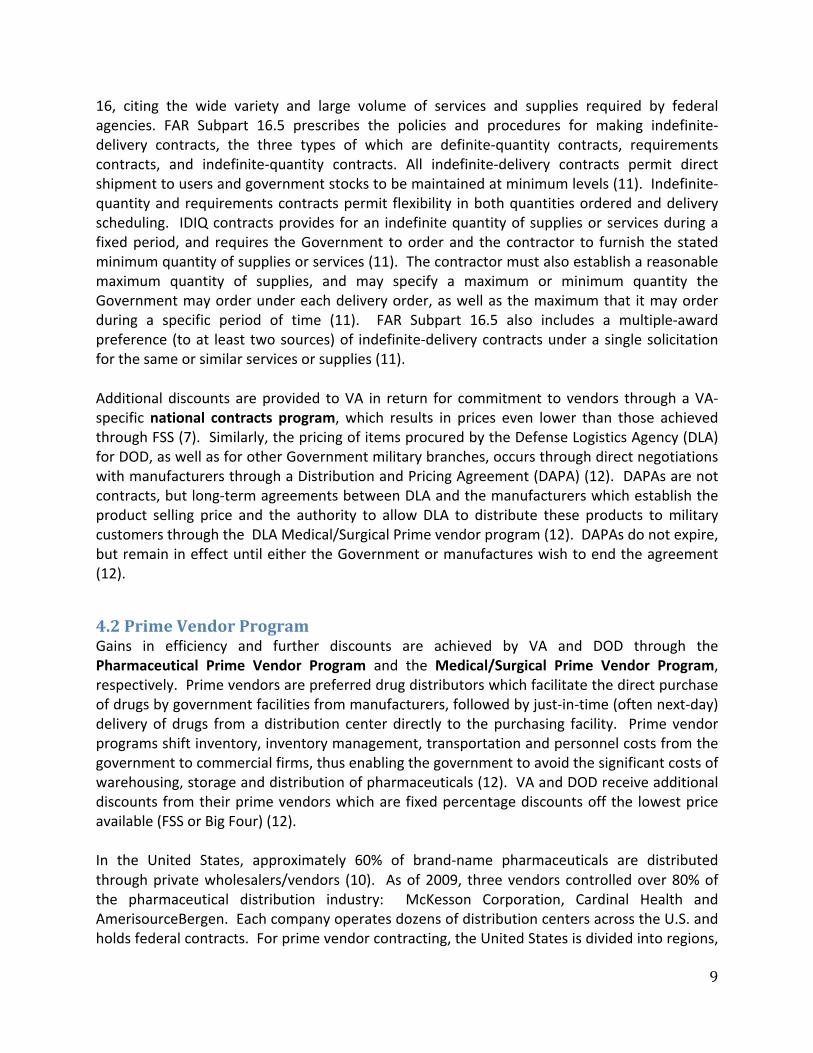
4.1 Pricing Arrangements Federal pricing arrangements, some of which are statutorily mandated, help the DOD and VA to control drug costs. DOD and VA, along with Public Health Service and U.S. Coast Guard, are eligible to receive federal ceiling prices, or “Big Four” prices on pharmaceuticals (8). By law, these prices are mandated to be 24 percent lower than the average manufacturer price for commercial customers (8). DOD and VA also maintain prescription drug formularies which help them obtain even more competitive prices from manufacturers for drugs included on the formularies (8). VA has been delegated the authority to establish the VA Federal Supply Schedule (FSS) for the procurement of healthcare and medical commodities on behalf of all federal government agencies. Under the FSS, VA negotiates firm-‐fixed ceiling prices directly with manufacturers based on their most-‐favored commercial customer price (9). In 2003, the average price on the FSS was 53% of the average wholesale price (10). Using full and open competition, VA establishes flexible long-‐term contracts of indefinite delivery/indefinite quantity (IDIQ) with pre-‐approved suppliers under multiple-‐award schedules. VA FSS-‐issued contracts have an initial base contract period of 5 years (9). These VA Schedules are essentially catalogues reflecting pharmaceutical products and prices negotiated through IDIQ contracts which are available to all government agencies (10). Agency facilities are then able to place orders directly with the prime vendors holding these Schedule contracts. All acquisition processes of U.S. Federal Executive agencies are regulated by the Federal Acquisition Regulation (FAR), which is codified in Title 48 of the United States Code of Federal Regulations. The need for flexibility in contracting practices is explicitly stated in FAR Subpart
9
16, citing the wide variety and large volume of services and supplies required by federal agencies. FAR Subpart 16.5 prescribes the policies and procedures for making indefinite-‐delivery contracts, the three types of which are definite-‐quantity contracts, requirements contracts, and indefinite-‐quantity contracts. All indefinite-‐delivery contracts permit direct shipment to users and government stocks to be maintained at minimum levels (11). Indefinite-‐quantity and requirements contracts permit flexibility in both quantities ordered and delivery scheduling. IDIQ contracts provides for an indefinite quantity of supplies or services during a fixed period, and requires the Government to order and the contractor to furnish the stated minimum quantity of supplies or services (11). The contractor must also establish a reasonable maximum quantity of supplies, and may specify a maximum or minimum quantity the Government may order under each delivery order, as well as the maximum that it may order during a specific period of time (11). FAR Subpart 16.5 also includes a multiple-‐award preference (to at least two sources) of indefinite-‐delivery contracts under a single solicitation for the same or similar services or supplies (11). Additional discounts are provided to VA in return for commitment to vendors through a VA-‐specific national contracts program, which results in prices even lower than those achieved through FSS (7). Similarly, the pricing of items procured by the Defense Logistics Agency (DLA) for DOD, as well as for other Government military branches, occurs through direct negotiations with manufacturers through a Distribution and Pricing Agreement (DAPA) (12). DAPAs are not contracts, but long-‐term agreements between DLA and the manufacturers which establish the product selling price and the authority to allow DLA to distribute these products to military customers through the DLA Medical/Surgical Prime vendor program (12). DAPAs do not expire, but remain in effect until either the Government or manufactures wish to end the agreement (12).
4.2 Prime Vendor Program Gains in efficiency and further discounts are achieved by VA and DOD through the Pharmaceutical Prime Vendor Program and the Medical/Surgical Prime Vendor Program, respectively. Prime vendors are preferred drug distributors which facilitate the direct purchase of drugs by government facilities from manufacturers, followed by just-‐in-‐time (often next-‐day) delivery of drugs from a distribution center directly to the purchasing facility. Prime vendor programs shift inventory, inventory management, transportation and personnel costs from the government to commercial firms, thus enabling the government to avoid the significant costs of warehousing, storage and distribution of pharmaceuticals (12). VA and DOD receive additional discounts from their prime vendors which are fixed percentage discounts off the lowest price available (FSS or Big Four) (12). In the United States, approximately 60% of brand-‐name pharmaceuticals are distributed through private wholesalers/vendors (10). As of 2009, three vendors controlled over 80% of the pharmaceutical distribution industry: McKesson Corporation, Cardinal Health and AmerisourceBergen. Each company operates dozens of distribution centers across the U.S. and holds federal contracts. For prime vendor contracting, the United States is divided into regions,

10
and contracts are awarded through a competitive process to the vendor, or combination of vendors, whose bid represents the best-‐value for the Government (10). It is important to recognize that these prime vendors are not involved in the agreements or price negotiations established between the Government and manufacturers. Although they may offer additional discounts, prime vendors are private wholesalers engaged in separate service contracts which facilitate the efficient ordering and delivery of the pharmaceutical products included under these government-‐wide contracts.
5. PUBLIC PROCUREMENT OF HEALTH COMMODITIES IN DEVELOPING COUNTRIES
5.1 Legislative Reform The procurement of essential medicines and health commodities in takes place within the larger framework of a national public procurement system. A general shift toward decentralization of public procurement has been observed in many developing countries, prompted by legislative reforms aimed to increase local involvement, accountability and availability of products and services (4). Although there is no “single appropriate model” of public procurement, there has been a trend toward harmonization of public procurement procedures both across and between countries in an effort to promote international trade (13). First issued in 1994, The United Nations Commission on International Trade Law Model Law on Procurement of Goods, Construction and Services (UNCITRAL Model Law), was designed to assist countries in the development of their public procurement systems and provide a framework for procurement regulation (13). The Model Law has been used as a template which national governments can flexibly use to reform or implement procurement legislation in accord with local circumstances and existing legislation (14). Generally, the Model Law promotes a procurement system based on a decentralized purchasing and decision-‐making mechanism and the establishment of a central regulatory or oversight authority (15). As of 2010, approximately 30 countries had enacted legislation based on the Model Law, including the following countries of sub-‐Saharan Africa: The Gambia, Ghana, Kenya, Malawi, Nigeria, Rwanda, Tanzania, Uganda and Zambia (14). The procurement legislations of these countries can therefore be considered generic versions of the Model Law, which share common guidelines and provisions but may differ slightly on specific issues, such as value thresholds for permissible procurement methods (15). This list may underestimate the influence of the UNCITRAL Model Law, as countries are not obligated to report their adoption or use of the Model Law to the UN (14). CPAR WEAKNESSES OBSERVED
5.3 Trends and Models of Public Procurement of Health Commodities Despite considerable diversity, trends have been observed across the public procurement systems of many developing countries. Over the past 10 years, many countries have seen the historical predominance of in-‐kind donations gradually replaced by direct budgetary support to governments (4). In other cases, donors have begun phasing out direct support to low-‐and

11
middle-‐income countries (LMIC) who have graduated from low-‐income status (4). As a result of these shifts in donor support, many countries have become increasingly responsible for the procurement of essential medicines and healthcare supplies, facing the challenges of limited experience, insufficient technical capacity and corruption (4). The procurement models commonly used by developing country governments in the procurement of health commodities include centralized procurement, the use of parastatal organizations or autonomous supply agencies, decentralized procurement and the use of procurement agents (4). Although these models can be clearly defined, in practice, their attributes may be combined and their use adapted to local circumstances. Among many other factors, funding streams, importer presence, donor regulations and national legislation affect the way in which a procurement model operates within a country’s public procurement system. However, even in the context of a largely decentralized public procurement system, many health commodities continue to be centrally procured by the national government or procuring entity. In most developing countries, the ministries of health and/or centralized government agencies (central medical stores) are largely responsible for the procurement, warehousing and distribution of medicines and health commodities. Centralized procurement may also be carried out by a parastatal or autonomous supply agency, as in Kenya and Tanzania (4). In some countries, decentralization has endowed procuring entities with the decision-‐making authority to choose whether or not to procure from the centralized system (16). Different health commodities may be procured differently. For example, predominately donor-‐funded health commodities, including vaccines and drugs for HIV, tuberculosis and malaria, continue to be centrally procured in most countries regardless of decentralization.
5.3A Case Studies of Sub-Saharan Africa
Ghana The management of the Ghana Health System is decentralized, with budget management centers at each level to facilitate the decentralization of procurement decision-‐making (16). Ghana’s public procurement system consists of the Central Medical Stores (CMS), the Regional Medical Stores (RMS), Service Delivery Points (SDPs) and the transportation network. The Ghana CMS is a unit of the Procurement and Supply Directorate of the Ministry of Health (MOH) and is responsible for the receipt, storage and distribution of commodities procured by the Procurement Unit. In this nested procurement system, medicines are first purchased by the CMS using International Competitive Bidding (ICB) and from local private suppliers and manufacturers (16). Lower levels of the health commodity supply chain then receive supplies through a pull system. RMS and teaching hospitals are expected to procure medicines from the CMS and then to the private sector if necessary. Similarly, all SDP are expected to procure from their respective RMS before turning to the private sector. The Ghana MOH conducted an in-‐depth assessment of the medicines procurement and supply management systems in the public health sector in 2009, and we have chosen to highlight a few of the assessment’s findings (16). Despite MOH policy to procure through the public system except in cases of unavailability, private sector purchases were found to be prevalent

12
throughout the supply chain. The procurement methods employed by the CMS included ICB, national competitive bidding (NCB) and selective bidding with frequencies of yearly or two times a year. The RMSs reported using NCB and direct procurement quarterly, and SDPs reported selective bidding and direct procurement on a quarterly, monthly or as and when needed basis. Procurement lead times were longest for more competitive methods, with an average lead time for ICB of 365 days, followed by selective bidding at 180 days, NCB at 90 days, and direct procurement at 14 days for RMSs and 1 day for SDPs. Average percentage days out of stock for 20 tracer medicines was also found to be greater than 50% at both the CMS and RMS, which may partially explain the prevalence of private sector purchases at lower-‐levels. Similarly, average purchase prices of the majority of tracer medicines were found to be substantially higher at SDPs than at the RMSs or CMS, which may reflect markups and/or the higher costs associated with low-‐volume private sector purchases. Errors in forecasting and delivery delays were cited as the causes of stock-‐outs at the CMS (16).
Zambia The Public Procurement Act of 2008 repealed the Zambia National Tender Board Act, decentralized public procurement and created the Zambia Public Procurement Authority as an independent oversight body (17). The Zambia MOH is responsible for the public procurement of medicines, with Medical Stores Limited (MSL) responsible for the storage and distribution of medicines throughout the country. Crown Agents was contracted by the Zambian government to manage MSL. The pharmacy unit of the MOH is responsible for quantification and forecasting of medicines, utilizing information from MSL. The MOH receives funds both from the Ministry of Finance (MOF) and from bilateral and multilateral donors, and has promoted a shift from in-‐kind donations to direct budgetary support to a sector-‐wide drug basket to improve procurement efficiency (18). The Drug Supply Budget Line (DSBL) is a unique feature of Zambia’s procurement system which coordinates procurement plans, multiple funding streams and the MOH budget (Figure 5) (18). MOF funds were historically disbursed to MOH quarterly or monthly, which often led to purchasing in smaller quantities, inhibiting the use of international tenders and resulting in higher commodity prices (18).
Tanzania As part of the 1992 Pharmaceutical Master Plan reforms, Tanzania created an autonomous Medical Stores Department (MSD) to replace the formerly ineffective Central Medical Store (19). Unlike Zambia, MSD is responsible for the procurement, storage and distribution of health commodities to the public sector and authorized private sector entities in Tanzania. Although MSD is the predominant single distributor of medical supplies and pharmaceuticals in the country, decentralization enabled hospitals and districts to control their own budgets and to procure health commodities from alternate sources (19). Many health facilities began to procure from private pharmacies and wholesalers in addition to MSD; only 33% of health facilities procured exclusively from MSD in 2007 (19). General stock availability and storage space within MSD has been historically problematic, and stock-‐outs were attributed to product delivery delays and insufficient forecasting by the MSD and its zonal stores (19). Assessments also highlighted the adverse effects of vertical, disease-‐specific supply chains on the existing

13
supply system for government-‐funded essential medicines; in addition to “crowding out” the government-‐funded supplies, non-‐coordinated vertical programs can result in duplicated efforts and increase the administrative burden of staff responsible for managing parallel funding streams and information flows (19). To characterize the complexity of the supply management system for health commodities, WHO assisted the Tanzania Ministry of Health and Social Welfare in 2007 in mapping the procurement and supply chain system of essential medicines and supplies, including funding streams (Figure 6) (20). At the time, supply system mapping was being undertaken in 10 other countries of the WHO Africa Region, including Cameroon, Ethiopia, Nigeria, Tanzania, Kenya, Zambia, Senegal, Rwanda, Mali, Uganda and the Republic of the Congo (20).
Figure 6: Medicines Supply Systems in Tanzania, 2007
5.3B Key Observation Procurement value thresholds are country-‐specific and play a significant role in determining which procurement methods are permissible and/or commonly used. Under the Model Law, ICB/open tender is the default method of procurement above a certain value threshold. ICB is widely considered to be the preferred method of procurement as it fulfills the objectives of full competition, transparency and increased value for money through bulk purchasing (13). However, the advantages of the annual or biannual ICB must be weighed against the costs. ICB is more costly, time-‐consuming and technically-‐demanding to carry out than informal methods (13). ICB also requires sufficient budgetary allocation and often inflexible forecasting and quantification, all of which can result in long lead times and stock-‐outs (16,18). As in the Ghana MOH assessment cited above, the average ICB lead time was found to be 365 days, and the resulting average percentage days out of stock for 20 tracer medicines was greater than 50% at

14
both the CMS and RMS (16). However, under the Model Law, the use of procurement methods other than open tender are only permissible in “limited and defined circumstances” and must be justified by the procuring entity (13). Many public procurement acts, including the Model Law, also explicitly prohibit the splitting of contracts by procuring entities attempting to avoid an approval threshold or a specific procurement procedure (13,17). The general lack of technical capacity, insufficient procurement planning, and the suboptimal financial and information flows characterizing many of these systems contribute to procuring entities’ poor execution of ICB, or their inability or disincentive to use ICB. The use of informal procurement methods, however, decreases competition, prohibits the achievement of economies of scale and leads to higher commodity prices. The question becomes how to maintain fair and open competition and achieve economies of scale while allowing for flexibility in quantification and ordering.
6. SYNTHESIS OF FINDINGS In comparing the public procurement systems of the U.S. Government with those of select countries of sub-‐Saharan Africa, it is important to distinguish between procurement functions and contracting practices. The procurement of health commodities is decentralized in the VA and DOD system, whereas the function remains largely centralized in the sub-‐Saharan African countries that were reviewed for this study. The key observation emerging from our assessment related to contracting practices. Centralized negotiation of pricing arrangements and the use of flexible contracts are fundamental components of VA and DOD procurement systems, but appeared to be generally absent from the procurement systems of the sub-‐Saharan African countries reviewed. Given the advantages of flexible contracting practices and the challenges faced by public procurement entities in developing countries, we assessed the current use and barriers to use of framework agreements in procurement systems of select countries of sub-‐Saharan Africa.
7. FRAMEWORK AGREEMENTS The IDIQ contracts utilized by the VA and DOD procurement systems are a type of framework agreement (13). The UNICITRAL Model Law 2011 defines a framework agreement procedure as, “…a procedure conducted in two stages: a first stage to select a supplier (or suppliers) or a contractor (or contractors) to be a party (or parties) to a framework agreement with a procuring entity, and a second stage to award a procurement contract under the framework agreement to a supplier or contractor party to the framework agreement” (21). In this context, the framework agreement itself is an agreement between the procuring entity and the selected supplier(s) or contractor(s) which is concluded after the first stage of the procedure (21). A framework agreement has been more specifically defined as contracting mechanism in which long-‐term contracts provide the terms and conditions under which smaller repeat purchasing orders (or call-‐off orders) may be issued for a defined period of time (22). Framework

15
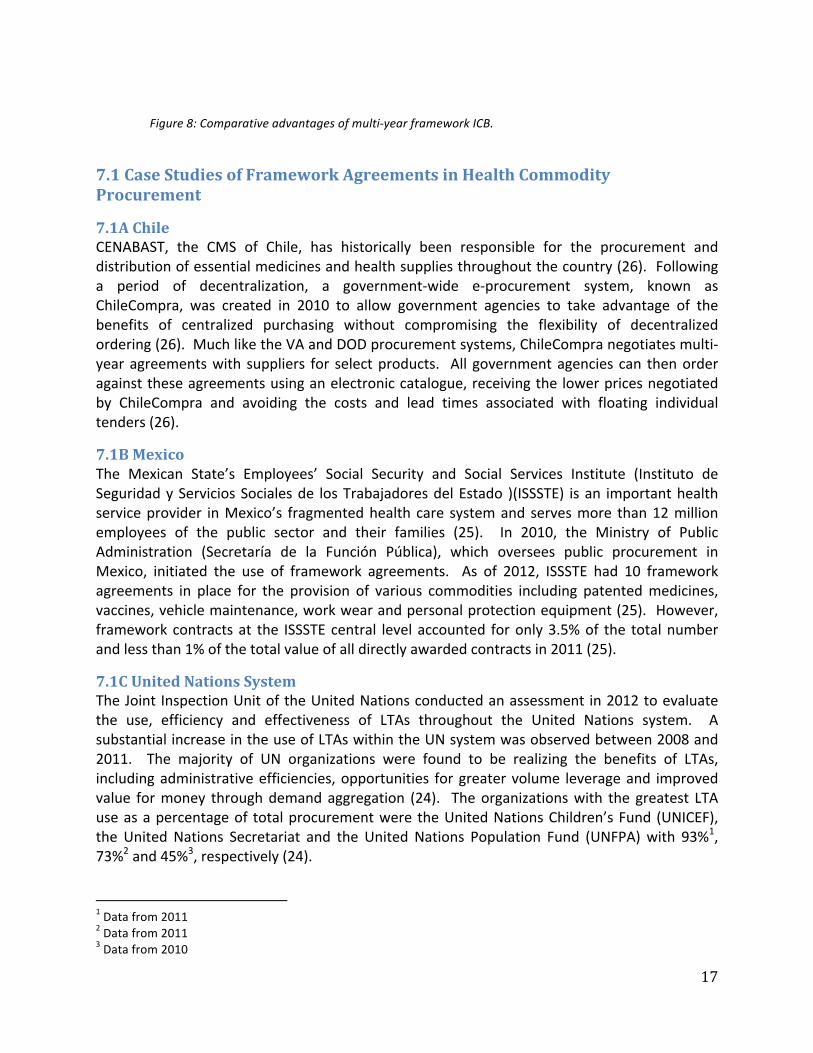
agreements are used when a recurring need is anticipated, and the procuring entity cannot predetermine the precise quantities or schedule of supplies that will be required during the contract period (11). It is important to note that different types of framework agreements may be referred to by different names depending on the specific context or legal system (13). Other names and sub-‐types include long-‐term agreements (LTAs), task-‐order contracts, call-‐off contracts, umbrella contracts, rate or running contracts, system contracts, general service agreements, blanket purchase agreements and standing offers (13,17,22–25). Framework agreements can involve single or multiple suppliers in the two stages of procurement. In a single supplier framework, a single contract is awarded to one supplier through a competitive process during the first stage of procurement, and multiple call-‐off orders are place directly against the contract throughout the duration of the agreement (13). In a multi-‐supplier framework agreement, a contract for the same good or service is signed with multiple suppliers in the first stage of procurement. The second stage of procurement in multi-‐supplier frameworks can be carried out in different ways: a secondary bidding process may take place for each call-‐off order, suppliers may have been ranked according to preference or capacity, orders may be rotated between the different suppliers, or fixed order amounts may be assigned to each supplier as part of the initial contract (13). According to European Union Public Procurement Law, multi-‐supplier frameworks can promote the participation of small and medium enterprises (SME), as call-‐off orders are smaller in size than a single bulk procurement and are spread over a longer period of time (13). By avoiding the need to repeat each step for every purchase, framework agreements can significantly reduce the time and resources required to carry out the procurement process (Figure 7) (13,22). Entities are also able to secure the benefits of centralized purchasing, through demand aggregation, while still retaining flexibility in purchase quantities and delivery schedules. Recall that all federal procuring entities of the U.S. Government may issue call-‐off orders against the IDIQ contracts centrally negotiated by the VA, thus taking advantage of the economies of scale achieved through centralized negotiation. As smaller procurements fall below the value threshold for formal methods, such as ICB, aggregation of these multiple orders into a larger framework agreement can result in increased transparency and value for money (13). The use of multiple supplier framework agreements can also help to ensure supply security, as a shortfall of one supplier can be compensated for or replaced by another supplier on the contract (13). Public procuring entities in many developing countries float ICB tenders yearly or multiple times a year, which, as noted above, is both time-‐ and resource-‐intensive, and commonly results in long lead times and stock-‐outs (16). In the face of stock-‐outs, procuring entities may turn to direct purchases from the private sector, sacrificing cost and competition for security of supply. Utilizing a framework agreement with a multi-‐year ICB procurement cycle encompasses the comparative advantages of the two procurement methods -‐ effectively preserving competition and achieving lower prices while shortening lead times and improving supply security (Figure 8). Multiple call-‐off orders and deliveries per year under framework contracts can minimize stock-‐holding expenses, improve inventory control and reduce the risk of

16
diversion or wastage common with bulk procurements (22). Administrative efficiencies can also be gained by consolidating multiple ICB tenders into a single tender every 2 years (22). Furthermore, carrying out the new ICB procurement process during the 2nd year of the previous contract creates an overlap in supply and may reduce the risk of stock-‐outs between tenders (22).
Figure 7: Framework contracts can significantly reduce the number of steps involved in the procurement process.
17
Figure 8: Comparative advantages of multi-‐year framework ICB.
7.1 Case Studies of Framework Agreements in Health Commodity Procurement
7.1A Chile CENABAST, the CMS of Chile, has historically been responsible for the procurement and distribution of essential medicines and health supplies throughout the country (26). Following a period of decentralization, a government-‐wide e-‐procurement system, known as ChileCompra, was created in 2010 to allow government agencies to take advantage of the benefits of centralized purchasing without compromising the flexibility of decentralized ordering (26). Much like the VA and DOD procurement systems, ChileCompra negotiates multi-‐year agreements with suppliers for select products. All government agencies can then order against these agreements using an electronic catalogue, receiving the lower prices negotiated by ChileCompra and avoiding the costs and lead times associated with floating individual tenders (26).
7.1B Mexico The Mexican State’s Employees’ Social Security and Social Services Institute (Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado )(ISSSTE) is an important health service provider in Mexico’s fragmented health care system and serves more than 12 million employees of the public sector and their families (25). In 2010, the Ministry of Public Administration (Secretaría de la Función Pública), which oversees public procurement in Mexico, initiated the use of framework agreements. As of 2012, ISSSTE had 10 framework agreements in place for the provision of various commodities including patented medicines, vaccines, vehicle maintenance, work wear and personal protection equipment (25). However, framework contracts at the ISSSTE central level accounted for only 3.5% of the total number and less than 1% of the total value of all directly awarded contracts in 2011 (25).
7.1C United Nations System The Joint Inspection Unit of the United Nations conducted an assessment in 2012 to evaluate the use, efficiency and effectiveness of LTAs throughout the United Nations system. A substantial increase in the use of LTAs within the UN system was observed between 2008 and 2011. The majority of UN organizations were found to be realizing the benefits of LTAs, including administrative efficiencies, opportunities for greater volume leverage and improved value for money through demand aggregation (24). The organizations with the greatest LTA use as a percentage of total procurement were the United Nations Children’s Fund (UNICEF), the United Nations Secretariat and the United Nations Population Fund (UNFPA) with 93%1, 73%2 and 45%3, respectively (24).
1 Data from 2011 2 Data from 2011 3 Data from 2010

18
UNICEF UNICEF establishes LTAs with manufacturers following a competitive tendering process (27). The objective of these LTAs is to establish forecasts on quantities to be produced by the manufacturer(s) and quantities to be purchased in order to secure the supply of the product over the duration of the agreement (27). UNICEF uses both single and multiple LTAs to ensure greater supply security, and commonly splits arrangements to issue awards to multiple suppliers per vaccine presentation (24,27). Two different types of LTAs are defined by the UNICEF procurement policies. Target-‐value LTAs are generally used for strategic essential supplies, are often split among multiple suppliers, and expire either when the maximum target amount or the date of contract expiry is reached (24). Time-‐bound LTAs are used when the unreliability of the historical data and/or forecasted demand precludes the creation of target-‐value LTAs and expire when the date of contract expiry is reached regardless of the volume procured (24). The contract duration for LTAs issued by UNICEF ranged from 1-‐10 years, with an average of 2 years plus a 1-‐year extension possibility (24). Framework agreements are often seen and/or feared as being anti-‐competitive; by engaging in a framework contract with one manufacturer, other manufacturers may be excluded from entering the market for the duration of the contract. However, UNICEF policies explicitly include provisions for allowing the entrance of new manufacturers into the market in the middle of a multi-‐year tender (27). A set of conditions is outlined under which awards would be considered after the initial awards had been issued for a specific tender. If a manufacturer is not WHO prequalified for the vaccine/product at the time of tender, the manufacturer must show a plan for obtaining prequalification (27). If WHO prequalification is obtained, UNICEF considers awarding or reallocating a quantity to the manufacturer if UNICEF is facing a monopoly situation, if there is a lack of performance from the current manufacturer(s) or if there is insufficient supply from the current manufacturer(s) (27)
UNFPA As the largest procurer of reproductive health commodities, United Nations Population Fund (UNFPA) is able to achieve economies of scale and competitive prices on a variety of quality assured products. UNFPA has established LTAs with more than 50 international manufacturers, with the intent to include all products under LTAs in the future (28). National governments, non-‐governmental organizations, and other public sector purchasers are able to take advantage of the competitive prices negotiated by UNFPA through the AccessRH portal: a UNFPA-‐managed procurement and information service for reproductive health commodities (29).
7.1D Global Fund to Fight AIDS, Tuberculosis and Malaria The Global Fund provides another example of a key global health stakeholder utilizing framework agreements to achieve greater value for money and supply security. A key component of the Global Fund’s Long-‐Lasting Insecticidal Net (LLIN) strategy is a shift toward the use of long-‐term contracts to provide production optimization, a more sustainable market, and greater visibility for capacity planning (30). The bulk of the forecasted volume of LLINs for 2014 will be allocated using a 2-‐year LTA to multiple suppliers (30).

19
7.2 Legislative Provision for Framework Agreements in Sub-Saharan Africa In assessing the use and challenges to use of framework agreements in countries of sub-‐Saharan Africa, we first looked to the public procurement legislation and official documents issued by the procurement authorities of select countries. The UNICTRAL Model Law of 1994, which served as the backbone of the public procurement legislation of many developing countries, made no explicit mention of framework agreements (13). However, The UNCITRAL Model Law of 2011 clearly outlines the conditions for use of framework agreements and corresponding procedures (21). According to the Model Law 2011, a framework agreement procedure may be utilized where the procuring entity determines that the procurement need is anticipated to arise on a repeated, indefinite or urgent basis during a given period of time (21). The Tanzania Public Procurement Act of 2004 and the Uganda Public Procurement and Disposal of Public Assets Act of 2003 both include provisions for the use of framework contracts, “wherever appropriate to provide an efficient, cost effective and flexible means to procure works, services or supplies that are required continuously or repeatedly over a set period of time” (31,32). The Zambia Public Procurement Act of 2008 includes almost verbatim provisions for making use of rate or running contracts (17). There was no mention of framework agreements in the Kenya Public Procurement and Disposal Act of 2005, but Framework Contracting Guidelines were issued by the Kenya Public Procurement and Oversight Authority in 2010 (33). Similarly, framework contracts were not mentioned in Ghana’s Public Procurement Act of 2003, but a subsequent manual issued by the Public Procurement Board to assist procuring entities in complying with the act includes provisions for using “Framework (Call-‐off) Contracts for six months or a year, to permit further economies of bulk purchasing, saving of time wasted by separate procurements, and a reduction of the need to maintain high stock levels” (34). The Mozambique Decree No. 15/2010 approving the Rules and Procedures on Procurement of Public Works, Supply of Goods and Services does not mention framework agreements, but does limit the duration of contracts “to a maximum duration of a year, prolonged only one time, for equal period, as long as the initial contractual conditions are maintained” (35).
7.3 Current Use of Framework Agreements in Select Countries of Sub-Saharan Africa The Zambia Ministry of Health acquired permission from the Public Procurement Authority in 2008 to utilize framework agreements in the procurement of medicines and health commodities in an effort to avoid the long lead times associated with international tenders. The same year, MOH and the Drug Supply Budget Line began creating flexible long-‐term contracts with national suppliers (36). As the goal of the MOH’s procurement plan is commodity security, the MOH aims to place as many strategic and essential products on framework contracts as possible. Currently, the Zambia MOH is engaged in single-‐supplier framework contracts with five manufacturers or wholesalers for essential medicines from the Zambia National Essential Drug List, including antimalarial drugs, I/V fluids, and various antibiotics for infectious diseases. These framework contracts are time-‐bound with fixed volumes per product and have a 2-‐year minimum duration. Forecasted orders are placed once a year, corresponding to budgetary allocation, and approximately four call-‐off orders and

20
deliveries take place per year per supplier. The use of framework agreements in Zambia has resulted in added flexibility in quantities ordered and delivery schedules, increased availability of medicines and a drop in stock-‐outs. Zambia MOH has also seen an improvement in relationships with suppliers, the creation of additional transparencies and overall efficiency gains from the use of framework contracts.4 In 2008, Ghana Health Service was in the process of establishing National Framework Agreements with local private sector suppliers so as to utilize the contracting capacity at the central level to negotiate lower prices for the decentralized procuring entities (36). Currently, time-‐bound framework agreements are used in Ghana in the procurement of antiretroviral medicines. Although the benefits of commodity assurance far outweigh the potential disadvantages, there have been issues with supplier adherence to the framework contracts, specifically regarding shipment schedules, which have led to overstocking, expiries or shortages.5 The Botswana Ministry of Health, in collaboration with USAID Supply Chain Management System and Crown Agents, began transformations to the Botswana CMS in 2007 (37). As part of these efforts, a new procurement strategy was implemented to include 140 vital drugs under long-‐term framework agreements (37). The Secretariat Procurement Unit of the Southern African Development Community (SADC) manages a database of approved suppliers and places purchase orders under multiple framework contracts (38). SADC is also engaged in pooled procurement, whereby Member States purchase directly from prequalified regional suppliers holding framework contracts (39).
7.4 Barriers to Use of Framework Agreements Mozambique’s public procurement legislation, Decree 15, does not mention framework agreements and does not allow for multi-‐year contracts. It is unclear if the absence of a provision to use framework agreements disallows their use or if the prohibition spurs from the limit on contract duration. Even though the aforementioned definitions for framework agreements do not include a minimum duration of time, they are usually valid for more than one year (13,21,24). In either case, framework agreements in Mozambique may not be an option in the future without legislative change. The lack of legislative provision for framework agreements may serve as a barrier in other developing countries. In the current procurement system in Mozambique, importers work with manufacturers to register and authorize market entry for new products. The Central de Medicamentos e Artigos Médicos (CMAM), the CMS of Mozambique, purchases medicines directly from importers and does not generally negotiate directly with manufacturers. 6 Operating through a third party
4 Correspondence with Dr. Bonface Fundafunda, Head of Zambia Drug Supply Budget Line 5 Correspondence with Joycelyn Azeez, Head of Procurement Unit of CMS 6 Correspondence with Rosalie Faniyo, Senior Technical Advisor for PSM – FORSSAS, Deloitte Consulting LLP, Central de Medicamentos e Artigos Médicos

21
importer to access supplies may result in efficiency gains from the private sector, but may also preclude centralized negotiation of flexible contracts by CMAM. Engaging in successful framework agreements requires adequate financial and human resources, including sufficient technical capacity in contract management and the ability to continually prepare, negotiate, manage, evaluate and conduct performance reviews.7 The general lack of technical capacity at both the national and procuring entity levels has been commonly cited as a barrier to more efficient procurement practices and supply security (4,16,40). Inadequate knowledge or understanding of the public procurement legislation may also serve as a barrier to the use of framework agreements, especially for countries that have undergone recent reforms. Additional concerns surrounding framework agreements which may act as a barrier to their implementation and use include price volatility, local manufacturer participation and the inclusion of new technology during the course of the framework contract. As mentioned, multi-‐supplier framework agreements involve two stages and varying levels of competition. In the case of volatile markets, prices may be excluded from the terms and conditions agreed upon in the first stage of competition. Call-‐off orders may then be allocated to suppliers on the framework through a mini-‐competition which includes revised, current prices (13). Similarly, as call-‐off orders are of smaller volumes than bulk procurements, multi-‐supplier framework agreements may promote participation of local manufacturers by rotating call-‐off orders among suppliers on the framework (13). Target-‐value (volume-‐based) LTAs may also be split among multiple suppliers, with an appropriate and capacity-‐based volume allocated to local suppliers. The need for flexibility and responsiveness in the procurement of health commodities is especially relevant when considering the entry of new technology into the market. So as to promote open competition, and to maintain the overarching goal of improving health, framework agreements for health commodities must consider provisions for entry of new suppliers into the market during the course of an existing framework contract. Although UNICEF procurement policies do include provisions for allowing entrance of new manufacturers into the middle of a multi-‐year tender, the set of conditions under which this entrance is permissible does not specifically include the emergence of new technology.
8. CONCLUSIONS With adequate technical capacity and appropriate legal provisions, framework agreements can allow for flexibility and responsiveness in ordering and delivery while maintaining transparency and achieving greater value-‐for-‐money in the procurement of essential medicines and health commodities. In assessing the public procurement systems of two US federal agencies involved in public procurement of health products (VA and DOD), the centralized negotiation of framework agreements with decentralized ordering were identified as key success factors. The
7 Correspondence with Dr. Bonface Fundafunda, Head of Zambia Drug Supply Budget Line

22
use of framework contracts is widespread in the U.S. federal government and the UN system, and may reflect the technical capacity more commonly found in developed countries and global agencies. In 2012, 97% of OECD countries responding to a OECD survey reported routine use of framework agreements in some or all procuring entities at the central level (25). In the VA and DOD procurement systems, framework agreements are utilized to control drug costs and are a fundamental component of the prime vendor program. Framework contracts for health commodities are first negotiated between the central government agency and multiple manufacturers. This facilitates direct ordering by the decentralized government procuring entities from private distributors/wholesalers operating under these service contracts. The extensive reach and commercial capacity of prime vendors enables just-‐in-‐time delivery of purchase orders directly to facilities. Rather than having high-‐volume on-‐hand inventory at a single or a few central warehouses, prime vendors operate dozens of smaller distribution centers and rely on timely data to increase the movement of inventory through the supply system. In contrast, the public procurement of health commodities in select countries of sub-‐Saharan Africa is largely centralized and the use of framework agreements appears to be limited. Ghana and Zambia provide examples of countries which have adopted single-‐supplier framework agreements in the procurement of select essential medicines. It remains unclear if the public procurement entities of other sub-‐Saharan African countries are utilizing framework agreements to some degree for select products. In some instances procurement legislation which prohibits the use of framework contracts may also serve as a key barrier to use, as is the case in Mozambique. Inadequate technical and contract management capacity was commonly cited as a weakness of national procurement systems and may serve as a more salient barrier to the use of strategic contracting practices within many developing countries.
9. RECOMMENDATIONS Additional and more comprehensive research on the use (and non-‐use) of framework agreements in the public procurement for health commodities in developing countries is warranted. Highlighting successful use of framework contracts in sub-‐Saharan Africa may incentivize additional countries to adopt more strategic contracting practices. For countries without the legislative provision for framework agreements, we recommend working toward legislative reform to include such provisions onto the public procurement legislation. Where legislative provision is in place, procuring entities must work to strengthen technical and contract management capacity and actively promote the use of framework agreements throughout the procurement system. A global task force would be well-‐positioned to address this issue and assist developing countries in the adoption and execution of framework agreements in the procurement of health commodities with use of sufficient data, evidence-‐based advocacy, strengthening of procurement capacity and change management.

23
REFERENCES
1. United Nations. The Millennium Development Goals Report 2013. New York; 2013.
2. Cameron a, Ewen M, Ross-‐Degnan D, Ball D, Laing R. Medicine prices, availability, and affordability in 36 developing and middle-‐income countries: a secondary analysis. Lancet. 2009 Jan 17;373(9659):240–9.
3. The World Bank. Least developed countries: UN classification [Internet]. Available from: http://data.worldbank.org/region/LDC
4. Dickens T, PATH, World Health Organization. The World Medicines Situation 2011: Procurement of Medicines. 2011.
5. OECD-‐DAC, Zambia National Tender Board. OECD-‐DAC JV For Procurement Country Pilot Programme Zambia: Assessment of Public Procurement System. 2007.
6. OECD Task Force on Public Financial Management. Policy Brief 1: Aid Effectiveness Community -‐ What are the benefits of using country systems? 2008.
7. United States Government Accountability Office. Prescription Drugs: Comparison of DOD and VA Direct Purchase Prices. 2013.
8. Dicken JE. Prescription Drugs: Overview of Approaches to Control Prescription Drug Spending in Federal Programs. 2009;
9. VA Federal Supply Schedule Service Home [Internet]. Available from: http://www.fss.va.gov/
10. Congressional Budget Office. The Department of Veterans Affairs’ Pharmaceutical Prime Vendor Program. 2009.
11. General Services Administration, Department of Defense, National Aeronautics and Space Administration. Federal Acquisition Regulation. 2005.
12. Directorate of Medical Material Defense Logistics Agency Troop Support. DAPAs Made Easy: A Guide to DAPAs and the Medical/Surgical Prime Vendor Program. 2011;
13. Arrowsmith S, Treumer S, Fejø J, Jiang L. Public procurement regulation: an introduction. 2011 [cited 2013 Nov 26]; Available from:
24
http://eprints.nottingham.ac.uk/1689/1/eprintspublicprocurementregulationintroduction.pdf
14. Nicholas C. Work of UNCITRAL on government procurement: purpose, objectives, and complementarity with the work of the WTO. The WTO Regime on Government Procurement: Challenge and Reform [Internet]. 2011 [cited 2013 Oct 28]. Available from: http://bit.ly/J9DQr5
15. World Health Organization, Management Sciences for Health, JSI. A Situational Analysis and Feasibility Study on Regional Pooled Bulk Procurement of Essential Medicines and Other Health Supplies in the East African Community Partner States: Final Report. 2007;
16. Ghana Ministry of Health, DFID, World Health Organization. Ghana: Assessment of Medicines Procurement and Supply Management Systems in the Public Health Sector. 2009.
17. Government of Zambia. The Public Procurement Act, 2008. 2008.
18. Yadav P. Analysis of the Public, Private and Mission Sector Supply Chains for Essential Drugs in Zambia. 2007 p. 0–24.
19. Management Sciences for Health. Chapter 8: Pharmaceutical supply strategies. MDS-‐3: Managing Access to Medicines and Health Technologies. Third. Arlington, VA; 2012.
20. Ministry of Health and Social Welfare, World Health Organization. Mapping of the Medicines Procurement and Supply Management System in Tanzania. 2008.
21. UNCITRAL. UNCITRAL MODEL LAW ON PUBLIC PROCUREMENT. 2011;17(17).
22. Hussain Z, Tukai M, Adu JA, Khan AI. Workshop on Framework Agreement and Two-‐Year Procurement Cycle at Proshika HRDC, Koitta, Manikgonj, March 6-‐8, 2012.
23. UNICEF. Procurement Process for Pharmaceuticals. Consultation with Pharmaceutical Manufacturers. 2010.
24. Terzi C, Callejas JF, United Nations Joint Inspection Unit. Review of Long-‐term Agreements in Procurement in the United Nations System. Geneva; 2013.
25. OECD Public Governance Committee. OECD Public Procurement Review of the Mexican Institute of Social Security and Services for State Workers (ISSSTE). 2013.
26. Bornbusch A, Bates J. Multiplicity in public health supply systems: a learning agenda. Glob Heal Sci Pract. 2013 Jun 13;1(2):154–9.

25
27. UNICEF Supply Division. Overview of UNICEF Procurement Processes: Industry Consultation. Copenhagen 27th January 2012. 2012.
28. UNFPA Procurement [Internet]. Available from: http://www.unfpa.org/public/procurement
29. About us -‐ AccessRH [Internet]. Available from: http://www.myaccessrh.org/about-‐us
30. The Global Fund to Fight AIDS Tuberculosis and Malaria. The Global Fund ’ s LLIN Procurement Strategy , Tender Process and Future Plans: Global Fund/UNICEF Pre-‐tender briefing, Copenhagen, 20th August 2013.
31. Uganda. The Public Procurement and Disposal of Public Assets Act. 2003;
32. Parliament of the United Republic of Tanzania. The Public Procurement Act, 2004. 2004.
33. Kenya Public Procurement Oversight Authority. The Public Procurement Guidelines for Framework Contracting. 2010 p. 1–12.
34. Ghana Public Procurement Board. Ghana Public Procurement Act, 2003 (Act 663) Manual. 2003 p. 1–132.
35. Republic of Mozambique. Decree No. 15. 2010;
36. Ballou-‐Aares D, Freitas A, Kopczak L. Private sector role in health supply chains: Review of the role and potential for private sector engagement in developing country health supply chains. Dalb Glob Dev Advis MIT-‐Zaragoza Int Logist Progr. 2008;
37. Crown Agents -‐ Central medical stores in Botswana: transformation from within (SCMS) [Internet]. Available from: http://www.crownagents.com/our-‐work/projects/detail/scms
38. Southern African Development Community :: Procurement [Internet]. Available from: http://www.sadc.int/sadc-‐secretariat/directorates/office-‐deputy-‐executive-‐secretary-‐finance-‐administration/procurement/
39. Southern African Development Community. DRAFT_SADC STRATEGY FOR POOLED PROCUREMENT OF ESSENTIAL MEDICINES AND HEALTH COMMODITIES 2013-‐2017. 2012.
40. World Bank, Republic of Mozambique. Update of the Country Procurement Assessment Review (CPAR). 2008.