Embed Size (px)
Citation preview

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 19
Asthma and allergy patterns over 18 years aftersevere RSV bronchiolitis in the first year of life
Nele Sigurs1 Fatma Aljassim23 Bengt Kjellman4 Paul D Robinson56
Fridrik Sigurbergsson7 Ragnar Bjarnason8 Per M Gustafsson249
ABSTRACTBackground An increased prevalence of asthma recurrent wheeze (RW) clinical allergy and allergicsensitisation up to age 13 years has previously beenreported in subjects hospitalised with respiratorysyncytial virus (RSV) bronchiolitis in their first year of lifecompared with matched controls A study wasundertaken to examine whether these features persistinto early adulthood to report longitudinal wheeze andallergy patterns and to see how large and small airwayfunction relates to RSV infection and asthmaMethods Follow-up at age 18 years was performed in46 of 47 subjects with RSV and 92 of 93 controls
Assessments included questionnaire clinicalexamination skin prick tests serum IgE antibodies toinhaled allergens blood eosinophils fraction of exhalednitric oxide (FeNO) spirometry multiple breath washout(lung clearance index LCI) and dry air hyperventilationchallengeResults Increased prevalence of asthmaRW (39 vs9) clinical allergy (43 vs 17) and sensitisation toperennial allergens (41 vs 14) were present at age18 in the RSV cohort compared with controls Persistent relapsing wheeze associated with early allergicsensitisation predominated in the RSV cohort comparedwith controls (30 vs 1) Spirometric function was
reduced in subjects with RSV with or without currentasthma but not in asthmatic controls LCI was linkedonly to current asthma airway hyperresponsiveness andFeNOConclusions Severe early RSV bronchiolitis isassociated with an increased prevalence of allergicasthma persisting into early adulthood Small airwaydysfunction (LCI) is related to current asthma and airwayinflammation but not to RSV bronchiolitis Reducedspirometry after RSV may reflect airway remodelling
INTRODUCTION
Respiratory syncytial virus (RSV) infection is themost common cause of severe bronchiolitis ininfants1 It is now established that early severe virallower respiratory tract infections (LRTI) arefrequently followed by recurrent wheeze asthmaand allergy during childhood2 3
A number of previous studies have investigatedthe association between RSV infection in infancy and later development of asthma although differ-ences in timing and severity of RSV infection existbetween studies The Tucson Childrenrsquos Respira-tory Study (a birth cohort study) reported anincreased prevalence of respiratory symptoms until
age 11 and residual impaired lung function at age 13in those experiencing a relatively mild RSV LRTI
(not requiring hospitalisation) during the 1047297rst3 years of life4 Impaired lung function at age 10 hasalso been reported following hospitalisation in the1047297rst year with proven LTRI5 Recently data froma cohort previously hospitalised in the 1047297rst 2 yearsof life and followed up at 18e20 years suggestedthat this impairment may persist into early adult-hood6 Histopathology studies of fatal RSV bron-chiolitis demonstrate extensive damage to theairway epithelium and marked small airway obstruction7 yet the presence of persistent smallairway damage in later life is unclear In adultasthma small airway dysfunction is closely asso-ciated with bronchial hyper-responsiveness8 9 afundamental component of asthma correlated todisease severity10
Our cohort represents infants aged lt1 year withsevere primary RSV bronchiolitis (4347 6 months of age at hospitalisation) We have previ-ously demonstrated increased prevalence of asthmaor recurrent wheeze (RW) and allergic sensitisationcompared with a matched control cohort at ages 37 and 13 years11e13 In this paper we present the18-year follow-up data together with a longitudinalanalysis of wheeze and allergy patterns Theprimary aim was to see if the higher prevalence of
asthma or RW clinical allergy and allergic sensiti-sation persist at age 18 The secondary aims were todescribe the wheeze patterns in both cohorts and toinvestigate how large and small airway functionrelate to severe RSV bronchiolitis current asthmaairway hyper-responsiveness (AHR) and markers of allergic in1047298ammation
METHODSThe study design is summarised in table 1 Forty-seven children aged lt1 year hospitalised with RSVLRTI14 between December 1989 and April 1990constituted the index group An age- and gender-
matched control group (nfrac1493) was recruited fromchildren attending the same child healthcarecentres as the index cases Both cohorts werefollowed up prospectively at ages 1 3 7 13 and18 years Diagnosis of bronchiolitis was originally based on criteria published by Court15 but was alsoconsistent with other later published criteria16
Demographic details at age 18 are given in table 2Structured questionnaires were completed at all
follow-up time points to record demographichereditary and clinical symptoms of allergy orwheeze A clinical examination was also performedThe investigations performed at each assessment
are summarised in table 1 Details on skin pricktests (SPT) and serum IgE tests are given in our
See Editorial p 1033
lt Additional tables arepublished online only To viewthese files please visit the
journal online (httpthoraxbmjcom)
1Department of PaediatricsBoras Central Hospital BorasSweden2Queen Silvia ChildrenrsquosHospital Goteborg Sweden3Department of PaediatricsAlwasl Hospital Dubai HealthAuthority Government of Dubai
UAE4Department of PaediatricsCentral Hospital SkovdeSweden5Department of RespiratoryMedicine The ChildrenrsquosHospital at Westmead Australia6The Childrenrsquos Hospital atWestmead Clinical SchoolDiscipline of Paediatrics andChild Health Faculty ofMedicine University of SydneyAustralia7Emergency DepartmentLandspitali University HospitalReykjavik Iceland8University of Iceland
Department of PaediatricsLandspitali University HospitalIceland Reykjavik Iceland9The Sahlgrenska Academy atthe University of GothenburgGothenburg Sweden
Correspondence toDr Nele Sigurs Department ofPaediatrics Boras CentralHospital Boras S-50182Swedennelesigursvgregionse
Received 14 June 2009Accepted 2 April 2010
Published Online First27 June 2010
Thorax 2010651045e1052 doi101136thx2009121582 1045
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 29
previous publications11e13 The speci1047297c IgE assay method used(ImmunoCAP) was consistent throughout the study period
Spirometry was performed at baseline from age 7 and post-
bronchodilator at ages 13 and 18 years according to AmericanThoracic Society recommendations17 and expressed as standarddeviation scores (z-scores) using recently published normativedata18 19 Inhaled long-acting b2 agonists were withheld for 24 hand short-acting b2 agonists or cromoglycates for 6 h prior totesting Inhaled corticosteroids (ICS) if used were not discon-tinued Isocapnic dry air hyperventilation challenge (DACh) wasperformed after baseline spirometry at age 13 and 18 years(described in more detail in the online supplement) At age 18prior to these lung function tests the fraction of nitric oxide inexpired air (FeNO) was measured in duplicate at an expiratory 1047298ow of 50 mls using the Niox Mino (Aerocrine StockholmSweden) and the mean FeNO result reported
Multiple-breath washout (MBW) was performed before
spirometry using sulfur hexa1047298uoride (SF6 ) as the marker gas and
a mass spectrometer for gas analysis and as previously describedin detail elsewhere20 Lung clearance index (LCI) was calculatedas the number of lung volume turnovers (ie the cumulative
expired volume divided by the functional residual capacity)needed to lower the end-tidal tracer gas concentration to 140thof the starting concentration A high value of LCI thus indicatesabnormal ventilation distribution The mean LCI result fromthree MBWs in each subject was reported In a previous study including healthy subjects the mean SD and upper limit of
Table 1 Study design and proportion of the 47 children in the RSV cohort and the 93 in the control cohort seen at follow-up during the study period
Age (years)
1 15 2 and 25 3 7 13 18
Total number (RSV controls) 47 93 47 93 47 93 47 93 46 92 46 92
of cohort (RSV and controls) 100 100 100 100 985 985
Questionnaire 3 3 3 3 3 3
Examination 3 3 3 (46 89) 3 (45 89) 3 (42 87)
Skin prick tests (RSV controls) 3 (47 92) 3 (45 92) 3 (44 89) 3 (42 87) 3 (41 85)
Egg white 3 3 3
Cat 3 3 3 3
Dog 3 3 3
Horse 3 3 3
Birch 3 3 3 3
Timothy 3 3 3
Mugworth 3 3
HDM ( D pteronyssinus) 3 3 3 3
HDM ( D farinae) 3 3
Mould (Cladosporium herbarum) 3 3 3
Mould ( Alternaria alternata) 3 3
Blood samples 3 3 (44 87) 3 (44 86) 3 (41 85)
IgE to food allergens (Fx5) 3 3
IgE to inhaled allergens (Phadiatop) 3 3 3 3 (41 85)
Blood eosinophil counts 3 (40 86)Lung function tests 3 (44 86) 3 (44 86) 3 (42 86)
Spirometry 3 3 3
Multiple breath washout (LCI) 3 (41 86)
FeNO 3 (42 86)
DACh 3 (43 86) 3 (41 86)
Numbers in parentheses (RSV controls) if differed from numbers followed up at that time pointA skin prick test weal with a mean diameter $3 mm was regarded positive Phadiatop (Pharmacia Upjohn Diagnostics AB Uppsala Sweden) is a screening test for antibodies to inhaledallergens Fx5 (Pharmacia Upjohn Diagnostics AB Uppsala Sweden) is a screening test for food allergensHDM house dust mite DACh dry air hyperventilation challenge LCI lung clearance index FeNO fractional exhaled nitric oxide RSV respiratory syncytial virus
Table 2 Demographic data and family history of the respiratorysyncytial virus (RSV) and control groups at age 18
Variable RSV (n[46) Controls (n[92)
Weight (kg) 65 (12) 70 (13)
Height (cm) 174 (10) 174 (10)
Parental atopy 3046 (65) 5292 (56)
Parental asthma 1846 (39) 2592 (27)
Tobacco smoke exposure
Active 1045 (22) 1492 (15)
Passive (family member) 1945 (42) 4092 (43)
Indoor furred pets 2446 (52) 5692 (61)
Mean (SD) or proportions (percentages) of subjects are given No significant differenceswere seen between the groups
Table 3 Wheeze patterns defined from the presenceabsence (+ ) ofasthmarecurrent wheeze at four follow-up stations and the numbers ofcases in each wheeze pattern group for each cohort
Wheeze pattern
Age (years)
RSV (n[46) Controls (n[92)3 7 13 18
Never wheeze 14 (3 11) 69 (27 42)
T ra nsient wheeze + 7 (5 2) 11 (8 3)
Remittingintermittent + 7 (4 3) 4 (2 2)
+
+ +
+ +
+ + +
Late onset + + 4 (1 3) 7 (3 4)
+
Persistentrelapsing + + + + 14 (7 7) 1 (1 0)
+ + +
+ + +
+ + +
+ +
Male female distribution shown in parenthesesStatistical evaluation refers to comparison of proportion of subjects in the different wheeze
pattern groups in the RSV and control cohorts plt0001RSV respiratory syncytial virus
1046 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 39
normality (ULN mean + 196 SD) for LCI were 633 043 and717 respectively20
At each follow-up time point asthma was de1047297ned as $3episodes of physician-veri1047297ed wheeze and RW as $3 episodes of parent-reported wheeze De1047297nitions of the wheezing patternsover time are shown in table 3 Allergic rhinoconjunctivitis(ARC) or clinical allergy was de1047297ned as rhinitisconjunctivitisoccurring at least twice following exposure to a particular
allergen and unrelated to infection Atopic dermatitis (AD) wasde1047297ned as a pruritic chronic or chronically relapsing non-infec-tious dermatitis Allergic sensitisation implied occurrence of IgEantibodies estimated by SPT andor serum IgE tests Currentdisorder denotes symptoms over the last 12 months Active andpassive smoke exposures the presence of pets in the householdand atopic or allergic heredity were assessed by questionnaire A positive history of atopic disease (AD ARC or asthma) in 1047297rst-degree relatives (parents or siblings) was based on physiciandiagnosis
Statistical analyses Yatesrsquo corrected c2 test was used for estimation of differences in
prevalence among groups and subgroups One-way ANOVA wasused for parametric continuous variables and Tukey HSD forsubsequent group comparisons if the overall F-test was signi1047297-cant A Manne Whitney test was used to test group differencesfor non-parametric continuous variables 95 CIs for mean andmedian differences were calculated c2 tests for trend were usedto assess the combined in1047298uence of group allocation (RSV vscontrol) and a parental history of physician-diagnosed asthmaon asthmaRW ARC and sensitisation at age 18 Pearsoncorrelation tests were used to assess correlation of parametricdata while the Spearman rank test was used for non-parametricdata KaplaneMeier survival analysis was used to compare timefree from diagnosis of asthma ARC positive Phadiatop test orpositive SPT to any perennial allergen at a follow-up station p
values based on Mantel-Cox log ranks were calculated Multi-variate logistic regression analyses were performed to establishrisk factors for asthmaRW asthma alone and ARC at age 18ORs with 95 CI and p values were reported Additionallyconditional logistic regression tests were performed to adjust forany degree of residual confounding due to the constitution of
the groups during the study period SPSS Version 150 softwarefor Windows (SPSS Inc Chicago Illinois USA) SPSS Sample-Power 20 software and CI Analysis software version 212(Trevor Bryant University of Southampton) were used for thestatistical analyses
RESULTSForty-six of the 47 subjects with RSV and 92 of the 93 controls
were followed up to 18 years of age The demographic details of the two cohorts at age 18 are summarised in table 2 and fromage 1e18 years in table E1 in the online supplement Nosigni1047297cant differences were seen at age 18
Cross-sectional data at age 18Current asthmaRW was documented in 18 of 46 (39) subjectswith RSV and 8 of 92 (9) controls (pfrac140001) Current asthmaalone was found in 15 of 46 (33) subjects with RSVand 6 of 92(7) controls (plt0001) ARC was diagnosed in 20 of 46 subjects with RSV (43) and 16 of 92 (17) controls (pfrac140002)No difference was found in the prevalence of AD (5 of 46 (11)subjects with RSV vs 8 of 92 (9) controls)
The prevalence of sensitisation determined by SPT wassigni1047297cantly increased in the RSV cohort compared withcontrols to any animal dander (cat dog horse) (33 vs 11pfrac140005) or any perennial (animal danders and house dust mites(HDM)) (41 vs 14 pfrac140001) (see table E2 in onlinesupplement) A higher prevalence of positive Phadiatopresponses was seen in the RSV cohort (56 vs 28 p frac140005)(see table E2 in online supplement) For the whole cohort themost commonly identi1047297ed speci1047297c IgE antibodies performed inthose testing positive to Phadiatop screening were to lsquoany perennialrsquo (39 of 126 31) and were signi1047297cantly increased insubjects with RSV compared with controls (51 vs 21pfrac140001)
Airway function data are summarised in table 4 Reduced
spirometric airway function (forced expiratory volume in 1 s(FEV1) ratio of FEV1 to forced vital capacity (FVC) and forcedexpiratory 1047298ow at 25e75 FVC (FEF25e75)) was documented inthe RSV cohort compared with controls but LCI did not differ
AHR bronchodilator response and blood eosinophil cell countswere greater in the RSV cohort than in the controls but FeNO
Table 4 Airway function and inflammatory markers in RSV and control groups at age 18 years
RSV (n[46) Control (n[92) 95 CI for difference
Resting
FEV1 (z-score) 028 (093) 011 (108) 000 to 07
FEV1 FVC (z-score) 068 (085) 008 (103) 024 to 097
FEF25e75 (z-score) 060 (077) 005 (085) 025 to 086
LCI 663 (052) 659 (043) 021 to 013Challenge (DACh)
Fall in FEV1 () 47 (00e378) 31 (00e428) 00 to 32
Post-bronchodilation
Rise in FEV1 () 59 (00e105) 31 (00e104) 05 to 34
FEV1 (z-score) 016 (071) 038 (130) -018 to 061
FEV1 FVC (z-score) 004 (088) 042 (095) 011 to 080
FEF25e75 (z-score) 001 (078) 038 (083) 009 to 069
Inflammatory markers
FeNO (ppb) 14 (6e84) 13 (5e74) 1 to 5
Blood eosinophil counts (3109 l) 020 (004e057) 014 (001e079) 001 to 010
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001For exact number of subjects in RSV and control group performing each test see Table 1
DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25
e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in
1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus
Thorax 2010651045e1052 doi101136thx2009121582 1047
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 49
was not FEV1 FVC and FEF25-75 remained lower in the RSVcohort after bronchodilation Subjects with RSV had lowerspirometry results than the controls irrespective of currentasthmaRW diagnosis (table 5) Spirometry 1047297ndings were similarin controls with or without current asthmaRW LCI wassigni1047297cantly raised in subjects with RSV (pfrac140006) and controls(pfrac140033) with current asthmaRW compared with corre-
sponding subjects without asthma (see table E3 in onlinesupplement) Only LCI differed signi1047297cantly between thecontrols with and those without current asthmaRW (see tableE4 in online supplement) In the RSV cohort the maximumpercentage fall in FEV1 after dry air challenge correlated signi1047297-cantly with LCI (r2
frac14044 plt0001) FeNO levels (r2frac14026
plt0001) and with blood eosinophil counts (r2frac14012 pfrac140011)
Table 5 Airway function and inflammatory markers in RSV versus control subjects with or without current asthmaRW at age 18 years
Current asthmaRW No current asthmaRW
RSV (n[18) Controls (n[8) 95 CI for difference RS V (n[24) Controls (n[78) 95 CI for difference
Resting
FEV1 (z-score) 064 (085) 005 (077) 003 to 142 000 (091) 011 (111) 000 to 077
FEV1 FVC (z-score) 089 (082) 008 (137) 009 to 186 053 (086) 010 (100) 024 to 097
FEF25e75 (z-score) 089 (071) 006 (086) 017 to 1 50 038 (075) 005 ( 0 85) 025 to 086
LCI 688 (063) 689 (025) 046 to 049 644 (031) 656 (043) 021 to 129
Challenge (DACh)
Fall in FEV1 () 85 (00e378) 75 (03e428) 55 to 115 36 (00e93) 31 (00e221) 09 to 18
Post-bronchodilation
Rise in FEV1 () 65 (00e102) 25 (00e99) 03 to 63 54 (00e105) 31 (00e104) 00 to 32
FEV1 (z-score) 018 (079) 025 (105) 034 to 120 041 (081) 039 (115) 018 to 061
FEV1 FVC (z-score) 023 (083) 048 (106) 009 to 150 011 (090) 041 (095) 011 to 080
FEF25e75 (z-score) 029 (076) 048 (072) 011 to 143 019 (074) 037 (084) 011 to 069
Inflammatory markers
FeNO (ppb) 22 (6e84) 15 (7e51) 7 to 26 13 (6e54) 12 (5e74) 3 to 3
Blood eosinophils (3109 l) 033 (006e057) 016 (004e031) 001 to 027 016 (004e037) 014 ( 001e079) 002 to 006
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus RW recurrent wheeze
0
10
20
30
40
50
60
70
80
0
10
20
30
40
50
60
70
80
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
623665
828
8101
1000ltp
626
6601
8201
8101
1000ltp
0
10
20
30
40
50
60
70
80
90
100
4271691
4201
7131
3000=p
1000ltp
0
10
20
30
40
50
60
70
80
90
426
956
428
619
A B
C D
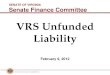
Figure 1 Proportion () with (A) current asthmarecurrent wheeze (B) current allergic rhinoconjunctivitis (C) current positive Phadiatop test and (D)
current positive skin prick test to perennial allergens in respiratory syncytial virus (RSV) and control cohorts with respect to heredity for asthma c2
test for trend was used in all graphs and error bars denote 95 CI
1048 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 59
but not with spirometry results (see table E5 in online supple-ment) Among the subjects with current asthmaRW regressionanalyses also demonstrated signi1047297cant relationships betweenLCI and the maximum percentage fall in FEV1 after dry airchallenge (r2
frac14026 pfrac140005) and between LCI and FeNO(r2
frac14029 pfrac140003)
Family history and other risk factors for asthma and ARC
at age 18 A family history of asthma and atopy did not differ between theRSV and control cohorts at age 18 A number of risk factors forcurrent asthmaRW current asthma and current ARC respec-tively were assessed using multivariate logistic regression anal-
yses including both cohorts For current asthmaRW and forcurrent asthma the risk factors included were allocation (RSVcontrol) gender domestic furred pets in the 1047297rst year of lifeparental smoking in the 1047297rst year of life own smoking at age 18current ARC of the subjects themselves physician-diagnosedparental ARC and physician-diagnosed parental asthma
For current asthmaRW only RSV (OR 62 95 CI 20 to192 plt0001) and current ARC of the subjects (OR 61 95 CI21 to 181 plt0001) were signi1047297cant independent risk factors
For current asthma alone similar results were found (RSV OR 72 (95 CI 21 to 239 plt0001) current ARC OR 44 (95 CI14 to 140 plt0001))
The risk factors included in the analysis for current ARC werethe same except for current ARC of the subjects Only RSV(OR 36 95 CI 16 to 85 pfrac140003) was a signi1047297cant inde-pendent risk factor Corresponding conditional logistic regres-sion tests gave similar results (see table E6 in the onlinesupplement)
Numerically the RSV subgroup with a parental history of asthma had a higher prevalence of asthmaRW ARC and positive
sensitisation than the RSV subgroup without parental asthmabut no signi1047297cant differences were found (pfrac140058e0308)The statistical power to detect signi1047297cant differences betweenthe RSV subgroups was lt50 For the two cohorts analysedtogether however the combination of RSV allocation andhistory of parental asthma resulted in signi1047297cant trends fordisease and sensitisation (1047297gure 1A eD)
Longitudinal data over the entire study period subjects with RSVversus controlsKaplaneMeier survival plots for time free from asthma diag-nosis ARC diagnosis positive Phadiatop test or positive SPTareshown in 1047297gure 2A eD The RSV group had signi1047297cantly shorter
time free from these diagnoses and test 1047297ndingsReduced lung function in the RSV cohort was evident from
the age of 7 years (mean (SD) baseline FEF 25e75 z-scores in RSV
0
20
40
60
80
100
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
RSV
Controls
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
A B
C D
Figure 2 Proportion () of subjects in the respiratory syncytial virus and control cohorts who never had (A) an asthma diagnosis at follow-up at ages3 7 13 and 18 years (log rank (Mantel-Cox) c2 210 df 1 plt0001) (B) an allergic rhinoconjunctivitis diagnosis at follow-up at ages 3 7 13 and
18 years (log rank (Mantel-Cox) c2
155 df 1 plt0001) (C) a positive Phadiatop test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox)c2 83 df 1 pfrac140004) and (D) a positive skin prick test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox) c2 80 df 1 pfrac140005)
Thorax 2010651045e1052 doi101136thx2009121582 1049
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 29
previous publications11e13 The speci1047297c IgE assay method used(ImmunoCAP) was consistent throughout the study period
Spirometry was performed at baseline from age 7 and post-
bronchodilator at ages 13 and 18 years according to AmericanThoracic Society recommendations17 and expressed as standarddeviation scores (z-scores) using recently published normativedata18 19 Inhaled long-acting b2 agonists were withheld for 24 hand short-acting b2 agonists or cromoglycates for 6 h prior totesting Inhaled corticosteroids (ICS) if used were not discon-tinued Isocapnic dry air hyperventilation challenge (DACh) wasperformed after baseline spirometry at age 13 and 18 years(described in more detail in the online supplement) At age 18prior to these lung function tests the fraction of nitric oxide inexpired air (FeNO) was measured in duplicate at an expiratory 1047298ow of 50 mls using the Niox Mino (Aerocrine StockholmSweden) and the mean FeNO result reported
Multiple-breath washout (MBW) was performed before
spirometry using sulfur hexa1047298uoride (SF6 ) as the marker gas and
a mass spectrometer for gas analysis and as previously describedin detail elsewhere20 Lung clearance index (LCI) was calculatedas the number of lung volume turnovers (ie the cumulative
expired volume divided by the functional residual capacity)needed to lower the end-tidal tracer gas concentration to 140thof the starting concentration A high value of LCI thus indicatesabnormal ventilation distribution The mean LCI result fromthree MBWs in each subject was reported In a previous study including healthy subjects the mean SD and upper limit of
Table 1 Study design and proportion of the 47 children in the RSV cohort and the 93 in the control cohort seen at follow-up during the study period
Age (years)
1 15 2 and 25 3 7 13 18
Total number (RSV controls) 47 93 47 93 47 93 47 93 46 92 46 92
of cohort (RSV and controls) 100 100 100 100 985 985
Questionnaire 3 3 3 3 3 3
Examination 3 3 3 (46 89) 3 (45 89) 3 (42 87)
Skin prick tests (RSV controls) 3 (47 92) 3 (45 92) 3 (44 89) 3 (42 87) 3 (41 85)
Egg white 3 3 3
Cat 3 3 3 3
Dog 3 3 3
Horse 3 3 3
Birch 3 3 3 3
Timothy 3 3 3
Mugworth 3 3
HDM ( D pteronyssinus) 3 3 3 3
HDM ( D farinae) 3 3
Mould (Cladosporium herbarum) 3 3 3
Mould ( Alternaria alternata) 3 3
Blood samples 3 3 (44 87) 3 (44 86) 3 (41 85)
IgE to food allergens (Fx5) 3 3
IgE to inhaled allergens (Phadiatop) 3 3 3 3 (41 85)
Blood eosinophil counts 3 (40 86)Lung function tests 3 (44 86) 3 (44 86) 3 (42 86)
Spirometry 3 3 3
Multiple breath washout (LCI) 3 (41 86)
FeNO 3 (42 86)
DACh 3 (43 86) 3 (41 86)
Numbers in parentheses (RSV controls) if differed from numbers followed up at that time pointA skin prick test weal with a mean diameter $3 mm was regarded positive Phadiatop (Pharmacia Upjohn Diagnostics AB Uppsala Sweden) is a screening test for antibodies to inhaledallergens Fx5 (Pharmacia Upjohn Diagnostics AB Uppsala Sweden) is a screening test for food allergensHDM house dust mite DACh dry air hyperventilation challenge LCI lung clearance index FeNO fractional exhaled nitric oxide RSV respiratory syncytial virus
Table 2 Demographic data and family history of the respiratorysyncytial virus (RSV) and control groups at age 18
Variable RSV (n[46) Controls (n[92)
Weight (kg) 65 (12) 70 (13)
Height (cm) 174 (10) 174 (10)
Parental atopy 3046 (65) 5292 (56)
Parental asthma 1846 (39) 2592 (27)
Tobacco smoke exposure
Active 1045 (22) 1492 (15)
Passive (family member) 1945 (42) 4092 (43)
Indoor furred pets 2446 (52) 5692 (61)
Mean (SD) or proportions (percentages) of subjects are given No significant differenceswere seen between the groups
Table 3 Wheeze patterns defined from the presenceabsence (+ ) ofasthmarecurrent wheeze at four follow-up stations and the numbers ofcases in each wheeze pattern group for each cohort
Wheeze pattern
Age (years)
RSV (n[46) Controls (n[92)3 7 13 18
Never wheeze 14 (3 11) 69 (27 42)
T ra nsient wheeze + 7 (5 2) 11 (8 3)
Remittingintermittent + 7 (4 3) 4 (2 2)
+
+ +
+ +
+ + +
Late onset + + 4 (1 3) 7 (3 4)
+
Persistentrelapsing + + + + 14 (7 7) 1 (1 0)
+ + +
+ + +
+ + +
+ +
Male female distribution shown in parenthesesStatistical evaluation refers to comparison of proportion of subjects in the different wheeze
pattern groups in the RSV and control cohorts plt0001RSV respiratory syncytial virus
1046 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 39
normality (ULN mean + 196 SD) for LCI were 633 043 and717 respectively20
At each follow-up time point asthma was de1047297ned as $3episodes of physician-veri1047297ed wheeze and RW as $3 episodes of parent-reported wheeze De1047297nitions of the wheezing patternsover time are shown in table 3 Allergic rhinoconjunctivitis(ARC) or clinical allergy was de1047297ned as rhinitisconjunctivitisoccurring at least twice following exposure to a particular
allergen and unrelated to infection Atopic dermatitis (AD) wasde1047297ned as a pruritic chronic or chronically relapsing non-infec-tious dermatitis Allergic sensitisation implied occurrence of IgEantibodies estimated by SPT andor serum IgE tests Currentdisorder denotes symptoms over the last 12 months Active andpassive smoke exposures the presence of pets in the householdand atopic or allergic heredity were assessed by questionnaire A positive history of atopic disease (AD ARC or asthma) in 1047297rst-degree relatives (parents or siblings) was based on physiciandiagnosis
Statistical analyses Yatesrsquo corrected c2 test was used for estimation of differences in
prevalence among groups and subgroups One-way ANOVA wasused for parametric continuous variables and Tukey HSD forsubsequent group comparisons if the overall F-test was signi1047297-cant A Manne Whitney test was used to test group differencesfor non-parametric continuous variables 95 CIs for mean andmedian differences were calculated c2 tests for trend were usedto assess the combined in1047298uence of group allocation (RSV vscontrol) and a parental history of physician-diagnosed asthmaon asthmaRW ARC and sensitisation at age 18 Pearsoncorrelation tests were used to assess correlation of parametricdata while the Spearman rank test was used for non-parametricdata KaplaneMeier survival analysis was used to compare timefree from diagnosis of asthma ARC positive Phadiatop test orpositive SPT to any perennial allergen at a follow-up station p
values based on Mantel-Cox log ranks were calculated Multi-variate logistic regression analyses were performed to establishrisk factors for asthmaRW asthma alone and ARC at age 18ORs with 95 CI and p values were reported Additionallyconditional logistic regression tests were performed to adjust forany degree of residual confounding due to the constitution of
the groups during the study period SPSS Version 150 softwarefor Windows (SPSS Inc Chicago Illinois USA) SPSS Sample-Power 20 software and CI Analysis software version 212(Trevor Bryant University of Southampton) were used for thestatistical analyses
RESULTSForty-six of the 47 subjects with RSV and 92 of the 93 controls
were followed up to 18 years of age The demographic details of the two cohorts at age 18 are summarised in table 2 and fromage 1e18 years in table E1 in the online supplement Nosigni1047297cant differences were seen at age 18
Cross-sectional data at age 18Current asthmaRW was documented in 18 of 46 (39) subjectswith RSV and 8 of 92 (9) controls (pfrac140001) Current asthmaalone was found in 15 of 46 (33) subjects with RSVand 6 of 92(7) controls (plt0001) ARC was diagnosed in 20 of 46 subjects with RSV (43) and 16 of 92 (17) controls (pfrac140002)No difference was found in the prevalence of AD (5 of 46 (11)subjects with RSV vs 8 of 92 (9) controls)
The prevalence of sensitisation determined by SPT wassigni1047297cantly increased in the RSV cohort compared withcontrols to any animal dander (cat dog horse) (33 vs 11pfrac140005) or any perennial (animal danders and house dust mites(HDM)) (41 vs 14 pfrac140001) (see table E2 in onlinesupplement) A higher prevalence of positive Phadiatopresponses was seen in the RSV cohort (56 vs 28 p frac140005)(see table E2 in online supplement) For the whole cohort themost commonly identi1047297ed speci1047297c IgE antibodies performed inthose testing positive to Phadiatop screening were to lsquoany perennialrsquo (39 of 126 31) and were signi1047297cantly increased insubjects with RSV compared with controls (51 vs 21pfrac140001)
Airway function data are summarised in table 4 Reduced
spirometric airway function (forced expiratory volume in 1 s(FEV1) ratio of FEV1 to forced vital capacity (FVC) and forcedexpiratory 1047298ow at 25e75 FVC (FEF25e75)) was documented inthe RSV cohort compared with controls but LCI did not differ
AHR bronchodilator response and blood eosinophil cell countswere greater in the RSV cohort than in the controls but FeNO
Table 4 Airway function and inflammatory markers in RSV and control groups at age 18 years
RSV (n[46) Control (n[92) 95 CI for difference
Resting
FEV1 (z-score) 028 (093) 011 (108) 000 to 07
FEV1 FVC (z-score) 068 (085) 008 (103) 024 to 097
FEF25e75 (z-score) 060 (077) 005 (085) 025 to 086
LCI 663 (052) 659 (043) 021 to 013Challenge (DACh)
Fall in FEV1 () 47 (00e378) 31 (00e428) 00 to 32
Post-bronchodilation
Rise in FEV1 () 59 (00e105) 31 (00e104) 05 to 34
FEV1 (z-score) 016 (071) 038 (130) -018 to 061
FEV1 FVC (z-score) 004 (088) 042 (095) 011 to 080
FEF25e75 (z-score) 001 (078) 038 (083) 009 to 069
Inflammatory markers
FeNO (ppb) 14 (6e84) 13 (5e74) 1 to 5
Blood eosinophil counts (3109 l) 020 (004e057) 014 (001e079) 001 to 010
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001For exact number of subjects in RSV and control group performing each test see Table 1
DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25
e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in
1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus
Thorax 2010651045e1052 doi101136thx2009121582 1047
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 49
was not FEV1 FVC and FEF25-75 remained lower in the RSVcohort after bronchodilation Subjects with RSV had lowerspirometry results than the controls irrespective of currentasthmaRW diagnosis (table 5) Spirometry 1047297ndings were similarin controls with or without current asthmaRW LCI wassigni1047297cantly raised in subjects with RSV (pfrac140006) and controls(pfrac140033) with current asthmaRW compared with corre-
sponding subjects without asthma (see table E3 in onlinesupplement) Only LCI differed signi1047297cantly between thecontrols with and those without current asthmaRW (see tableE4 in online supplement) In the RSV cohort the maximumpercentage fall in FEV1 after dry air challenge correlated signi1047297-cantly with LCI (r2
frac14044 plt0001) FeNO levels (r2frac14026
plt0001) and with blood eosinophil counts (r2frac14012 pfrac140011)
Table 5 Airway function and inflammatory markers in RSV versus control subjects with or without current asthmaRW at age 18 years
Current asthmaRW No current asthmaRW
RSV (n[18) Controls (n[8) 95 CI for difference RS V (n[24) Controls (n[78) 95 CI for difference
Resting
FEV1 (z-score) 064 (085) 005 (077) 003 to 142 000 (091) 011 (111) 000 to 077
FEV1 FVC (z-score) 089 (082) 008 (137) 009 to 186 053 (086) 010 (100) 024 to 097
FEF25e75 (z-score) 089 (071) 006 (086) 017 to 1 50 038 (075) 005 ( 0 85) 025 to 086
LCI 688 (063) 689 (025) 046 to 049 644 (031) 656 (043) 021 to 129
Challenge (DACh)
Fall in FEV1 () 85 (00e378) 75 (03e428) 55 to 115 36 (00e93) 31 (00e221) 09 to 18
Post-bronchodilation
Rise in FEV1 () 65 (00e102) 25 (00e99) 03 to 63 54 (00e105) 31 (00e104) 00 to 32
FEV1 (z-score) 018 (079) 025 (105) 034 to 120 041 (081) 039 (115) 018 to 061
FEV1 FVC (z-score) 023 (083) 048 (106) 009 to 150 011 (090) 041 (095) 011 to 080
FEF25e75 (z-score) 029 (076) 048 (072) 011 to 143 019 (074) 037 (084) 011 to 069
Inflammatory markers
FeNO (ppb) 22 (6e84) 15 (7e51) 7 to 26 13 (6e54) 12 (5e74) 3 to 3
Blood eosinophils (3109 l) 033 (006e057) 016 (004e031) 001 to 027 016 (004e037) 014 ( 001e079) 002 to 006
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus RW recurrent wheeze
0
10
20
30
40
50
60
70
80
0
10
20
30
40
50
60
70
80
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
623665
828
8101
1000ltp
626
6601
8201
8101
1000ltp
0
10
20
30
40
50
60
70
80
90
100
4271691
4201
7131
3000=p
1000ltp
0
10
20
30
40
50
60
70
80
90
426
956
428
619
A B
C D
Figure 1 Proportion () with (A) current asthmarecurrent wheeze (B) current allergic rhinoconjunctivitis (C) current positive Phadiatop test and (D)
current positive skin prick test to perennial allergens in respiratory syncytial virus (RSV) and control cohorts with respect to heredity for asthma c2
test for trend was used in all graphs and error bars denote 95 CI
1048 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 59
but not with spirometry results (see table E5 in online supple-ment) Among the subjects with current asthmaRW regressionanalyses also demonstrated signi1047297cant relationships betweenLCI and the maximum percentage fall in FEV1 after dry airchallenge (r2
frac14026 pfrac140005) and between LCI and FeNO(r2
frac14029 pfrac140003)
Family history and other risk factors for asthma and ARC
at age 18 A family history of asthma and atopy did not differ between theRSV and control cohorts at age 18 A number of risk factors forcurrent asthmaRW current asthma and current ARC respec-tively were assessed using multivariate logistic regression anal-
yses including both cohorts For current asthmaRW and forcurrent asthma the risk factors included were allocation (RSVcontrol) gender domestic furred pets in the 1047297rst year of lifeparental smoking in the 1047297rst year of life own smoking at age 18current ARC of the subjects themselves physician-diagnosedparental ARC and physician-diagnosed parental asthma
For current asthmaRW only RSV (OR 62 95 CI 20 to192 plt0001) and current ARC of the subjects (OR 61 95 CI21 to 181 plt0001) were signi1047297cant independent risk factors
For current asthma alone similar results were found (RSV OR 72 (95 CI 21 to 239 plt0001) current ARC OR 44 (95 CI14 to 140 plt0001))
The risk factors included in the analysis for current ARC werethe same except for current ARC of the subjects Only RSV(OR 36 95 CI 16 to 85 pfrac140003) was a signi1047297cant inde-pendent risk factor Corresponding conditional logistic regres-sion tests gave similar results (see table E6 in the onlinesupplement)
Numerically the RSV subgroup with a parental history of asthma had a higher prevalence of asthmaRW ARC and positive
sensitisation than the RSV subgroup without parental asthmabut no signi1047297cant differences were found (pfrac140058e0308)The statistical power to detect signi1047297cant differences betweenthe RSV subgroups was lt50 For the two cohorts analysedtogether however the combination of RSV allocation andhistory of parental asthma resulted in signi1047297cant trends fordisease and sensitisation (1047297gure 1A eD)
Longitudinal data over the entire study period subjects with RSVversus controlsKaplaneMeier survival plots for time free from asthma diag-nosis ARC diagnosis positive Phadiatop test or positive SPTareshown in 1047297gure 2A eD The RSV group had signi1047297cantly shorter
time free from these diagnoses and test 1047297ndingsReduced lung function in the RSV cohort was evident from
the age of 7 years (mean (SD) baseline FEF 25e75 z-scores in RSV
0
20
40
60
80
100
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
RSV
Controls
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
A B
C D
Figure 2 Proportion () of subjects in the respiratory syncytial virus and control cohorts who never had (A) an asthma diagnosis at follow-up at ages3 7 13 and 18 years (log rank (Mantel-Cox) c2 210 df 1 plt0001) (B) an allergic rhinoconjunctivitis diagnosis at follow-up at ages 3 7 13 and
18 years (log rank (Mantel-Cox) c2
155 df 1 plt0001) (C) a positive Phadiatop test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox)c2 83 df 1 pfrac140004) and (D) a positive skin prick test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox) c2 80 df 1 pfrac140005)
Thorax 2010651045e1052 doi101136thx2009121582 1049
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 39
normality (ULN mean + 196 SD) for LCI were 633 043 and717 respectively20
At each follow-up time point asthma was de1047297ned as $3episodes of physician-veri1047297ed wheeze and RW as $3 episodes of parent-reported wheeze De1047297nitions of the wheezing patternsover time are shown in table 3 Allergic rhinoconjunctivitis(ARC) or clinical allergy was de1047297ned as rhinitisconjunctivitisoccurring at least twice following exposure to a particular
allergen and unrelated to infection Atopic dermatitis (AD) wasde1047297ned as a pruritic chronic or chronically relapsing non-infec-tious dermatitis Allergic sensitisation implied occurrence of IgEantibodies estimated by SPT andor serum IgE tests Currentdisorder denotes symptoms over the last 12 months Active andpassive smoke exposures the presence of pets in the householdand atopic or allergic heredity were assessed by questionnaire A positive history of atopic disease (AD ARC or asthma) in 1047297rst-degree relatives (parents or siblings) was based on physiciandiagnosis
Statistical analyses Yatesrsquo corrected c2 test was used for estimation of differences in
prevalence among groups and subgroups One-way ANOVA wasused for parametric continuous variables and Tukey HSD forsubsequent group comparisons if the overall F-test was signi1047297-cant A Manne Whitney test was used to test group differencesfor non-parametric continuous variables 95 CIs for mean andmedian differences were calculated c2 tests for trend were usedto assess the combined in1047298uence of group allocation (RSV vscontrol) and a parental history of physician-diagnosed asthmaon asthmaRW ARC and sensitisation at age 18 Pearsoncorrelation tests were used to assess correlation of parametricdata while the Spearman rank test was used for non-parametricdata KaplaneMeier survival analysis was used to compare timefree from diagnosis of asthma ARC positive Phadiatop test orpositive SPT to any perennial allergen at a follow-up station p
values based on Mantel-Cox log ranks were calculated Multi-variate logistic regression analyses were performed to establishrisk factors for asthmaRW asthma alone and ARC at age 18ORs with 95 CI and p values were reported Additionallyconditional logistic regression tests were performed to adjust forany degree of residual confounding due to the constitution of
the groups during the study period SPSS Version 150 softwarefor Windows (SPSS Inc Chicago Illinois USA) SPSS Sample-Power 20 software and CI Analysis software version 212(Trevor Bryant University of Southampton) were used for thestatistical analyses
RESULTSForty-six of the 47 subjects with RSV and 92 of the 93 controls
were followed up to 18 years of age The demographic details of the two cohorts at age 18 are summarised in table 2 and fromage 1e18 years in table E1 in the online supplement Nosigni1047297cant differences were seen at age 18
Cross-sectional data at age 18Current asthmaRW was documented in 18 of 46 (39) subjectswith RSV and 8 of 92 (9) controls (pfrac140001) Current asthmaalone was found in 15 of 46 (33) subjects with RSVand 6 of 92(7) controls (plt0001) ARC was diagnosed in 20 of 46 subjects with RSV (43) and 16 of 92 (17) controls (pfrac140002)No difference was found in the prevalence of AD (5 of 46 (11)subjects with RSV vs 8 of 92 (9) controls)
The prevalence of sensitisation determined by SPT wassigni1047297cantly increased in the RSV cohort compared withcontrols to any animal dander (cat dog horse) (33 vs 11pfrac140005) or any perennial (animal danders and house dust mites(HDM)) (41 vs 14 pfrac140001) (see table E2 in onlinesupplement) A higher prevalence of positive Phadiatopresponses was seen in the RSV cohort (56 vs 28 p frac140005)(see table E2 in online supplement) For the whole cohort themost commonly identi1047297ed speci1047297c IgE antibodies performed inthose testing positive to Phadiatop screening were to lsquoany perennialrsquo (39 of 126 31) and were signi1047297cantly increased insubjects with RSV compared with controls (51 vs 21pfrac140001)
Airway function data are summarised in table 4 Reduced
spirometric airway function (forced expiratory volume in 1 s(FEV1) ratio of FEV1 to forced vital capacity (FVC) and forcedexpiratory 1047298ow at 25e75 FVC (FEF25e75)) was documented inthe RSV cohort compared with controls but LCI did not differ
AHR bronchodilator response and blood eosinophil cell countswere greater in the RSV cohort than in the controls but FeNO
Table 4 Airway function and inflammatory markers in RSV and control groups at age 18 years
RSV (n[46) Control (n[92) 95 CI for difference
Resting
FEV1 (z-score) 028 (093) 011 (108) 000 to 07
FEV1 FVC (z-score) 068 (085) 008 (103) 024 to 097
FEF25e75 (z-score) 060 (077) 005 (085) 025 to 086
LCI 663 (052) 659 (043) 021 to 013Challenge (DACh)
Fall in FEV1 () 47 (00e378) 31 (00e428) 00 to 32
Post-bronchodilation
Rise in FEV1 () 59 (00e105) 31 (00e104) 05 to 34
FEV1 (z-score) 016 (071) 038 (130) -018 to 061
FEV1 FVC (z-score) 004 (088) 042 (095) 011 to 080
FEF25e75 (z-score) 001 (078) 038 (083) 009 to 069
Inflammatory markers
FeNO (ppb) 14 (6e84) 13 (5e74) 1 to 5
Blood eosinophil counts (3109 l) 020 (004e057) 014 (001e079) 001 to 010
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001For exact number of subjects in RSV and control group performing each test see Table 1
DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25
e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in
1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus
Thorax 2010651045e1052 doi101136thx2009121582 1047
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 49
was not FEV1 FVC and FEF25-75 remained lower in the RSVcohort after bronchodilation Subjects with RSV had lowerspirometry results than the controls irrespective of currentasthmaRW diagnosis (table 5) Spirometry 1047297ndings were similarin controls with or without current asthmaRW LCI wassigni1047297cantly raised in subjects with RSV (pfrac140006) and controls(pfrac140033) with current asthmaRW compared with corre-
sponding subjects without asthma (see table E3 in onlinesupplement) Only LCI differed signi1047297cantly between thecontrols with and those without current asthmaRW (see tableE4 in online supplement) In the RSV cohort the maximumpercentage fall in FEV1 after dry air challenge correlated signi1047297-cantly with LCI (r2
frac14044 plt0001) FeNO levels (r2frac14026
plt0001) and with blood eosinophil counts (r2frac14012 pfrac140011)
Table 5 Airway function and inflammatory markers in RSV versus control subjects with or without current asthmaRW at age 18 years
Current asthmaRW No current asthmaRW
RSV (n[18) Controls (n[8) 95 CI for difference RS V (n[24) Controls (n[78) 95 CI for difference
Resting
FEV1 (z-score) 064 (085) 005 (077) 003 to 142 000 (091) 011 (111) 000 to 077
FEV1 FVC (z-score) 089 (082) 008 (137) 009 to 186 053 (086) 010 (100) 024 to 097
FEF25e75 (z-score) 089 (071) 006 (086) 017 to 1 50 038 (075) 005 ( 0 85) 025 to 086
LCI 688 (063) 689 (025) 046 to 049 644 (031) 656 (043) 021 to 129
Challenge (DACh)
Fall in FEV1 () 85 (00e378) 75 (03e428) 55 to 115 36 (00e93) 31 (00e221) 09 to 18
Post-bronchodilation
Rise in FEV1 () 65 (00e102) 25 (00e99) 03 to 63 54 (00e105) 31 (00e104) 00 to 32
FEV1 (z-score) 018 (079) 025 (105) 034 to 120 041 (081) 039 (115) 018 to 061
FEV1 FVC (z-score) 023 (083) 048 (106) 009 to 150 011 (090) 041 (095) 011 to 080
FEF25e75 (z-score) 029 (076) 048 (072) 011 to 143 019 (074) 037 (084) 011 to 069
Inflammatory markers
FeNO (ppb) 22 (6e84) 15 (7e51) 7 to 26 13 (6e54) 12 (5e74) 3 to 3
Blood eosinophils (3109 l) 033 (006e057) 016 (004e031) 001 to 027 016 (004e037) 014 ( 001e079) 002 to 006
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus RW recurrent wheeze
0
10
20
30
40
50
60
70
80
0
10
20
30
40
50
60
70
80
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
623665
828
8101
1000ltp
626
6601
8201
8101
1000ltp
0
10
20
30
40
50
60
70
80
90
100
4271691
4201
7131
3000=p
1000ltp
0
10
20
30
40
50
60
70
80
90
426
956
428
619
A B
C D
Figure 1 Proportion () with (A) current asthmarecurrent wheeze (B) current allergic rhinoconjunctivitis (C) current positive Phadiatop test and (D)
current positive skin prick test to perennial allergens in respiratory syncytial virus (RSV) and control cohorts with respect to heredity for asthma c2
test for trend was used in all graphs and error bars denote 95 CI
1048 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 59
but not with spirometry results (see table E5 in online supple-ment) Among the subjects with current asthmaRW regressionanalyses also demonstrated signi1047297cant relationships betweenLCI and the maximum percentage fall in FEV1 after dry airchallenge (r2
frac14026 pfrac140005) and between LCI and FeNO(r2
frac14029 pfrac140003)
Family history and other risk factors for asthma and ARC
at age 18 A family history of asthma and atopy did not differ between theRSV and control cohorts at age 18 A number of risk factors forcurrent asthmaRW current asthma and current ARC respec-tively were assessed using multivariate logistic regression anal-
yses including both cohorts For current asthmaRW and forcurrent asthma the risk factors included were allocation (RSVcontrol) gender domestic furred pets in the 1047297rst year of lifeparental smoking in the 1047297rst year of life own smoking at age 18current ARC of the subjects themselves physician-diagnosedparental ARC and physician-diagnosed parental asthma
For current asthmaRW only RSV (OR 62 95 CI 20 to192 plt0001) and current ARC of the subjects (OR 61 95 CI21 to 181 plt0001) were signi1047297cant independent risk factors
For current asthma alone similar results were found (RSV OR 72 (95 CI 21 to 239 plt0001) current ARC OR 44 (95 CI14 to 140 plt0001))
The risk factors included in the analysis for current ARC werethe same except for current ARC of the subjects Only RSV(OR 36 95 CI 16 to 85 pfrac140003) was a signi1047297cant inde-pendent risk factor Corresponding conditional logistic regres-sion tests gave similar results (see table E6 in the onlinesupplement)
Numerically the RSV subgroup with a parental history of asthma had a higher prevalence of asthmaRW ARC and positive
sensitisation than the RSV subgroup without parental asthmabut no signi1047297cant differences were found (pfrac140058e0308)The statistical power to detect signi1047297cant differences betweenthe RSV subgroups was lt50 For the two cohorts analysedtogether however the combination of RSV allocation andhistory of parental asthma resulted in signi1047297cant trends fordisease and sensitisation (1047297gure 1A eD)
Longitudinal data over the entire study period subjects with RSVversus controlsKaplaneMeier survival plots for time free from asthma diag-nosis ARC diagnosis positive Phadiatop test or positive SPTareshown in 1047297gure 2A eD The RSV group had signi1047297cantly shorter
time free from these diagnoses and test 1047297ndingsReduced lung function in the RSV cohort was evident from
the age of 7 years (mean (SD) baseline FEF 25e75 z-scores in RSV
0
20
40
60
80
100
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
RSV
Controls
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
A B
C D
Figure 2 Proportion () of subjects in the respiratory syncytial virus and control cohorts who never had (A) an asthma diagnosis at follow-up at ages3 7 13 and 18 years (log rank (Mantel-Cox) c2 210 df 1 plt0001) (B) an allergic rhinoconjunctivitis diagnosis at follow-up at ages 3 7 13 and
18 years (log rank (Mantel-Cox) c2
155 df 1 plt0001) (C) a positive Phadiatop test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox)c2 83 df 1 pfrac140004) and (D) a positive skin prick test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox) c2 80 df 1 pfrac140005)
Thorax 2010651045e1052 doi101136thx2009121582 1049
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 49
was not FEV1 FVC and FEF25-75 remained lower in the RSVcohort after bronchodilation Subjects with RSV had lowerspirometry results than the controls irrespective of currentasthmaRW diagnosis (table 5) Spirometry 1047297ndings were similarin controls with or without current asthmaRW LCI wassigni1047297cantly raised in subjects with RSV (pfrac140006) and controls(pfrac140033) with current asthmaRW compared with corre-
sponding subjects without asthma (see table E3 in onlinesupplement) Only LCI differed signi1047297cantly between thecontrols with and those without current asthmaRW (see tableE4 in online supplement) In the RSV cohort the maximumpercentage fall in FEV1 after dry air challenge correlated signi1047297-cantly with LCI (r2
frac14044 plt0001) FeNO levels (r2frac14026
plt0001) and with blood eosinophil counts (r2frac14012 pfrac140011)
Table 5 Airway function and inflammatory markers in RSV versus control subjects with or without current asthmaRW at age 18 years
Current asthmaRW No current asthmaRW
RSV (n[18) Controls (n[8) 95 CI for difference RS V (n[24) Controls (n[78) 95 CI for difference
Resting
FEV1 (z-score) 064 (085) 005 (077) 003 to 142 000 (091) 011 (111) 000 to 077
FEV1 FVC (z-score) 089 (082) 008 (137) 009 to 186 053 (086) 010 (100) 024 to 097
FEF25e75 (z-score) 089 (071) 006 (086) 017 to 1 50 038 (075) 005 ( 0 85) 025 to 086
LCI 688 (063) 689 (025) 046 to 049 644 (031) 656 (043) 021 to 129
Challenge (DACh)
Fall in FEV1 () 85 (00e378) 75 (03e428) 55 to 115 36 (00e93) 31 (00e221) 09 to 18
Post-bronchodilation
Rise in FEV1 () 65 (00e102) 25 (00e99) 03 to 63 54 (00e105) 31 (00e104) 00 to 32
FEV1 (z-score) 018 (079) 025 (105) 034 to 120 041 (081) 039 (115) 018 to 061
FEV1 FVC (z-score) 023 (083) 048 (106) 009 to 150 011 (090) 041 (095) 011 to 080
FEF25e75 (z-score) 029 (076) 048 (072) 011 to 143 019 (074) 037 (084) 011 to 069
Inflammatory markers
FeNO (ppb) 22 (6e84) 15 (7e51) 7 to 26 13 (6e54) 12 (5e74) 3 to 3
Blood eosinophils (3109 l) 033 (006e057) 016 (004e031) 001 to 027 016 (004e037) 014 ( 001e079) 002 to 006
Data are shown as mean (SD) or median (range)For normally distributed data differences between the two groups are shown with 95 CI for the mean values and for non-normally distributed data as the 95 CI for the mediansplt005 plt001 plt0001DACh isocapnic dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in1 s FVC forced vital capacity LCI lung clearance index ppb parts per billion RSV respiratory syncytial virus RW recurrent wheeze
0
10
20
30
40
50
60
70
80
0
10
20
30
40
50
60
70
80
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes Any parent with asthma
RSV bronchiolitis
No Yes YesNo
No YesNo Yes
623665
828
8101
1000ltp
626
6601
8201
8101
1000ltp
0
10
20
30
40
50
60
70
80
90
100
4271691
4201
7131
3000=p
1000ltp
0
10
20
30
40
50
60
70
80
90
426
956
428
619
A B
C D
Figure 1 Proportion () with (A) current asthmarecurrent wheeze (B) current allergic rhinoconjunctivitis (C) current positive Phadiatop test and (D)
current positive skin prick test to perennial allergens in respiratory syncytial virus (RSV) and control cohorts with respect to heredity for asthma c2
test for trend was used in all graphs and error bars denote 95 CI
1048 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 59
but not with spirometry results (see table E5 in online supple-ment) Among the subjects with current asthmaRW regressionanalyses also demonstrated signi1047297cant relationships betweenLCI and the maximum percentage fall in FEV1 after dry airchallenge (r2
frac14026 pfrac140005) and between LCI and FeNO(r2
frac14029 pfrac140003)
Family history and other risk factors for asthma and ARC
at age 18 A family history of asthma and atopy did not differ between theRSV and control cohorts at age 18 A number of risk factors forcurrent asthmaRW current asthma and current ARC respec-tively were assessed using multivariate logistic regression anal-
yses including both cohorts For current asthmaRW and forcurrent asthma the risk factors included were allocation (RSVcontrol) gender domestic furred pets in the 1047297rst year of lifeparental smoking in the 1047297rst year of life own smoking at age 18current ARC of the subjects themselves physician-diagnosedparental ARC and physician-diagnosed parental asthma
For current asthmaRW only RSV (OR 62 95 CI 20 to192 plt0001) and current ARC of the subjects (OR 61 95 CI21 to 181 plt0001) were signi1047297cant independent risk factors
For current asthma alone similar results were found (RSV OR 72 (95 CI 21 to 239 plt0001) current ARC OR 44 (95 CI14 to 140 plt0001))
The risk factors included in the analysis for current ARC werethe same except for current ARC of the subjects Only RSV(OR 36 95 CI 16 to 85 pfrac140003) was a signi1047297cant inde-pendent risk factor Corresponding conditional logistic regres-sion tests gave similar results (see table E6 in the onlinesupplement)
Numerically the RSV subgroup with a parental history of asthma had a higher prevalence of asthmaRW ARC and positive
sensitisation than the RSV subgroup without parental asthmabut no signi1047297cant differences were found (pfrac140058e0308)The statistical power to detect signi1047297cant differences betweenthe RSV subgroups was lt50 For the two cohorts analysedtogether however the combination of RSV allocation andhistory of parental asthma resulted in signi1047297cant trends fordisease and sensitisation (1047297gure 1A eD)
Longitudinal data over the entire study period subjects with RSVversus controlsKaplaneMeier survival plots for time free from asthma diag-nosis ARC diagnosis positive Phadiatop test or positive SPTareshown in 1047297gure 2A eD The RSV group had signi1047297cantly shorter
time free from these diagnoses and test 1047297ndingsReduced lung function in the RSV cohort was evident from
the age of 7 years (mean (SD) baseline FEF 25e75 z-scores in RSV
0
20
40
60
80
100
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
RSV
Controls
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
A B
C D
Figure 2 Proportion () of subjects in the respiratory syncytial virus and control cohorts who never had (A) an asthma diagnosis at follow-up at ages3 7 13 and 18 years (log rank (Mantel-Cox) c2 210 df 1 plt0001) (B) an allergic rhinoconjunctivitis diagnosis at follow-up at ages 3 7 13 and
18 years (log rank (Mantel-Cox) c2
155 df 1 plt0001) (C) a positive Phadiatop test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox)c2 83 df 1 pfrac140004) and (D) a positive skin prick test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox) c2 80 df 1 pfrac140005)
Thorax 2010651045e1052 doi101136thx2009121582 1049
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 59
but not with spirometry results (see table E5 in online supple-ment) Among the subjects with current asthmaRW regressionanalyses also demonstrated signi1047297cant relationships betweenLCI and the maximum percentage fall in FEV1 after dry airchallenge (r2
frac14026 pfrac140005) and between LCI and FeNO(r2
frac14029 pfrac140003)
Family history and other risk factors for asthma and ARC
at age 18 A family history of asthma and atopy did not differ between theRSV and control cohorts at age 18 A number of risk factors forcurrent asthmaRW current asthma and current ARC respec-tively were assessed using multivariate logistic regression anal-
yses including both cohorts For current asthmaRW and forcurrent asthma the risk factors included were allocation (RSVcontrol) gender domestic furred pets in the 1047297rst year of lifeparental smoking in the 1047297rst year of life own smoking at age 18current ARC of the subjects themselves physician-diagnosedparental ARC and physician-diagnosed parental asthma
For current asthmaRW only RSV (OR 62 95 CI 20 to192 plt0001) and current ARC of the subjects (OR 61 95 CI21 to 181 plt0001) were signi1047297cant independent risk factors
For current asthma alone similar results were found (RSV OR 72 (95 CI 21 to 239 plt0001) current ARC OR 44 (95 CI14 to 140 plt0001))
The risk factors included in the analysis for current ARC werethe same except for current ARC of the subjects Only RSV(OR 36 95 CI 16 to 85 pfrac140003) was a signi1047297cant inde-pendent risk factor Corresponding conditional logistic regres-sion tests gave similar results (see table E6 in the onlinesupplement)
Numerically the RSV subgroup with a parental history of asthma had a higher prevalence of asthmaRW ARC and positive
sensitisation than the RSV subgroup without parental asthmabut no signi1047297cant differences were found (pfrac140058e0308)The statistical power to detect signi1047297cant differences betweenthe RSV subgroups was lt50 For the two cohorts analysedtogether however the combination of RSV allocation andhistory of parental asthma resulted in signi1047297cant trends fordisease and sensitisation (1047297gure 1A eD)
Longitudinal data over the entire study period subjects with RSVversus controlsKaplaneMeier survival plots for time free from asthma diag-nosis ARC diagnosis positive Phadiatop test or positive SPTareshown in 1047297gure 2A eD The RSV group had signi1047297cantly shorter
time free from these diagnoses and test 1047297ndingsReduced lung function in the RSV cohort was evident from
the age of 7 years (mean (SD) baseline FEF 25e75 z-scores in RSV
0
20
40
60
80
100
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
181373
Age at follow-up visit (years)
RSV
Controls
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
A B
C D
Figure 2 Proportion () of subjects in the respiratory syncytial virus and control cohorts who never had (A) an asthma diagnosis at follow-up at ages3 7 13 and 18 years (log rank (Mantel-Cox) c2 210 df 1 plt0001) (B) an allergic rhinoconjunctivitis diagnosis at follow-up at ages 3 7 13 and
18 years (log rank (Mantel-Cox) c2
155 df 1 plt0001) (C) a positive Phadiatop test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox)c2 83 df 1 pfrac140004) and (D) a positive skin prick test at follow-up at ages 3 7 13 and 18 years (log rank (Mantel-Cox) c2 80 df 1 pfrac140005)
Thorax 2010651045e1052 doi101136thx2009121582 1049
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 69
group vs controls at age 7 063 (104) vs 022 (095) (95 CI005 to 077 pfrac140025) at age 13 058 (077) vs 012 (078)(95 CI 017 to 074 pfrac140002) At ages 13 and 18 a greater fallin FEV1 after DACh was seen in subjects with RSV13
Wheeze patterns up to age 18 yearsThe persistentrelapsing asthmaRW pattern occurred morefrequently in the RSV cohort with fewer non-wheezers in the
RSV group (table 3) No difference in other wheeze patterns wasseen All 14 individuals with a persistentrelapsing asthmaRW pattern in the RSV cohort had current symptoms on at leasttwo time points (seven on all four and six on three occasions)
AsthmaRW was noted from age 3 in 11 of 14 subjects in thisgroup The one individual in the control group with persistentrelapsing asthma had symptoms at all occasions from age 7Nine subjects with RSV (7 with persistentrelapsing asthmaRW and 2 with late onset asthmaRW) and 3 control subjectswith late-onset asthmaRW were treated with ICS (p frac140002)The persistentrelapsing group (14 RSV and 1 control) wascharacterised by the highest prevalence of co-existing ARC(1047297gure 3A) and sensitisation (1047297gure 3B) The signi1047297cantly higherprevalence of sensitisation was evident at ages 3 7 and 13 andsimilarly for ARC at age 7 and 13 (data not shown)
At 18 years of age the persistentrelapsing wheeze group hadsigni1047297cantly lower airway function (FEV1 FEV1 FVC andFEF25e75 z-scores) higher LCI and AHR than the non-wheezegroup (table 6) Bronchodilator response FeNO and blood eosin-ophil counts were signi1047297cantly increased compared with neverwheezers only in the persistentrelapsing asthmaRW group
DISCUSSIONThe previously reported over-representation of asthma (andasthmaRW) clinical allergy and allergic sensitisation in thisRSV cohort persisted into early adulthood The high prevalenceof current asthmaRW in the RSV cohort was due to a high
proportion of subjects with early-onset allergy-associatedwheezing persisting through childhood and adolescence andwas accompanied by reduced airway function elevated FeNOand eosinophil counts A history of hospitalisation for RSVbronchiolitis was the only signi1047297cant risk factor identi1047297ed at age18 for current asthmaRW asthma alone or ARC
At age 18 spirometry results were reduced in subjects withRSV with or without current asthmaRW compared withcorresponding controls but subjects with RSV without currentasthma did not show evidence of small airway dysfunction asmeasured by LCI Spirometry results showed no relationshipwith AHR or markers of allergic in1047298ammation In contrastsmall airway dysfunction (LCI) correlated with current asthma
AHR and FeNO a marker of ongoing allergic airway in1047298am-
mationThis controlled follow-up study and its 1047297ndings are unique It
describes the development of asthma and allergy prospectively after severe primary RSV bronchiolitis in the 1047297rst year life andhas involved several follow-up time points from infancy to
young adulthood all with very high attendance rates Thesubsequent high frequency of early-onset allergic asthmapersisting to age 18 has not previously been reported Only twoother prospective studies of RSV have documented a highprevalence of early sensitisation comparable to ours at 1 year21
and 3 years of age22
The debate between a causal or genetic predisposition rela-tionship between RSV and asthma has continued for decades
and cannot be answered by this study Two recent large registry-based studies have attempted to answer this question with each
declaring opposite conclusions23 24 The weaknesses in the study designs and the dif 1047297culties in answering this question have beenhighlighted in a recent editorial25 RSV-positive infants withwheezing may include both those with primary RSV LRTI orthose with an existing non-atopic or atopic wheezing disorderexacerbated by RSV In our cohort 91 of the index subjectswere 6 months or younger when admitted and only one hada previous history of lower airway symptoms which strongly
suggests that our cohort comprises subjects with early primary severe RSV LRTI It is thought that early infancy with a rela-tively Th-2 skewed immune system may constitute a particu-larly vulnerable period of life for subsequent development of asthma following severe viral LRTI3 Viral airway infections andatopy may interact in a multiplicative way to promote asthmadevelopment in young childhood26 In addition predispositionto both early severe RSV bronchiolitis and allergic sensitisationmay be related to the interleukin (IL)-13IL-4 gene locus27
Potential hereditary susceptibility to RSV bronchiolitis has alsobeen reported28
Potential confounding factors do exist within our cohort Malliaand Johnston29 have previously suggested that the higher rate of asthma in our RSVcohort compared with controls could be duetoselection bias generated by the selection of controls contempora-neously from the same child healthcare centres as the indexcasesTheoretically our selection process during an ongoing RSVepidemic could generate controls with a lower susceptibility forsevere RSV bronchiolitis and a lower risk for subsequent allergicasthma if severe RSV bronchiolitisand subsequentallergic asthmaare markers of the same genotype There are two main reasons
0
10
20
30
40
50
60
70
80
Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
1511111883No total
1447714No RSV
1741169No controls
14991777
1345712
1541065
Wheeze phenoype
0Remitting
intermittent
TransientNo wheeze Persistent
relapsing
Late onset
No total
No RSV
No controls
Wheeze phenoype
10
20
30
40
50
60
70
80
90
100
A
B
Figure 3 Proportion () of subjects with (A) allergic rhinoconjunctivitisin different wheezing phenotypes (overall c2 plt0001 plt001plt0001 vs the no-wheeze phenotype) and (B) positive Phadiatoptest in different wheezing phenotypes (overall c2 plt0001 plt0001
vs the no-wheeze phenotype) Error bars denote 95 CI RSV respiratorysyncytial virus
1050 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 79
why we do not feel that selection bias signi1047297cantly affected ourresults First the RSV cohort had the same ARC and asthmaparentalsibling heredity prevalence as the controls and the RSVand control cohorts had a similar prevalence of AD Second thecontrol group had a similar prevalence of current asthmaRW
ARC and positive SPT at age 13 to a recent population-basedsample of 12e13-year-old Swedish children living in an over-lapping geographical area(85 17 and 225 respectively)30 31
Ourstudywas intended to be a descriptive study and as such wasnot powered to detect differences in hereditary rates of allergicdiseaseasthma between asthmatic and non-asthmatic indexcases Fifty index cases in each group would have been required toachieve adequate power Nevertheless there are indicationsthat early severe RSV bronchiolitis is associated with a greater
increased risk for subsequent asthma clinical allergy and allergicsensitisation when combined with a history of parental asthma(1047297gure 1 A eD)
The FEV1 FVC ratio and the FEF25e75 the most reliable andthe most sensitive spirometric indices of airway obstructionrespectively were reduced both at baseline and post-bronchodi-lator in our RSV cohort Airway obstruction was mostpronounced in subjects with a persistentrelapsing wheezingpattern at age 18 and this pattern could be traced back to ages 7and 13 years Interestingly spirometric indices were also reducedin subjects with RSV without current asthma These changesmay re1047298ect premorbid airway function32 or the presence of airway remodelling due to a severe RSV infection occurring-during a critical period of lung development with or without
subsequent interaction with early allergic sensitisation2 33
Young age at 1047297rst wheezing episode is an important riskfactor for subsequent persistent asthma in sensitised cohorts34
In the present study LCI was increased in both RSV andcontrol subjects with current asthma while spirometry resultswere impaired only in the subjects with RSV Increased LCI canresult from non-uniformity of ventilation distribution amonglung regions sharing branch points in the conducting airway zone or even more peripherally in the vicinity of the terminalbronchioles35 36 These results suggest that residual small airway dysfunction is not a result of RSV infection per se but is relatedto a subsequent diagnosis of asthma Peripheral airway obstruction and the patchy distribution of airway disease are
both recognised characteristics of asthma
9 37
Our 1047297
ndings areconsistent with other studies documenting raised LCI despite
normal spirometry in subjects with current mild asthma aged5e
15 years38 and normal small airway function in an RSVcohort without asthma followed up at age 10 using single-breath nitrogen washout5 The marked alveolarisation andcompletion of distal airway formation occurring during the 1047297rstthree years of life may compensate for the more peripheralairway sequelae of early severe RSV infection while moreproximal changes persist Increased AHR was present in thesubjects with asthma although not to the magnitude previ-ously reported in other studies in part due to the decision not towithhold ICS prior to testing A fall in FEV1 of 10 or more(mean 221) was seen in 8 of 41 subjects with RSV and in 5 of 86 tested controls (mean 201 pfrac140038 c2 with Yatesrsquo
correction) Despite this a signi1047297cant correlation of LCI but not
spirometry with AHR was ween in our RSV cohort andcon1047297rms the important 1047297ndings of Downie et al8 LCI but notspirometry was also signi1047297cantly correlated with ongoingairway in1047298ammation (FeNO)
In summary this study shows that severe primary RSVbronchiolitis in the 1047297rst year of life is frequently followed by allergic asthma persisting into early adulthood Subjects withRSV with and without current asthmaRW have reduced airway function as measured by spirometry Ventilation inhomogeneitya measure of small airway function is normal in subjects withRSV without current asthma but is linked to current asthma
AHR and ongoing airway in1047298ammation Our 1047297ndings suggestthat early severe RSV bronchiolitis has lifelong consequences of allergic asthma and airway remodelling
Acknowledgements The authors thank Mrs Gunilla Holmgren Wallmyr for skilfulassistance at all follow-up visits in this study and Mr Salmir Nasic for statisticaladvice
Funding The study was supported by grants from the Regional Health Care Authorityof West Sweden from Boras Hospital the Fokus Foundation and SeBersquos Fund
Competing interests None
Ethics approval This study was conducted with the approval of the Human ResearchCommittee of the Medical Faculty at the University of Gothenburg All parents andsubjects gave consent to the study
Provenance and peer review Not commissioned externally peer reviewed
REFERENCES1 Smyth RL Openshaw PJ Bronchiolitis Lancet 2006368312e22
2 Gelfand EW Pediatric asthma a different disease Proc Am Thorac Soc20096278e82
Table 6 Airway function and inflammatory markers in the different wheeze pattern groups for the entire cohort at age 18 years
Variable Never wheez e Transi ent wheez e Remitti ngintermittent wheez e Persistentrel apsing wheeze Late onset wheez e
Number of subjects 83 18 11 15 11
Airway function
FEV1 (z-score) 010 (093) 015 (163) 016 (097) 080 (079) 007 (074)
FEV1 FVC (z-score) 014 (097) 025 (121) 062 (102) 091 (088) 016 (124)
FEF25-75 (z-score) 008 (083) 016 (089) 045 (085) 093 (073) 024 (085)
LCI 654 (038) 652 (055) 646 (035) 681 (042) 697 (067)
FeNO (ppb) 13 (6e
74) 12 (6e
34) 21 (5e
34) 25 (7e
84) 18 (7e
69)Challenge (DACh)
Fall in FEV1 () 31 (00e113) 45 (00e221) 11 (00e64) 80 (00e310) 118 (03e428)
Reversibility
Rise in FEV1 () 30 (00e106) 48 (00e102) 61 (06e102) 67 (00e102) 54 (00e78)
Inflammatory markers
Blood eosinophils (3109 l) 013 (001e079) 018 ( 004e072) 016 (009e020) 030 (006e057) 019 (004e047)
Data are displayed as mean (SD) or median (range)Statistical analyses refer to comparison with the non-wheeze groupplt005 plt001 plt0001DACh dry air hyperventilation challenge FEF25e75 forced expiratory fraction at 25e75 forced vital capacity FeNO fraction exhaled nitric oxide FEV1 forced expiratory volume in 1 s FVCforced vital capacity ppb parts per billion
Thorax 2010651045e1052 doi101136thx2009121582 1051
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 89
3 Walton RP Johnston SL Role of respiratory viral infections in the development ofatopic conditions Curr Opin Allergy Clin Immunol 20088150e3
4 Stein RT Sherrill D Morgan WJ et al Respiratory syncytial virus in early life andrisk of wheeze and allergy by age 13 years Lancet 1999354541e5
5 Pullan CR Hey EN Wheezing asthma and pulmonary dysfunction 10 years afterinfection withrespiratorysyncytialvirusin infancy BMJ (Clin Res Ed) 19822841665e9
6 Korppi M Piippo-Savolainen E Korhonen K et al Respiratory morbidity 20 yearsafter rsv infection in infancy Pediatr Pulmonol 200438155e60
7 Johnson JE Gonzales RA Olson SJ et al The histopathology of fatal untreatedhuman respiratory syncytial virus infection Mod Pathol 200720108e19
8 Downie SR Salome CM Verbanck S et al Ventilation heterogeneity is a majordeterminant of airway hyperresponsiveness in asthma independent of airwayinflammation Thorax 200762684e9
9 Venegas JG Winkler T Musch G et al Self-organized patchiness in asthma asa prelude to catastrophic shifts Nature 2005434777e82
10 Juniper EF Frith PA Hargreave FE Airway responsiveness to histamine andmethacholine relationship to minimum treatment to control symptoms of asthmaThorax 198136575e9
11 Sigurs N Bjarnason R Sigurbergsson F et al Asthma and immunoglobulin Eantibodies after respiratory syncytial virus bronchiolitis a prospective cohort studywith matched controls Pediatrics 199595500e5
12 Sigurs N Bjarnason R Sigurbergsson F et al Respiratory syncytial virusbronchiolitis in infancy is an important risk factor for asthma and allergy at age 7
Am J Respir Crit Care Med 20001611501e713 Sigurs N Gustafsson PM Bjarnason R et al Severe respiratory syncytial virus
bronchiolitis in infancy and asthma and allergy at age 13 Am J Respir Crit Care Med 2005171137e41
14 Swierkosz EM Flanders R Melvin L et al Evaluation of the Abbott Testpack RSV
enzyme immunoassay for detection of respiratory syncytial virus in nasopharyngealswab specimens J Clin Microbiol 1989271151e4
15 Court SD The definition of acute respiratory illnesses in children Postgrad Med J197349771e6
16 Ruuskanen O Ogra PL Respiratory syncytial virusCurrProblPediatr 19932350e7917 American Thoracic Society Standardization of spirometry 1994 update
Am J Respir Crit Care Med 19951521107e3618 Stanojevic S Wade A Stocks J et al Reference ranges for spirometry across all
ages a new approach Am J Respir Crit Care Med 2008177253e6019 Cole TJ Stanojevic S Stocks J et al Age- and size-related reference ranges
a case study of spirometry through childhood and adulthood Stat Med 200928880e98
20 Gustafsson PM Aurora P Lindblad A Evaluation of ventilation maldistribution as anearly indicator of lung disease in children with cystic fibrosis Eur Respir J200322972e9
21 Schauer U Hoffjan S Bittscheidt J et al RSV bronchiolitis and risk of wheeze andallergic sensitisation in the first year of life Eur Respir J 2002201277e83
22 Castro M Schweiger T Yin-Declue H et al Cytokine response after severerespiratory syncytial virus bronchiolitis in early life J Allergy Clin Immunol 2008122726e33
23 Thomsen SF van der Sluis S Stensballe LG et al Exploring the associationbetween severe respiratory syncytial virus infection and asthma a registry-basedtwin study Am J Respir Crit Care Med 20091791091e7
24 Wu P Dupont WD Griffin MR et al Evidence of a causal role of winter virusinfection during infancy in early childhood asthma Am J Respir Crit Care Med 20081781123e9
25 Kuehni CE Spycher BD Silverman M Causal links between RSV infection andasthma no clear answers to an old question Am J Respir Crit Care Med 20091791079
e80
26 Kusel MM de Klerk NH Kebadze T et al Early-life respiratory viral infections atopicsensitization and risk of subsequent development of persistent asthma J Allergy Clin
Immunol 20071191105e1027 Forton JT Rowlands K Rockett K et al Genetic association study for RSV
bronchiolitis in infancy at the 5q31 cytokine cluster Thorax 200964345e5228 Thomsen SF Stensballe LG Skytthe A et al Increased concordance of
severe respiratory syncytial virus infection in identical twins Pediatrics2008121493e6
29 Mallia P Johnston SL Respiratory viruses do they protect from or induce asthma Allergy 2002571118e29
30 Hesselmar B Aberg B Eriksson B et al Asthma in children prevalence treatmentand sensitization Pediatr Allergy Immunol 20001174e9
31 Hesselmar B Aberg B Eriksson B et al Allergic rhinoconjunctivitis eczema andsensitization in two areas with differing climates Pediatr Allergy Immunol 200112208e15
32 Stern DA Morgan WJ Wright AL et al Poor airway function in early infancy and
lung function by age 22 years a non-selective longitudinal cohort study Lancet 2007370758e64
33 Illi S von Mutius E Lau S et al Perennial allergen sensitisation early in life andchronic asthma in children a birth cohort study Lancet 2006368763e70
34 Matricardi PM Illi S Gruber C et al Wheezing in childhood incidence longitudinalpatterns and factors predicting persistence Eur Respir J 200832585e92
35 Crawford AB Makowska M Paiva M et al Convection- and diffusion-dependent ventilation maldistribution in normal subjects J Appl Physiol 198559838e46
36 Paiva M Verbanck S van Muylem A Diffusion-dependent contribution to the slopeof the alveolar plateau Respir Physiol 198872257e70
37 King GG Eberl S Salome CM et al Differences in airway closure between normaland asthmatic subjects measured with single-photon emission computedtomography and technegas Am J Respir Crit Care Med 19981581900e6
38 Macleod KA Horsley AR Bell NJ et al Ventilation heterogeneity in children withwell controlled asthma with normal spirometry indicates residual airways diseaseThorax 20096433e7
1052 Thorax 2010651045e1052 doi101136thx2009121582
Asthma
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from
7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from

7262019 VRS vs asma
httpslidepdfcomreaderfullvrs-vs-asma 99
of lifeyearafter severe RSV bronchiolitis in the first
yearsAsthma and allergy patterns over 18
Sigurbergsson Ragnar Bjarnason and Per M GustafssonNele Sigurs Fatma Aljassim Bengt Kjellman Paul D Robinson Fridrik
doi 101136thx20091215822010 65 1045-1052 originally published online June 27 2010Thorax
httpthoraxbmjcomcontent65121045Updated information and services can be found at
These include
MaterialSupplementary
htmlhttpthoraxbmjcomcontentsuppl20111216thx2009121582DC1Supplementary material can be found at
References BIBLhttpthoraxbmjcomcontent65121045
This article cites 38 articles 13 of which you can access for free at
serviceEmail alerting
box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(943)Inflammation (1145)TB and other respiratory infections
(219)Bronchitis (104)Bronchiolitis
(1649)Asthma
Notes
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcomon June 27 2015 - Published by httpthoraxbmjcom Downloaded from