Embed Size (px)
Citation preview

512
von Willebrand disease revealed after extraction … Aoun N et al Journal of International Oral Health 2016; 8(4):512-517
Received: 19th October 2015 Accepted: 20th January 2016 Conflict of Interest: None
Source of Support: Nil
Contributors:1Clinical Instructor, Department of Oral Pathology and Diagnosis, Lebanese University, Faculty of Dentistry, Beirut, Lebanon; 2Senior Lecturer and Postgraduate Tutor, Departments of Oral & Maxillofacial Surgery, and Oral Pathology & Diagnosis, Lebanese University, Faculty of Dentistry, Beirut, Lebanon; 3Assistant Professor and Chairperson, Doctorate of Odontological Sciences, Department of Oral Pathology and Diagnosis, Lebanese University, Faculty of Dentistry, Beirut, Lebanon.Correspondence:Dr. El Toum S. Second Floor, Bloc A, Mehanna Center, Main Road, Dekwaneh, P.O: 55-053, Beirut, Lebanon. Tel.: +961(0)3302803. Fax: +961(0)1687315. Email: [email protected] to cite the article:Aoun N, Noujeim Z, El Toum S. von Willebrand disease revealed after dental post-extractional bleeding: A case report. J Int Oral Health 2016;8(4):512-517.Abstract:A persistent post-extractional bleeding in an apparently healthy patient must warn dentists about a possible bleeding diathesis such as misdiagnosed von Willebrand disease (vWD), hemophilia A, and hemophilia C. Mild type of vWD and mild hemophilia A can be diagnosed in women with menorrhagia, in persons with excessive mucocutaneous bleeding such as bruising without recognized trauma, in persons with recurrent nose bleeds and prolonged oral cavity bleeding including gingivorragia after brushing or flossing teeth or dental cleaning or extractions, and in persons with persistent post-extractional bleeding. Dentists have indeed a primordial role in the management of post-extractional bleeding complications related to these diseases and in the orientation of patient to a specialized medical center for further investigations and management. In this study, a case of mild vWD was diagnosed after persistent post-extractional bleeding of the right second maxillary molar, on a 43-year-old patient without medical or bleeding history. Extraction of 17 was performed and 24 h later persistent bleeding was noted. Ruling out local causes by clinical examination and periapical radiograph, a complete blood screening including complete blood count, platelets count, bleeding time, prothrombin time (PT), and cephalin kaolin clotting time (CKCT) was performed to evaluate the primary hemostasis and coagulation. Prolonged CKCT (46.30 s) and normal PT (14 s) illustrated a disorder function of intrinsic coagulation pathway including Factors VIII, IX, and XI. Factors VIII and IX had normal values. Further laboratory investigations of Ag von Willebrand factor and its ristocetin cofactor activity permitted the diagnosis of vWD.
Key Words: Bleeding, hemophilia A, hemophilia C, post-extractional, von Willebrand
IntroductionThe post-extractional hemorrhagic risk in a healthy patient with no documented medical history is rare. When local etiology
of post-extractional persistent bleeding and consumption of anticoagulant or antiplatelet medicine are ruled out, a screening of the coagulation is recommended.1,2 Further investigations and appropriate laboratory tests must be done to screen hemostasis factors and function. Hemostasis disorders were described in von Willebrand disease (vWD), hemophilia A, B, and C.3-5
vWD may cause excessive or extended bleeding. This condition is often inherited as an autosomal dominant trait, but may develop in adult life, in rare cases.6-14 It is the most common of inherited bleeding disorders affecting an estimated prevalence of 0.1 to 1% in the population worldwide.6,7,9,15,16 vWD is associated with mutations on chromosome 12 in the region p13.2, encoding the von Willebrand factor (vWF), which is synthesized in endothelial cells and megakaryocytes.9,16 vWF aids in the adhesion of platelets at a site of bleeding, and it also binds to Factor VIII acting as a transport molecule.6-14
The current International Society on Thrombosis and Hemostasis Scientific and Standardization Committee classified vWD into three subtypes:• Type 1 - vWD is a partial quantitative deficiency of
essentially normal vWF: It affects 85% of patients• Type 2 - vWD is a qualitative deficiency and defective vWF
(further subdivided into Types 2A, 2B, 2M, and 2N)• Type 3 - vWD is a virtually complete quantitative deficiency
of vWF9 and mostly diagnosed in childhood.15,17
Clinical expression of vWD is usually mild in Type 1, increasing in severity in Types 2 and 3.11,15 However, mild vWD may be clinically insignificant6 and misdiagnosed.11
Mild type of vWD can be diagnosed in women with menorrhagia, in persons with excessive mucocutaneous bleeding9,11 such as bruising without recognized trauma, and in persons with recurrent nose bleeds and prolonged oral cavity bleeding including gingivorragia9,14,16,18 after brushing or flossing teeth or dental cleaning or extractions.9,15,18
Hemophilia represents a variety of bleeding disorders associated with a genetic deficiency of any one of the following clotting factors: Factor VIII (hemophilia A), Factor IX (hemophilia B), and Factor XI (hemophilia C).6,19,20
Hemophilia A is the most significant and widely recognized form of hemophilia. It accounts for 80% to 85% of bleeding diatheses associated with a specific clotting factor deficiency6
Case Report
von Willebrand Disease Revealed after Dental Post-extractional Bleeding: A Case ReportNicole Aoun1, Ziad Noujeim2, Sami El Toum3
Doi: 10.2047/jioh-08-04-21

513
Journal of International Oral Health 2016; 8(4):512-517von Willebrand disease revealed after extraction … Aoun N et al
being transmitted in an X-linked pattern.6,19,20 Females typically carry the trait, but it is expressed primarily in males. Approximately 1 in 8,000 to 10,000 males is born with this genetic disease. It is a heterogeneous disorder that is caused by any one of a variety of mutations associated with the gene for Factor VIII.6 It can be severe, moderate, and mild. The moderate and mild types can be diagnosed in adults either after persistent post-extractional bleeding or in women after menorrhagia.19,20
Hemophilia B or Christmas disease is similar to hemophilia A in its presentation, being transmitted in an X-linked fashion. It is much less common than hemophilia A, occurring with a prevalence of 1 in 50,000.6
Hemophilia C or Rosenthal syndrome is a hemostatic plasma glycoprotein which circulates as a serine protease zymogen of activated Factor XI. It is essential for the generation of thrombin during coagulation. Factor XI deficiency is one of the most frequent genetic disorders in Ashkenazi Jews (it affects 8% of them).21 It is an autosomal bleeding disorder characterized by variable bleeding tendency.22 Unlike hemophilia, Factor XI deficiency is rarely manifested as spontaneous bleeding; the associated bleeding usually occurs after trauma, surgery, or other challenges to hemostasis.23
In this study, a case of prolonged bleeding after a dental extraction (maxillary second right molar) in an apparently healthy patient conducting after appropriate laboratory tests, to the diagnosis of vWD is reported.
Case ReportA 43-year-old male patient consulted us for full mouth rehabilitation. His medical observation revealed a scar resulting from trauma in 2003, on the right frontal region, and in 2006, on the forearm following an occupational accident by the grinder. He did not report any abnormal bleeding complication during and after these two accidents.
Orofacial history revealed multiple extractions. In 2009, mild bleeding for 24 h after extraction of 24 and 36 was noticed, these bleeding episodes resolved without any treatment.
Our treatment plan involved extraction of 17, 45, and 48. The periapical radiograph showed a radiolucency image at furcation of 17 (Figure 1).
Second maxillary right molar was extracted under periapical analgesia (scandicain special 2% with epinephrine 1:100,000) and the patient left our dental surgery with a controlled bleeding.
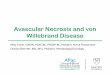
About 2 days after the extraction, patient consulted for an extra-alveolar clot on extraction site. No local etiologies (such as residual roots and bone sequestrum) were identified on a
periapical radiograph of 17 justifying this bleeding (Figure 2a). Analgesia was performed to remove the clot and permit a control of buccal and palatal cortical bones. A hemostatic sponge filled the empty alveolar cavity and bleeding were controlled with sutures. The patient left dental office with a gauze soaked with tranexamic acid (Exacyl®), an antifibrinolytic agent.
On the 3rd day, the patient presented with the same clinical situation, with ruptured sutures and new formation of the extra-alveolar clot at extraction site (Figure 2b). Hemostatic gelatin sponge (Gelfoam®) and sutures assured a bleeding control for 24 h only. For continuous compression of the extracted site, a thermoplastic splint was designed to cover the site and overflow 5 mm on each site. It assured stabilization of hemostatic sponge and protection of sutures, but this procedure failed to control bleeding.
A complete blood screening including complete blood count, platelets count (PC), bleeding time (BT), prothrombin time (PT), and cephalin kaolin clotting time (CKCT) was performed to evaluate the primary hemostasis and coagulation.
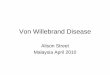
On 4th post-operative day, the patient came back with the same clinical figure with an overlapped clot covering adjacent teeth and impression of the antagonist was noticed (Figure 3). Elimination of the clot was done, and results of blood tests showed the followings:• PC 266 000 G/mm3 and BT (with Duke Method) 1’ 45’’
which are normal values.• PT was 14 s and witness time 11 s. CKCT was 46.30 s. He
had a prolonged CKCT and normal PT which illustrated a disorder function of intrinsic coagulation pathway including Factors VIII, IX, and Factor XI.
The patient was referred to a hematologist to explore coagulation factors and to diagnose a possible blood diathesis responsible of this coagulation disorder. The hematologist
Figure 1: Pre-operative periapical radiograph of 17.
514
von Willebrand disease revealed after extraction … Aoun N et al Journal of International Oral Health 2016; 8(4):512-517
asked for liver screening factors, creatinine, and Factor VIII. Furthermore, Etamsylate (Dicynone® 500 mg tablets, 1 tablet each 8 h for 1 week), an antihemorrhage drug capable of reducing BT, was prescribed.
On 7th post-operative day, bleeding persisted and the hematologist, after the normal result of liver factors and creatinine, suspected a local factor and referred the patient to an oral maxillofacial surgeon who performed bone compression on the alveolar socket and filled the socket with gauzes, then sutured wound edges.
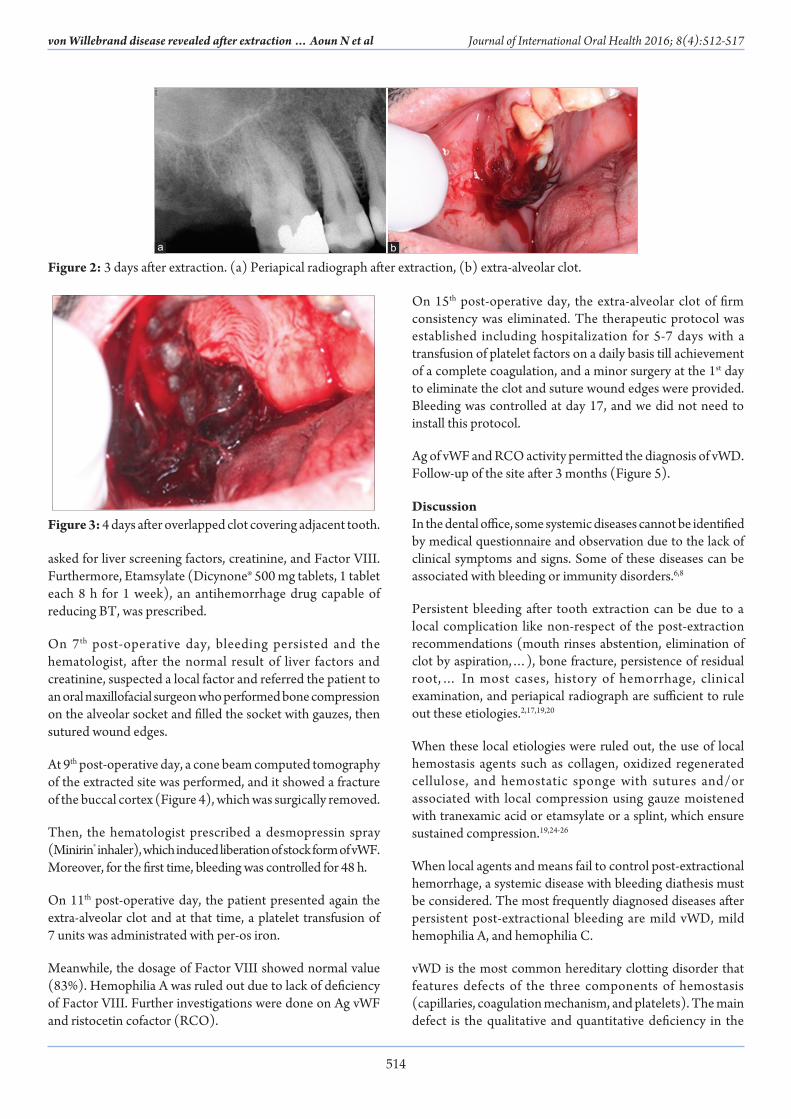
At 9th post-operative day, a cone beam computed tomography of the extracted site was performed, and it showed a fracture of the buccal cortex (Figure 4), which was surgically removed.
Then, the hematologist prescribed a desmopressin spray (Minirin® inhaler), which induced liberation of stock form of vWF. Moreover, for the first time, bleeding was controlled for 48 h.
On 11th post-operative day, the patient presented again the extra-alveolar clot and at that time, a platelet transfusion of 7 units was administrated with per-os iron.
Meanwhile, the dosage of Factor VIII showed normal value (83%). Hemophilia A was ruled out due to lack of deficiency of Factor VIII. Further investigations were done on Ag vWF and ristocetin cofactor (RCO).
On 15th post-operative day, the extra-alveolar clot of firm consistency was eliminated. The therapeutic protocol was established including hospitalization for 5-7 days with a transfusion of platelet factors on a daily basis till achievement of a complete coagulation, and a minor surgery at the 1st day to eliminate the clot and suture wound edges were provided. Bleeding was controlled at day 17, and we did not need to install this protocol.
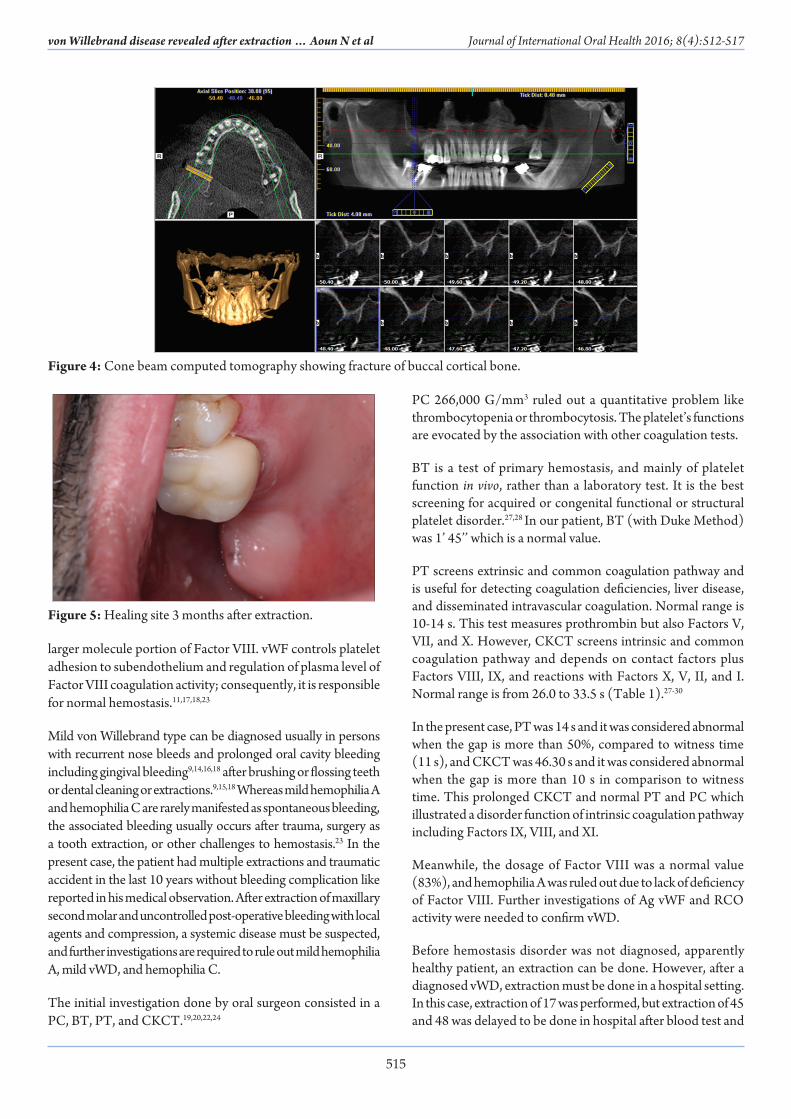
Ag of vWF and RCO activity permitted the diagnosis of vWD. Follow-up of the site after 3 months (Figure 5).
DiscussionIn the dental office, some systemic diseases cannot be identified by medical questionnaire and observation due to the lack of clinical symptoms and signs. Some of these diseases can be associated with bleeding or immunity disorders.6,8
Persistent bleeding after tooth extraction can be due to a local complication like non-respect of the post-extraction recommendations (mouth rinses abstention, elimination of clot by aspiration,…), bone fracture, persistence of residual root,… In most cases, history of hemorrhage, clinical examination, and periapical radiograph are sufficient to rule out these etiologies.2,17,19,20
When these local etiologies were ruled out, the use of local hemostasis agents such as collagen, oxidized regenerated cellulose, and hemostatic sponge with sutures and/or associated with local compression using gauze moistened with tranexamic acid or etamsylate or a splint, which ensure sustained compression.19,24-26
When local agents and means fail to control post-extractional hemorrhage, a systemic disease with bleeding diathesis must be considered. The most frequently diagnosed diseases after persistent post-extractional bleeding are mild vWD, mild hemophilia A, and hemophilia C.
vWD is the most common hereditary clotting disorder that features defects of the three components of hemostasis (capillaries, coagulation mechanism, and platelets). The main defect is the qualitative and quantitative deficiency in the
Figure 3: 4 days after overlapped clot covering adjacent tooth.
Figure 2: 3 days after extraction. (a) Periapical radiograph after extraction, (b) extra-alveolar clot.ba
515
Journal of International Oral Health 2016; 8(4):512-517von Willebrand disease revealed after extraction … Aoun N et al
larger molecule portion of Factor VIII. vWF controls platelet adhesion to subendothelium and regulation of plasma level of Factor VIII coagulation activity; consequently, it is responsible for normal hemostasis.11,17,18,23
Mild von Willebrand type can be diagnosed usually in persons with recurrent nose bleeds and prolonged oral cavity bleeding including gingival bleeding9,14,16,18 after brushing or flossing teeth or dental cleaning or extractions.9,15,18 Whereas mild hemophilia A and hemophilia C are rarely manifested as spontaneous bleeding, the associated bleeding usually occurs after trauma, surgery as a tooth extraction, or other challenges to hemostasis.23 In the present case, the patient had multiple extractions and traumatic accident in the last 10 years without bleeding complication like reported in his medical observation. After extraction of maxillary second molar and uncontrolled post-operative bleeding with local agents and compression, a systemic disease must be suspected, and further investigations are required to rule out mild hemophilia A, mild vWD, and hemophilia C.
The initial investigation done by oral surgeon consisted in a PC, BT, PT, and CKCT.19,20,22,24
PC 266,000 G/mm3 ruled out a quantitative problem like thrombocytopenia or thrombocytosis. The platelet’s functions are evocated by the association with other coagulation tests.
BT is a test of primary hemostasis, and mainly of platelet function in vivo, rather than a laboratory test. It is the best screening for acquired or congenital functional or structural platelet disorder.27,28 In our patient, BT (with Duke Method) was 1’ 45’’ which is a normal value.
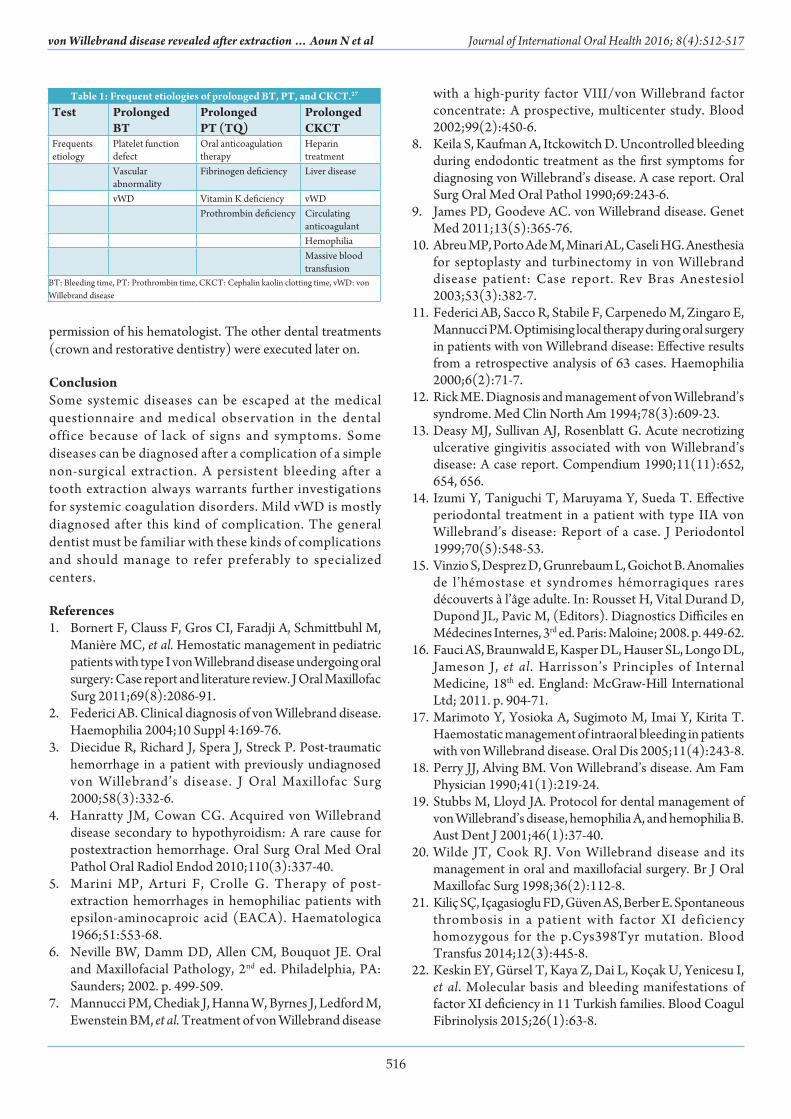
PT screens extrinsic and common coagulation pathway and is useful for detecting coagulation deficiencies, liver disease, and disseminated intravascular coagulation. Normal range is 10-14 s. This test measures prothrombin but also Factors V, VII, and X. However, CKCT screens intrinsic and common coagulation pathway and depends on contact factors plus Factors VIII, IX, and reactions with Factors X, V, II, and I. Normal range is from 26.0 to 33.5 s (Table 1).27-30
In the present case, PT was 14 s and it was considered abnormal when the gap is more than 50%, compared to witness time (11 s), and CKCT was 46.30 s and it was considered abnormal when the gap is more than 10 s in comparison to witness time. This prolonged CKCT and normal PT and PC which illustrated a disorder function of intrinsic coagulation pathway including Factors IX, VIII, and XI.
Meanwhile, the dosage of Factor VIII was a normal value (83%), and hemophilia A was ruled out due to lack of deficiency of Factor VIII. Further investigations of Ag vWF and RCO activity were needed to confirm vWD.
Before hemostasis disorder was not diagnosed, apparently healthy patient, an extraction can be done. However, after a diagnosed vWD, extraction must be done in a hospital setting. In this case, extraction of 17 was performed, but extraction of 45 and 48 was delayed to be done in hospital after blood test and
Figure 4: Cone beam computed tomography showing fracture of buccal cortical bone.
Figure 5: Healing site 3 months after extraction.
516
von Willebrand disease revealed after extraction … Aoun N et al Journal of International Oral Health 2016; 8(4):512-517
permission of his hematologist. The other dental treatments (crown and restorative dentistry) were executed later on.
ConclusionSome systemic diseases can be escaped at the medical questionnaire and medical observation in the dental office because of lack of signs and symptoms. Some diseases can be diagnosed after a complication of a simple non-surgical extraction. A persistent bleeding after a tooth extraction always warrants further investigations for systemic coagulation disorders. Mild vWD is mostly diagnosed after this kind of complication. The general dentist must be familiar with these kinds of complications and should manage to refer preferably to specialized centers.
References1. Bornert F, Clauss F, Gros CI, Faradji A, Schmittbuhl M,
Manière MC, et al. Hemostatic management in pediatric patients with type I von Willebrand disease undergoing oral surgery: Case report and literature review. J Oral Maxillofac Surg 2011;69(8):2086-91.
2. Federici AB. Clinical diagnosis of von Willebrand disease. Haemophilia 2004;10 Suppl 4:169-76.
3. Diecidue R, Richard J, Spera J, Streck P. Post-traumatic hemorrhage in a patient with previously undiagnosed von Willebrand’s disease. J Oral Maxillofac Surg 2000;58(3):332-6.
4. Hanratty JM, Cowan CG. Acquired von Willebrand disease secondary to hypothyroidism: A rare cause for postextraction hemorrhage. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110(3):337-40.
5. Marini MP, Arturi F, Crolle G. Therapy of post-extraction hemorrhages in hemophiliac patients with epsilon-aminocaproic acid (EACA). Haematologica 1966;51:553-68.
6. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 2nd ed. Philadelphia, PA: Saunders; 2002. p. 499-509.
7. Mannucci PM, Chediak J, Hanna W, Byrnes J, Ledford M, Ewenstein BM, et al. Treatment of von Willebrand disease
with a high-purity factor VIII/von Willebrand factor concentrate: A prospective, multicenter study. Blood 2002;99(2):450-6.
8. Keila S, Kaufman A, Itckowitch D. Uncontrolled bleeding during endodontic treatment as the first symptoms for diagnosing von Willebrand’s disease. A case report. Oral Surg Oral Med Oral Pathol 1990;69:243-6.
9. James PD, Goodeve AC. von Willebrand disease. Genet Med 2011;13(5):365-76.
10. Abreu MP, Porto Ade M, Minari AL, Caseli HG. Anesthesia for septoplasty and turbinectomy in von Willebrand disease patient: Case report. Rev Bras Anestesiol 2003;53(3):382-7.
11. Federici AB, Sacco R, Stabile F, Carpenedo M, Zingaro E, Mannucci PM. Optimising local therapy during oral surgery in patients with von Willebrand disease: Effective results from a retrospective analysis of 63 cases. Haemophilia 2000;6(2):71-7.
12. Rick ME. Diagnosis and management of von Willebrand’s syndrome. Med Clin North Am 1994;78(3):609-23.
13. Deasy MJ, Sullivan AJ, Rosenblatt G. Acute necrotizing ulcerative gingivitis associated with von Willebrand’s disease: A case report. Compendium 1990;11(11):652, 654, 656.
14. Izumi Y, Taniguchi T, Maruyama Y, Sueda T. Effective periodontal treatment in a patient with type IIA von Willebrand’s disease: Report of a case. J Periodontol 1999;70(5):548-53.
15. Vinzio S, Desprez D, Grunrebaum L, Goichot B. Anomalies de l’hémostase et syndromes hémorragiques rares découverts à l’âge adulte. In: Rousset H, Vital Durand D, Dupond JL, Pavic M, (Editors). Diagnostics Difficiles en Médecines Internes, 3rd ed. Paris: Maloine; 2008. p. 449-62.
16. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson J, et al. Harrisson’s Principles of Internal Medicine, 18th ed. England: McGraw-Hill International Ltd; 2011. p. 904-71.
17. Marimoto Y, Yosioka A, Sugimoto M, Imai Y, Kirita T. Haemostatic management of intraoral bleeding in patients with von Willebrand disease. Oral Dis 2005;11(4):243-8.
18. Perry JJ, Alving BM. Von Willebrand’s disease. Am Fam Physician 1990;41(1):219-24.
19. Stubbs M, Lloyd JA. Protocol for dental management of von Willebrand’s disease, hemophilia A, and hemophilia B. Aust Dent J 2001;46(1):37-40.
20. Wilde JT, Cook RJ. Von Willebrand disease and its management in oral and maxillofacial surgery. Br J Oral Maxillofac Surg 1998;36(2):112-8.
21. Kiliç SÇ, Içagasioglu FD, Güven AS, Berber E. Spontaneous thrombosis in a patient with factor XI deficiency homozygous for the p.Cys398Tyr mutation. Blood Transfus 2014;12(3):445-8.
22. Keskin EY, Gürsel T, Kaya Z, Dai L, Koçak U, Yenicesu I, et al. Molecular basis and bleeding manifestations of factor XI deficiency in 11 Turkish families. Blood Coagul Fibrinolysis 2015;26(1):63-8.
Table 1: Frequent etiologies of prolonged BT, PT, and CKCT.27
Test Prolonged BT
Prolonged PT (TQ)
Prolonged CKCT
Frequents etiology
Platelet function defect
Oral anticoagulation therapy
Heparin treatment
Vascular abnormality
Fibrinogen deficiency Liver disease
vWD Vitamin K deficiency vWDProthrombin deficiency Circulating
anticoagulantHemophiliaMassive blood transfusion
BT: Bleeding time, PT: Prothrombin time, CKCT: Cephalin kaolin clotting time, vWD: von Willebrand disease

517
Journal of International Oral Health 2016; 8(4):512-517von Willebrand disease revealed after extraction … Aoun N et al
23. Asakai R, Chung DW, Davie EW, Seligsohn U. Factor XI deficiency in Ashkenazi Jews in Israel. N Engl J Med 1991;325(3):153-8.
24. Sakurai Y, Shima M, Imai Y, Omura S, Kirita T, Yoshioka A. Successful use of recombinant factor VIII devoid of von Willebrand factor during multiple teeth extractions in a patient with type 3 von Willebrand disease. Blood Coagul Fibrinolysis 2006;17(2):151-4.
25. Saulnier J, Marey A, Horellou MH, Goudemand J, Lepoutre F, Donazzan M , e t al . Evaluation of desmopressin for dental extractions in patients with hemostatic disorders. Oral Surg Oral Med Oral Pathol 1994;77(1):6-12.
26. Williamson R, Eggleston DJ. DDAVP and EACA used for
minor oral surgery in von Willebrand disease. Austral Dent J 1998;33(1):32-6.
27. Provan D. Oxford Handbook of Clinical and Laboratory Investigation, 2nd ed. Oxford: Oxford University Press; 2005. p. 197-247.
28. Hillman RS, Keneth A, Ault-Henry M. Hematology in Clinical Practice, 4th ed. New York: McGraw Hill Professional; 2005.
29. Beers MH, Berkow R, Fletcher AJ, (Editors). Manual Merck de Diagnostic et Thérapeutique, 17th ed. Rahway, NJ: Merck Research Laboratories; 2000.
30. Chbicheb S, Hakkou F, El Wady W. Coagulation Troubles: Oral Manifestations and management. EMC – Chirurgie Orale et Maxillo-Faciale 2014;9(2):1-8.












![Journal of Blood Disorders & Transfusion...disorders include hemophilia, von Willebrand disease, thrombophilia, thalassemia and sickle cell anemia [2]. Thalassemia is a blood related](https://img.pdfslide.us/doc/110x75/60dd4fbd4ae15219f42ad898/journal-of-blood-disorders-transfusion-disorders-include-hemophilia-von.jpg)