Embed Size (px)
Citation preview
This publication is a Family Focus Program of the
National Kidney Foundation and is made possible in part through
an educational grant from
in this issue
VOLUME 10 NUMBER 3 SUMMER 2001
The Renal Community’s Newspaper
Patient and Family Cornerpage 5
Good Nutritionpage 6
The More You Knowpage 10
A Look Into the Futurepage 11
Fitnesspage 12
The Parent Connectionpage 13
National KidneyFoundation®
Use of Complementary &Alternative Medicine
Do you take herbalsupplements, do yoga or see achiropractor? All of these
treatments and many others arecalled complementary or alternativemedicine. Traditional medicineconsiders complementary andalternative medicine (CAM) to beoutside the range of “proven”treatments. People use complemen-tary medicine along with what theirdoctor prescribes. People usealternative medicine instead of whattheir doctor prescribes.
The basis of traditional medicine isthat the doctor knows best and thepatient does what the doctor says.The basis of CAM is that patients andhealers work together. Rather thanthe doctor taking full responsibility forthe patient’s health, both shareresponsibility for the patient’s healthand choices.1,2
CAM’s Use & Acceptance
One national study compared theuse of CAM treatments in 1990 withthose used in 1997. Thirty-threepercent of those surveyed reportedthey used CAM treatments in 1990,while 42 percent reported they usedCAM treatments in 1997. People saidthey used CAM for ailments like backproblems, headaches, depression andanxiety.3 Eighty percent of elderlyCalifornians insured by a MedicareHMO said CAM treatments helpedthem. However, 58 percent did not telltheir doctors they used CAMpractices.4 Ninety percent of familydoctors said they believed exerciseand diet, biofeedback, psychotherapyand behavioral medicine were reliable.Fifty percent of these doctors wouldrefer for these services.5
Study of CAM Practices
Congress funded an office in theNational Institutes of Health in 1992that was charged with studying CAMpractices and informing the public ofits findings. This office became theNational Center for Complementaryand AlternativeMedicine(NCCAM) in1998. TheNCCAM hasfound that sometreatments thatwere onceconsidered CAMwork and aregainingacceptance intraditionalmedicine. Manydoctors whowould haveconsideredpatienteducation,behavioral and“talk therapy” tobe CAM 20 yearsago are embracing these treatmentstoday. Doctors will also accept othertreatments when research shows theyare safe and effective.6
Mind-Body Medicine
Can the mind affect the body?Research has shown that stress canaffect blood pressure, pulse andbreathing. It can also affect bloodclotting, blood sugar levels, sodiumretention and the immune system.7 Itmakes sense that if stress can harmthe body, techniques to reduce stressmight help the body. Research hasshown that this is indeed the case.Relaxation, yoga, biofeedback,
meditation, guided imagery andpsychotherapy may reduce stress andcontrol blood pressure,8 reduce painand anxiety and shorten hospitalstays following surgery.9
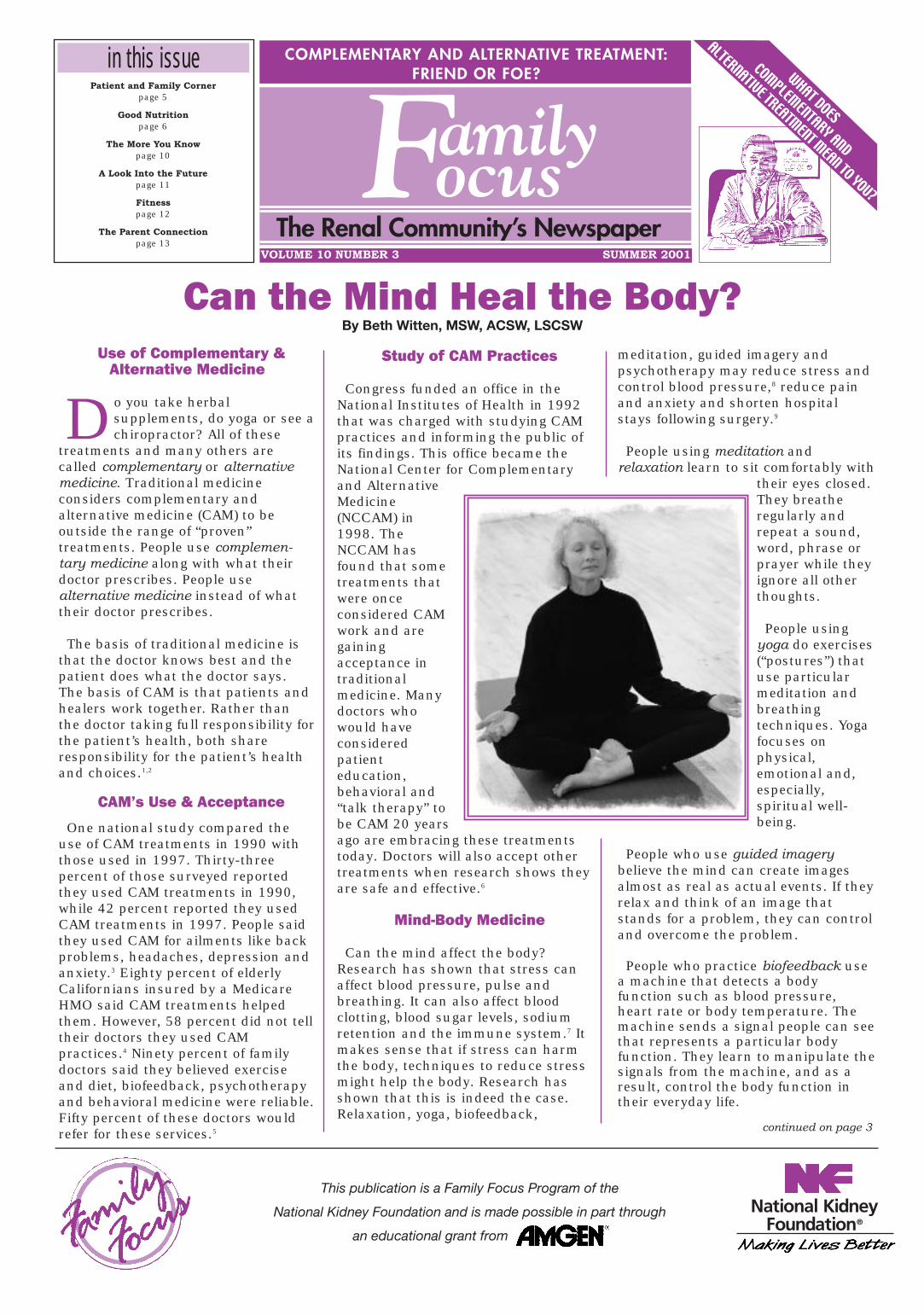
People using meditation andrelaxation learn to sit comfortably with
their eyes closed.They breatheregularly andrepeat a sound,word, phrase orprayer while theyignore all otherthoughts.
People usingyoga do exercises(“postures”) thatuse particularmeditation andbreathingtechniques. Yogafocuses onphysical,emotional and,especially,spiritual well-being.
People who use guided imagerybelieve the mind can create imagesalmost as real as actual events. If theyrelax and think of an image thatstands for a problem, they can controland overcome the problem.
People who practice biofeedback usea machine that detects a bodyfunction such as blood pressure,heart rate or body temperature. Themachine sends a signal people can seethat represents a particular bodyfunction. They learn to manipulate thesignals from the machine, and as aresult, control the body function intheir everyday life.
Can the Mind Heal the Body?By Beth Witten, MSW, ACSW, LSCSW
COMPLEMENTARY AND ALTERNATIVE TREATMENT:FRIEND OR FOE?
continued on page 3
WHAT DOES
COMPLEM
ENTARY AND
ALTERNATIVE TREATMENT M
EAN TO YOU?
2
Family Focus Volume 10 Number 3
After preparing and editing thisissue on complementary and alternative treatment, as well
as being an occasional consumer, Istill have a difficult time categorizingthe treatments as either friend or foe.The main points we want to stress arethat we should take all of thesetreatments seriously and that each ofthem has the potential to aid or toharm us, as well as to have norealizable impact at all. The FamilyFocus Editorial Board is by no means
attempting to influence you to use ornot to use complementary andalternative treatments. We, however,do want to influence you to informyour partners on your health careteam about any treatments that youare either considering trying or arecurrently using. We want to ensurethat if you use complementary andalternative treatments, you do sowithout any ill effect.
There are two issues that yourEditorial Board regrets we did nothave the opportunity to explore foryou in this issue. One of these is howour ethnic and cultural backgroundsmay influence how we view and usevarious forms of complementary andalternative treatments. While somecultures may see certain types ofthese treatments as "mainstream,"others will view the same treatmentsas anything but common! The otherissue we did not delve into is thehistorical aspect of these treatments.As Dale Ester points out in hisarticle, "Cautions about Using
Karren King
NKF Family Focus is published quarterly by the National Kidney Foundation
Editorial Office:National Kidney Foundation30 E. 33rd Street, New York, NY 10016(800) 622-9010 • (212) 889-2210http://www.kidney.org
Editor-in-Chief:Karren King, MSW,ACSW, LCSWKansas City, MO
Medical Editor:Wendy W. Brown, MD St. Louis, MO
Nursing Editor:Bobbie Knotek, RN, BSN Plano, TX
Fitness Editor:Susan Carey, ACSM, MSEugene, OR
Nutrition Editor:Lori Fedje, RD, LD Portland, OR
Pediatric Editor: Barbara Fivush, MDBaltimore, MD
Patient Editor:Dale EsterGlendale, AZ
Social Work EditorBeth Witten, MSW,ACSW, LSCSWOverland Park, KS
Opinions expressed in this newspaper do not necessarily represent the position of the National Kidney Foundation
Editorial Director: Gigi PolitoskiEditorial Manager:Sheila Weiner, MSW, CSWExecutive Editor: Diane GoetzManaging Editor: Sara KosowskyProduction Manager: Emily ZelnerDesign Director: Oumaya Abi Saab
FROM THE EDITOR Alternative Treatments," some formsof treatment were used by the "humanrace long before the present time."While we couldn’t cover all aspects ofthis topic in one issue, we do hopethat you will enjoy and be informed bythe wide range of information that wehave provided.
It is hard to believe that the first yearof this Editorial Board will be comingto a close after our next issue,Chronic Kidney Disease and the LifeCycle. As we wrap up this year, webegin to look to future issues ofFamily Focus. With that in mind, wewould love to hear from you. We inviteyou to share with us suggested"themes" that you believe are timely,needed and important for futureissues of this newspaper. Please sendyour ideas to me in care of theNational Kidney Foundation. After all,who knows better what is needed thanpeople like you who live with chronickidney disease? We can all learn fromwhat you have to share.
Karren King, MSW, ACSW, LCSWEditorFor the Editorial Board
We’d like to make sure that NKF
Family Focus is making its way to
every dialysis unit and transplant
center in the country. If we’re
missing anyone, or if you
would like to receive a free copy at
your home, please let us know
by dropping us a note or
by giving us a call at:
(800) 622-9010.
Are we
missing you?
F
Family Focus Volume 10 Number 3
3
Can the Mind Heal the Body?continued from page 1
People who seek psychotherapy(counseling) talk about their problems,feelings, behaviors, hopes and dreamswith trained mental healthprofessionals such as social workers,psychologists and psychiatrists. Bytalking through their problems, they“get problems off their chests” andlearn new ways to cope.
Learning What You Can About ACAM Provider
Although some CAM therapies can behelpful, others are dangerous and cancause serious problems. Be on guardif you think claims sound “too good tobe true.” A fact sheet from theNCCAM10 recommends that you:
� Talk with others who have used theCAM provider.
� Ask the CAM provider about his orher qualifications.
� Check with your State Departmentof Health to find out if the CAMspecialty is regulated in your state,and how to find out if your provideris licensed or certified.
� Interview the provider so you’remore comfortable receiving servicesthere.
� Learn what treatments cost andwhat is covered by insurance.
� Tell your kidney doctor and health
care team all the CAM treatmentsyou are using.
Remember, you have a duty toyourself and your family to protectyour health and your life. Learn allyou can about all your treatmentoptions. Choose what you do wiselyusing the information you learn.
References:1. Rubik B: Can western science
provide a foundation foracupuncture? Altern Ther HealthMed 1:41-47, 1995.
2. Cook CAL, Becvar DS, Pontious SL:Complementary alternativemedicine in health and mentalhealth: Implications for socialwork practice. Social Work HealthCare 31: 39-56, 2000.
3. Eisenberg DM, Davis RB, Ettner SL,Appel S, Wilkey S, Van Rompay M,Kessler RC: Trends in alternativemedicine use in the United States,1990-1997: Results of a follow-upnational survey. JAMA 280: 1569-75, 1998.
4. Astin JA, Pelletier KR, Marie A,Haskell WL: Complementary andalternative medicine use amongelderly persons: One-year analysisof a Blue Shield Medicare supplement. J Gerontol A Biol SciMed Sci 55: M4-9, 2000.
5. Berman BM, Singh BK, Lao L, SinghBB, Ferentz KS, Hartnoll SM:Physicians’ attitudes towardcomplementary or alternativemedicine: A regional survey. J AmBoard Fam Pract. 8: 361-366,1995.
6. National Center for Complementary& Alternative Medicine: AboutNCCAM: General information.http://nccam.hih.gov/nccam/an/general/index.html.
7. Seaward BL: Managing stress:Principles and strategies for healthand wellbeing. Boston: Jones andBartlett Publishers, 1997.
8. Anand MP: Non-pharmacologicalmanagement of essentialhypertension. J Indian Med Assoc97: 220-225, 1999.
9. Tusek DL: Guided imagery: Apowerful tool to decrease length ofstay, pain, anxiety, and narcoticconsumption. J Invasive Cardiol11: 265-267, 1999.
10. National Center for Complementary& Alternative Medicine:Considering complementary andalternative medicine.http://nccam.nih.gov/fcp/faq/considercam.html. F
Letter to the EditorIn 1993, my medical doctor at that time informed me thatproteins were "spilling" into my urine. My hematologistreferred me to my renal doctor of eight years now. By June22, 1998, a Tenckhoff catheter was placed in myabdomen. I began peritoneal dialysis on July 8, 1998. Istarted out with four treatments a day, but it wasdetermined that I would need five a day after the first year.
I have suffered with sickle cell disease since the age of fiveyears. Frankly, ESRD and sickle cell are in direct conflictin my body. Consequently, I’ve been having a tough time.I’ve been going into crisis much too often.
As painful as my crisis can be, I’m in even more pain nowand it’s constant. I also have hepatitis C, contracted froma blood transfusion in 1989. I need as much informationas I can get. To be able to correspond or talk with someonedealing with the same situation might be helpful also.Thank you for any time and attention you can give to thismatter.
If you would like to correspond with the above patientplease send your reply to Family Focus Friends, National Kidney Foundation, 30 East 33rd Street,New York, NY 10016. F
Meet Us In San Francisco As we continue to move
across the country with our educational program for:
• individuals with kidney disease who are not yet on treatment • dialysis patients • donor families • transplant recipients of all organs • and family members
October 13, 2001 San Francisco, California
The National Kidney Foundationis pleased to bring youeducational programs such asthese to help improve yourquality of life!!!
For more information contact the National Kidney Foundation at30 East 33rd Street, New York, NY 10016 or call 800-622-9010.
Family Focus Volume 10 Number 3
4
addition, they make blood vesselsgrow smaller, which leads to lessblood flow or supply of blood totissues and organs. Tissues aredamaged when they don’t receiveenough blood. Cells may die. Scarsform. If the affected organ is thekidney, it loses the ability to do itswork. The kidney disease thathappened so rapidly in these Belgianwomen may have been caused by acombination of exposure at the sametime to the toxin and the twomedicines that caused a decrease inappetite and a decrease in blood flow.
It is also notknown why onlysome patients whotook the herbs gotkidney disease, andfor some reasonwomen appear tobe at greater riskthan men. Otherpossible factorsinclude the amountof herbs that weretaken, batch-to-batch differences intoxin content, indi-vidual differencesin the way the bodyhandles the toxinand an inherited
tendency of a persontowards kidney damage from suchtoxins and/or towards development ofcancer.
Regardless of how it occurred,there is no question that kidneydisease from Chinese herbs isassociated with the development ofcancer.
Presentation and PrognosisAffected patients typically present
to a medical professional with kidneyfailure. Their blood pressure is eithernormal or only slightly increased.They don’t have a lot of protein intheir urine, and the urine containsonly a few red blood cells and whiteblood cells.
Kidney function may range frombeing slightly decreased or severelydecreased when patients first seetheir doctor. The patients’ creatinineshave ranged from 1.4 to 12.7 mg/dl.Those patients with serumcreatinines closer to the normal rangeseem to do well and do not needdialysis. However, progressive kidneyfailure leading to a need for dialysisor a transplant may occur in patients
with more severe disease even if theystop taking the Chinese herbs. Thelonger patients take the herbs, themore likely they are to have severekidney damage. A similar problemhappened to a group of patients fromTaiwan who took some othertraditional Chinese herbs that werenot the same as the weight lossherbs. Even though the Taiwanesepatients stopped taking the herbs,they had kidney failure. Theimportant point to remember is thatthese herbs are not tested likeprescription medications to makesure that they don’t cause harm tothe body. In addition, they may notbe “pure” but may be mixed withother ingredients that can beharmful. It is always a good idea toask your doctor before you take anyherbs.
TreatmentThere is no effective treatment for
the kidney disease that the Chineseherbs cause, although it is possiblethat corticosteroids such asprednisone, may slow the course ofdisease. Because of the risk of cancer,these patients have to be examinedon a regular basis to look for cancerin the kidney, ureters or bladder.Some doctors have suggested thatthese patients should have theirkidneys and ureters surgicallyremoved because of the high risk ofcancer.
Lessons� Not everything “natural” is
healthy.
� Don’t take any herbs or herbalremedies without talking to yourdoctor first. You can buy many“over-the-counter naturalmedicines” without a prescriptionthat can harm you.
� Natural herbs may be moreharmful for patients who alreadyhave kidney disease. St. John’sWort, for example, which hasbeen used to treat depression,shouldn’t be used by anyone witha transplant because it affects theblood level of medicines that helpprevent transplant rejection.
Marc E. DeBroe, MD, PhD, is withthe Department of Nephrology at theUniversity of Antwerp in Belgium.
Kidney Disease Caused By Chinese HerbsBy Marc E. DeBroe, MD, PhD
It is very important to be awarethat “natural” herbal remedies,many of which can be pur-
chased easily in grocery, drug orhealth food stores, can be harmful tothe kidneys or other organs. Doctorsin Belgium noted an increasingnumber of women who developedacute, often near end-stage kidneyfailure after taking Chinese herbs ata weight reduction clinic in 1991. Atotal of 14 women were found to havesevere kidney disease over a threeyear period of time in Brussels,Belgium. They had kidney biopsiesthat showed a type of kidney diseasecalled chronic tubulo-interstitialnephritis; nine of these women tookChinese herbs to lose weight. Morethan 100 women who had developedkidney disease from taking Chineseherbs were identified by early 1999.More than one-third of these patientshave already had kidney transplants.
In addition to causing kidneyfailure, these Chinese herbs alsoaffect cells in the kidneys andureters, causing changes that canresult in cancer of the kidneys orureters (tubes that carry urine fromthe kidney to the bladder). As aprecaution against developing cancer,Belgian doctors have removed nativekidneys and ureters from 10 patientsduring or after kidney transplant. Atleast one of these patients hadbladder cancer. Four patients had anearly form of cancer. The rest of thepatients had cells which lookedabnormal and showed changes thatmight lead to cancer.
The reason that Chinese herbscause kidney disease is not wellunderstood. A toxin (poison),aristolochic acid, found in someChinese plants that cause kidneydamage was thought to be a possiblecause of the kidney failure, but it wasnot part of the herbal preparationsused by all the patients. In addition,this chemical has been used bythousands of patients in Germany formore than 20 years to regulate theimmune system and has not causedkidney disease in any of thesepatients.
In addition to Chinese herbs,patients who developed kidneydisease also took two medicines forweight loss. These medicines,fenfluramine and diethylpropion,cause a decrease in appetite. In
F
5
Family Focus Volume 10 Number 3
It may seem that herbalformulations can’t be life-threatening or even the least bit
dangerous because they are sold overthe counter in grocery and healthfood stores. Buyer beware! You mustbe careful because herbal treatmentsare medications and all drugs havesome effect on the human body.
Although herbs were used largely intheir raw and unprocessedform by the human race longbefore the present time, it doesnot mean they are any safer orhave fewer risks or benefitstoday. We have simply come toknow more about them. Herbsare often called complementarymedicines or herbal treat-ments, but don’t be fooled by thedifferent names used to explain thesame thing. Many of thesetreatments, regardless of the nameused to describe them, could result ina serious and dangerous, possiblyeven life-threatening, crisis.
How does one know if an herbaltreatment is safe? If it works well fora friend or a family member, willit be a good treatment for you?No two people are alike. Thismeans that what works well forthem may not work well for you.In fact, it may not work at all foryou! They may not have had abad reaction from taking aparticular supplement but youmight.
Are the risks worth it? It isimportant to look closely at theproposed benefits and to decidewhether they outweigh the potentialrisks. An herbal formulation thatsolves a specific problem withoutcausing other health problems wouldbe beneficial. However, if thetreatment creates problems on top ofthe existing condition it could be
risky. Weighing the pros and consmay be confusing, so here are somesuggestions for how to approachherbal treatments:
1) Proceed with extreme caution.
2) Discuss the treatment idea withyour health care team before youstart the treatment.
3) If your doctor says it isokay to take thesupplement, learn as
much as possible about itto familiarize yourself withany potential side effects.
4) Share the responsibilityabout whether to use
herbal treatments with yourhealth care team by knowing theproposed benefits and thepotential risks before making apersonal choice. Ask yourself, “Dothe potential positive effectsoutweigh the negative ones?”
Herbal treatments can be a friend ifthey solve health problems or a foe if
they create more problemsthan expected. Since no two
people are alike, the benefits ofcomplementary medicine for oneperson will be different from thosefor another. The benefits shouldalways outweigh the potentialrisks. Discussing any treatmentideas with your health care team
and kidney doctor before youdecide to start an herbal treatmentprogram will always be the wisestway to achieve the best possiblehealth outcome. Remember thatsafety begins by knowing that herbaltreatments and complementarymedicines are real drugs in adifferent form than what you may beused to seeing. Your life may dependon proceeding with caution andlearning the facts.
✒ To Learn More About CAM
• Alternative Medicine:www.nccam.nih.gov or call theNational Center for Complementaryand Alternative Medicine at 888-644-6226
• NCCAM fact sheets:http://nccam.nih.gov/fcp/factsheets
• Research centers working with theNCCAM:http://nccam.nih.gov/nccam/fi/research/centers.html or call the NCCAMClearinghouse at (301) 589-5367 or(888) 644-6226
• National Library of Medicine databaseof free abstracts of journal articles onCAM:http://www.nlm.nih.gov/nccam/camonpubmed.html#
• The Combined Health InformationDatabase: http://www.chid.nih.gov
• Acupuncture:www.medicalacupuncture.org or callthe American Academy of MedicalAcupuncture at 323-937-5514
• Herbal remedies: www.herbs.org orcall the Herb Research Foundation at800-748-2617
PATIENT AND FAMILY CORNER
Cautions About Using AlternativeTreatments
By Dale Ester
F
Donate your used car to the NationalKidney Foundation Kidney Cars Program. The funds can help save lives. We’ll arrange a pickup and you might qualify for a tax deduction.*
Call l-800-488-CARS
*Consult your tax advisor for details.
Ready ToSay Goodbye
To YourOldCar?
Put Some“Good” In the Goodbye!
6
Family Focus Volume 10 Number 3
Alternative medicine has beenaround for centuries and it’smaking a comeback. An
estimated 629 million Americanssought alternative medicine practi-tioners and 60 million Americans weretaking herbs daily in 1997.1 Onereason for this increase is that herbalsupplements appeal to people’sdesires for a quick fix, and they allowpeople to participate in their own care.You must be aware though becausesupplements may not be safe for thosesuffering from kidney disease, dia-betes and other diseases.
Who regulates herbal supplements?
According to the Dietary Supple-ments Health and Education Act(DSHEA) of 1994, dietary supplementsinclude ingredients such as herbs,vitamins, minerals, amino acids andsubstances such as enzymes, organtissues, glandulars and metabolite.2
The manufacturer regulates the safetyof its own product according to theAct2 and is not required to notify theFederal Drug Administration (FDA) orconsumers of any reported adverseeffects. However, the FDA monitorsthe safety of these products throughvoluntary reports.3
How safe are herbal supplements?
The safety of the supplementdepends on the consumer’s medicalhistory. Side effects have beendocumented about consumers whohave taken “safe” herbs such asginkgo biloba, ginseng and St. John’sWart. Ginkgo biloba may causeinfrequent headaches or gastro-intestinal upset and shouldn’t betaken if you have a bleeding disorder.4
Ginseng may cause someone to sufferfrom headaches, inability to sleep,nervousness, diarrhea, rashes,asthma attacks, high blood pressureand arrhythmias.4 St. John’s Wart,which is often taken to improve aperson’s emotional well-being, is notwithout its share of complications. Itmay hinder the effectiveness ofcyclosporin and other immunosup-pressants used to prevent transplantrejection and cause high bloodpressure when taken with beta-blockers medication.4,5
Aristolochic acid is sometimes usedto stimulate the immune system. It
may also be used for treating GI andgallbladder colic that is caused byallergies, gynecological problems,wounds and ulcers and problemsassociated with the ears, nose andthroat. Artistolochic acid andproducts that contain it have beenfound to be toxic to the kidney and tocause cancer.6 Approximately 100cases of kidney disease werediagnosed in people who used aproduct containing aristolochic acid inBelgium, and 70 of them requireddialysis or transplantation.7
Why may supplements be unsafe?
Complications from taking herbalsupplements may arise due tounknown effects that have not yetbeen documented, long-term use orthe kidney’s inability to filter wasteproducts. Consumers may alsoexperience negative side effects fromcomplications caused by their diseasewhen taking a supplement. Forinstance, those on dialysis should bewary of herbs that do not listpotassium and phosphorus on thelabel. Also, contamination of herbalsupplements with such ingredients aslead, arsenic, gasoline and bleachhave been well documented.8,9
What can you do?
Learn about theingredients listedon the label. It’simportant to beaware thatmanufacturers arenot required to listpotassium andphosphorus on thelabel. You mayneed to call themanufacturers fornutrient analysis. Most important,talk to your medical professionalsabout their experiences with variousherbal products and theirrecommendations about using them.Use the Internet to gain productinformation. Finally, tell the medicalprofessionals on your kidney teamabout any herbal supplements thatyou are taking and report anyphysical and emotional changes thatyou have noticed since taking them. Itmay be the most important piece ofinformation that you provide to them!
References1. Eisenberg DM et al: Trends in alternative
medicine use in the United States 1990-1997: Results of a follow-up nationalsurvey. JAMA 280: 1569, 1998
2. Overview of Dietary Supplements. U.S. Foodand Drug Administration Center for FoodSafety and Applied Nutrition. April 3,2001.http://www.cfsan.fda.gov/~dms/ds-oview.html. (April 20, 2001)
3. Labeling of Dietary Supplements. U.S. Foodand Drug Administration Center for FoodSafety and Applied Nutrition. April 9,2001.http://www.cfsan.fda.gov/~dms/ds-oview.html. (April 20, 2001)
4. Gruenwald J, Bendler T, Jaenicke C (eds.):PDR for Herbal Medicines. Montvale, NJ,Medical Economics Co, Inc., 1998
5. Hauschildt E: Herbal Supplements CanAffect Drug Interactions In TransplantRecipients. January 31, 2001.http://www.docguide.com/news/content.nsf. (April 19, 2001)
6. Lewis C: Letter to Health ProfessionalsRegarding Safety Concerns Related to theUse of Botanical Products ContainingAristolochic Acid. U.S. Food and DrugAdministration Center for Food Safetyand Applied Nutrition. April 4, 2001.http://www.cfsan.fda.gov/~dms/ds-oview.html. (April 19, 2001)
7. Vanherweghem JL, Depierreux M, TielmanC et al: Rapidly progressive interstitialrenal fibrosis in young women:Association with slimming regimenincluding Chinese herbs. Lancet341:387, 1993
8. Edzard E: Harmless herbs? A review ofrecent literature. Am J Med 104:170,1998
9. Gerraghty M: Herbal supplements for renalpatients: What do we know? NephrologyNews & Issues p.12, March 2000.
Kim Stevens, RD, has been a renaldietitian for four years. She currentlyworks with Renal Care Group ofOshtemo in Michigan.
F
Good NutritionNaturally Safe
By Kim Stevens, RD
In the Winter “Quality ofCare” issue of FamilyFocus we included a list ofhigh potassium foods. Wewant to let our readersknow that anytime FamilyFocus prints lists of foodsit is recommended that youcheck with your owndietitian for what worksfor you, as every diet isindividualized for thatspecific patient.
Family Focus Volume 10 Number 3
7
What are over-the-counter drugs?
Over-the-counterdrugs are medicines thatyou buy without a doctor’sprescription. You may alsohear them called OTCdrugs or non-prescriptiondrugs. You can buy OTC
drugs from grocerystores, convenience
stores, gas stations,drug stores and even from TV ads andInternet Web sites.
The most common OTC drugs aremedicines for cold, cough, fever,headache, pain, constipation ordiarrhea. Other products that areconsidered OTC drugs are herbal ornatural medicines, vitamins, minerals,weight loss drugs and diet supple-ments. OTC drugs are very popularbecause you don’t need a prescription,you can find them in almost any storeand they’re usually cheaper thanprescription drugs.
If you or a family member haschronic kidney disease or kidneyfailure, however, you need to be verycareful with all OTC drugs. Justbecause you can buy these medicineswithout a prescription doesn’t meanit’s safe for you to take them. OTCdrugs are serious medicines and if youhave kidney disease or kidney failure,they can make you sick or cause life-threatening side effects.
Should I check with my kidney doctorbefore I start taking an OTC drug?
YES! Many medicines act differentlyor build up inside your body when youhave kidney failure. Ask your kidneydoctor about an OTC drug before youbuy the drug and start taking it. If youare already taking any OTC drugs,take time during your next treatmentto tell your kidney doctor or nursewhat OTC drugs you’re taking. It’s veryimportant that you tell your kidneydoctor if you’re taking any OTC drugsbecause:
� Some OTC drugs can change howyour prescribed medicines work.They can make prescribedmedicines weaker or make them toostrong. They can even stop yourprescribed medicines from working.
� Chemicals or electrolytes in someOTC drugs (like potassium, sodium,phosphorus, magnesium andaluminum) can build up in yourbody and make you sick or even putyour life in danger.
� The OTC drugs and your prescrip-tion medicines could “fight” insideyour body and cause serious sideeffects or allergic reactions.
� Some OTC drugs can causeincreased bleeding. If you have agraft or fistula, this could makeyour needle sites bleed longer afterdialysis.
Are there common OTC drugs that Ishould avoid?
YES! You should not take the OTCdrugs listed below unless your kidneydoctor tells you to take them.
� Alka-Seltzer, baking soda or otherbubbling medicines—high insodium, cause extra fluid gains.
� Milk of Magnesia or antacids—manyhave magnesium or aluminum thatcan build up in your body andcause nervous system problems.
� Enemas or laxatives—may be high inphosphorus; can also make youdehydrated and make your bodylose important chemicals.
� Aspirin—can cause increasedbleeding.
� Vitamins and minerals—vitaminsand minerals are also medicinesand some can make you sick if youtake them; take only vitamins yourkidney doctor prescribes for you.
� Diet supplements—contain highlevels of potassium and magnesium;check with your kidney doctor ordietitian about these products.
Do I need to tell my kidney doctor if I’mtaking herbs or herbal products?
YES! You should always tell yourdoctor if you are taking or plan on
taking an herbal product. Manypeople think that because herbalproducts are “natural” they’re safe.That is not true, especially for peoplewith kidney disease and kidneyfailure. Many herbal products can bevery dangerous for you. They maycause:
� Worsening of kidney disease � Loss of a kidney transplant� High potassium or phosphorus
levels� Increased bleeding� Changes in how your prescribed
medicines such as those for yourblood pressure work.
Does my care team need to know about“home remedies” that I use?
YES! You should tell your kidneydoctors and nurses about any homeremedies that you use. Most of thesehome remedies are probably safe.However, there’s always a chance thatyour home remedy could make yousicker. It could be full of potassium orsalt, or it could change how yourmedicines work. Your kidney doctorwill be able to tell you if your homeremedy is safe for you.
Remember—every OTC, homeremedy, herbal product or alternativetreatment (i.e., acupuncture,chiropractic treatment) that you usehas an impact on your personal healthand well-being. You can help yourselfby keeping your treatment teaminformed about the use of any of theseOTC drugs or treatments! F
Questions and Answers About Over-the-Counter DrugsBy Bobbie Knotek, RN, BSN
For People With Chronic Kidney Disease and Kidney Failure
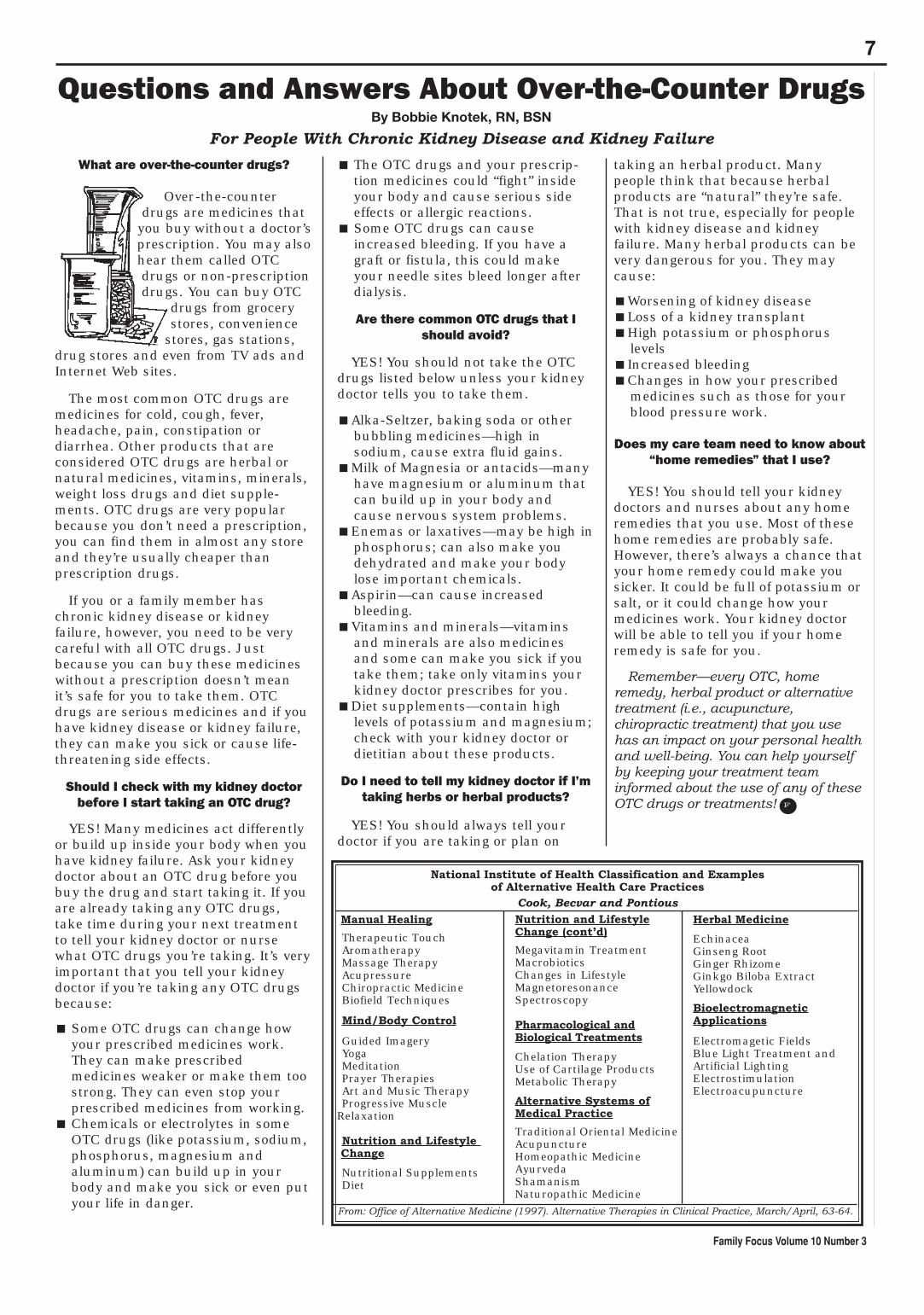
Manual Healing
Therapeutic TouchAromatherapyMassage TherapyAcupressureChiropractic MedicineBiofield Techniques
Mind/Body Control
Guided ImageryYogaMeditationPrayer TherapiesArt and Music TherapyProgressive Muscle
Relaxation
Nutrition and Lifestyle Change
Nutritional SupplementsDiet
Nutrition and LifestyleChange (cont’d)
Megavitamin TreatmentMacrobioticsChanges in LifestyleMagnetoresonanceSpectroscopy
Pharmacological andBiological Treatments
Chelation TherapyUse of Cartilage ProductsMetabolic Therapy
Alternative Systems ofMedical Practice
Traditional Oriental MedicineAcupunctureHomeopathic MedicineAyurvedaShamanismNaturopathic Medicine
Herbal Medicine
EchinaceaGinseng RootGinger RhizomeGinkgo Biloba ExtractYellowdock
BioelectromagneticApplications
Electromagetic FieldsBlue Light Treatment andArtificial LightingElectrostimulationElectroacupuncture
National Institute of Health Classification and Examples of Alternative Health Care Practices
Cook, Becvar and Pontious
From: Office of Alternative Medicine (1997). Alternative Therapies in Clinical Practice, March/April, 63-64.

Family Focus Volume 10 Number 3
8
T he Centers for Medicareand Medicaid Services(CMS), formerly known as
the Health Care FinancingAdministration (HCFA), reports thatmore than 230,000 Americans arebeing treated for kidney failure. I’mone of them. Learning how to livesuccessfully with a chronic illnesshas been the biggest challenge of mylife.
Chronic illness is different fromother maladies. Seemingly endless,its cure lies in some distant future.It can be life threatening or simplyannoying. You are forced to face liferather than face death; putting thebrakes on a once complacent,confident perspective and beingsent forth into the unknown.
Living successfully with anillness seems like an oxymoronand almost impossible to some. Iwas tossed on the flip side of lifeinstantly, seeing everythingthrough dark, distorted glasses. Irealized our society slices us intotwo distinct groups—the healthyand the not-so healthy, with thehealthy confounded as to how tohandle the not so healthy. I couldsee them but could they see me?
I was expected to at least appearwhole, and quickly, thank you.Stories about “overcoming,” or even“denying,” disability lurched out atme; running the marathon with oneleg, climbing Mt. Everest whileblind. Surely acts of heroism, butnot truly mainstream. These are the“disability superstars,” anointed torepresent all the nameless rest of uswho aren’t quite so brave, quite soresilient.
It sometimes seems that peoplewith disabilities have to dance just abit better and faster than others tomake other people feel good aboutthemselves. We’re made to feel guiltyjust sloshing through the day likeeverybody else instead of trying to be“more than.”
Kidney failure is deceptive. “Youlook terrific!” If you look well thensurely you are well, regardless ofhow you feel. We’re all products of aperfection-seeking childhood. Our
feelings about illness are rooted inour earliest memories; thoseworried parental whispers whensomething is “wrong.” We learnstraight from the womb to befearful of “different.”
Society follows a rigid set of rulesfor what is considered “normal.”“Be yourself,” yet we chastise theindividuality out of our little ones,lest they be shunned as“unpopular.” We prize individualitybut assess it within very narrowparameters, comparing ourselvesincessantly to the perfect ones inmagazines.
“Don’t be a crybaby!” We chideour children to blink back tears,hide their anger or disappointment,bite their lips and avoid eyecontact. Try to be brave. Ratherthan teaching them how to face andget past their fears, we teach thefine art of numbing, of self-paralysis—to not feel at all, to bealone with their boogey men. It’show we become grown-ups—todistance ourselves from ourselves.And it has a profound effect on howwe handle illness later. It traps usin fear. Culturally fanatic aboutstrength, we espouse the belief thatnegative emotions are weak.“Nothing ever gets you down,” or“You’re tougher than you think”only tighten our vise-like sense ofanxiety.
Think positive. O.K, but I was
You Can Be WholeBy Pat Donnelly
mad as hell when I found out I wasdealt a chronic illness. I couldn’tthink of a single positive thingabout it. I felt cheated, envious ofthe still healthy, absolute despairfor my own future and frightened ascan be. I wanted to run, to hide, butthere was no place to go. Andalways, there’s a fathomless,nagging loneliness.
I began to search for the “cure,”examining every treatment thatcame down the pike. I bought everyNew Age book, studied Easternreligions, learned to meditate,visualized, changed my diet, bulked
up on seaweed and learnedbiofeedback. Vitamin therapy,herbs, magnets, shamans;somewhere, someone musthold the answer, the key tocontrolling or even obliteratingmy illness. I thought I couldrise above it, cleanse my bodyof its frailties, overpower it withmy will. When I couldn’t, I feltdefeated, worthless, inept anddeserving to be sick. I waslooking for a way out ratherthan creating a way to stay in.
I blamed God. How could Helet this happen? What had I
done? How could I win back Hisfavor and perhaps, dream ofdreams, maybe procure a littlemiracle?
How foolish I was. I truly believedI was capable of controlling everyaspect of my life. Why not? That’swhat I’d been taught. When thatmiracle didn’t come, somewheredeep inside, a piece of me whisperedthat perhaps I didn’t deserve one.
Finally, a break came. Months ofsearching began piecing itselftogether into an almost crazypatchwork of ideas, bits and piecespilfered from this belief or thatopinion. I chewed up what I likedand spat out what I didn’t.
Reality is I'm not a Tibetan monk.I’m a Westerner whose mind iscluttered with insignificant culturalfacts and brimming with single,unrelated refrains to a thousand
Pat Donnelly has learned to live with her illness, in part, by focusing on her present quality of life.
continued on next page
9
Family Focus Volume 10 Number 3
Exercise. Move. Check with yourphysician first but don’t not do it. Youhave a million choices. I’m partial toyoga. Make an appointment withyourself and do it. Exercise countersdepression. Give it a shot.
Keep a journal. Keep lists with titleslike “I hate not being able to,” “Things Ilike about myself” or a “Goal fortoday.” I don’t care if it’s watering theplants or baking cookies. Walk to thekitchen and back 10 times, five times,once. Go. Start small and if you thinkit’s too small remember all the dayswhen you were well and you didn’t doa darned thing.
Hum. Sing. Listen to music like B.B.King, Chopin or whatever. Laugh. Cry.Let your emotions roll over you.Dance. Feel silly. Be silly. Get out. Goout to the woods and scream a fewtimes. You don’t have to proveanything to anyone but yourself.
Call somebody this week. Volunteerone hour anywhere. Everybody needshelp. If you can’t get out, knit, cook,write notes or make calls for someone.Giving has a remarkable way of gettingback. It feeds on itself. Say hello to aneighbor or a child. Open your heart.
Delay any important decisions for abit. You’re bound to have a differentperspective six months or a year fromnow. Be kind to yourself. It’s not thedestination but the journey.Remember that.
Focus on the quality of your life as itexists right now. We flourish when wesurrender to the way life is and not tothe way life should be. FranklinRoosevelt once said, “It’s commonsense to take one method and try it. Ifit fails, admit it frankly and tryanother. But above all, try something.”In the end, all you really need to do isto cooperate with life. It will, in shortorder, open itself up to you.
songs. I am undisciplined butresolute. It takes more than will toovercome an organic illness. Ithappens, but truthfully, aren’t wetalking super mystics here, peopleway more advanced than the averageJoe?
Face it. Chronic illness evolves.Assume it’s not anything you alonedid or did not do. Assume it was allpart of an organic misstep that youhappened to be involved in—a cosmicthing. Let’s move toward dumpingyour guilt. Forget and forgive the “ifonly.”
You can’t reason your cure. I’m allfor miracles, but I can’t wait for mine.I have to find ways of living that existfor me today. It’s only in this momentthat I have any pretense of control,and that’s because the goals for thisday and this hour little influence thegreat scheme of things. They are goalsfor the now. I don’t have a monopolyover myself, my own health or mypotential cure.
This is my reality, and I cannotchange it, despite all the goodintentions of every guru I’ve ever met
or read. Our reality is the “is” of truththat we all share. You can, however,change your reaction to, yourperception of your reality and devise anew set of insights and ways of livingyour life for yourself. You can redirectyour energies and effect change,especially in the process andexperience. That’s the essence of life.Tomorrow will take care of itself.Today is alive.
Living with life as it really isprovides the true path to healing andliving successfully with a chronicillness. You’ll see the landscape is notsimply composed of black and white.There are nuances in nature, subtlevariances that defy accepted or
normal classifications. Nature ischange, truth in an inconsistentpresent.
Sometimes it seems hard toimagine our way through, to ever finda way to live with imperfect health.We become so identified with theillness that we lose sight of ourselves.Categorized by labels, our names arelost to our conditions. This worlddefines us by what we do andmeasures and evaluates us by ouraccomplishments. Illness uproots us;we must find new meaning for ourself.
And, of course, there’s that issue ofcontrol, or lack thereof, that sodefines our culture today. Yet facingloss and pressing through anger andgrief and coming out the other sidewhole, embracing change as the stuffof life, is to triumph. You can bewhole again. Control and change arelousy bedmates. You either commit tocontrol or to change, to stuffing youremotions or experiencing them.Control is stagnant; change isprogress. Remember that allemotions have value. All emotionshave truth.
Let’s say you have kidney failureand you’re feeling pretty low.Depressed. Tired. Angry. Frustrated.Scared. How can you get from pointA to point B? What’s the secret? Howcan you create new dreams andenrich your days? How can you go tosleep at night and not be afraid of thedark?
Start now. There is a distinct mind-and-body link that can be honed andused. Breathe. Fill your lungs deeplyand then let go. Visualize yourselfcalmer and under less stress and inless pain. Systematically relax eachpart of your body until you arecompletely at ease. Imagine and go toa quiet place in your mind. Visualizechanging what you can control andletting go of anger and resentment.See yourself happy.
Be aware of your pain. Its severitycan be managed. Your fear of painmight actually be a bigger pinkelephant than the thing itself. Pain isas much a part of life as is joy. Theyare opposite sides of a coin, equallyvaluable and equally viable. They aretruly a part of the spirit of ourexistence.
F
You Can Be Whole continued from page 8
Sometimes it seems
hard to imagine our
way through, to ever
find a way to live with
imperfect health.
Focus on the quality of
your life as it exists
right now. We flourish
when we surrender to
the way life is and not to
the way life should be.
and lifestyle choices and are taughtby skilled professional volunteers, aswell as patients and family members.
The RISE Program was developed toencourage individuals with kidneydisease to return to meaningfulactivity, which may include resumingdaily routines, employment, continu-ing education and volunteering.Individuals learn decision-makingskills to help them pursue the optionsavailable to them to maximize theirquality of life. Sessions includeinformation on interviewing skills,resume writing, importance ofexercise, Social Security and muchmore!
Peers Program
The NKF Peers Program providesspecial training to people with chronickidney disease and transplantrecipients and their family memberswho have made a positive adjustmentto their chronic illness with the goal ofhaving them provide support to otherswho are new to treatment. Peersempower individuals with chronicillness to become active members of
their health care team and to assumeresponsibility for their own healthcare.
The Patient Services Committee hascreated suggested guidelines to helpthe NKF affiliates develop programs inaddition to those listed above. Some ofthe guidelines that have beendeveloped include those for emergencyfinancial assistance programs,establishing a discount medicationprogram, implementing a nutritionalsupplement program andimplementing an educationalscholarship program. Other programsoffered by some Patient ServicesCommittees of local NKF affiliatesinclude medical alert jewelry, campsand camp sponsorships andeducational seminars.
This information about PatientServices provides a glimpse into theactivities and commitment of ourhardworking national committeemembers and staff and the affiliatesthat provide these programs. Thecommittee wants you to know thatMaking Lives Better is the true focusof all of the programs. For moreinformation about any of theseprograms, please contact your localNKF affiliate office or the NationalOrganization at (800) 622-9010.
Family Focus Volume 10 Number 3
10
News from the National Kidney Foundation’s Patient Services Committee
T h e M o r eY O U K N O W
The NKF’s Patient ServicesCommittee identifies andevaluates the needs of people
with kidney and urinary tract diseaseand organ transplants and the needsof their families. Once it has takenthese diagnostic steps, the committeethen develops programs to addressthe identified concerns.
National Kidney Foundationprograms are developed by obtainingthe input of the 51 NKF affiliatesaround the country. All of theprograms mentioned below may notbe available in your specific locationdue to the size and particular focus ofeach affiliate. We want to keep youinformed of the current programs andwill highlight a few of them here.
KEEP is ahealthscreeningprogramoffered inlocalcommunitiesto identify
individuals who are at an increasedrisk of developing kidney disease,inform them of their risk andencourage them to seek appropriatemedical attention that may prevent ordelay the onset or progression ofkidney disease. Goals of the programare early detection and interventionand the prevention of kidney diseasethrough treatment of risk factorssuch as hypertension and diabetes.Local NKF affiliates select the KEEPscreening sites and work with trainedvolunteers to conduct the program intheir communities.
Individuals withkidney disease, boththose currently ondialysis or thoseconsideringtreatment options,and their family
members can learn about kidneydisease, treatment options, nutrition,coping and other related informationat a People Like Us, Live! program.Sessions provide unbiasedinformation and the emotionalsupport needed to make treatment
F
MAIL BOX
Dear Donor’s family,
Hello. My name is Kelly and I am 14 years old. First off Iwould like to say how sorry I am for your loss. I hope it willcomfort you to know how much better I feel after receiving akidney from your loved one. Everyone is amazed, because itwas a PERFECT match. EVERYTHING matched up. I feel betterthan I have in YEARS. I just got out of the hospital five days ago.You have been in my prayers ever since I got that call that Iwas going to get the transplant. It was surprising because Ihave only been on the list for six months and the average is three years. Itwas a very unexpected thing that I am VERY grateful for.
I hope this will help you with your loss. I am very grateful for this gift thatI have been given. God bless you and your family. F
Kelly
Family Focus Volume 10 Number 3
11
Hemodialysis therapy hascome a long way since thefirst outpatient dialysis
program was established in Seattle inthe 1960s. New dialyzers andhemodialysis machines allow dialysisfluid to flow faster, resulting in betterremoval of toxins from the blood.Severe nausea and fatigue caused bydialysis don’t occur as often as theyused to due to changes in the dialysisfluid chemicals and new dialysismachines that control the amount ofwater removed. Measurement of theflow of the blood through dialysisgrafts and fistulas allows early repairof accesses that are not working wellbefore they become completelyunusable. Current research is beingdone in two areas: increasing thenumber of dialysis treatments given toa patient each week, or increaseddialysis frequency, and improvementsin the design of hemodialysiscatheters.
Increased Dialysis Frequency
Undergoing three hemodialysissessions a week seems hardenough. Increasing the number oftreatments hardly seems like animprovement. However, manyexperts point out that healthykidneys clean the blood 24 hourseach day, seven days a week, sowhy should we expect that threetreatments a week of only three tofour hours each would be enough fordialysis patients?
Carl Kjellstrand, MD, PhD, FACP,FRCPC, an expert in daily dialysistherapy, points out that after eachdialysis session, waste products andfluid build up in the body until thenext treatment. Since the nexttreatment is usually two or three dayslater, toxins and fluid reach highlevels, only to be rapidly removedduring dialysis and then the cycle isrepeated all over again. It looks likethis constant up and down pattern ofwaste products and fluid can, overtime, cause damage to the heart,brain and bones. Also, many of thecommon side effects of hemodialysissuch as cramps, sudden drops inblood pressure and the “washed-out”feeling that many experience arecaused by the rapid removal of thesetoxins and fluid. Daily dialysis forshorter periods of time or with slowerblood flow rates may do away withsome of the side effects of dialysistreatments. Many people would rather
have a short dialysis treatment everyday and feel well afterward thanhave only three treatments a weekand feel sick and tired after eachone.
Most people who have dailydialysis have better blood pressurecontrol and need fewer bloodpressure medicines. Phosphate levelsare often lower and the red blood cellcount is usually higher in those ondaily dialysis. Perhaps mostimportant, people who are on thistype of dialysis tend to feel better, aremore active and have a greaterenjoyment of life.
Daily dialysis may be done indifferent ways. Some units have youcome to the dialysis unit for shortdaily treatments. Other centers usenightly dialysis in special unitswhere you may sleep while receiving
treatment. You or your partner canbe taught to operate the dialysismachine in the home for shortdaytime or overnight dialysissessions. Also, some centers use theInternet to connect dialysismachines in the home to the dialysisunit where the treatment is checkedby trained technicians.
Daily dialysis is, in fact, moreconvenient than traditional dialysisin that it may take place in thehome. It also allows you to takefewer medicines, have a lessrestrictive diet and fluid limit andfeel better, while possibly reducingheart and bone disease. At present,one of the main reasons that dailydialysis isn’t done more often is thatMedicare and insurers don’t want topay for it.
New Hemodialysis Catheters
Many people need dialysis before agraft or fistula is ready to use, orthey have problems with their graftor fistula and need to use a dialysis
catheter. Sometimes those ondialysis run out of places to put newgrafts and must use catheterspermanently. Unfortunately, thesecatheters may cause life-threateninginfections. In addition, blood flowthrough catheters may not be goodenough to clear waste productsadequately from the blood.
New dialysis catheters have beenmade that have specially shapedtubing that improves blood flow.Some catheters are made out ofplastic containing antibiotics orsilver, both of which may helpprevent infections by not allowingbacteria to grow. Another way toprevent infections is to have thewhole catheter placed under the skinso it is harder for bacteria to enter.Special dialysis needles are placedthrough the skin into the catheter. Itwill take some time before we know ifthese catheters will do a better job.
Though hemodialysis is life-sustaining for hundreds ofthousands of patients, significantcomplications are an all too commonoccurrence in dialysis patients. Newcatheter designs and increased useof daily dialysis are revolutionarychanges with tremendous potentialto improve your quality of life. Theseadvances in the science andtechnology of dialysis may soonallow hemodialysis patients to livelonger, healthier and more satisfyinglives.
References:The benefits of daily dialysis are wellreviewed in the followingreferences:
Kjellstrand CM, Ing T: Daily hemodialysis: History and revival of a superior method. ASAIO J 44:117-112, 998.
Woods J, et al. Clinical and biochemical correlates of starting 'daily' hemodialysis. Kidney Int 55:2467-2476, 1998.
Pierratos A: Daily hemodialysis: Why therenewed interest? Am J Kidney Dis 32:S76-S82, 1998 (suppl 4)
Buoncristiani U, et al. Reversal of left ventricular hypertrophy in uremic patients by treatment with daily hemodialysis. Cont Neph 119:152-156, 1996.
Sanford Reikes, MD, is an assistantprofessor of internal medicine at St.Louis University School of Medicineand the associate medical director ofSt. Louis Renal Care, LLC. F
A L K A T T H E F U T U R E
What’s New in HemodialysisBy Sanford Reikes, MD
Teresa Hernandez receives her dialysis treatment at Mt. Sinai Hospital in New York City.
12
Family Focus Volume 10 Number 3
F I T N E S S
Fluid Removal Fiesta: How I Learned to Love to SweatBy Monique Janelle London
This article will give you yet another good reason to adopt a regular exercise program. Remember to check with your physician before embarking on a new exercise regimen. Read on!
Ithought sweat was disgustingbefore I developed kidney failure.After all, I’m a girl and girls don’t
sweat! We have make-up, hairdos anddelicate clothes to protect. Sweat isnot pretty; it stinks; it certainly won’tattract a guy. It doesn’t feel clean tosweat. How could it be clean, whenyou always have to wash the clothesyou have worn when sweating? So Itrained myself from an early age not tosweat. I had the appropriate light-weight clothing, the air conditionerand the iced tea—all ready to launchan attack at any hint of a glisten.
Then I developed kidney failure. Iwas told the goal was to gain less thantwo pounds between hemodialysistreatments. But what about thosedays when I was ridiculously thirstyfor no apparent reason? When I took asip, I would put the drink back in therefrigerator and try to walk away, but Iwould make a U-turn back and gulpthat precious fluid down! What aboutwhen I would stingily pour out a tinyglass of cranberry juice over ice, thenfeel that cold explosion of flavor as itflowed over my parched throat, andpour myself another and another andanother?
I had blown the fluid restriction onlots of days before I knew it. I couldtell. My eyes were puffy. I failed my“ring test,” which is when the ring Iwore that fit loosely on my finger justafter dialysis was too tight to remove.Whenever I failed the “ring test,” Iknew it was time to take action. But atfirst, I didn’t know what action totake. I just had to try to not drinkanother DROP of fluid until the nextdialysis session. Rarely was that plansuccessful. I would step sheepishlyonto the scale at dialysis and realizethat I had a hellish session ahead ofme—one filled with plummeting bloodpressure and plenty of cramps as Itried to remove too many kilos of fluidin such a short time.
Then it dawned on me one very hotday. Sweat is fluid—fluid that I couldget rid of before my next dialysistreatment even if I couldn’t urinate. Istarted changing my attitude aboutsweat. I tried to convince myself, “It’snot disgusting; it’s beautiful!” I askedmy dialysis nurse what exactly is insweat. She told me that sweat
includessodiumand asmallamount ofpotassium.She saidthat skinis actually
like a third kidney in that it can filterout some toxins through sweat. Ithought, “Hallelujah!” Why had no onetold me this before? I envisionedgetting a sweat box for my living roomwith just my head sticking outthrough a hole, like I’d seen on I LoveLucy and in cartoons. Oh, theliberation I could get from this nuggetof wisdom!
I sprang into action. I startedwearing more clothes than I needed towear. I kept the heater on in my caruntil I could feel myself start to sweat.I took long walks and bike rideswearing extra sweatshirts and awindbreaker. Sometimes I would come
home drenched from sweat. True, Ihad to do more laundry, but my ringturned easily on my finger. I waspassing the “ring test” with flyingcolors. I was able to arrive at dialysisonly a pound or two over my dryweight even though I was drinkingmore fluid. I felt much better. My labresults were great. Sweat was my newbest friend.
I still enjoy sweating even now that Ihave a kidney transplant. It feels goodto know that I am cleansing my body oftoxins when I sweat. When I’m sweat-ing a lot, I always keep track of myweight to make sure I’m not losing toomuch fluid and getting dehydrated.Usually, I’m not. Sweat is beautiful.
Monique Janelle London lives in SanFrancisco, California. She waspreviously on dialysis and now has atransplant. She works at DaVita, aDialysis Provider. Ms. London is anavid exerciser.
F
Examples of Alternative Health Care PracticesBy Dale Ester
N V C T E V S R C K I T C G Q F X U O N P S M M L A M E M D B O Y H V M I X M S G K U I K V V W A N T H E A E F E N A P E K I E I B T T X G J I K L I L Q T P N D J G N R U D I D E H P N T D R G C O L D J X T N E U M E N L S A U U D I C E F A Y O G A N O T A E I C Y M N R P M I Y C E V A S E T I V E U R R K X X P P D R P W Y L O K E M P Q L J I L S E A D R C H Q T P W S A I R R T L E P N L D A S E F W T H E L T E U O D E J I P F M L W A O X A H P W R Q C F N I A E R E I M Y V Z L R J F A Y N E R C T E P I E F T A M Z X M A P C O L A Y F Y K B G I H A T R H T U A H W R T I K S I I L U T N A S P G L P E A K C N X I E S I T B O P Q B E H O N I C R O T E A I I R A S L O I C S L L C C A O C S I Y L W T N A O Q N U R K Y N J R C M M A A Y I C C M O L P O C F O R G L S B E Q E S A D S Y E E E N L S P U S V E A I C B S I E J E T Z I I H Y E W D E D H O D U L P A Y U R D R B W W T A G O I R R N T S M O U I N I T M I U I E R E M H I G O C N T O H M P O H C I B P C E T G D A N C L G H E K E Z C Y G S M H D U E L C I T Z I T I R N R C M L I T H X H C V A I Y K E M J L H A E L A N U R G A N T O O O R N Y T H T Y I E N V N S B A Z N T O E G T K T K U R W O E R U E Z I K N T S C E T I X T A O D B C U I R G R V D N Y T B A K Q O N U O B S A K G G I W I L A N M A M E K O P A A S E Z E W G M G O I A E N A O O K T E T U S E O F C A R T I L A G E P R O D U C T S R I Q N D I I E U E I H K T P M A S S A G E T H E R A P Y A K G H O D D F M E M O Z I H R R E G N I G M S I N A M A H S L Y O C X A O X E N I C I D E M C I H T A P O E M O H Q Z E B E Q R E R I C H C U O T C I T U E P A R E H T Y U L S E K C M H A P T B H I P N O I A Y M M J A C U P U N C T U R E V K G T C C R M A K H B I X A L O Z B L U E L I G H T T R E A T M E N T S Z O Y P O C S O R T C E P S E C N A N O S E R O T E N G A M M W
WORDS TO SEARCH:
ACUPRESSURE ACUPUNCTURE AROMATHERAPYARTANDMUSICTHERAPYARTIFICIALLIGHTING AYURVEDABIOFIELDTECHNIQUESBLUELIGHTTREATMENT BODYCONTROL CHELATIONTHERAPYCHIROPRACTICMEDICINE ECHINACEAELECTROACUPUNCTURE
ELECTROSTIMULATION GINGERRHIZOME GINKGOBILOBAEXTRACT GINSENGROOT GUIDEDIMAGERYHERBALMEDICINEHOMEOPATHICMEDICINEMAGNETORESONANCESPECTROSCOPYMANUALHEALING MASSAGETHERAPY MEDITATIONMEGAVITAMINTREATMENT
METABOLICTHERAPY MINDNATUROPATHICMEDICINENUTRITIONALSUPPLEMENTSPRAYERTHERAPIESPROGRESSIVEMUSCLERELAXATIONSHAMANISMTHERAPEUTICTOUCHTRADITIONALORIENTALMEDICINEUSEOFCARTILAGEPRODUCTSYELLOWDOCK YOGA
(answers can be found on page 16)
Family Focus Volume 10 Number 3
13
� Set realistic expectations forinvolvement
It is very important to be realisticabout how involved and independentyour child can be in home dialysis.Your expectations should take intoconsideration your child's learningabilities and motivation. Awareness ofyour child's current abilities will helpyou determine which tasks your childcan be successful in doing alone orwith your assistance and which tasksyou will need to do for your child.When skill problems are identified,the clinic nurse can often help teachyour child.
It is equally important to be awareof your child's skill strengths. It islikely that your child will be interestedin participating in aspects of thedialysis routine that he or she is goodat doing. It is also possible that yourchild may be better able than you todo some of the dialysis tasks.
Being aware of your child's feelingsregarding the benefits and drawbacksof independence in dialysis will allowyou to use strategies to decreaseunrealistic fears he or she may haveabout doing dialysis alone. Finally, itis important to reevaluate yourexpectations for your child'sindependence and participation as heor she grows and develops.
� Organize the homeenvironment to boost successful
participation
Home dialysis can be a complicatedand time-consuming responsibility.You will be able to increase yourchild's motivation and success indoing dialysis independently ifsupplies are kept together in aconsistent location, the room that isused during the hook-up is quiet and
calm and you insist that dialysis bedone at approximately the same timeeach day. Use of these strategies givesa child a sense of comfort, control andconfidence about safety and successwith home dialysis.
� Provide regular enthusiasticpraise and occasional tangiblereinforcement for adherence
Withoutobtaining yourchild's interestin participatingin homedialysis, there isno hope ofincreasing thechild’sinvolvement.You can get and
keep your child’s interest by providingreinforcement that is rewarding adesired behavior. Since reinforcementof desired behavior leads to itscontinuation and improvement orincrease, it is particularly importantto pay attention to the kinds ofreinforcement that are meaningful toyour child.
It is important to praise a child'sattempts at increased independencerather than waiting until he or she isfully successful. Many children havebehavioral improvements when theyare given reinforcement in the form ofenthusiastic praise for their efforts.Other children need tangible rein-forcement such as toys, food treats orprivileges for behavioral improvementsto occur.
Unfortunately, performing dialysisis not a very rewarding task. In otherwords, staying healthy is often not astrong enough reinforcement toencourage adherence to dialysis. In
fact, performing dialysis ofteninterferes with a child's ability toparticipate in more enjoyableactivities, and for many children,dialysis is perceived as an unpleasantor disagreeable experience. Therefore,you will need to give praise andoccasional rewards. This will helpyour child achieve involvement andindependence that is age-appropriatein home dialysis. If serious adherenceproblems surface, you may want toconsult with the unit social worker orask your child's health care providerto refer you to a therapist who canhelp you identify your child’spreferred rewards.
� Provide a safety net ofsupervision to assure that the
treatment regimen is carried out
It is important to recognize that achild's interest in participating indialysis treatment will wax and wanethroughout childhood, adolescenceand early adulthood. You will need tomonitor this and vary your interven-tions to increase participation andindependence as needed. Ultimately,however, parents need to provide asafety net of supervision to assurethat dialysis is being completedcorrectly and consistently.
In summary:• Be realistic about your
expectations.• Organize your home environment
to encourage and support yourchild's successful involvement.
• Give your child positive feedbackabout his or her involvement andindependence.
• Always supervise.
How to Increase Your Child’s Adherence With Home DialysisBy Arlene C. Gerson, PhD, and Barbara Fivush, MD
Adherence is defined by how well patients follow medical advice. Most parents know thatadherence has health benefits and that non-adherence usually results in health problems.Unfortunately, children and adolescents often do not recognize the relationship between their
behavior and their health. As a result, many children do not participate eagerly in their medical self-care. Infact, when home dialysis is needed, parents frequently have problems getting their child to follow thedoctor's orders. This article will suggest strategies to improve your child's adherence with home dialysis.
F

14
Family Focus Volume 10 Number 3
Government Support of MedicalResearch Benefits Kidney Patients
By Dolph Chianchiano, JD, MPA
The National Kidney Foundation(NKF) Office of Scientific and PublicPolicy, in addition to its advocacy forMedicare and Medicaid programs thatbenefit kidney patients, is activelyinvolved in generating support for thekidney research programs of theNational Institutes of Health (NIH), anagency of the U.S. government.
The principle organization suppor-ting kidney research at the NIH is theNational Institute of Diabetes andDigestive and Kidney Diseases (NIDDK).A 17-member Advisory Council decidesfunding priorities for the NIDDK. JudgeLevan Gordon, a member of the Boardof Directors of the NKF, is also amember of that Advisory Council.NIDDK is supporting many researchprojects that pertain to the well-being ofdialysis patients.
The Hemodialysis Study, forexample, is designed to investigatewhether higher levels of dialysis doseand changes in dialysis flux improvehow long those on dialysis live and if itreduces their hospitalization. Thereare 15 centers representing 900patients that are involved in the study.The study began on June 1, 1995, andthe final results should be available byNovember 2001.
The goal of the Vascular AccessClinical Trials Network, which wasdeveloped last year and is funded bythe NIDDK, is to study ways todecrease hospitalization for those ondialysis due to vascular accessproblems. Problems related to vascularaccess account for 15 to 25 percent ofthe hospital admissions for people ondialysis in the United States. TheVascular Access Clinical TrialsNetwork was begun because there havebeen few rigorous studies that usemedications to prevent vascular accessfailure, and because there are newtherapies on the horizon that shouldbe thoroughly evaluated. The researchon vascular access, which will soon beunder way, will be conducted at sixcenters: University of Texas SouthwestMedical Center (Dallas), Maine MedicalCenter, University of Iowa, ClevelandClinic Foundation, Duke UniversityMedical Center (Durham, NorthCarolina) and Boston Medical Center.Ultimately 2,000 patients will beinvolved in this project.
Dr. Alan Christensen at theUniversity of Iowa has been funded bythe NIDDK since 1995 to study thequality of life of those with kidneyfailure. His research examines whethercertain psychosocial characteristicsmake some people better candidates forcertain kinds of dialysis therapy. He isalso identifying personal characteristicsthat are related to adjustment for thosewith a kidney transplant. AnotherNIDDK grant has been awarded to Dr.Ashwini Sehgal at Case WesternReserve University in Cleveland, Ohio,for the project, “Overcoming Barriers toAdequate Delivery of Hemodialysis.”This study will explore whether patient-provider communication is a barrier toadequate delivery of hemodialysis, andit will test interventions that couldimprove this communication. Inaddition, NIDDK has provided grants toVanderbilt University in Nashville,Tennessee, for a study of malnutritionin people on dialysis, and to theNorthern California Institute ofResearch and Education for researchon exercise for those on hemodialysis.
An additional NIDDK study iscurrently in the planning stage. Thistrial will compare the outcomes ofpeople who are on daily hemodialysiswith those who receive hemodialysistreatments three times a week. The costof the study is being shared by theCenters for Medicare and MedicaidServices (CMS), formerly known as theHealth Care Financing Administration.The trial will document the cost of dailydialysis so that a payment policy can bedeveloped for it.
It is clear that NIH-financed researchis paving the way for better treatmentof kidney disease. However, funding forthe study of kidney disease competeswith demands for research on otherimportant health problems, such asAIDS, arthritis and cancer. We need tocontinually remind members ofCongress that breakthroughs in ourunderstanding of kidney disease and itstreatment are vital. If you are willing tohelp get that message across todecision makers in Washington, pleasecall the National Kidney FoundationOffice of Scientific and Public Policy at (800) 889-9559.
Dolph Chianchiano is NKF’s director ofscientific and public policy. F
Good Luck or GoodManagement
By Richard Dulebohn
This article was written in response to “Whatis Quality Care?” which was featured in theWinter 2001 issue of Family Focus.
Ifeel cold dread knowing againtoday that I must go…to what?Will it be another day like that?
Wheeled down into the icy, night-marish, dialysis dungeon where, itseemed, civilized life came to a halt. Iwas manacled to the rack; a beepingred-eyed monster sucked my bloodand then spat it out. Masked, robedimps with blue hands crept aroundpinching my arm and mutteringincantations. Later, I felt weary relief,not that my life was reprieved foranother treatment—just that theordeal was over.
Yet I have felt the wonder of being ina well-run, comfortable unit in adistant city, like a dream where thereis no dread of dialysis, no halted life,no stress. I have rejoiced in my goodluck. In my more lucid moments, Irecognize it’s not luck or anythingmysterious that results in this type ofunit. It is good management.
Good managers can be found. Theyneed to be told what their job involves,to stay within the budget and to followthe prescription for each patient’streatment. Additionally, they must seethat the time the patient spends intheir care is pleasant. The goal shouldbe to provide a non-jarring ambiencethat allows the mind to drift andmeditation to happen. Two types ofchanges, one involving the facility andthe other the personnel, are needed tocreate this type of environment.
Architectural and mechanical
Managers should have budgetedfunds to keep machines and dialysischairs in repair and to make changesto things that jar or irritate people inthe unit. The following are just a fewexamples of annoying deficiencies thatI have observed in various clinics.
� The wheelchair accessibility is toodifficult.
continued on next page
Richard Dulebohn relaxes in front of hishome in western Oregon
15
Family Focus Volume 10 Number 3
� There are no nurse or attendantcall buttons.
� The chairs are poorly designed andconstructed so that in the positionfurthest down, a little squirming causesthe chair back to drop and the footrestto rise abruptly. Chair footrest’s adjust-ments are faulty, as they often requirethe use of stools to hold them up.
� The automated blood pressure cuffworks on only a few chairs.
� When chair backs are lowered,patients face dazzling ceiling lights.This strains the eyes when reading abook or watching TV.
� No diversion other than TV isoffered.
� Ventilation and air-conditioningproduce cold drafts.
� Patients have to carry blankets andother personal items from home eachtime they come to dialysis becausestorage space is unavailable.
� The waiting room is too small anddrafty because the entrance door opensdirectly to the street. Waits in thoserooms are long.
Things like these are easy to spot andrepair. One just has to look!
Personnel selection and education
Even with low staff turnover, staffselection and training are difficultbecause every patient has his or herunique problems and the personnel
have their own strengths andweaknesses. The manager must moldthem into a team and pass a positiveattitude on to both.
A nurse assesses the patientphysically before and after eachtreatment. At that time, the nurseshould also monitor the technician’sfinesse and gentleness in handling theneedles and the patient’s access. It isalso the nurse’s responsibility to assessthe patient’s emotional condition andmorale and then advise the technicianif the patient needs special attentionthat day or about conditions to watch
for during blood pressure checks. Forexample, the technician can offer a cupof ice, help arrange pillows or blankets,assist with the adjustment of the chairor provide earphones, TV remotecontrol or a portable phone. Thusguided, a potentially good technicianwill learn to ask, “Is there anything elseyou need?” before leaving.
The manager should arrange informalstaff conferences to emphasize the needto treat patients with respect andcourtesy. This should include a reviewof the clinic’s policy on noise, radio andTV. Loud personal conversationsbetween patients and even staff caninterfere with healing. The socialworker, with the patient’s consent,should also brief the staff on relevantpatient needs or preferences that havebeen identified.
Good management of dialysis unitscan assure that all patients receive thetype of stress-free care they deserve.
Mr. Dulebohn was born in 1919. Hepracticed architecture and engineering inOhio, California and Idaho. He retired in1981, married Mary C., and moved to amountain cabin in northern Idaho. Afteran operation to replace a dissectingaorta in 1992, he lost kidney functionand began hemodialysis. The Dulebohnsmoved to western Oregon in 1999.
Ihave been on dialysis for four years and the firsttwo of those were awful for me. I got cramps, had abadly bruised arm and was often dizzy and
nauseous. My strength, ability to work and play, finan-cial circumstances, physical appearance, sexual driveand outlook on life were changing. I asked "why me" andfelt extremely sorry for myself. I avoided family andfriends, cried a lot when I was alone and I only did whatI had to do for my daughter. I was in a deep depression.
My attitude began to change, however, and as aresult, things became easier to handle. While it iscertainly true that I would be much luckier if I hadnever gotten kidney disease, it could be a lot worse. If ithad been my heart or another organ rather than mykidneys that failed, I would probably be dead now.Thank goodness for the inventors of dialysis machines.
I have learned to appreciate so much that I once tookfor granted. I used to worry about everything, but I havecome to realize that worrying only wastes time. It won’tchange the outcome. Arguing over trivial things withloved ones also seems foolish. Who cares whoseviewpoint is right? Just think of each other’s feelingsand drop unimportant issues. Every day we need to actas if it may be the last time we will see our loved onesand never part ways angry or with a bad word. We neverknow what will happen in this world and to live withregrets forever would be unbearable. I am so grateful formy loving family and friends who are there for me nomatter what happens.
I am also extremely grateful for Dena, my angel, whohas recently come into my life. I was at my sister’s homein December 2000 at the same time that Dena wasvisiting. She had noticed that I was ill and called mysister the next day to ask about me. When she discov-ered that I needed a kidney transplant she decided to tryto donate one of her kidneys to me. She wanted to seethe results of being a donor in her lifetime rather thanwaiting until after her death. I was speechless! What doyou say to someone who offers you health after 10 longyears with kidney disease and four years on dialysis? Iwill soon be free of dialysis because of the kind-heartedselflessness of Dena, who is a 28-year-old mother oftwo.
Dena’s response to my words is "How can people notdo this…give up a few months in order to give someoneso much?" It isn’t just giving to one person but also to aspouse, children, parents, siblings and friends. Denahas said that her scar will be a reminder that she notonly gave life to her two boys but to me as well. She isGod-sent. If only more people were like Dena, my angel.
The transplant surgery was a success and both Donnaand Dena are doing well. Dena was released from thehospital only four days after the surgery to remove herkidney, and she returned to work 26 days afterward. Sheis now interested in becoming a bone marrow donor.Donna had some initial rejection of the kidney but is nowoff dialysis. Dena 2, the name Donna has given her newkidney, seems to be adjusting.
Good Luck or Good Management continued from page 14c
My AngelBy Donna Joy
T R A N S P L A N TRAANSP
N
LA
TN
Mr. Dulebohn has experienced well-manageddialysis units and knows what a valuabledifference they make for the patient.
F
F
RT R A N S P L A N T
SPLANT
16
National Kidney Foundation30 East 33rd StreetNew York, NY 10016
P O E T R Y CORNER
GivingBy John (Buddy) Muzzy
For the past several years her father had a routine
Every day he had to be hooked up to a dialysis machine.
It ached her heart to see her dad go through this each day,
But there was nothing she could do, much to her dismay.
The doctors ran all kinds of tests on his kidneys,
to see what could be done,
They concluded he could live a normal life, if
he had a good one.
They ran compatibility tests with the family,
including her sister and her brother,
The doctors decided the donor should be Debbie and no other.
What a decision she had to make,
Would she someday need the kidney they wanted to take?
But this was her dad who made sacrifices for her
throughout the years,
When she thought about her decision it brought her to tears.
What better way to show the love that she had,
Than to give the "Gift of Life" to her cherished dad?
So on April 14, 1993, this courageous young lady
showed the ultimate meaning of love,
Now they’ll both lead productive lives with God’s
blessings from above.
What an inspiration she has been and as long as she’s living,
She’ll always be happy, because she knows the joy of giving.
DialysisBy Jose A. Carmona
Dialysis
Crimson runs wild through
Plastic veins sewn to
The appendix of an arm
Artificial system to
Maintain a life gone by
Lent to a world
Of internal suffering
Stampede of broncos
Inside an enclosed valley
Of desperate hope.
F
F
Answers to the Words Search Puzzle on page 12 (Over,Down,Direction)
ACUPRESSURE(25,12,N) ACUPUNCTURE(11,28,E)AROMATHERAPY(13,21,NW) ARTANDMUSICTHERAPY(3,22,NE) ARTIFICIALLIGHTING(1,5,SE)AYURVEDA(29,9,N) BIOFIELDTECHNIQUES(29,27,N)BLUELIGHTTREATMENT(10,29,E) BODYCONTROL(2,17,NE)CHELATIONTHERAPY(26,28,NW) CHIROPRACTICMEDICINE(3,1,SE)ECHINACEA(27,26,NW) ELECTROACUPUNCTURE(22,5,SW)ELECTROSTIMULATION(26,6,S) GINGERRHIZOME(13,25,W)GINKGOBILOBAEXTRACT(25,21,NW) GINSENGROOT(1,11,SE)GUIDEDIMAGERY(14,1,SW) HERBALMEDICINE(1,7,SE)HOMEOPATHICMEDICINE(19,26,W) MAGNETORESONANCESPECTROSCOPY(28,30,W)MANUALHEALING(24,1,S) MASSAGETHERAPY(8,24,E)MEDITATION(27,1,S) MEGAVITAMINTREATMENT(23,1,S)METABOLICTHERAPY(30,24,N) MIND(18,6,NE)NATUROPATHICMEDICINE(20,1,SW) NUTRITIONALSUPPLEMENTS(1,22,NE)PRAYERTHERAPIES(7,24,NE) PROGRESSIVEMUSCLERELAXATION(27,27,NW)SHAMANISM(22,25,W) THERAPEUTICTOUCH(16,27,W)TRADITIONALORIENTALMEDICINE(28,27,N)USEOFCARTILAGEPRODUCTS(1,23,E) YELLOWDOCK(14,15,SW) YOGA(2,5,E)
Compassion SitsBy Mary Lou Kennerly
and Robert Fisher
Arms
Hugging snug
Water mug
Chugging spring
Drip drop
Ring door bell
Well wishers
Healing touch
Feeling words
Birds passing
Verbal concern
One by one
Done
One day
Say a cure
For sure will be
Found sound mind
Find kind of
Relief have belief F