Embed Size (px)
Citation preview
Volume 10 Number 2, 2004
eurohealthThe media& health
The future direction of EU health policy
Promoting musculoskeletal health across Europe
Evaluating complex social interventions
Social and private health insurance: recent developments

Today’s news, tomorrow’s chip paper?
There is a saying in England that today’s news will be endup being used as a wrapping for fish and chips tomorrow,and that a story will burn brightly but then be long forgot-ten. This era itself is now fading away in an age of 24 mediacoverage, the incredible expansion of the internet and aninsatiable public appetite for stories. This should not be loston those working in the health field. We need to strive con-tinuously to get our message across, whether as policy mak-ers, researchers, healthcare professionals or consumergroups. Development and implementation of policies,uptake of new treatments and the promotion of healthylifestyles are heavily dependent on public engagement.Transparency and an opportunity to ask questions, providefeedback, and influence this process are critical.
The media has a powerful role to play in this process, andwe ignore it at our peril. Negative public perceptions areformed quickly and then may be reinforced by a constantstream of adverse headlines. Immunisation rates againstmeasles, mumps, and rubella in the UK have continued toremain below target, now many years after concerns werefirst raised in a single scientific journal paper that subsequently hit the headlines of the mainstream media.One of the lessons arising from this is that stakeholdersneed to pause for thought before releasing information andshould consider carefully how accessible this is, both tojournalists and the general public. In particular, the conceptof risk needs to be communicated more effectively to avoidunintended adverse consequences on the utilisation of services and perhaps ultimately on the direction of policy.
A welcome step to improve communication and provideopportunities for feedback has been the first EU OpenHealth Forum, and the ensuing opportunity for all to reflecton a new health strategy for the EU. Key themes on thefuture European health policy, observations on the healthforum process and responses to the reflection process allfeature in this issue of Eurohealth. The reflection process isdesigned to be inclusive, noting how “different actors mustwork together to foster good health across the EU”. Thereis still time to input into this process and it is to be hopedthat the responses are as diverse as hoped for by theCommission. However, all these positive developments atthe European level are unlikely to receive much attention inthe mainstream media. How much better it would be if suchpositive opportunities for engagement with European structures that often seem remote to the ordinary citizen,might be publicised in the mainstream media? Trying to getacross these positive challenges is very much an uphill challenge, as the news media have different priorities andneeds, but it is a challenge to which we must rise.
David McDaidEditor
MENT
LSE Health and Social Care, London School ofEconomics and Political Science, Houghton Street,London WC2A 2AE, United Kingdomtel: +44 (0)20 7955 6840fax: +44 (0)20 7955 6803email: [email protected]: www.lse.ac.uk/Depts/lsehsc
EDITORIAL
EDITOR: David McDaid: +44 (0)20 7955 6381email: [email protected]
SENIOR EDITORIAL ADVISER:Paul Belcher: +44 (0)7970 098 940email: [email protected]
DESIGN EDITOR: Sarah Moncrieff: +44 (0)20 7834 3444email: [email protected]
EDITORIAL TEAM:Julian Le Grand, Josep Figueras, Walter HollandMartin McKee, Elias Mossialos
SUBSCRIPTIONS
Champa Heidbrink: +44 (0)20 7955 6840email: [email protected]
Published by LSE Health and Social Care and theEuropean Observatory on Health Systems and Policies,with the financial support of Merck & Co and theEuropean Observatory on Health Systems and Policies.News section compiled by Eurohealth with some addi-tional input from EurohealthNet.
Eurohealth is a quarterly publication that provides aforum for policy-makers and experts to express theirviews on health policy issues and so contribute to a constructive debate on public health policy in Europe.
The views expressed in Eurohealth are those of theauthors alone and not necessarily those of LSE Healthand Social Care, EuroHealthNet or the EuropeanEuropean Observatory on Health Systems and Policies.
The European Observatory on Health Systems andPolicies is a partnership between the WHO RegionalOffice for Europe, the governments of Belgium, Finland,Greece, Norway, Spain and Sweden, the EuropeanInvestment Bank, the Open Society Institute, the WorldBank, the London School of Economics and PoliticalScience and the London School of Hygiene & TropicalMedicine.
Advisory Board
Dr Anders Anell; Professor David Banta; Mr Nick Boyd;Professor Reinhard Busse; Professor Johan Calltorp;Professor Correia de Campos; Mr Graham Chambers;Professor Marie Christine Closon; Professor MiaDefever; Dr Giovanni Fattore; Dr Livio Garattini; DrUnto Häkkinen; Professor Chris Ham; Dr MariaHöfmarcher; Professor David Hunter; Professor EgonJonsson; Dr Meri Koivusalo; Professor Felix Lobo;Professor Guillem Lopez-Casasnovas; Dr BernardMerkel; Dr Stipe Oreskovic; Dr Alexander Preker; Dr Tessa Richards; Ms Heather Richmond;ProfessorRichard Saltman; Mr Gisbert Selke; Professor IgorSheiman; Professor JJ Sixma; Professor Aris Sissouras; Dr Hans Stein; Dr Jeffrey L Sturchio; Dr Miriam Wiley
© LSE Health and Social Care 2004. No part of this publication may be copied, reproduced, stored in a retrievalsystem or transmitted in any form without prior permissionfrom LSE Health and Social Care.
Design and Production: Westminster European,email: [email protected]
Printing: Seven Corners Press Ltd
ISSN 1356-1030
eurohealthCOM
Contents Volume 10 Number 2
Health policy
4 The future direction of EU health policy?David Byrne and Pavel Telicka
6 Citizens and healthTamsin Rose
Reflection process
8 A health strategy for the EU: A response to Commissioner Byrne’s call for reflectionMartin McKee and Paul Belcher
Dutch presidency
12 The Dutch presidency: Some activities in the field of healthFrits Tjadens and Benno van Beek
Media and health
15 Headlines and deadlines: the media and health issuesDavid McDaid
18 The role of the press media in reporting on genetically modified food in UK and SpainMarta Vilella-Vila and Joan Costa-Font
Health care reform
21 Individual incentive schemes in social health insurance systemsRichard B Saltman and Hans FW Dubois
26 Private health insurance, commercialisation and EU legislationThe next stage in Dutch health care reformTom ED van der Grinten and Marina W de Lint
Musculoskeletal health
30 Musculoskeletal health: Preventing a dependent populationAnthony D Woolf, Kristina Åkesson, Juliet Compston, Karl-Göran Thorngren, Piet van Riel and Alex Watt
Older people
33 Advancing integrated care for older people through EU Policy: CARMEN thematic network expertise informs the European agendaNicoline Tamsma, Philip Berman and Henk Nies
Quality
37 Evaluating complex social interventionsJohn Øvretveit
Informed patient
41 E-Health and the informed patientAnders Olauson
Monitor43 Web Watch
44 Publications
46 European Union Newsby Eurohealth with input fromEuroHealthNet

eurohealth Vol 10 No 22
Contributors to this issue
Paul Belcher is European Union Adviser,Royal College of Physicians of Londonand Senior Editorial Adviser, Eurohealth.
Philip Berman is Director, EuropeanHealth Management Association, Dublin.
David Byrne is European Commissionerfor Health and Consumer Protection.
Juliet Compston is Professor of BoneMedicine, University of CambridgeSchool of Clinical Medicine, UK.
Joan Costa-Font is Research Fellow, LSEHealth and Social Care, London Schoolof Economics and Political Science.
Marina de Lint is a legal advisor at theDutch Council for Public Health andHealth Care.
Hans FW Dubois is Research Officer,European Observatory on Health Systemsand Policies, Ministerio de Sanidad yConsumo, Madrid.
David McDaid is Research Fellow, LSEHealth and Social Care and EuropeanObservatory on Health Systems andPolicies, at the London School ofEconomics and Political Science. He isalso editor of Eurohealth.
Martin McKee is Professor of EuropeanPublic Health, London School ofHygiene and Tropical Medicine andFellow of the Royal College ofPhysicians of London.
Henk Nies is Director, Division on Care,Netherlands Institute for Care andWelfare, Utrecht.
Kristina Åkesson is Associate Professor,Department of Orthopedics, MalmöUniversity Hospital, Sweden.
Anders Olauson is President and ChiefExecutive Officer of the AgrenskaFoundation, Hovås, Sweden.
eurohealth Vol 10 No 23
Richard B Saltman is Professor of HealthPolicy and Management, Rollins Schoolof Public Health, Emory University,Georgia, USA, and Research Director ofthe European Observatory on HealthSystems and Policies, Ministerio de Sanidad y Consumo, Madrid.
Nicoline Tamsma is Senior Adviser forInternational Health Policy, NetherlandsInstitute for Care and Welfare, Utrecht.
Frits Tjadens is Project Leader for theNetherlands for the EU Phare twinningproject with Poland on the mutual recog-nition of the qualifications of medicalprofessionals at the International Centreof the Netherlands Institute for Care andWelfare, Utrecht.
Pavel Telicka is a Member of theEuropean Commission.
Karl-Göran Thorngren is Professor,Department of Orthopedics, UniversityHospital, Lund, Sweden.
Benno van Beek is Secretary of theEuropean Society for Quality and Healthat the International Centre of theNetherlands Institute for Care andWelfare, Utrecht.
Tom Van der Grinten is Professor ofHealth Care Policy and Organisation,Department of Health Policy andManagement, Erasmus University,Rotterdam.
Piet van Riel is Head of Department andProgramme Director of ClinicalResearch, Rheumatology, University ofNijmegen, The Netherlands.
Marta Vilella-Vila is an analyst, FutureFoundation, London.
Alex Watt is Project Manager, Bone andJoint Health Strategies Office, RoyalCornwall Hospital, Truro, UK.
Anthony D Woolf is Professor ofRheumatology, Peninsula MedicalSchool, Truro, UK.
Tamsin Rose is General Secretary,European Public Health Alliance,Brussels.
John Øvretveit is Director of Research,The Karolinska Institute MedicalManagement Centre, Stockholm, andProfessor of Health Policy andManagement, The Nordic School ofPublic Health, Gothenburg, and BergenUniversity Faculty of Medicine, Norway.
Our work on health has shifted a great dealover the past years from reaction to action.In the first few years of the DirectorateGeneral for Health and ConsumerProtection (DG SANCO) its work wasmainly defensive, i.e. it sought essentiallyto protect the European public, forinstance, by overhauling the EU’s foodsafety laws; by addressing risks associatedwith blood and blood products; and by discouraging tobacco use.
However, as soon as this work was underway, attention was turned towards thedevelopment of a more proactive approachto public health. A strong emphasis wasput on the broad concept of ‘good health’which identifies health not only as a keyelement of individual welfare and happi-ness, but also as a key element in a broadersocietal context, that is, for social cohesion,productivity and economic sustainability.The protective and the proactive nature ofour work are essential and have become afundamental expectation of European citizens.
In order to achieve healthy public policy,health needs to be at the heart of the policyagenda. The challenge is therefore to ensurethat health interests are properly recog-nised and articulated, whether we are dis-cussing inner city development, regionaltransport infrastructure, social policy,atmospheric pollution or internationaltrade, to mention just a few examples.
So, what is the EU’s role in this? What canwe add at the European level? The EU canfunction as a catalyst for change and facili-tate progress. For example, the EU can
support the work of the Member States’health authorities with key policy chal-lenges such as how to ‘square the circle’ ofmeeting ever rising patient expectationswhile keeping control of healthcare spend-ing; how to identify which new treatmentsand technologies our healthcare systemsshould invest in; how to rise to the chal-lenge of the obesity epidemic in Europe;and how to make the healthy option theeasy option for our citizens, whether this issaying no to tobacco, taking more exerciseor making healthier food choices.
There have been some major health policyachievements at European level in recentyears. For example, there has been signifi-cant progress in the fight against tobaccouse, including high visibility health warn-ings on tobacco products and restrictionson tobacco promotion; the 2003-2008 pub-lic health programme is in place and pro-ducing results; we have created a frame-work to promote the safety of blood, tis-sues and cells; our planned EuropeanCentre on Disease Prevention and Controlis on course to open its doors in 2005; andthe Commission has just recently set up aHigh Level Group on Health Services andMedical Care.
However, there are still several healthissues which need to be addressed: the risein the incidence of chronic diseases; thethreat from newly emerging infectious dis-eases; the influence of new patterns ofbehaviour and consumer choices on health;the increasing longevity of the population;the rising expectations of citizens as regardshealth information and healthcare; and the
eurohealth Vol 10 No 24
HEALTH POLICY
The future direction of EU health policy
David Byrne andPavel Telicka
This article summarises the key points presented byCommissioners David Byrne and Pavel Telicka at thefirst EU Open Health Forum in Brussels on 17 May 2004.
“The challenge is to
ensure that health
interests are properly
recognised and
articulated”

health gap between the 10 new MemberStates and the rest of the Union.
More specifically, HIV/AIDS is an area forurgent action where priority setting andstrong leadership are of utmost importance,and crucial at all levels. In Western Europethe number of HIV infections is on the riseand in some Eastern European countriesthe epidemic is growing faster than any-where else in the world. A new HIV/AIDSagenda needs to be defined and to be suc-cessful this requires concerted actions.Society at large has to be mobilised andappropriate policy responses need to beidentified.
Yet another area of great importance con-cerns the environment and health. Thereare a number of environmental factors thatplay a strong role in causing or aggravatingdisease. For example, the link betweensmoking, respiratory diseases and cancer isobvious. On the other hand, there is a realneed to improve our understanding of thecausal links and to improve our efforts tomonitor emissions, exposures and healthoutcomes. We also need to ensure that pol-icy instruments, research programmes andactions are appropriately coordinated tomaximise benefits. The EU Action Plan onEnvironment and Health addresses severalof these issues and covers a whole range ofEU policies.
The main theme at the Open Health Forumwas Health and Enlargement. It hasbecome common to classify the EUMember States into the ‘old’ and the ‘new’Member States. A more realistic statementis that there are real differences between theMember States. We may all live in the samevillage, but some families are, in fact, betteroff than others. If we want to build aEurope of equal health, bridging the healthgap will be one of the biggest challenges weneed to address in the coming years.
Clearly, this cannot be achieved withoutsubstantial financial resources. Resourcesfor investing in health will have to comefrom national budgets as well as from theEU. Several Member States are alreadychannelling some of their EU StructuralFunds allocations towards health invest-ment. The Structural Funds provide a goodopportunity to finance health related pro-jects, particular for the new Member States.
However, the new Members States andCandidate countries also need know-howand support in developing their healthexpertise and in building the capacity oftheir health sectors to compete for the lim-ited funds available.
In more general terms, there are four dis-tinct areas where the EU can make a tangi-ble contribution to improving the health ofEurope’s citizens:
1. Focusing on citizens and patients: tomake reliable information on healthavailable to European citizens, and topromote their active participation in thehealth decision-making process;
2. Promoting health as a driver of econom-ic growth, sustainable development andquality of life;
3. The High Level Reflection Process onpatient mobility and healthcare develop-ments has led to the identification ofactions that will help the health sector.We need to find ways of improving co-operation to ensure resources are usedwell, information is improved, and theexchange of best practice promoted; and
4. The EU needs to develop its role ininternational forums in response toglobalisation.
The Commission’s EU Health Strategyfrom May 2000, identified integratinghealth into all EU policies as one of its keyobjectives. This means ensuring that publichealth experts and health policy stakehold-ers have a strong input in EU decisionmaking.
The Health Policy Forum, launched by theCommission in 2001 and bringing togethersome 60 representatives of European levelhealth networks and stakeholders, was animportant step towards this objective.However, the Open Health Forum, bring-ing together as it does some of the leadinghealth experts and opinion-formers fromall across Europe, provides a platform foreven wider participation of stakeholders.The Open Health Forum has the potentialto be a powerful voice in Brussels whichwill be heard not just in the Commission,but also in the European Parliament, theCouncil, the media and, beyond Brussels,the general public.
eurohealth Vol 10 No 2 5
HEALTH POLICY
The first Open Forum took place on 17 May in Brussels with the overall theme ‘Health in the Enlarged Europe’ and attractedaround 300 participants from a wide range of organisations. You can find speeches, presentations and photos of the event athttp://europa.eu.int/comm/health/ph_overview/health_forum/open_forum_04/contributions_en.htm. Participants’ feedbackand evaluation of the conference will also be posted on the site.
“HIV/AIDS is an area
for urgent action”

The Workshop on Citizens and Health atthe EU Open Forum on 17 May 2004 wasdesigned to open a debate on some keyquestions:
– What are citizen and patient rights andhow do they alter the roles and respon-sibilities for health?
– How do socioeconomic factors impacton health and therefore to what extentcan individuals be made responsible fortheir own health?
– In terms of equity in treatment choiceand availability how is complementaryand alternative medicine (CAM)addressed in Europe?
– What are the barriers to greater patientparticipation in decision-making inhealth and how can they be addressed?
These are complex and important questionswhich however need more considerationthan that possible in a short workshop. Thediscussions at the Forum (See Box) raisesome issues for further exploration.
RightsThe patients’ rights agenda has emergedfrom patient advocacy and a growing frus-tration with poor medical responsiveness toindividual needs, concerns and situations.In addition a series of studies looking atcivil servants in England (the Whitehallstudies) have demonstrated that the morechoices and power an individual has, thenthe better their health status. The WorldHealth Organization has developed exten-sive material on health rights as part of thefundamental human rights process as wellas specific rights for patients when enteringthe healthcare system. At the Europeanlevel there is no standardised approach tohealth rights other than Article 35 of theCharter of European Fundamental Rights,now included in Part II of the new EUConstitutional Treaty. This states thateverybody has the right to treatment andpreventative health care. Each MemberState has pursued a different path onpatient rights, some through legislation andothers through guidelines, codes or othernon-binding mechanisms.
A rights based approach to health providesa road map for empowerment, ensuringthat when individuals become ill and enterthe healthcare system that they are stilltreated with respect and dignity. It is achallenge for health professionals and forhealth service planners to respond ade-quately to citizen and patient rights. Thisrequires a re-balancing of the power rela-tionship and recognition that improvinghealth is a shared process with both profes-sional and patient playing a part in takingdecisions. But do all individuals want to beactively involved in making decisions?Anecdotal evidence shows that there areoften wide divergences between those whowant to be part of developing a treatmentplan and individuals who want the health-care system to deliver a solution withouthaving to understand and debate the issueswith a health professional. This raises thequestion about who is responsible for thesubsequent health outcome? For example,if an individual exercises their right not toreveal information about previous condi-tions or symptoms or other medicationthat they take and there is a negative side-effect from treatment, where does responsi-bility lie? If a patient does not complete amedication regime or ignores professionaladvice, where does the fault lie? Surveysshow that only about 50% of those withchronic conditions follow their treatmentregimes. Furthermore 10% have to receivemedical treatment because of harm causedby earlier medical care. Perhaps the root ofthe problem is a search for blame when anegative health outcome occurs. If inputinto health is a shared responsibility thenwho is accountable for poor results? It isimportant to understand the responsibilityissues because litigation for health prob-lems is increasingly common.
Information and choiceThere is a continuing information need forindividuals and family members.Information about diagnosis, prognosis,treatment options but also more informalsharing of experience about how illnessesand conditions affect everyday life, work,relationships etc. Concerns were also raisedthat there is an information overload whichrequires time, persistence and luck to navi-gate successfully to find information that isrelevant, useful and appropriate.Information alone is not enough, neither is
eurohealth Vol 10 No 26
HEALTH POLICY
Citizens and health
Tamsin Rose is General Secretary, European Public Health Alliance, Brussels.E-mail: [email protected]
Tamsin Rose
“Empowerment and
responsibility must not
become a mechanism
to penalise individuals
for ‘wrong’ choices”

blind provision of more information.Patient organisations, advocacy groups andsupport networks can help by acting as afilter, collating information and helping tointerpret and use this material. This placesgreat responsibility on these structuresmany of whom have strong personalinvolvement but are very under-resourced.
As the political emphasis on providingchoice in health is expanded, attentionneeds to be paid to the CAM community,facing similar issues to those currentlybeing addressed by the medical communitysuch as training and qualifications, qualityand safety, access and affordability. Insome countries, European governmentshave tended towards prohibitive regulationwhile others have opted for a more struc-tured approach to address training stan-dards, quality and safety. For recognisedCAM disciplines several health insurerswill reimburse costs. This situation ofpatchy regulation and unequal access mustbe addressed to enable all citizens to havereal choice in health treatment and encour-age them to be more pro-active on theirown health. Political will can ensure thesignificant economic and institutionalresources that are needed to enable patientand public involvement in health services.This pressure can also overcome inertia ortradition in the education of healthcareprofessionals to incorporate the principlesof partnership with patients, the need forclear communication and the provision oftimely information.
The limitations of the goal of making indi-viduals responsible for their health becomeclear when the impact of socioeconomicstatus is examined. The key determinant inpoor health status is poverty which com-pounds the negative effects of inadequatehousing, degraded environment, limitededucation, a lack of employment opportu-nities, high-risk behaviours and unhealthylifestyles. It seems that money can buygood health. The most critical ‘choice’ inlife is in having parents from a privilegedbackground with all the social and eco-nomic advantage that this can provide.
Linking citizens with their health statusmeans recognising that there must beopportunities for decisions, input andchoice throughout the healthcare system. Italso means recognising that individuals arevery different and some may want exten-sive information, to exercise real choice andgain knowledge and skills on their own ill-ness or conditions. Others may expect theirhealthcare systems to take care of theirhealth problems and not have to engage in
choices. The greatest challenge will bemeeting the needs of individuals through-out this spectrum particularly as sometimesone person may be passive for some healthelements and extremely active on anotherhealth question. Acknowledgement of theimportance of socioeconomic status onopportunities in life means that empower-ment and responsibility must not become amechanism to penalise individuals for‘wrong’ choices.
eurohealth Vol 10 No 2 7
HEALTH POLICY
EU OPEN HEALTH FORUM, PARALLEL SESSION III, CITIZENS AND HEALTH
Rapporteur: Deirdre O’Connell, European Patients Forum.
The four contributors to the session covered various aspects of the topic, Citizensand Health.
Stella Kyriakides, EUROPA DONNA – The European Breast Cancer Coalition,(Patient and citizen rights: a statement of values) discussed values of patientrights from an advocacy perspective, using Europa Donna as an example of howpatient rights can be ensured by patient advocates, trained in advocacy methodsand aware of their rights.
Darja Havelkova, Czech Shiatsu Federation, (Exercising choice in health treat-ment) spoke about the extensive use of complementary and alternative medicinein Europe today, the differing national regulations, and current trends in regulationin relation to the active involvement of citizens in their own health care.
Tamsin Rose, General Secretary, of the European Public Health Alliance, (Accessto health for all citizens) reviewed determinants of health, including health ser-vices, barriers to access and empowerment, concluding that lifting people out ofpoverty would do most to improve health.
Barrie Taylor, from the Commission for Public and Patient Involvement in Health(Citizens and health: the road to empowerment), described how the Commission isoffering opportunities for citizens to have an input into health planning and policyissues, bringing together lay and professional strands to work together. The keythemes covered in the discussion were information, access, responsibility, partner-ship/integration, and training/empowerment.
Information: There can be too much or too little information, or not the right kind.What is needed is accurate and performance tested information, with awarenessthat people have varying capabilities. Do carers or families have enough goodinformation? How to access information should be part of citizenship programmesand we must have ways of assessing information. The use of the internet shouldhave been covered in the agenda; it has been very valuable to people with raredisorders, while it can also be abused
Access: There are various barriers to access, many socioeconomic. Eveninformed patients cannot always get access, if, for example, they do not live in aplace with good services. As regards access to CAM, the EU should put moreresources into studying this area; at present there could be said to be discrimina-tion against CAM and its users.
Responsibility: Who is responsible for the health of citizens? The government hasa responsibility to enable individuals to take more responsibility. Some groups, forinstance the homeless face huge barriers. There are moral assumptions underly-ing the lifestyle approach to health and health prevention.
Partnership/Integration: This is required between scientists, doctors, patients, andindustry and also between decision makers and the public. There is a need forequal respect and for forming alliances.
Empowerment/Training: Governments and the EU should fund training pro-grammes via patient advocacy groups.
A questionnaire was handed out at the session looked at responsibility for healthand key actions for government. When asked, “Who should have the main respon-sibility for our health?” responses were: individuals, national governments, health-care professionals, parents/family and local/regional authorities. Key areas identi-fied for government action were: education in schools, banning smoking in publicplaces, use of financial incentives, increased availability of health promotion, morespace for exercise, regulation of access to products that may be harmful with pro-vision of health warnings and prioritisation of access to health care services.

IntroductionOn the 15th July 2004 David Byrne, theEuropean Commissioner for Health andConsumer Protection, launched a processof reflection that will shape a new healthstrategy for the EU.1 He emphasised howimportant it is that the people of Europecan live longer, healthier lives, and notedthe progress that has been made, asEurope’s citizens are now living in betterhealth than ever before. Yet he also sound-ed a note of caution, highlighting the largedifferences in health that have persisted,with the poor, the socially excluded, andminorities particularly affected by illhealth.
The consultation document sets out wherewe are now and identifies much that needsto be done. However a health strategyinvolves choices, about priorities, policies,and means. The reflection process isdesigned to be inclusive, noting how “different actors must work together tofoster good health across the EU”. Tomake this a reality, Byrne asks a series ofquestions about how to proceed. In thispaper we have tried to answer some ofthese questions.
The role of the individualMany factors contribute to the unequalburden of disease and premature death inEurope but four, smoking, poor diet, lackof physical activity, and hazardous drink-ing are especially important. The documentmakes much of the importance of individ-ual choice: “health is, to a great extent,determined by individual choices” and“Many of the choices for achieving goodhealth lie in the hands of the citizens them-selves”. Of course, ultimately, people do
make choices about how they lead theirlives, yet it is also important to understandhow those choices are frequently con-strained.
This is most obvious in the case of smok-ing; exposure to the harmful effects oftobacco is not a matter of free choice formost people. First, surveys consistentlyshow that most smokers want to quit.2
Many fail to because of the highly addictiveproperties of nicotine, with modern ciga-rettes containing additives such as ammoniadesigned to boost the nicotine kick thatkeeps people addicted.3 Second, thoseworking in places where they are exposedto other people’s smoke have no choice.
However there are many other constraintson an individual’s ability to make healthychoices. Many people are unable to gainaccess to affordable nutritious food, as theretail food industry concentrates itsresources on those with the greatest pur-chasing power and public transport is with-drawn from unprofitable routes.4 Physicalactivity becomes a difficult choice for thoseworking long hours, perhaps with multiplejobs and inadequate childcare provision,with no nearby leisure facilities.
So for many of Europe’s citizens, and espe-cially the most vulnerable to poor health,choice is often an illusion. The resourcesrequired to promote health are especiallysusceptible to market failure. Many are‘public goods’, which are under-producedif left to the market. Individual choice isimportant but it can only be effective ifgovernments step in to make it a reality.
Putting health at the centre of EU policy makingThe document emphasises the role ofhealth as a driver of economic develop-ment, an issue that is now on the globalagenda as a result of the pioneering work ofthe Commission on Macro-Economics andHealth.
The contributions of health to wealth areseveral. Most obviously, a healthy work-force is more productive and a healthier
eurohealth Vol 10 No 28
REFLECTION PROCESS
A health strategy for the EU:
A response to Commissioner Byrne’s call for reflection
Martin McKee is Professor of European Public Health, London School ofHygiene and Tropical Medicine and Fellow of the Royal College ofPhysicians of London. E-mail: [email protected]
Paul Belcher is European Union Adviser, Royal College of Physicians ofLondon and Senior Editorial Adviser, Eurohealth. E-mail: [email protected]
Martin McKee and Paul Belcher
“Individual choice is
important but it can
only be effective if
governments step in to
make it a reality.”

population places fewer demands on themoney required for health care. Howeverwealth also contributes to health, andhealth is, in itself, a perfectly good indica-tor of the progress of nations and even, ashas been suggested by Amartya Sen,5 mayeven be better than conventional measuressuch as Gross National Product, which area far from perfect measure of human happi-ness. If this mutually reinforcing relation-ship is to be sustained, there is a need forcontinuing investment in both the preven-tion of disease and the means of treating itwhen it occurs.
The document asks whether the EU can domore to disseminate evidence on the rela-tionship between health and wealth and onthe efficiency of health systems but alsoasks whether it should do more. It is onlybeginning to take on these roles so thisquestion may be premature. However whatis clear is that there is a considerabledemand for such exchange of informationand, if adequately resourced, the EU couldmake an important contribution to thisprocess, building on the many existing ini-tiatives. Perhaps more importantly, thedevelopment of a new strategy offers theopportunity to make a reality of the Treatyrequirement that a high level of health pro-tection should be part of all EU policies.Health can also be a casualty of economicgrowth, especially where that growth isunevenly distributed or is achieved at thecost of environmental degradation. Thismust not happen.
Specific issuesThe document asks what should be doneon certain specific issues. One is how theEU’s role in communicable diseases shoulddevelop. The new European Centre forDisease Prevention and Control will beginwork in May 2005. This is a long overduedevelopment. However, compared with theAmerican Centres for Disease Control, itwill operate on a very limited scale. Ofcourse the analogy is not perfect; the newEuropean centre will be grafted on to exist-ing national infrastructure. Yet it will beimportant to monitor the demands placedon the new centre, ensuring that it has theresources to do its job.
A European centre is critically dependenton the information fed to it by nationalsurveillance systems. Yet in many parts ofEurope these systems are far from perfect.The centre will build on a series of existingnetworks, frequently built up in the face ofconsiderable difficulty, by a few dedicatedenthusiasts who had the vision to see that a
coordinated European response to commu-nicable disease was needed.6 Yet in manycases the coverage of these networks ispatchy. There are large parts of Europe inwhich reporting and investigation of out-breaks is far from adequate. Putting thisright, with sustained investment in labora-tories and public health systems, is primari-ly a responsibility for Member States butthe EU can also play a role in developingstandards and exchanging information ongood practice.
It will be essential that the work of the newcentre is not confined to the territory of theMember States. As was all too apparent inthe SARS outbreak, communicable diseasesdo not respect national frontiers. It will beimportant that the EU’s often labyrinthinerules facilitate rather than obstruct theCentre’s ability to work in other parts ofthe world, and in particular in the EU’snew neighbours in eastern Europe andNorth Africa.7
The document also identifies tobacco as anissue requiring action by the EU. It asks,should all governments follow the Irishexample and ban smoking in public places.The answer must be an emphatic yes. First,improved research methods, with moreprecise measures of exposure, have revealedthat exposure to second hand smoke is con-siderably more dangerous than was previ-ously believed,8 a finding consistent withrecently discovered tobacco industryresearch on animal testing. Second, surveysin many European countries are showingmajority support for smoking bans; inmany cases most smokers are also in favourof action. Third, as the Irish experienceshows, as long as there is some attempt atenforcement, that bans work and are wide-ly accepted.
But what can the EU do to facilitate thisprocess? First, it should support work thatexposes the depressing number of ‘inde-pendent’ experts who have succumbed tothe temptation to take money from thetobacco industry,9 including several whohave influential links with governments insome Member States. Ironically, this yearone highly paid tobacco industry consul-tant was appointed to a EU health commit-tee, although his extensive links were notknown to the Commission when theappointment was made. The availability ofmillions of pages of industry documents onthe internet as a result of American courtsettlements means that these people can nolonger hide. The apparent ease with whichindividuals can enter such committees isextraordinary. Greater scrutiny, by experts
eurohealth Vol 10 No 2 9
REFLECTION PROCESS
“Should all
governments follow the
Irish and ban smoking
in public places? The
answer must be an
emphatic yes.”

from the health sector, is required of indi-viduals who put themselves forward forEU health related committees. In addition,the European Commission must publish adeclaration of interest for each applicant.
Second, it can disseminate evidence thatdispels the many myths pedalled by theindustry. This includes exposing theresearch commissioned by the industry,some of which was fraudulent and somesimply designed to mislead, that sought toundermine the evidence that second-handsmoke is harmful.10 It also involves expos-ing the fallacy that the problem can be dealtwith by improved ventilation. It must berecalled that many of the harmful con-stituents of second-hand smoke are odour-less; to reduce them to safe levels wouldrequire a system that could create a rate ofairflow similar to sitting outside during agale.11
Finally, it must expose the myths about theeconomic impact of smoking bans. In NewYork sales tax receipts on food and drinkincreased by 12% and employment in thehospitality industry increased in the ninemonths after the smoking ban was intro-duced.12 However, the most important evi-dence is from a systematic review ofresearch on the impact of bans on bar andrestaurant revenue.13 All of the 37 studiesthat found an adverse economic impact hadbeen funded by the tobacco industry orwere written by consultants known to haveindustry links. In contrast, all of the 60independent studies found either no impactor an increase in sales or employment.
However, the EU can also do much to helpthose who are smokers. For example:
– It can do more to clamp down on smug-gling, recognising the key role played bysome tobacco companies in facilitatinglarge scale smuggling activity. 14
– It can step back and ask what cigarettesare actually for? The answer should beclear; they are methods for deliveringnicotine, an addictive drug with impor-tant effects on the cardiovascular andnervous system. This then raises thequestion of why this drug remainsunregulated. There is a strong case forestablishing a nicotine regulatoryauthority that can consider the variousroles of the increasing sources of nico-tine (chewing gum, patches) many ofwhich have fewer harmful effects thancigarettes.
– Finally, given the scale of health damagefrom tobacco in Europe, the EU can
shape the policy dialogue by committingto a long term goal of a smoke-freeEurope and a medium term goal ofreaching levels already achieved in someparts of the world, such as the 11% inCalifornia.
A third set of questions ask about the EU’sroles on nutrition and obesity. The EU isespecially well-placed to do something byvirtue of the many areas where it hasresponsibility that have an impact on theseissues. These include transport, agricultureand fisheries, trade, and the internal mar-ket. Its scope for action extends fromexchanging evidence of best practice topassing legislation. A major challenge, butone that, experience suggests, may besomewhat problematic, involved reform ofthe Common Agricultural Policy.15 At lasttobacco subsidies are on the way out, butEurope’s agricultural policy continues tofavour production of fats over fruit andvegetables. The EU destroys 1 million tonsof fruit and vegetables each year whileover-producing 6 million tons of sugarannually, not to mention subsidising theprovision of high fat milk in schools.
The document contains a welcome recogni-tion of the role of health impact assess-ment, asking how it might operate in prac-tice. The challenge for the Commission ishow to learn from the growing body ofexperience in both health and environmen-tal impact assessment. These experiencesare showing that impact assessment canprovide the information that is needed toshape policy but is also highlighting theneed to build sufficient capacity to under-take such assessments.
ResearchThe document’s recognition of the impor-tance of health research is also welcome,asking whether new infrastructures such asthe US National Institutes of Health(NIH) would bring benefits. This is a ques-tion that merits further consideration. Itseems unlikely that a EU institution wouldever have the resources available to theNIH and there is also the risk that thevagaries of EU legislation and budget set-ting would compromise the continuity thatsuch a major initiative would require.Furthermore, while much has been done toreduce the administrative burden involvedin the 6th Framework Programme, there isstill much that needs to be done. As anintermediate step, there may be more bene-fit to be achieved by facilitating closercooperation between national and non-governmental funding bodies.
eurohealth Vol 10 No 210
REFLECTION PROCESS
“Greater scrutiny is
required of individuals
who put themselves
forward for EU health
related committees”

Mobilising different actors: partnerships for healthThe document notes the importance ofopenness and civil society participation inthe development of health policy. Theexisting mechanisms, such as the OpenForum and the Health Policy Forum, havenot been especially successful and somequestion whether these and other process-es, such as G10 (pharmaceuticals) and theHigh Level Reflection Process on PatientMobility and Healthcare, actually fulfil theCommission’s own criteria for consulta-tions as set out in the White Paper onGovernance. The breadth and diversity ofthe public health and healthcare communi-ty must also be recognised and included inthese processes and not left to single sec-tors, such as patient or healthcare groups.There is a need to rethink these models,developing a shared understanding amongthose involved about what the realisticexpectations should be for these bodies.There is also a need to extend participationto organisations with something to say butwhich might not be organised at aEuropean level. For example, many nation-al organisations have much to contribute tothe development of policies on particularissues.
It also asks about how to foster partner-ships. DG Sanco works with very limitedresources. It has few, often overstretched,staff and little easy access to technicalexpertise. One possible solution might bemodelled on the WHO system ofCollaborating Centres, in which certainacademic and technical centres would bedesignated as providing expertise in specificareas. In most cases, this would onlyinvolve some minor adjustment of theirexisting work to ensure that it met the par-ticular needs of the Commission. However,it would also provide a rich source ofadvice that could be tapped when rapidanswers are needed.
Health on the international agendaA final set of questions relate to health onthe international agenda, in particular inrelation to policies such as trade and inter-national development. With an economythat is now larger than that of the UnitedStates, the EU has the potential to be aneven greater force for good in the world,offering an alternative vision to what hasbecome the dominant neo-liberal economicparadigm. This has become increasinglyimportant as the USA has, in areas rangingfrom landmines to climate change, retreat-ed from multi-lateral solutions to the
world’s shared problems. The challenge,once again, is ensuring that health really isan integral element of all the EU’s policies.
Moving forwardCommissioner Byrne has embarked on anambitious programme that, if successful,really will put health at the centre of theEU’s activities. Unfortunately despite theTreaty obligations and the strenuousefforts of many people, health can toooften seem a peripheral issue at a Europeanlevel, taking second place to the promotionof the internal market. We are now pre-sented with an opportunity to make a dif-ference. In this article we have set out someresponses to this consultation. It is impor-tant that others do so too.
eurohealth Vol 10 No 2 11
REFLECTION PROCESS
REFERENCES
1. Byrne D. Enabling Good Health for All. A Reflection Process for a NewEU Health Strategy. Brussels: European Commission, 15 July 2004.
2. National Statistics. Omnibus survey for ASH (M298) smoking: weight AOctober and November 2001. London: National Statistics, 2002.
3. Wayne GF, Connolly GN. How cigarette design can affect youth initiationinto smoking: Camel cigarettes 1983-93. Tob Control 2002;11 Suppl 1:I32–9.
4. Dowler E. Inequalities in diet and physical activity in Europe. PublicHealth Nutr 2001;4(2B):701–9.
5. Sen A. Mortality as an indicator of economic success and failure. Econ J1998;108:1–25.
6. MacLehose L, McKee M, Weinberg J. Responding to the challenge of com-municable disease in Europe. Science 2002:295:2047–50.
7. Coker RJ, Atun RA, McKee M. Health care system frailties and publichealth control of communicable disease on the European Union’s new easternborder. Lancet 2004;363:1389–92.
8. Whincup PH, Gilg JA, Emberson JR, Jarvis MJ, Feyerabend C, Bryant A,Walker M, Cook DG. Passive smoking and risk of coronary heart disease andstroke: prospective study with cotinine measurement. BMJ 2004;329:200–5.
9. McKee M. Competing interests: the importance of transparency. Eur JPubl Health 2003;13:193–94.
10. Ong EK, Glantz SA. Tobacco industry efforts subverting InternationalAgency for Research on Cancer’s second-hand smoke study. Lancet 2000;355:1253–9.
11. Drope J, Bialous SA, Glantz SA. Tobacco industry efforts to present ven-tilation as an alternative to smoke-free environments in North America. TobControl 2004;13 Suppl 1:i41–7.
12. Stark M. Commissioner to the New York City Department of Finance.Letter to the Editor. New York Times 4 Jan 2004.
13. Scollo M, Lal A, Hyland A, Glantz S. Review of the quality of studies onthe economic effects of smoke-free policies on the hospitality industry. TobControl 2003;12:13–20.
14. Joossens L, Raw M. Turning off the tap: the real solution to cigarettesmuggling. Int J Tuberc Lung Dis 2003;7:214–22.
15. Lock K, Gabrijelcic-Blenkus M, Martuzzi M, Otorepec P, Wallace P,Dora C, Robertson A, Zakotnic JM. Health impact assessment of agricultureand food policies: lessons learnt from the Republic of Slovenia. Bull WorldHealth Organ 2003;81:391–8.

The Dutch presidency of the EU is the firstof the EU25. This will clearly shape thispresidency, as well as possibly the after-math of the Convention. The enlargementis an unprecedented activity that posesenormous challenges. Furthermore, theDutch Presidency will be faced with arenewed European Parliament and with anew Commission. Thus, the DutchPresidency is an unprecedented one, facingchallenges never seen before. The samegoes for the challenges that the Dutch pres-idency meets in the field of health. In thisarticle we identify some of the relevantissues. Also we discuss some of the activi-ties that the Dutch Presidency is undertak-ing to address these issues, such as an infor-mal Health Council, preceded by an EU-wide NGO-conference on Health and theMarket and a side event linked to mutualcooperation European Economic Areawide between health care registers andsupervisory bodies.
Enlargement in a renewed contextThe accession is a fact, and 29 countries arenow within the European Economic Area.The new member states have gone througha transition that will hardly have finishedand that will require a lot of after-care.Most have experienced much turmoil,hopes and despair in the aftermath of thedecline of the Soviet empire and have hadto reinvent themselves. This they have doneover the last 15 years, sometimes stumblingalong the way, and now communism issomething that the older generation speaksof, but that the younger generation, full ofaspirations and dreams, while sometimesdisappointed by the treatment given by theEU15, (as new Polish Commissioner,Danuta Hubner, intimated in a March 2004interview to Euroactiv), neverthelessregards as ancient history.
Because of the enormous differencesbetween these countries and the previous
EU15,1 programmes were developed toassist the Accession States to deal with thestructures and Acquis to be implementedall over the enlarged EU according to theCopenhagen criteria. Thus the newMember States have received an enormousamount of assistance in the implementationof the Acquis Communautaire.
Health issues in the enlarged EUThe Convention was disappointing in thenaming of health(care) in the draftConstitution but the recent IrishPresidency took up the issue to strengthenthe health component. Even though therestill is uncertainty about the realisation of areal European Constitution (because now itis up to citizens of the EU member states tovote for it), it is fairly safe to state that theissue of health and the internal market is
eurohealth Vol 10 No 212
DUTCH PRESIDENCY
The Dutch presidency: Some activities in the field of health
Frits Tjadens is Project Leader for the Netherlands for the EU Phare twinningproject with Poland on the mutual recognition of the qualifications of medicalprofessionals. E-mail: [email protected]. Benno van Beek is Secretary of theEuropean Society for Quality and Health. E-mail: [email protected]. Both authors work at the International Centre of the Netherlands Institutefor Care and Welfare, Utrecht.
Frits Tjadens andBenno van Beek
Assistance for new Member States: EU PHARE TWINNING AND HEALTH PROFESSIONALS
With the means of the EU PHARE Twinningfunding, the Ministry of Health of theNetherlands is assisting the Ministry ofHealth of the republic of Poland to fullyimplement the current acquis concerningthe mutual recognition of qualifications ofmedical professions. This, as may beknown, concerns both the so-calledGeneral System professions as well as theprofessions, regulated in the currentSectoral Directives (doctors, dentists,pharmacists, general care nurses and mid-wives).
On the Polish side it requires the imple-mentation of the Directives in relevantPolish legislation and the build-up of rele-vant infrastructure. The Dutch have assist-ed by having a so-called Pre-AccessionAdvisor (now after May 1 a ResidentTechnical Advisor) in Poland for the dura-tion of the project and by bringing inexperts from the Netherlands, UK ,Germany, Belgium and Sweden dependingon the Polish request for assistance.
Similar assistance programmes have beenor are being implemented in other newMember and Candidate States: the Frenchare assisting the Romanians and theGermans, together with the English, assistthe Czech Republic. The Netherlands isalso helping Lithuania with this task. ThePHARE program runs across all EU-AcquisChapters.
“Enlargement is an
unprecedented activity
that poses enormous
challenges”

growing in importance rather quickly.Several developments in the near futurewill need to be dealt with on a Europeanlevel:
The accession of new Member States leadsto worries about:
Communicable and/or infectious diseasesthat may be on the rise in new MemberStates.
Food safety.
Health care labour markets: even thoughthere are serious discussions going onabout quantity (and fears of floodinglabour markets led to restrictions on accessto many western labour markets), it can beexpected that the mobility of health profes-sionals will grow. This will lead to issues ofpatient safety and thus of a need for furtherdevelopment of the quality control ofhealth care systems and health profession-als.
Life style related illnesses
On the other hand the EuropeanCommission has recently set out its overallhealth strategy for the coming years:*
Patient mobility.
Ageing and the sustainability of healthcaresystems, especially with regards to the careof the elderly; tackled using the OpenMethod of Coordination.
The issue of E-health, which is growing inimportance from the introduction of aEuropean health insurance card to telemed-icine.
Furthermore, the following issues couldalso be mentioned:
Mobile delivery of health services mightdevelop if health organisations in the EU15use the lower cost of labour in the newMember States and arrange ‘medicaltourism’ to these states backed by ECJ rul-ings.
In an enlarged EU diseases that had beenrare may seem less so, thus the issue oforphan drugs will play an even bigger rolethan before, even though access to medica-tions in many of the new Member States isstill lagging behind that found elsewhere inthe EU.
The interrelationship between employmentand family caring responsibilities in ageingsocieties will gain importance. Even thoughthe need to work longer, both in terms ofhours per week and also in total years maybe an economic necessity, it adds to theburden of an ageing society that needs to
take care of chronically or terminally ill rel-atives. Furthermore, it is not only thehealth workforce that faces increasingshortages; family networks are alsodecreasing in size rapidly. This could leadto ever growing burdens for informal car-ers and to an increasing risk of thembecoming patients as well. This leads to theconclusion that European health policy aswell as economic and social policy shouldact on the health of, and support for, familycarers as part of the complete health work-force by taking steps to prevent their healthdeteriorating as a result of caregiving.
Health and the CommunityThe Dutch presidency in the autumn of2004 will be the first to deal with thisexpanded European Union, with all theseissues on the health front in full glare of thecommunity. This perhaps is one of the rea-sons why several initiatives are taken,another being the increasing ‘interference’by the ECJ (and thus: of the InternalMarket) on, according to the subsidiarityprinciple, national health issues.
So, just before the informal Council ofHealth Ministers (9 September 2004),NGOs from all over Europe will gather todiscuss all topics in relation to the fourfreedoms and health during a two day-con-ference in the Hague under the title‘Shaping the EU Health Community,Balancing Health, Social Developments andInternal Market’. European NGOs andtheir Dutch counterparts are workingclosely together to develop a programmethat tackles the crux of current Europeandiscussions.
In the background several Commissionpapers may play a crucial role. Not only isit about the three ‘health-communications’mentioned previously, but also about otherCommunications such as the Green Paperon Services of General Interest, and theProposal for a Directive on Services in theInternal Market (COM(2004)2; 2004/0001(COD). Both papers serve as foundationstones for a Europe-wide discussion thatmay have a severe impact on healthcare.Thus, the conference basically deals withthe essential dualism existing in theEuropean Community on issues such ashealth, health care delivery and equity ofaccess. At all stages one can see the funda-mental dilemma creeping up between thegrowing influence of the Internal Marketover issues that are part of the competenceof national governments. It is thought thatnot only might the outcomes prove pro-ductive for the Informal Council of Health
eurohealth Vol 10 No 2 13
DUTCH PRESIDENCY
* See COM(2004)301final:Follow-up on the High Levelreflection process on patientmobility and health care devel-opments in the EuropeanUnion of 20 April, to whichCommissioner Byrne addedhis Health Strategy on 15 July.
“it is not only the
health workforce that
faces increasing
shortages; family
networks are also
decreasing in size
rapidly”

Ministers, but that they might also providerelevant input to the newly developed HighLevel Group on Health Services andMedical Care.
Mutual recognition EEA-wideAnother issue gaining importance is themutual recognition of qualifications ofmedical professions. The shortages in somelabour markets in Western-Europe and theabundance (at least, for the near future) inthe new Member States, leads to the expec-tation that mobility will be on the increase.For instance, even though the Netherlandsis not opening up its labour market to mostof the new Member States during the tran-sitional period, for certain health profes-sions the restrictions are lifted, due toshortages that impair the quality of healthcare.2
As such, migration of health care profes-sionals is and will remain an issue on theEU-agenda, both as issue of immigrationand as issue of (temporary) emigration.And, yes, the combination also may occur.This issue is linked to several other health-topics:
– Regulating migration in relation to healthcare workforce surpluses and shortages. ACouncil of Europe working group at thismoment is working on this. At EU-level,discussions are also linked to the issue ofmonitoring both labour-supply in healthcare systems and migration flows.
– A possible further harmonisation of qual-ifications without new directives (forinstance as triggered by European Centresof Excellence).
– Professional misconduct crossing nation-al borders. Recently the Commission intro-duced a revised proposal COM(2004)314,which (partly) accepts 55 of 125 amend-ments made by the European Parliament tothe original proposal. It has now beenaccepted by the Council.
For this purpose it is interesting to notethat the Dutch Presidency will also becharacterised by a EEA-wide conferencefor (sectoral) health care registration andclinical governance bodies in Amsterdamon 9–10 December 2004. It will be a fol-low-up to the last Dutch Presidency in1997. The current objective is to discuss theoptions for registration bodies to workmore closely together on the issue of crossborder movement of health care profes-sionals, especially on the issue of profes-sional misconduct, while at the same timetaking into account issues of privacy andthe potential for blacklisting. While the
basic foundations are already in place in thecurrent Sectoral Directives, there is never-theless much that still can be gained,through better knowledge of the registra-tion process and it’s workings in countries.
On the other side there are the clinical gov-ernance bodies, linked to the quality ofhealth care. Increasingly they are facedwith cross border care scenarios, eitherthrough the mobility of health care work-ers or through the mobility of patients.Thus, there is an increasing awareness thatcross-national cooperation between bodiesresponsible for quality control acrossEurope could prove useful, but it stillsomewhat unclear as to how this coopera-tion could be achieved and under whatconditions.
In order to provide relevant input for theconference, an EEA-wide analysis to tacklethese questions will be conducted. Theresults will not only be made public duringthe Amsterdam-conference, but will also becompiled for a public website,www.nizw.nl/eeahealthpros. Thus infor-mation on all aspects of the registration ofhealth care professionals will be madeavailable. Furthermore, the conference willdeal with questions such as how coopera-tion between registration bodies can beenhanced, how regulatory bodies responsi-ble for safeguarding quality perform, whatlegal restrictions exist, what can be learntacross bodies and what are the possibilitiesand constraints in respect of cross bordercare.
ConclusionThe Dutch presidency of the EU in theautumn of 2004 will be special, charac-terised by full membership of ten newMember States, complemented by a NewCommission and new EuropeanParliament. Furthermore, within the healthfield it will try to tackle in practical wayssome of the topics that will quickly gainprominence as a result of the formation ofnew policy goals, and because of the sheerscale of geographical enlargement.
eurohealth Vol 10 No 214
DUTCH PRESIDENCY
REFERENCES
1. McKee M, MacLehose L,Nolte E (eds). Health Policyand European EnlargementOpen University Press, 2004.
2. De Volkskrant 20 April2004.
As a preparatory activity, Polish andDutch twinners on the ‘mutual recognitionof the qualifications of health care profes-sionals’ decided to redevelop their 1-yearcelebration of twinning into a 2-day inter-national seminar with the title ‘From mutu-al recognition to mutual communication?Five months of the Internal Market in newMember States’. Participants from all thenew member states and elsewhere wereinvited to a seminar held in Warsaw inSeptember 2004.
“migration of health
care professionals is
and will remain an
issue on the EU
agenda”

eurohealth Vol 10 No 2 15
MEDIA AND HEALTH
We live in the age of the soundbite, whereboth print and broadcast media outlets arehighly fragmented, and the need to hookpotential consumers to maintain circulationand/or viewing ratings through eye catch-ing news stories has never been greater. Yetat the same time we also live in a world ofrolling 24 hour news coverage where sto-ries that once may have been covered for afew hours are constantly recycled, devel-oped and re-examined to unearth all possi-ble angles. It is a world where some healthrelated issues are widely covered, often fea-turing as lead stories in both print andbroadcast media.
Fostering good links between media out-lets, health policy makers and researcherscan potentially be very beneficial in gettingacross public health related messages: pro-viding information and dispelling mythsabout health care interventions and healthyliving.1 It can therefore be an excellent toolto help individuals make informed choiceson health related issues. In reality thoughthe picture seems to be one where goodcommunication between these groups is theexception rather than the rule, and wherethe focus tends to be on negative events,such as failing hospitals or the latest healthscare, rather than on positive health mes-sages.
Conveying the concept of risk in a waythat can be easily related to by a generalpublic whose knowledge and understand-ing of science is limited remains a chal-lenge. The risks associated with stories canbe blown out of all proportion. These diffi-culties have meant that coverage of healthstories can have disproportional adverseconsequences such as reducing the willing-ness of individuals to seek medical care orto use specific health promoting interven-tions. They may also have the potential toinfluence the eventual development of gov-ernment policy.
MMR controversyThis can perhaps best be illustrated by theongoing controversy in the UK over thesafety of the measles, mumps and rubella(MMR) vaccination and it’s possible linkswith bowel disease and autism.
Sensationalist reporting of the findings ofone published scientific paper had a dra-matic impact on the level of public confi-dence in the vaccine. Vaccination rates forinfants that had peaked at 92% in 1996, fellback to 84% by 2002, following negativepress coverage. The effects of this mediacoverage may be long lasting, one recentanalysis suggests that resistance to vaccina-tion is likely to remain high, despite amajor publicity and awareness campaign, asparents balance the risk of infection againstthe risk of vaccination. This study con-cludes that it will take a considerable timeto restore vaccination rates, in similar fash-ion to what transpired with the whoopingcough vaccine two decades earlier.2
A recent study funded by the Economicand Social Research Council in the UKassessed the media’s role in the publicunderstanding of science, based on ananalysis of both television, radio and pressnews on science in over a seven monthperiod, coupled with two nationwide sur-veys which looked at the public’s knowl-edge, opinion and understanding of sciencerelated issues reported in the media.3 Thestudy focused on MMR and two other wellreported issues, climate change andcloning/genetic medical research.
In all three cases while knowledge of theissues did not improve over the study peri-od, the authors noted that “what peopleknew usually corresponded with thoseaspects of the science stories that receivedmost persistent coverage. The details or sub-tleties of media coverage are, in this respect,much less important than the generalthemes of that coverage, in which certainideas are repeated and associated with oneanother. While this does mean some infor-mation is communicated effectively to mostpeople, it can also result in widespread mis-understanding – even if the reporting itselfis generally accurate.”
Of the three issues that were looked at,MMR had by far the biggest level of publicengagement, even though there were fewerarticles compared with the other twoissues. MMR was more likely to be thefocus of editorials and opinion pieces, and
Headlines and deadlines: the mediaand health issues
David McDaid is ResearchFellow, LSE Health and SocialCare and EuropeanObservatory on HealthSystems and Policies, at theLondon School of Economicsand Political Science. He isalso editor of Eurohealth. E-mail: [email protected]
David McDaid
“the focus tends to be
on negative events,
such as failing hospitals
or the latest health
scare”

covered by news reporters rather than sci-ence/health specialists, and furthermorestories were most likely to feature contri-butions by members of the public.Coverage of the MMR debate appeared tohave been skewed so that in spite of the factthe overwhelming body of evidence indi-cated that the vaccine was safe, the publicperceived that the scientific communitywere evenly split on the issue. Some news-papers even actively campaigned for singlevaccinations despite the lack of any evi-dence that this was a safer alternative. Thestudy concluded that “research questioningthe safety of something that is widely usedshould be approached with caution, both byscientists publishing that research and jour-nalists covering it. This is especially the caseif any decline in public confidence has nega-tive consequences for public health.” Thisview was shared by almost half of therespondents in their public survey.
Impact on resource allocation andpolicyThe impact of the MMR debate in the UKis by no means an isolated case of theadverse impact that media reports can havefor health. Another example, which hadimplications for resource allocation can beseen in Italy, following claims in the mediaof the success of what in reality was a newunproven treatment (di Bella) for a widerange of cancers. This publicity fuelledpublic demands for access to the treatment,leading to the health authorities providingfunding for a large scale trial, which ulti-mately was shown to be ineffective and awaste of a valuable resources, not to men-tion the false hope that it generated.4
In Canada, coverage in the press of therisks of the infection of blood productswith Creuzfeldt-Jakob disease (CJD), waslinked directly to changes in policy, poten-tially having both health and resource con-sequences.5 One newspaper reported state-ments by an American haemotologist giv-ing evidence to an inquiry on the bloodsystem; these were subsequently picked upthe Canadian newswire leading to stories ofa “new killer virus”. A chain of events ledto the Red Cross recalling all their bloodproducts, an event estimated to have cost11 million Canadian dollars and creatingshortages of some blood products. Inanalysing the views of journalists later itwas suggested that some felt that becausethey had not done enough previously toreport the potential risks of hepatitis C andHIV contamination of blood products,they over reacted in the case of CJD.
The nature of newsThe media can have an influence on healthbehaviour and ultimately on policies bothfor good and for bad. Principal challengesinclude improving the way in which infor-mation is communicated to the public, andin particular the concept of risk, as well asensuring that stories are based on goodquality information. Another challenge isto encourage the publication of less sensa-tional positive health stories and messages.However all this must be grounded with anunderstanding of the reality in which themedia must operate, and in particular whatconstitutes ‘news’.
It is important to distinguish between spe-cialist media outlets such as health maga-zines and documentary style in depth for-mat features about health issues, and evenfeatures buried deep within newspapers,with what will appear in headlines and bethe subject of rapid deadlines. For the for-mer, journalists are more likely to havesome expertise in the area, or to have dia-logue with experts, and there is typicallymore time to corroborate facts, and obtaina range of perspectives from stakeholdersincluding policy makers, scientists andhealth care professionals, patient groupsand the public. Moreover editorial deci-sion-making may remain in the hands of aspecialist ‘science’ or ‘health’ editor. Thereis much also to gain from the journalist’sperspective if they can develop a good rela-tionship with a reliable source of informa-tion on a variety of health related issues.
The greater challenge is faced at the sharpend of news production, where as studieshave shown, although detailed messagesmay not be assimilated by the public, keyperceptions of health issues such as MMRand CJD can be quickly formed, and rein-forced through constant repetition of asmall number of headlines, and perhapsdistorted views on an issue. For instance ananalysis of health news in the press, radioand television commissioned by the King’sFund6 calculated a crude number of deathsrequired for a story in the UK in order toraise the debate on the balance of healthnews coverage in the media. Whereas therewere more than 8,500 deaths due to smok-ing and 7,500 due to obesity for each relat-ed story covered, it took only 0.25 deathsfrom measles, 0.33 deaths from variantCJD and 19.56 deaths from AIDs per storycovered.
Barriers faced by journalistsThere are many difficulties to face. Can wereally expect journalists to change their
eurohealth Vol 10 No 216
MEDIA AND HEALTH
“Journalists will
always need to find
headline grabbing
stories”

focus of coverage? How can journalistsmeet the demands of their audience to pro-vide attractive and entertaining news sto-ries, while at the same time minimising thereduction in the quality of information?How can this take account of the limitedgeneral understanding of science?
One recent study convened two focusgroups of journalists writing on healthrelated issues in Sweden and the UK, andalso conducted surveys worldwide to iden-tify some of the challenges and barriers tothe communication of health messagesfrom the perspectives of the journalist.7
Respondents in the UK identified commer-cial pressures, and weak editorial controlwhere accuracy was not a major issue askey barriers, whereas in Sweden the lack oftime to prepare stories, the sheer volume ofinformation and the difficulty in findingreliable sources were all cited. Other barri-ers identified included a lack of knowledge,limited space for stories and too much ter-minology. The study highlighted the diffi-culties journalists can have in finding trulyindependent expert sources, as manyresearchers may have conflicts of interests,which may bias their responses, or at bestmean that they will only talk ‘off therecord’. It did though find that the journal-ists wanted to explore ways of improvingthe quality of information in their stories.
Meeting the challengeJournalists will always be faced by timepressures and the need to find headlinegrabbing stories, this is simply the natureof the news media. Researchers and policymakers cannot assume that the news shouldfeature positive health stories and have agreater focus on public health messages.The media operate in a different environ-ment where news worthiness does not takeaccount of such public health goals. This isnot to say though that there are not timeswhen public health and positive stories willnot be prominent in the news. Nor shouldit imply that is impossible to improve thequality of information used, or the way inwhich stories are reported so that risks andbenefits are communicated in a way thatcan be more easily understood by the gen-eral public. Unfortunately there is as yetlittle evidence as to which approaches maybe effective in achieving this modest goal.However it is reasonable to assume thattheories used for the dissemination ofknowledge more broadly are applicablehere as well.
This inevitably means that a number of dif-ferent mechanisms will need to be used,
perhaps most importantly strengtheningthe links between researchers and themedia. Researchers need to be aware of theconstraints faced by journalists includingtheir lack of time and limited knowledge ofan area. Research units, many of whom stilloften pay only lip service to the notion ofdissemination outside of academic publica-tions, need not only to set aside resourcesto prepare concise briefs for policy makers,but similarly should prepare sound, non-jargonistic and informative information forthe press.
There may also be some merit in runningshort courses for journalists to help themunderstand scientific jargon, and get a basicgrasp of the evidence based medicineapproach, including both it’s strengths andlimitations. This may also help them intheir interpretation of absolute and relativerisks and in the challenge of attributingoutcomes to specific interventions orpotential health risks. Another mechanismmay be for media organisations to draw upguidance for their staff when reporting onhealth issues.
While this will not change the understand-able need for headline grabbing stories itmay at least help promote balance and bet-ter communication of information on riskwhen a story breaks. It is in this early stagethat key public perceptions are formed onhealth issues, which, as is evident in thecase of MMR in the UK, may be difficultto change later on, in spite of an over-whelming body of scientific evidence.
eurohealth Vol 10 No 2 17
MEDIA AND HEALTH
REFERENCES
1. Grilli R, Ramsay C, Minozzi S. Mass media interventions: effects on healthservice utilisation (Cochrane Review). In: The Cochrane Library. Chichester:John Wiley & Sons Ltd, Issue 3, 2004.
2. Bauch C T, Earn D J D. Vaccination and the theory of games. Proceedingsof the National Academy of Sciences of the United States of America.2004;101(36):13391–94.
3. Hargreaves I, Lewis J, Speers T. Towards a Better Map: Science, the Publicand the Media. Economic and Social Research Council, 2003.
4. Benelli E. The role of the media in steering public opinion on healthcareissues. Health Policy 2003;63(2):179–86.
5. Wilson K, Code C, Dornan C, Ahmad N, Hebet P, Graham I. The report-ing of theoretical health risks by the media: Canadian newspaper reporting ofpotential blood transmission of Creutzfeldt-Jakob disease. BMC PublicHealth 2004;4(1):1–9.
6. Harrabin R, Coote A, Allen J. Health in the News: Risk, Reporting andMedia Influence. London: King’s Fund, 2003.
7. Larsson A, Oxman A D, Carling C, Herrin J. Medical messages in themedia – barriers and solutions to improving medical journalism. HealthExpectations 2003;6:323–31.
“Researchers need
to be aware of the
constraints faced by
journalists”
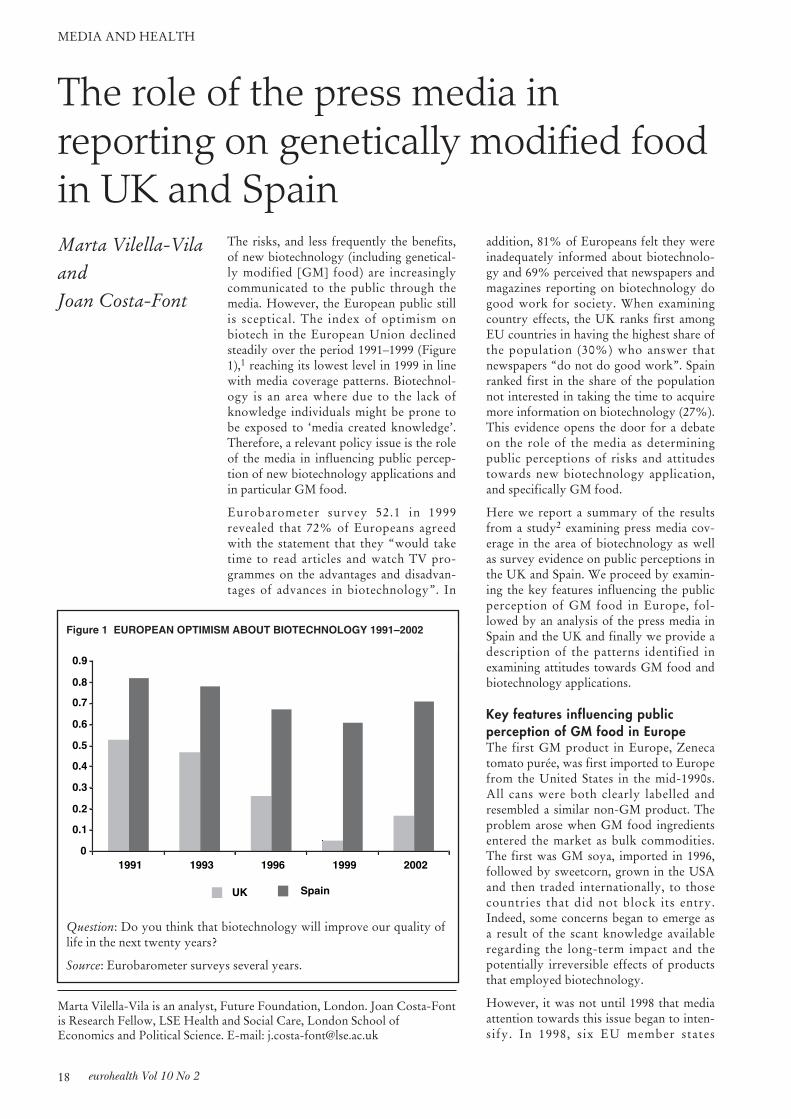
The risks, and less frequently the benefits,of new biotechnology (including genetical-ly modified [GM] food) are increasinglycommunicated to the public through themedia. However, the European public stillis sceptical. The index of optimism onbiotech in the European Union declinedsteadily over the period 1991–1999 (Figure1),1 reaching its lowest level in 1999 in linewith media coverage patterns. Biotechnol-ogy is an area where due to the lack ofknowledge individuals might be prone tobe exposed to ‘media created knowledge’.Therefore, a relevant policy issue is the roleof the media in influencing public percep-tion of new biotechnology applications andin particular GM food.
Eurobarometer survey 52.1 in 1999revealed that 72% of Europeans agreedwith the statement that they “would taketime to read articles and watch TV pro-grammes on the advantages and disadvan-tages of advances in biotechnology”. In
addition, 81% of Europeans felt they wereinadequately informed about biotechnolo-gy and 69% perceived that newspapers andmagazines reporting on biotechnology dogood work for society. When examiningcountry effects, the UK ranks first amongEU countries in having the highest share ofthe population (30%) who answer thatnewspapers “do not do good work”. Spainranked first in the share of the populationnot interested in taking the time to acquiremore information on biotechnology (27%).This evidence opens the door for a debateon the role of the media as determiningpublic perceptions of risks and attitudestowards new biotechnology application,and specifically GM food.
Here we report a summary of the resultsfrom a study2 examining press media cov-erage in the area of biotechnology as wellas survey evidence on public perceptions inthe UK and Spain. We proceed by examin-ing the key features influencing the publicperception of GM food in Europe, fol-lowed by an analysis of the press media inSpain and the UK and finally we provide adescription of the patterns identified inexamining attitudes towards GM food andbiotechnology applications.
Key features influencing public perception of GM food in EuropeThe first GM product in Europe, Zenecatomato purée, was first imported to Europefrom the United States in the mid-1990s.All cans were both clearly labelled andresembled a similar non-GM product. Theproblem arose when GM food ingredientsentered the market as bulk commodities.The first was GM soya, imported in 1996,followed by sweetcorn, grown in the USAand then traded internationally, to thosecountries that did not block its entry.Indeed, some concerns began to emerge asa result of the scant knowledge availableregarding the long-term impact and thepotentially irreversible effects of productsthat employed biotechnology.
However, it was not until 1998 that mediaattention towards this issue began to inten-sify. In 1998, six EU member states
eurohealth Vol 10 No 218
MEDIA AND HEALTH
The role of the press media in reporting on genetically modified foodin UK and Spain
Marta Vilella-Vila is an analyst, Future Foundation, London. Joan Costa-Fontis Research Fellow, LSE Health and Social Care, London School ofEconomics and Political Science. E-mail: [email protected]
Marta Vilella-Vilaand Joan Costa-Font
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1991 1993 1996 1999 2002
UK Spain
Figure 1 EUROPEAN OPTIMISM ABOUT BIOTECHNOLOGY 1991–2002
Question: Do you think that biotechnology will improve our quality oflife in the next twenty years?
Source: Eurobarometer surveys several years.

imposed an unofficial moratorium on theapproval of new varieties of GM crops. On14 February 1999, the bio-safety conven-tion to establish international regulationsgoverning GM organisms began inCartagena, Colombia. Again, GM foodscame dramatically to the public’s attentionwith the publication in 1999 of a statementsigned by 126 influential food writers andjournalists condemning the use of GMfoods. This initiative was promoted by theenvironmental organisation, Greenpeace.
In October 2001, German Agriculture/Consumer Affairs Minister Renate Künastand Environment Minister Jürgen Trittinwrote to the European Commission statingthat the moratorium should remain in placeuntil the revised GMO deliberate releasedirective came into force in October 2002and future traceability/labelling regulationswere clarified. In May 2003, PresidentGeorge W Bush launched a legal challengeto the EU at the World Trade Organisa-tion, to force Europe to accept imports ofUS GM crops. In July 2003 laws intendedto end a European Union-wide ban on newgenetically modified foods were passed bythe European Parliament. Europe’s Healthand Consumer Protection CommissionerDavid Byrne, told the EuropeanParliament: “I believe we have got in placelegislation … to enable consumers to makethe choice for themselves whether to con-sume GM foods or not”. Under the newlaw, all foods with more than 0.9 per centgenetically modified content will have to belabelled.
In the UK, the government launched apublic debate in June 2003. The aim was tolisten to the public’s views before decidingwhether to license GM crops in the coun-try. This is arguably the country’s firstnationwide public discussion around GMissues. Local authorities and networkgroups organised meetings to weigh up thepros and cons. The findings, along with theviews submitted to an internet site, werethen fed back to the government to helpinform their policymaking on GM. The sit-uation thus is now rather different to thatof the late-1990s, when the story of GMfood began to be written. Almost all foodin the shops is non-GM and it could beargued that it is those who would wish tobuy GM food that are being denied achoice. The new (2003) EU labelling regu-lations are now even stricter than beforeand consumers will finally have a choiceabout whether or not they aim to consumeproducts containing modified crops. Asnoted, in July 2003, the European
Parliament approved a new set of regula-tions that impose additional labellingrequirements on those wishing to sell anyfoods derived from GM sources.
Content analysis findings in the UKand Spanish pressPublic debate on genetically modifiedfoods has become highly polarised. Somegroups have set out to establish a less parti-san perspective by involving a range ofpeople with different viewpoints and work-ing towards consensus. In the meantime,the amount of media coverage has beenextensive, especially in the UK. Our find-ings indicate a great increase in coverage inEurope during early 1999. It is worth not-ing that after the peak in 1999, there wascertainly a reduction in the volume ofnewspaper coverage. Overall, this qualita-tive content analysis reveals that coveragein the UK and Spain has been characterisedby an extreme focus on risks and the poten-tial hazards to public health. Overall,European coverage is biased towards nega-tive effects, framing the reality of GM foodas a highly controversial issue. Thus, theBritish and Spanish media coverage is dri-ven mostly by controversy, as the domi-nant themes rarely display a positiveemphasis on the potential benefits of GMfood. The empirical evidence on mediacontent reveals that GM food is a topicalissue within the British press, as a high levelof reporting led GM food to become afront-page news story 13 times during 1999.Within a press that influences opinion lead-ers and policy makers, the theme emergesas a complex debate that involves manystakeholders, namely scientists, politiciansand state headquarters, food companies andother interested parties. All employ themedia as a risk communication tool.
In the UK there is a remarkable variationbetween broadsheet and tabloid reporting.Whereas The Guardian acts as a significantagenda-setter in the GM food debate, TheSun tabloid courts extensive popular atten-tion. Contrary to The Guardian’s broadand somewhat pedagogical coverage, itbecame noticeable that a detailed debatewas rarely found in The Sun. In a tabloid,there is no pretension of generating a richdebate among the counterparts involvedand the language constantly aims at rein-forcing the idea of “Frankenstein food”and “mutant food”. Unlike the UK, GMfood was not reported as a topical issue bythe Spanish press, where there was less cov-erage, resulting in less controversy, withcomparatively poor public debate. In Spain,
eurohealth Vol 10 No 2 19
MEDIA AND HEALTH
“a important policy
issue is the role of the
media in influencing
public perception”

where the tabloid press does not exist inthe same way as in the UK, the results ofcontent analysis among the different news-papers’ appear fairly diluted. We looked atwhether this media reality corresponds toreaders’ perceptions, in showing them to becloser in knowledge, attitudes and riskawareness.
Attitudes and public perception ofGM foodThe evidence examined suggests that bothpeople in the UK and in Spain envisage theuse of modern technology in the produc-tion of foods to be a decidedly risky busi-ness. On the other hand, research showsthat the lay public perceive some biotechprocedures as beneficial, since their usemay make it possible to feed more peoplein a more efficient way ultimately benefit-ing consumers, but simultaneously poten-tial human risks and ethical concerns arerecognised to be causing anxiety.
Trust in stakeholders plays a meaningfulrole in influencing safety concerns. In boththe UK and Spain, the sources of informa-tion most trusted by the public are themedical profession, consumer and environ-mental organisations. On the other hand,the media ranks among the least trusted.Therefore, it is worth pointing out thatalthough the media is often regarded asresponsible for socially amplifying risk, ifthey are among the least trusted stakehold-ers one might expect to find readers to bemore critical with the information reported.Thus, a lack of trust might be a key elementin the role of the media in influencing atti-tudes. Distrustfulness is especially relevantamong UK society, where 30% declare thatnewspapers “do not do good work”.
The newspapers examined highlight howdifferent journalistic treatment and cover-age has an influence in public perceptionsof GM food and biotechnology in generalAttitudes and perceptions of risk in the UKappear to be different when consideringthose people who read The Sun or TheGuardian. Sun readers exhibit higher dis-agreement with GM food and their riskperceptions are also lower. In contrast,Guardian readers appear to be more awareof the potential risks of GM food and con-sequently, their attitudes tend to be morenegative. In Spain, general attitudes appearto be similar regardless of the newspaperconsidered. Here, where tabloid press doesnot exist, the disparities among consumersof different newspapers appear to be ratherweak, as they are found to be closer inknowledge, attitudes and risk perception.
Policy implicationsInformation sources and organs of media-tion, the media among them, will be keyactors in influencing public perceptions ofGM food. Therefore, substantive effortsneed to be made to communicate risks inorder to allow individuals to makeinformed decisions. Content analysisbetween a sample of the UK and Spanishpress exhibits substantial differences inboth the amount of news and the publicdebate generated. The more limited sup-port for GM food in the UK coincides witha major social debate played out in themedia, which appears to have negativelyinfluenced public acceptance of GM food.Furthermore, perceptions of risk on GMfood have increased in line with newsreporting. However there is still little evi-dence to set up a direct cause-effect rela-tionship between negatively biased newsand the lack of public trust in the field.Furthermore, it should be acknowledgedthat scepticism in Europe might be partlythe consequence of the BSE crisis and otherfood scares.
Several policy implications can be drawnfrom our study:
First, informing the public about the risksand benefits on issues that constrain cur-rent and future innovation should beundertaken in the light of known individ-ual psychological responses.
Second, governments and the EuropeanUnion should make use of existing policytools to overcome market failures resultingfrom a public lack of knowledge andunderstanding of biotechnology.
Third, if risk communication is to rely ontrusted channels, then if as we find themedia does not stand among the mosttrusted information channels, other societalstakeholders, namely the medical profes-sion and consumer and environmentalorganisations might be employed.
Further, the media, however, should beencouraged to provide information onbiotechnology in a way that convinces thepublic of both the benefits and the risks.Accordingly, it is possible that some incen-tives should be introduced into the marketto reduce the temptation for journalists toprovide ambiguous although sometimessensational information.
Finally, a key information source is educa-tion. The technical nature of biotechnologyinformation might generate the need toprovide the public with better education onscientific developments.
eurohealth Vol 10 No 220
MEDIA AND HEALTH
REFERENCES
1. Gaskell G, Allum N,Stares S. Europeans andBiotechnology in 2002. Areport to the EC DirectorateGeneral for Research from theproject ‘Life Sciences inEuropean Society’ QLG7-CT-1999-00286, March 2003.
2. Vilella-Villa M, Costa-FontJ. The media influence in pub-lic risks perceptions of GMfood in the UK and Spain.LSE Health and Social Care,Discussion Paper Series No.12, 2004.
“a lack of trust is a
key element in the
influence of the
media on attitudes”

eurohealth Vol 10 No 2 21
HEALTH CARE REFORM
IntroductionStarting in the late 1980s, Social HealthInsurance (SHI) systems in WesternEurope sought to develop and/or applynew organisational approaches capable ofconstraining overall expenditures. Underincreasing fiscal pressure and anxious toachieve more market-style levels of operat-ing efficiency, these systems experimentedwith a variety of different demand-sidemechanisms. On closer consideration,however, many of the more sweeping pro-posals were found to be incompatible withcore commitments to solidarity in accessand treatment, and, over time, were modi-fied or dropped.1
This interest in the potential advantages ofdemand-side reforms continued to evolveduring the 1990s. Several market-derivedmeasures were adopted in countries likeGermany (choice of sickness fund) and theNetherlands (choice of sickness fund; nom-inal flat-rate premiums). Switzerland’s SHIsystem, introduced in 1996, contained avariety of choice and competition-orientedmeasures.2 Most recently, existing mea-sures have been supplemented by a varietyof additional, typically voluntary experi-ments and/or sick fund-initiated pilot pro-jects. The range and scope of these newapproaches suggest the possibility that anew period of reform may be germinating,one in which the market-oriented changesmay be less global in character, yet stillpotentially in conflict with traditional com-mitments to solidarity.
Recent mechanismsThe range of demand-side mechanisms cur-rently in use or under development in pilotprojects includes a number of approachesthat appear to reflect a new policy depar-ture for SHI systems. These can begrouped into four distinct categories:
1. Provider networks and/or selective con-tracting
Sickness funds shift from broad open-ended contracts with all providers to speci-fied arrangements with selected physiciansand/or hospitals. In return for voluntaryadherence to this sub-set of providers,patients receive better continuity of care(clinical benefit) but normally no financialbenefit (Switzerland is an exception).Sickness funds hope these networks willreduce unnecessary care and thus reduceoverall expenditures.
2. Large up-front deductibles
A form of cost-sharing, deductibles requiresubscribers to pay 100% of initial medicalcosts up to a pre-set ceiling. As with motoror property insurance, subscribers whoelect higher deductibles have increased self-risk, and, therefore, receive a reduction intheir premium.
3. No-claim bonuses
A no-claim bonus rewards the subscriberfor not using services. Rewards can take awide variety of forms (partial reimburse-ment of a paid premium, lower future pre-miums or bonus credits exchangeable forgoods). No-claim bonuses give the sub-scriber a financial incentive not to use ser-vices, or, if feasible, to pay out-of-pocketfor occasional use. The mandatory slidingno-claim bonus currently proposed in theNetherlands would institute a special typeof no-claim bonus, resembling a deductible.
4. Flat-rate premiums
Flat-rate premiums require the insured topay the same amount regardless of income.These differ dramatically from the normalarrangement in SHI systems, collected as apercentage of wages up to an income ceil-ing. The traditional approach, while notprogressive in its impact on equity, is onlymildly regressive.3 Flat-rate premiums arehighly regressive.
Country experienceExperiments and/or pilot projects withthese four types of individual incentiveschemes are currently ongoing inGermany, the Netherlands, and
Individual incentive schemes in socialhealth insurance systems
Richard B Saltman is Professor of Health Policy and Management, RollinsSchool of Public Health, Emory University, Georgia, USA, and ResearchDirector of the European Observatory on Health Systems and Policies,Ministerio de Sanidad y Consumo, Madrid.
Hans FW Dubois is Research Officer, the European Observatory on HealthSystems and Policies, Ministerio de Sanidad y Consumo, Madrid. E-mail:[email protected] or [email protected]
Richard B Saltmanand Hans FW Dubois
“market-oriented
changes are potentially
in conflict with
traditional
commitments to
solidarity.”

Switzerland as well as (to a lesser degree)France. Since the application in each coun-try differs, this section looks more closelyat specific country approaches.
Provider networks and selective contracting
German law hardly allowed sickness fundsto negotiate individual physician contractsprior to the implementation of GKV-Modernisierungsgesetz on 1 January 2004.However, this new law now expandsprovider-contracting possibilities, allowingfor individual contracts with medical cen-tres with salaried doctors, and individualcontracts with organisations that offer inte-grated clinical services. The new law alsostipulates that 1% of total payments toproviders should be directed to these inte-grated care initiatives.
Germany has had physician networks inthe narrow sense since the late 1980s. Thereare also physician networks with emer-gency services and coordinated timetables,and practice networks with integrated careassociated with hospitals. Examples of thelatter are the Diagnostischen Zentrums inPapenburg and the AOK networkPraxisnetz Nürnberg Nord. A special casewas the Praxisnetz Berlin where the indus-try sickness fund association (BKK) wasactively involved (although since 2003 sev-eral German sickness funds also participatein Regional Disease ManagementProgrammes). This project began in 1996,however it was unable to attract large num-bers of patients, and in 2002 was discontin-ued. Patients were asked to join voluntarilyand, while better continuity of care wasprovided, there were no financial incen-tives.
A successor project was set up inNordrhein-Westfalen in January 2004. Itdiffers from the Berlin project in that itintends to concentrate only on patientswith three severe conditions (breast cancer,coronary disease, and a need fororthopaedics), and it will work with highquality clinics and use treatment patternsbased on best practice. It is presumed thatpatients will have less incentive to shoparound, and that the financial benefit ofhaving longer-term contracts with clinicswill outweigh extra treatment costs. Theproject started only with 5 of the 220 BKKsickness funds, but if deemed successful,the model will be applied to all BKKfunds.*
In France, since the beginning of 1998, anoptional gate-keeping system in ambulato-ry services exists. If patients choose a GP
acting as a gatekeeper, those patients with-out complementary health insurance (thatcovers GP fees) no longer have to pay theentire visit fee up front, but only the ticketmodérateur (about 1/3). The médecinsréférents, as participating GPs are called,receive the balance directly from the socialsecurity system. Patients benefit clinicallyfrom better continuity of care.4,5 Themédecin référent benefits financially,receiving a fixed amount per year perpatient enrolled (for 2004 this amount is€45.74).* In September 2003, 6,363 physi-cians participated (about 12% of all FrenchGPs), and the number of patients partici-pating has nearly doubled since 2000,reaching 1,032,760, or 1.7% of the Frenchpopulation.6 The impact of these arrange-ments on health care costs and qualityseems to be marginal so far,5 and consulta-tions seem to be slightly higher for partici-pating physicians, but there are signs thatmédecins référents prescribe less while theirpatients are typically older and high-cost-diseases are more frequent among themthan is the case for other GPs.7
In the Netherlands, both the sickness fundAGIS and the private company, AlantMedical, are experimenting with integratedcare concepts. Since 2000, AGIS (1.5 mil-lion sickness fund insured, about 15% ofall Dutch sickness fund insured) has beendeveloping a preferred provider project fordiabetes patients. The first phase involvedsome 6,000 patients in Amsterdam as ofApril 2003. The next phase will be largerand AGIS will reward providers withbonuses tied to outcomes (physiologicalindicators, quality of life, consumer sur-veys). All AGIS insured with diabetes canchoose to participate if they are willing tolimit their diabetes-related visits to the con-tracted group of ‘best practice’ providers.As Dutch law does not allow premium dif-ferentiation within one sickness fund,patients receive no financial benefit.Nevertheless, the long-term purpose of theproject is to offer such a premium discountas soon as the law allows it.* Alant Medicalalso is experimenting with integrated carearrangements, which it offers to sicknessfunds. They consist of specialised clinicsfor prevention of coronary diseases and forwomen’s health.*
In all three countries, France, Germany,and the Netherlands, patients can still optto go to a doctor outside the network with-out penalty. The Swiss case is different.Swiss sickness funds are allowed to offercertain legally determined premium dis-counts to those insured who choose to
eurohealth Vol 10 No 222
HEALTH CARE REFORM
“In France, Germany
and the Netherlands
patients can visit a doc-
tor outside the network
without penalty…Swiss
sickness funds can offer
discounts to those who
are willing to restrict
provider choice”.

restrict provider choice by participating ina provider network. The first such network(HMO-Gruppenpraxen) was established in1990.8 One year earlier, the Bundesrat cre-ated the legal framework that allowed forexperimental implementation of alternativeforms of health insurance. The 1994 HealthInsurance Law (KVG) legalised networkconstructions from 1 January 1996 for allsickness funds. Currently, different config-urations of provider networks exist overthe whole spectrum: from loose networksto full staff model HMOs.9 More than2,000 doctors and, on 12 December 2002,7.6% of the insured participate in one ofthese networks.10 Patients are restricted intheir choice of provider to, typically, 5–7doctors, but sometimes more than 30 as inGeneva, working in the group (GPs andsome specialists), and are referred to otherspecialists if needed. In return, patientsreceive a premium discount of between 8and 25%.* There are signs that solidarityhas been affected as these networks appearto encourage risk selection.9,11
Upfront deductibles
In Switzerland, all sickness fund sub-scribers have an initial deductible each year.The amount was set at 230 SFr since 1January 1998, but has been increased to300SFr as of 1 January 2004. While option-al deductibles have existed since 1987, the1996 compulsory sickness insurance actgave all Swiss the possibility to opt for ahigher deductible of (for adults): SFR 400,600, 1200 or 1500. In return, a discountedpremium is offered. These discounts werereduced on 1 January 2004 when the newminimum deductible was introduced.Now, they amount respectively to 3, 9, 24and 30%.* Between 1994 and 2002 the per-centage of insured choosing to participatein one of the four higher deductibleschemes increased steadily from 9.0% to40.5%.10
Since 1 January 2004, some BKK sicknessfunds in Germany also offer deductibles.The highest income insured can elect eithera deductible or a no-claim bonus scheme(see below). Beyond the mandatory enrol-ment period of one year, sickness fundshave considerable freedom in designing thesystem. An example is the Bayer BKKwhich offers a maximum deductible of€750 for 2004 in return for a €600 premiumdiscount if no care is used during a year(preventive care is excluded). This arrange-ment is intended to restrain voluntarilyinsured members from switching to com-mercial health insurers.*
No-claim bonuses
In Switzerland no-claim bonuses have beenallowed since 1990.* Subscribers have theoption to enroll in a five-year schemewhich charges a 10% higher initial premi-um, but each subsequent year offers anincreasing premium discount if no servicesare used. The largest insurer (CSSVersicherung, covering 1.2 million people,about 15% of the Swiss population) imple-mented this tiered bonus system on 1January 1993, however, the number of per-sons enrolled never exceeded 300 anddecreased steadily to 227 in 2003.* In 1995,only 0.46% of the overall Swiss populationsubscribed to this voluntary scheme, a per-centage that fell to 0.12% of the Swiss pop-ulation in 2002.10
While in 1989 and 1990 there were someexperiments with paying back contribu-tions by private insurance companies inGermany, sickness funds were onlyallowed to experiment with no-claimbonuses from the late 1990s. The AOKsickness funds started a pilot project in1996 in Hamburg with a no-claim bonus(some other pilot projects followed). In1998 the project was cancelled, when itbecame clear that only a few healthy AOKinsured would benefit from the scheme.
Since 1 January 2004, German law hasallowed sickness funds to offer a voluntaryno-claim scheme. So far, several AOK andBKK funds introduced some variation ofthe system. The government determinedthat it should only apply to the highest-income participants: those who earnincomes above the mandatory ceiling andthen voluntarily choose to remain in thestatutory system. The thinking is that thislimitation protects lower income sub-scribers from abstaining from necessarycare for financial reasons. A spokespersonof the AOK expects the concept to beexpanded in the future to a broader rangeof sickness fund insured, as inSwitzerland.* Sickness funds are free todesign key aspects of the scheme. SeveralAOK funds introduced systems thatreward patients with financial bonuses forpreventive measures (for example, immuni-sation, healthy life style, etc.), while otherfunds reward their insured with bonuscredits (exchangeable for goods).
Thus far, no-claim bonuses have been vol-untary. The Dutch proposal for a mandato-ry, sliding, no-claim bonus, if approved byParliament, will change this (see Table 1).Subscribers will be reimbursed by theirsickness fund for a certain part of the pre-
eurohealth Vol 10 No 2 23
HEALTH CARE REFORM
“So far, no-claim
bonuses have been
voluntary, the Dutch
proposal will change
this”.
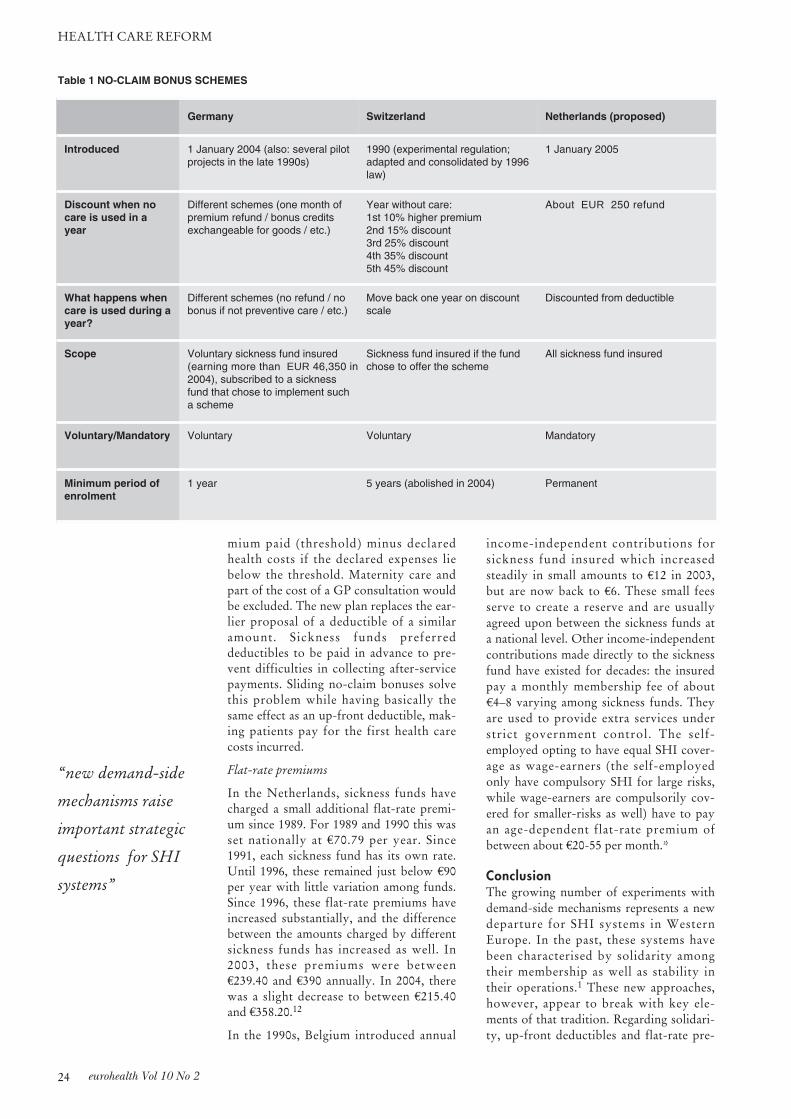
mium paid (threshold) minus declaredhealth costs if the declared expenses liebelow the threshold. Maternity care andpart of the cost of a GP consultation wouldbe excluded. The new plan replaces the ear-lier proposal of a deductible of a similaramount. Sickness funds preferreddeductibles to be paid in advance to pre-vent difficulties in collecting after-servicepayments. Sliding no-claim bonuses solvethis problem while having basically thesame effect as an up-front deductible, mak-ing patients pay for the first health carecosts incurred.
Flat-rate premiums
In the Netherlands, sickness funds havecharged a small additional flat-rate premi-um since 1989. For 1989 and 1990 this wasset nationally at €70.79 per year. Since1991, each sickness fund has its own rate.Until 1996, these remained just below €90per year with little variation among funds.Since 1996, these flat-rate premiums haveincreased substantially, and the differencebetween the amounts charged by differentsickness funds has increased as well. In2003, these premiums were between€239.40 and €390 annually. In 2004, therewas a slight decrease to between €215.40and €358.20.12
In the 1990s, Belgium introduced annual
income-independent contributions forsickness fund insured which increasedsteadily in small amounts to €12 in 2003,but are now back to €6. These small feesserve to create a reserve and are usuallyagreed upon between the sickness funds ata national level. Other income-independentcontributions made directly to the sicknessfund have existed for decades: the insuredpay a monthly membership fee of about€4–8 varying among sickness funds. Theyare used to provide extra services understrict government control. The self-employed opting to have equal SHI cover-age as wage-earners (the self-employedonly have compulsory SHI for large risks,while wage-earners are compulsorily cov-ered for smaller-risks as well) have to payan age-dependent flat-rate premium ofbetween about €20-55 per month.*
ConclusionThe growing number of experiments withdemand-side mechanisms represents a newdeparture for SHI systems in WesternEurope. In the past, these systems havebeen characterised by solidarity amongtheir membership as well as stability intheir operations.1 These new approaches,however, appear to break with key ele-ments of that tradition. Regarding solidari-ty, up-front deductibles and flat-rate pre-
eurohealth Vol 10 No 224
HEALTH CARE REFORM
Germany Switzerland Netherlands (proposed)
Introduced 1 January 2004 (also: several pilotprojects in the late 1990s)
1990 (experimental regulation;adapted and consolidated by 1996law)
1 January 2005
Discount when nocare is used in ayear
Different schemes (one month ofpremium refund / bonus creditsexchangeable for goods / etc.)
Year without care:1st 10% higher premium2nd 15% discount3rd 25% discount4th 35% discount5th 45% discount
About EUR 250 refund
What happens whencare is used during ayear?
Different schemes (no refund / nobonus if not preventive care / etc.)
Move back one year on discountscale
Discounted from deductible
Scope Voluntary sickness fund insured(earning more than EUR 46,350 in2004), subscribed to a sicknessfund that chose to implement sucha scheme
Sickness fund insured if the fundchose to offer the scheme
All sickness fund insured
Voluntary/Mandatory Voluntary Voluntary Mandatory
Minimum period ofenrolment
1 year 5 years (abolished in 2004) Permanent
Table 1 NO-CLAIM BONUS SCHEMES
“new demand-side
mechanisms raise
important strategic
questions for SHI
systems”

miums are highly regressive in that lower-income members have proportionally high-er costs. No-claim bonuses encouragepatients to not seek care (or potentially topay out-of-pocket) in order to obtain afinancial benefit, an incentive that, again,typically has a stronger attraction forlower-income subscribers. Selective con-tracting creates the potential for a multi-tiered system, differentiated initially byquality of care, but potentially, if tied toany of the other three mechanisms, byfinancial status. Regarding stability, intro-ducing price differentials for individualsubscribers can trigger self-selection andadverse selection in patterns that under-mine collective insurance. Thus, it wouldappear that these new demand-side mecha-nisms raise important strategic questionsabout the likely long-term consequencesfor SHI systems.
Several mitigating circumstances should benoted, however. First, these measures so farhave not been generalised to the entire pop-ulation (the additional flat-rate premium inthe Netherlands is an exception). Second,they thus far involve only voluntary partic-ipation by patients (again, the Netherlandsmay soon be an exception). Third, the sumsinvolved are relatively small, with mosthealth system funding still tied to the tradi-tional percentage-of-income arrangement.Moreover, in Germany, the sickness fundsare already compensated by the nationalrisk adjustment scheme for those enrolledin a disease management programme.
Finally, these new measures are not beingutilised within all SHI systems. Thus far,there has been no movement toward suchexperiments in Austria and Luxembourg(where subscribers have no choice of sick-ness fund) or in Belgium (where the ideo-logical roots of sickness fund membershipremain undiluted).
Despite these caveats, however, there maybe legitimate concern that these demand-side mechanisms represent a break with theprevious SHI understanding of solidarity.Some observers worry, for example, thatthe Dutch (AGIS) and German (BKK)experiments may be laying the groundworkfor more fundamental health system re-structuring.
REFERENCES
1. Saltman RB, Busse R, Figueras J. SocialHealth Insurance Systems in WesternEurope. Buckingham/Philadelphia: OpenUniversity Press, 2004.
2. Minder A, Schoenholzer H, Amiet, M. In:A Dixon (ed) Health Care Systems inTransition: Switzerland. Copenhagen:European Observatory on Health Systemsand Policies, 2000.
3. Wagstaff A, Van Doorslaer E, Van derBurg H, et al. Equity in the finance of healthcare: some further international compar-isons. Journal of Health Economics1999;18:263–90.
4. Aguzzoli F, Aligon A, Com-Ruelle L,Frézot L. Choisir d’avoir un médecinréférent: une analyse realisée à partir du pre-mier dispositif en place début 1998. Bulletind’information en économie de la santé, ques-tions d’économie de la santé. 1999; 23.www.credes.fr/Publications/Bulletins/QuestEco/pdf/qesnum23.pdf
5. Or Z. Improving the Performance ofHealth Care Systems: From Measures toAction (A Review of Experiences in FourOECD Countries). Paris: OECD Labourmarket and social policy – occasional papers,2002, Number 57.
6. ERASME. Bilans de l’option convention-nelle medecin referent: Tableaux recapitulat-ifs. Paris: ERASME, 2004.
7. CNAMTS. Les Médecins Référents en2002. Paris: CNAMTS, 2004.
8. Weber A. HMOs und Hausartzmodelle[HMOs and GP models]. In: M Egli (ed).Lehrgang Gesundheitswesen Schweiz,Chapter 4.4, Hünenberg: Trend Care, 2000.
9. Klingenberger D. Health MaintenanceOrganisations in der Schweiz: Darstellungund Kritik. IDZ-Forschung 2002;1.www.wzn.de/hmo-schweiz.pdf
10. Bundesamt für Gesundheit. Statistiek derObligatorische Krankenversicherung 2002.Table 1.05. Berne: Bundesamt fürGesundheit, 2004.www.bag.admin.ch/kv/statistik/d/2004/KV_2002.pdf
11. Beck K, Spycher S, Holly A, Gardiol L.Risk adjustment in Switzerland. HealthPolicy 2003;65:63–74.
12. Ministerie van Volksgezondheid,Welzijn en Sport. Nominale premie [Flat-rate premium], database. Den Haag:Ministerie van Volksgezondheid, Welzijn enSport, 2004.
eurohealth Vol 10 No 2 25
HEALTH CARE REFORM
* ACKNOWLEDGEMENT: We would like to thank the following for informa-tion and comments: Aldien Poll (AGIS), Jaap Maljers (Alant Medical),Anne-Kathrin Haas (AOK-Bundesverband), Beatrix Grohn and BeateMännel (BKK-Bundesverband), Dirk Van Herzele (Christelijke MutualiteitMidden-Vlaanderen), Beat Haeflinger (CSS), Marie-Odile Safon (l’IRDES),Frans van Zon (Ministerie van Volksgezondheid, Welzijn en Sport), HermanDevis (Socialistische Mutualiteit Antwerpen) and Patricia Leiber and UrsulaScherrer (Swiss Federal Office for Public Health).
“Observers worry, that
Dutch and German
experiments may be
laying the groundwork
for more fundamental
health system
restructuring.”
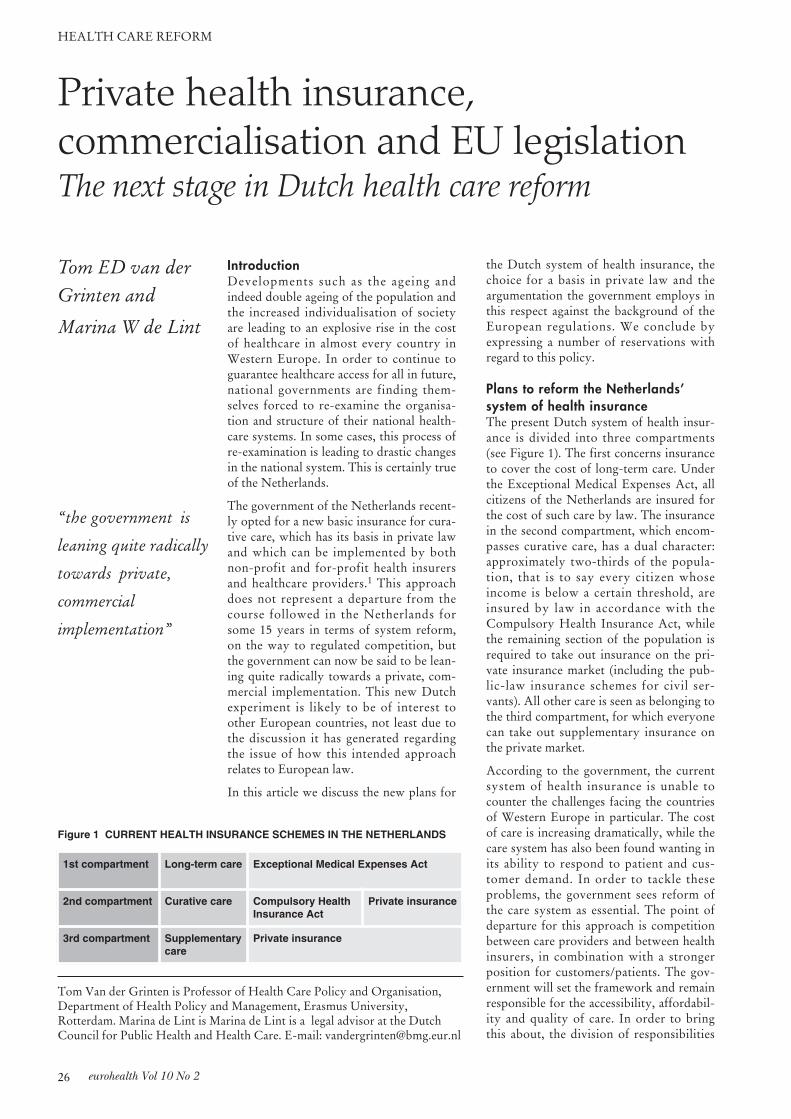
IntroductionDevelopments such as the ageing andindeed double ageing of the population andthe increased individualisation of societyare leading to an explosive rise in the costof healthcare in almost every country inWestern Europe. In order to continue toguarantee healthcare access for all in future,national governments are finding them-selves forced to re-examine the organisa-tion and structure of their national health-care systems. In some cases, this process ofre-examination is leading to drastic changesin the national system. This is certainly trueof the Netherlands.
The government of the Netherlands recent-ly opted for a new basic insurance for cura-tive care, which has its basis in private lawand which can be implemented by bothnon-profit and for-profit health insurersand healthcare providers.1 This approachdoes not represent a departure from thecourse followed in the Netherlands forsome 15 years in terms of system reform,on the way to regulated competition, butthe government can now be said to be lean-ing quite radically towards a private, com-mercial implementation. This new Dutchexperiment is likely to be of interest toother European countries, not least due tothe discussion it has generated regardingthe issue of how this intended approachrelates to European law.
In this article we discuss the new plans for
the Dutch system of health insurance, thechoice for a basis in private law and theargumentation the government employs inthis respect against the background of theEuropean regulations. We conclude byexpressing a number of reservations withregard to this policy.
Plans to reform the Netherlands’ system of health insuranceThe present Dutch system of health insur-ance is divided into three compartments(see Figure 1). The first concerns insuranceto cover the cost of long-term care. Underthe Exceptional Medical Expenses Act, allcitizens of the Netherlands are insured forthe cost of such care by law. The insurancein the second compartment, which encom-passes curative care, has a dual character:approximately two-thirds of the popula-tion, that is to say every citizen whoseincome is below a certain threshold, areinsured by law in accordance with theCompulsory Health Insurance Act, whilethe remaining section of the population isrequired to take out insurance on the pri-vate insurance market (including the pub-lic-law insurance schemes for civil ser-vants). All other care is seen as belonging tothe third compartment, for which everyonecan take out supplementary insurance onthe private market.
According to the government, the currentsystem of health insurance is unable tocounter the challenges facing the countriesof Western Europe in particular. The costof care is increasing dramatically, while thecare system has also been found wanting inits ability to respond to patient and cus-tomer demand. In order to tackle theseproblems, the government sees reform ofthe care system as essential. The point ofdeparture for this approach is competitionbetween care providers and between healthinsurers, in combination with a strongerposition for customers/patients. The gov-ernment will set the framework and remainresponsible for the accessibility, affordabil-ity and quality of care. In order to bringthis about, the division of responsibilities
eurohealth Vol 10 No 226
HEALTH CARE REFORM
Private health insurance, commercialisation and EU legislationThe next stage in Dutch health care reform
Tom Van der Grinten is Professor of Health Care Policy and Organisation,Department of Health Policy and Management, Erasmus University,Rotterdam. Marina de Lint is Marina de Lint is a legal advisor at the DutchCouncil for Public Health and Health Care. E-mail: [email protected]
Tom ED van derGrinten and
Marina W de Lint
1st compartment Long-term care Exceptional Medical Expenses Act
2nd compartment Curative care Compulsory HealthInsurance Act
Private insurance
3rd compartment Supplementarycare
Private insurance
Figure 1 CURRENT HEALTH INSURANCE SCHEMES IN THE NETHERLANDS
“the government is
leaning quite radically
towards private,
commercial
implementation”

needs to be modified and the associatedinstruments must be reviewed.
In terms of the health insurance system, thegovernment believes it is essential to aban-don the dual insurance structure in the sec-ond compartment and replace it with a sin-gle general insurance provision for curativecare (and that this new insurance should beintegrated with the existing ExceptionalMedical Expenses Act provision in the longterm). This is because there are major dif-ferences between the compulsory forms ofhealth insurance set out in the CompulsoryHealth Insurance Act on the one hand andthe private health insurance schemes on theother hand.
First of all, there is the legal basis for theinsurance: the former are public-law insur-ance provisions, which means that every-one who meets certain criteria laid downby law is insured. This also means that thelaw imposes obligations on the organisa-tions that implement these compulsoryforms of insurance, such as the duty ofacceptance, the obligation to offer a clearlydefined basic package and obligatory par-ticipation in an equalisation fund. Privatehealth insurance schemes, on the otherhand, have their legal basis in private law:insured status is not determined directly bylaw but by an insurance agreement betweenthe insurer and the policy holder. In princi-ple, the insurer is free to determine the con-ditions under which he is prepared to enterinto such an agreement (with the exceptionof policies under the Health InsuranceAccess Act).
A second important difference betweenthese two types of insurance is that theorganisations that implement theCompulsory Health Insurance Act are sub-ject to a not-for-profit regulation notapplicable to the private insurers. Doingaway with these differences creates a levelplaying field for health insurers in the sec-ond compartment, thereby strengtheningthe desired competition.
The government’s aim of removing theduality in the second insurance compart-ment enjoys wide-ranging support and isnot subject to discussion. However, there iscontroversy surrounding the type of actionto be taken in this regard. In order to doaway with this duality, there are in fact twooptions available: a public-law approach(along the lines of the current compulsoryhealth insurance funds) and a private-lawapproach (along the lines of the current pri-vate health insurance). The government hasopted for the second approach, a contro-
versial choice because it represents a radicalshift in the way typical government tasksare carried out. Since the advent of the wel-fare state, the Dutch government has man-aged the structure, organisation and imple-mentation of social health insurance as partof the social security system, sharingresponsibility with the social partners andorganisations in the field (an approachknown as neo-corporatism). Now, howev-er, the government has put considerablefaith in private initiative and commerce,without being able to fully foresee whatconsequences this move will have for howthe system functions.
One possible consequence of the govern-ment’s choice deserves to be examined par-ticularly closely, since it forms the focusfor the discussion in the Netherlands.Various observers have pointed out that thechoice for the private-law approach bringswith it the risk that the European Union’sinternal market regulations will apply infull to the new health insurance, therebyundermining the foundation of income sol-idarity and risk solidarity upon which thesystem is based. A particular concern inthis regard is that the new health insurancewill fall within the scope of Europe’s regu-lations governing private insurance, thenon-life directives.
EU legislation and health insuranceThe Member States of the European Unionhave the power to structure their ownsocial security systems as they see fit.However, recent legal precedents set by theEuropean Court of Justice have made itclear that even health insurance systems,which are clearly identified as part of a sys-tem of social security, are not exempt fromEuropean influence.2 It therefore seemslikely that this influence will extend furtheras more market-related elements are incor-porated into a social security system.3
The government plans in question havebeen designed with the express intention ofincreasing the influence of the market onthe health insurance sector, as attested bysuch measures as the prospective private-law basis, commercial implementation andfull nominal premium. At the same timethe government also wants to anchor thesystem firmly in social parameters (risk andincome solidarity) by regulating the con-duct of those implementing the new insur-ance. It is at this point that the above-men-tioned non-life directives appear on thehorizon. These directives are based on thetreaty provisions for the free movement ofservices and freedom of establishment and
eurohealth Vol 10 No 2 27
HEALTH CARE REFORM
“will the non-life
directives apply to the
new standard insurance
for curative care?”

are intended to encourage these freedomsin the non-life insurance sector. The non-life directives forbid Member States fromintervening in the general and specific con-ditions of a non-life insurance policy. Thismeans that in principle a national govern-ment cannot impose obligations on privateinsurers.
The question that has come to concern theNetherlands is whether the non-life direc-tives will in fact apply to the new standardinsurance for curative care. The third non-life directive does not apply to forms ofinsurance which are part of a statutorysocial security system (Article 2, paragraph2). It is up to the European Court to decideon the applicability of this social securitystipulation, as set out in the non-life direc-tive, based on substantive criteria and noton the qualification given by a MemberState itself. In the case of the Commissionagainst Belgium (C-206/98), the Courtruled that this article must be interpreted insuch a way that this directive applies toinsurance provisions implemented byinsurance companies at their own cost andat their own risk within the framework of astatutory social security system.
None of the parties to the discussion in theNetherlands dispute the fact that, in princi-ple, this ruling must mean that the newstandard insurance falls within the scope ofapplication of the non-life directives. Afterall, the express aim of the Dutch reforms isthat the organisations implementing thisinsurance will compete with one anotherand that taking financial risks is essential tothis process.
What is subject to discussion, however, iswhether the Netherlands can appeal to theexemption clause in the third non-lifedirective, thereby ensuring that the non-lifedirectives cannot be applied after all. Somepeople are of the opinion that Article 54 ofthe third directive should be interpretedstrictly and that the exemption only applieswhen there is a statutory social securitysystem in force alongside the private healthinsurance (the new standard insurance).Given that the new Dutch standard insur-ance is intended to replace the statutorysocial security system as a whole, anyappeal for an exemption on such groundswould have no chance of success. Othersmaintain that the exemption need not beinterpreted so strictly and that it can alsobe invoked in cases where the new private-law system is set to replace the social secu-rity system in the course of time. TheEuropean Court of Justice has yet to ruleon the exact scope of Article 54 of the third
non-life directive, so it remains unclearwhich interpretation is the correct one.
All things considered, there is at least a riskthat the non-life directives will apply andthat an appeal to the exemption clause willnot succeed. This brings with it the riskthat it will be impossible for the Dutchgovernment to impose the statutory restric-tions needed to safeguard the income andrisk solidarity of the new system.
Dealing with uncertaintyWith the aim of obtaining greater certaintyabout the feasibility of the government’splans, the Ministry of Health, Welfare andSport consulted European Commissionerfor the Internal Market Frits Bolkestein on1 October 2003. His answer came backwithin a matter of weeks.4
According to Mr Bolkestein, Article 54 ofthe third non-life directive does not have tobe interpreted strictly and can be invokedto ensure that private insurers are subject toobligations in the interest of the commongood, such as a duty to accept and a ban onpremium differentiation. However, insofaras these obligations restrict the free move-ment of services and freedom of establish-ment, they must be objectively necessaryand must not extend further than needed toaccomplish the goal for which they wereintended. While Mr Bolkestein does notexpect any problems in this regard, he doespoint out that, due to the lack of a detailedlegal text, it is not possible to say whetherthe intended Dutch system meets theserequirements.
The European Internal MarketCommissioner also expresses a number ofreservations. In his view, the setting up of arisk equalisation fund should be examinedwith reference to the European regulationson state support. He is also of the opinionthat, although there are no objections toincluding a choice between monetary andnon-monetary options from the perspectiveof EC legislation, the exclusive prescriptionof a non-monetary approach could wellmeet with objections. According to MrBolkestein, it cannot be ruled out thatlegally obliging insurers to offer services inkind (as opposed to restitution) contra-venes decrees regarding the free movementof services. Such an obligation could form amajor barrier to foreign insurers seeking tooffer their services in the Dutch market,since they would be obliged to engage incontracts with local healthcare providersfor this purpose and this would be muchmore difficult for them than for theirDutch counterparts. Mr Bolkestein there-
eurohealth Vol 10 No 228
health care reform
“The non-life
directives mean that a
national government
cannot impose
obligations on
private insurers.”

fore argues that such an obligation shouldbe seen as going against the principles ofproportionality and necessity.
Lastly, Mr Bolkestein makes another rele-vant comment on the option (apparentlysuggested by the health ministry) of keep-ing the new health insurance system entire-ly beyond the reach of the non-life direc-tives. The Commissioner feels that this isnot a realistic option. After all, according tothe Court of Justice, all insurance activitiesthat form part of a compulsory social secu-rity system are within the scope of the non-life directives if they are carried out byinsurance companies operating at their ownrisk and using insurance techniques basedon private-law contractual relations. If theNetherlands were to decide to set up a sys-tem outside of the scope of the non-lifedirectives, it would have to ensure that itsactivities could not be regarded as insur-ance activities. In this regard it wouldprobably not be enough to have theseactivities carried out by organisations witha legal form different to those explicitlymentioned in the non-life directives. Whatis more, a Member State is not allowed topermit an organisation with another legalform to carry out insurance activities.
Based on its consultation with theEuropean Internal Market Commissioner,the Dutch government concludes that theprivate insurance approach does not forman impediment to imposing a duty ofacceptance, an obligation to provide apackage compiled by the government or aban on premium differentiation. Whileacknowledging that the demands of neces-sity and proportionality must still be takeninto account, the government does notregard this as an insurmountable problem.Besides, it is not necessarily so that a pub-lic-law approach would exempt the insur-ance from the applicability of the non-lifedirectives.
The government therefore concludes thatboth approaches are within the realm ofpossibility and that they do not differ sig-nificantly in terms of both their substantivefunctioning and the extent to which theyserve the objectives of efficiency and quali-ty. However, the government has a clearpreference for a private-law design withstrong public safeguards. It believes thatthis approach best realises the desired clari-ty in terms of the division of responsibilitybetween government, citizens and insurers.In December 2003, the Minister of Health,Welfare and Sport informed parliament ofthe government’s decision to go ahead withits plans in their present form.
CommentaryFrom a European perspective, a number ofnoteworthy points emerge from the way inwhich the Dutch government has dealtwith the uncertainty surrounding the feasi-bility of its plans for reforming the systemof health insurance.
First of all, the decision to consult a mem-ber of the European Commission regardingquestions about the feasibility of the Dutchplans is an unusual one. After all, the onlyEU body in a position to examine nationalregulations with reference to the EC Treatyand secondary community law is theEuropean Court of Justice. An explanationsupplied by the European Commission or amember thereof can never be binding insuch a case, neither for the Member Statesnor for the Court. It is obvious that suchassurances do not provide the desired cer-tainty on this issue. Nor do they dispel thedanger that the approach selected may yetencounter problems in relation toEuropean legislation.
Another singular aspect of this process isthe government’s assertion that bothapproaches, the public-law approach andthe private-law approach, are more or lessequally matched in terms of their substan-tive functioning, while it neverthelessexpresses a clear preference for the latter,without offering further clarification.
Considering these two points, one is com-pelled to ask why the Dutch government isprepared to take a legislative risk withregard to the approach it has chosen whilean alternative exists, in their own words anequally good alternative, which does nothave this risk attached or at least to a farlesser extent. In our opinion this legislativediscussion masks the real issue at stake, thatis to say the issue of the added valueoffered by a private-law insuranceapproach as opposed to a public-lawapproach. What ‘profit’ is there to begained and by whom? This discussion isneglected when it should in fact take prece-dence over deliberations with regard topossible legal risks. After all, a legal risk isthere to be taken when it is evident that thematter at hand is worth or more thanworth the risk. In our view, this is sympto-matic of a fundamental turnaround inpolitical and social relations in theNetherlands: from a Christian and social-democratic inspired design of the welfarestate to a neo-liberal order with a strongemphasis on individual freedom andresponsibility, and considerable faith in theinfluence of the market. In such a climate,
eurohealth Vol 10 No 2 29
HEALTH CARE REFORM
“the decision to consult
a member of the
European Commission
is unusual”
eurohealth Vol 10 No 230
MUSCULOSKELETAL HEALTH
privatisation and commercialisation aretaken for granted, which means that theirapplication to healthcare (and other sectorswithin the welfare state) requires no justifi-cation in its own right. It is an ideologywhich steers decisions in a given directionand yet which is not really open to politicaldiscussion at present. In the current politi-
cal climate it is enough for the health min-ister to announce that the government isembarking on a particular course and willconsider the need to shift direction as andwhen the time comes.
Apart from all this, it is also worth remind-ing ourselves of the possibility that thesereforms may not end up being implement-ed in the form envisaged by the presentgovernment. Although the conditions forreform of the healthcare system appear tobe more favourable than ever before (thesense of urgency is great) previous attemptsat reforming the Dutch healthcare sectorhave demonstrated just how powerful aveto the stakeholders are able to mobilise atcrucial moments, to block developmentsthey regard as disagreeable. In other words,the ball is still very much in play…
REFERENCES
1. Dutch Minister of Health. Letter to Parliament. December 19, 2003.
2. Van der Grinten T E D, de Lint M. The impact of Europe on health care:the Dutch case. Eurohealth 2001;7(1):19-22.
3. Mossialos E. et al. The Influence of EU Law on the Social Character ofHealth Care Systems in the European Union. Brussels, s.n., 2001.
4. European Commissioner for the Internal Market, Mr. Frits Bolkenstein.Letter to the Dutch Minister of Health, 25 November 2003.
Musculoskeletal healthPreventing a dependent population
Anthony D Woolf,Kristina Åkesson,Juliet Compston,Karl-GöranThorngren, Piet van Riel andAlex Watt
Musculoskeletal conditions are commonand their impact is pervasive. They are themost common cause of severe long-termpain and physical disability across Europe.They are a major burden on health andsocial care. In Europe 20% to 30% ofadults are affected at any one time by mus-culoskeletal pain and the WHO GlobalBurden of Disease Project1 has identifiedosteoarthritis as one of the top ten causesof disability for countries within the EUand back pain is a major cause of workincapacity.
Two in five women over 50 years will sus-tain an osteoporotic fracture. Two in fivepeople with a musculoskeletal problem arelimited in their every day activities.Musculoskeletal conditions (excludingtrauma) account for almost 25% of thetotal cost of illness in European countries.2
They are the second most common reasonfor consulting a doctor and in most coun-tries constitute between 10% to 20% of theprimary care practice burden.3 One in fiveof all Europeans are under long term treat-ment for rheumatism and arthritis.4 Theyare the commonest cause of health prob-lems limiting work and up to 60% of peo-ple on early retirement or long-term sickleave claim musculoskeletal problems as theprimary reason.5
Throughout Europe, the burden on theindividual and society of musculoskeletalconditions will increase dramatically. Thepresence of many of these conditionsincreases markedly with age and many areaffected by lifestyle practice, such as obesi-ty, smoking and lack of physical activity.This potential dramatic increase in the bur-den of musculoskeletal conditions has beenrecognised by the UN and WHO with theendorsement of the Bone and Joint Decade,
Anthony D Woolf is Professor of Rheumatology, Peninsula Medical School,Truro, UK.
Kristina Åkesson is Associate Professor, Department of Orthopedics, MalmöUniversity Hospital, Sweden.
Piet van Riel is Professor and Head of Department of Rheumatology,Radboud University Nijmegen Medical Centre, The Netherlands.
Juliet Compston is Professor of Bone Medicine, University of CambridgeSchool of Clinical Medicine, UK.
Karl-Göran Thorngren is Professor, Department of Orthopedics, UniversityHospital, Lund, Sweden.
Alex Watt is Project Manager, Bone and Joint Health Strategies Office, RoyalCornwall Hospital, Truro, UK. E-mail:[email protected]
Further information: www.boneandjointdecade.org

an initiative that is globally supported byprofessional, scientific and patient organi-sations. Recognition of this problem hasalso lead to the European Union support-ing two major projects. The first to identifyindicators of musculoskeletal health thatshould be used across the community tomonitor the burden of disease6 and the sec-ond to develop a public health strategy toreduce the burden of musculoskeletal con-ditions across Europe – The EuropeanAction Towards Better MusculoskeletalHealth Report.7
Musculoskeletal conditions and theirimpactMusculoskeletal conditions are a diversegroup of complaints brought together bytheir association with pain and impairedphysical function. The most importantconditions in terms of frequency andimpact are osteoarthritis, rheumatoidarthritis, osteoporosis (including fragilityfractures) low back pain and musculoskele-tal injuries including sprains and strains.The Eurobarometer survey8 found thatnearly a quarter of all Europeans havelong-standing problems with their muscles,bones and joints of which back pain is themost common.
Musculoskeletal pain is often recurrent orpersistent and this in combination withlack of function of the musculoskeletal sys-tem results in disability. The prevalence ofmusculoskeletal conditions increases withage and although most common at olderages, there is a major impact on the work-ing population leading to work loss andearly retirement which has an associatedeconomic burden on society.Musculoskeletal conditions cause morefunctional limitations in the adult popula-tion in most welfare states than any othergroup of disorders. In the Ontario HealthSurvey9 musculoskeletal conditions caused40% of all chronic conditions, 54% of alllong-term disability, 24% of all restrictedactivity days and there are similar statisticsin Western Europe.
As a consequence musculoskeletal com-plaints are a major cause of sicknessabsence, and come second only to respira-tory disorders in short-term sicknessabsence and are the major cause of long-term absence. They are also the most com-mon reasons for disability pensions andback pain is the most common of the mus-culoskeletal conditions causing this. In theNetherlands musculoskeletal diseases havebeen found to be the most expensive dis-ease category regarding work absenteeism
and disablement.
Musculoskeletal conditions were alsofound to be the most expensive disease cat-egory in the Swedish Cost of Illness Studyrepresenting 22.6% of the total cost of allillness, 90% of these were indirect costs.2,10
47% were attributable to back pain, 14%to osteoarthritis and 5.5% to rheumatoidarthritis. In the Netherlands musculoskele-tal costs ranked fifth at age 15 to 44 years,second at age 45 to 64 years and third at age65 to 84 years after dementia and stroke.11
Disability generates a lot of hidden costsassociated with support by family and car-ers and lost opportunities such as a historyof back pain preventing somebody pursu-ing a physically active career. There is alsothe issue of stigma and social exclusionassociated with physical disability. Thereare therefore clearly strong arguments for implementing a public health policy to improve musculoskeletal health by pre-vention and control of musculoskeletalproblems.
Strategies for the prevention andcontrol of musculoskeletal conditionsCommon themes for the prevention andcontrol of musculoskeletal problems havebeen identified in the European Actiontowards Better Musculoskeletal HealthReport.7 There is a large body of evidenceabout specific interventions for the preven-tion and treatment of the different muscu-loskeletal conditions. The European Boneand Joint Health Strategies Project devel-oped these strategies by bringing togetherthis evidence with experts and relevanthealth professionals along with the experi-ence of those who have or are at risk ofmusculoskeletal problems. This collabora-tion provided a unique opportunity todevelop a methodology that would allowthe integration of the evidence for all thedifferent major musculoskeletal conditions.This has resulted in strong clear messages.
As musculoskeletal problems are so com-mon and pervasive, there is a strong argu-ment for a European health promotioncampaign aimed at their prevention andthus minimising their impact. There is evi-dence that musculoskeletal health can beimproved by a number of health promo-tion strategies. These include: physicalactivity to maintain physical fitness, main-taining an ideal body weight, having a bal-anced diet, avoiding smoking and the bal-anced use of alcohol, promoting accidentprevention programmes, programmes toavoid abnormal or overuse of the muscu-
eurohealth Vol 10 No 2 31
MUSCULOSKELETAL HEALTH
“Musculoskeletal
problems are the
ommonest cause of
health problems
limiting work”

eurohealth Vol 10 No 232
MUSCULOSKELETAL HEALTH
loskeletal system at the workplace and dur-ing leisure activities.
Overall it is important to raise the aware-ness of problems that relate to the muscu-loskeletal system to create a more positiveattitude to the importance of its preventionand the need for early effective manage-ment.
It is also clear that some groups of the pop-ulation are at greater risk than others and itis more cost effective to target these. Casefinding strategies have been developed forosteoarthritis, rheumatoid arthritis, backpain, osteoporosis and musculoskeletalinjuries that need to be disseminated,implemented and evaluated. Once those atgreatest risk are identified there are noweffective interventions for prevention. Forexample the progressive destructive courseof rheumatoid arthritis can be reduced andosteoporosis can be effectively preventedand treated to reduce the risk of fracture.
Musculoskeletal problems like many otherhealth conditions, do not often becomeapparent until their first manifestation andthe prevention of long-term disability
requires early case identification, assess-ment and appropriate care. There is strongevidence that this will not only reduce thesymptoms but also maintain function andreduce dependency and costs. This needs tobe achieved on a background of enablingthose with musculoskeletal conditions toknow what to do and to have the skills tomanage and take responsibility for theirown condition in the long-term.
Effective treatments have been recom-mended in the European Action towardsBetter Musculoskeletal Health Report forthe major musculoskeletal conditions butthe greatest barrier is ensuring access tothese. This not only requires the provisionof services but also awareness among thepublic, patients and health professionals ofwhat can and should be achieved. Many ofthe musculoskeletal problems are consid-ered to be an inevitable part of ageing andtheir impact at younger ages on quality oflife and the economic burden on the indi-vidual and society have not been fullyappreciated. Traditionally the education ofhealth care professionals has been inade-quate in this area. In parallel to the initia-tives to recommend public health policiesfor the prevention and control of muscu-loskeletal conditions, there have also beenrecommendations developed for educationof health care professionals by the Boneand Joint Decade Education Task Force.
What are the implications for different stake holders?The identification of the enormous burdenof musculoskeletal conditions and of strate-gies for their prevention requires Europeanand national policies that recognise theimportance of musculoskeletal health andencourage and facilitate implementation ofthe European Action towards BetterMusculoskeletal Health Report. The burdenalong with the evidence of what can beachieved to reduce it justifies muscu-loskeletal conditions standing alongsideother healthcare priorities across Europe.These preventative strategies will also havebenefits for other areas such as cardiovas-cular disease. There is a need for furtherresearch that will facilitate the implementa-tion of the strategies as well as the collec-tion of data, for example as part of healthinterview surveys, to monitor their effec-tiveness. The investment is not only neededin the provision of appropriate care but inraising awareness and knowledge amongstthe public, patients and healthcareproviders on how musculoskeletal healthcan be improved.
REFERENCES
1. Murray CJL, Lopez AD. The Global Burden of Disease: A ComprehensiveAssessment of Mortality and Disability from Diseases, Injuries and RiskFactors in 1990 and Projected to 2020. (Global Burden of Disease and InjurySeries, Vol 1). Cambridge: Harvard University Press, 1996.
2. Jacobson L, Lindgren B. Vad kostar sjukdomarna? (What are the costs ofillness?). Stockholm: Socialstyrelsen (National Board of Health and Welfare),1996.
3. Rasker JJ. Rheumatology in general practice. Br J Rheumatol1995;34(6):494–97.
4. Woolf AD, Zeidler H, Haglund U, Carr AJ, Chaussade S, Cucinotta D etal. Musculoskeletal pain in Europe: its impact and a comparison of populationand medical perceptions of treatment in eight European countries. AnnRheum Dis 2004;63(4):342–47.
5. National Board on Health and Welfare (Sweden). Yearbook of Health andMedical Care 2001. 2001.
6. Indicators for Monitoring Musculoskeletal Problems and Conditions.Musculoskeletal Problems and functional Limitation. Oslo: University ofOslo, 2003.
7. European Action Towards Better Musculoskeletal Health. Lund, Sweden:Bone and Joint Decade, 2004.
8. European Opinion Research Group EEIG. Health, Food and Alcohol andSafety. Special Eurobarometer 186. European Commission, 2003.
9. Badley EM, Ibanez D. Socioeconomic risk factors and musculoskeletal dis-ability. J Rheumatol 1994;21(3):515–22.
10. Jonsson D, Husberg M. Socioeconomic costs of rheumatic diseases.Implications for technology assessment. Int J Technol Assess Health Care2000;16(4):1193–200.
11. Meerding WJ, Bonneux L, Polder JJ, Koopmanschap MA, van der MaasPJ. Demographic and epidemiological determinants of healthcare costs inNetherlands: cost of illness study. BMJ 1998;317(7151):111–15.
eurohealth Vol 10 No 2 33
OLDER PEOPLE
Europe’s population is getting older. Thechallenges that this poses to EU memberstates are reflected in many Communitypolicies and programmes. The Lisbonagenda, the EU’s roadmap to a knowledge-based economy and to modernising theEuropean social model is one example, as isthe Community’s programme for researchand development. Funded though the FifthFramework Programme, the CARMEN(Care and Management of Services forOlder People in Europe Network) projectsought to improve the management of inte-grated care services for older people. Theproject explored a range of avenuestowards good quality, accessible and sus-tainable client-centred services. While facil-itating the exchange of expertise and goodpractice, the project also specificallyfocused on policy issues both at nationaland European levels.
Managed and coordinated by the EuropeanHealth Management Association (EHMA),40 European organisations from 11European countries participated in CAR-MEN between March 2001 and June 2004.The Network brought researchers togetherwith a broad range of stakeholders, includ-ing professionals, providers, purchasers,informal carers, and representatives ofolder people themselves. The dialoguebetween this diverse group of expertsformed the heart of the project. Thisenabled problems and good practices to beexplored from many different angles.Although finding common ground was notnecessarily the main objective, there wasstriking agreement over the key challengesas well as over the key components of solu-tions leading to better and more efficientintegration of services.1,2
Policy focusGrounded in practice as well as theory, theinsights acquired through the CARMENproject provided solid building blocks forpolicy. As pointed out earlier, strategicmanagement of services at policy level wasan explicit focus of the project. The resultsof these efforts with regard to national pol-icy are reflected in the CARMEN PolicyFramework,3 which offers a checklist forpolicy makers at national and regionallevel.
In addition to its policy recommendations,the CARMEN network has also publishedrecommendations for a European researchagenda4 with strong connections to the EUpolicy issues described in this article. Thereis a real need for the Commission to sup-port research on integrated care for olderpeople if its policy objectives are to be met.
When the CARMEN project was still onthe drawing board, it was anticipated thatany analysis of relevant implications forpolicy development and implementation atEU level would have to target various poli-cy processes that the Council, Parliamentand Commission are involved in. Underthe principle of subsidiarity, the organisa-tion and delivery of health and social careservices are the responsibility of MemberStates and the EU has no specific compe-tency in this field. Consequently, there isno such thing as an EU policy on healthcare, let alone a policy on long-term orintegrated care.
There are, however, a range of EU policyareas that do impact more or less indirectlyon the further advancement of integratedcare, such as internal market and social pol-icy (including employment, social exclu-sion, pensions and social protection). Overthe period of the CARMEN project, newdevelopments emerged from these frame-works that would have implications for thewhole system of services involved in inte-grated care, for carers, and for older peoplethemselves.
Advancing integrated care for olderpeople through EU Policy: CARMEN thematic network expertise informs theEuropean agenda
Nicoline Tamsma is Senior Adviser for International Health Policy, andHenk Nies is Director, Division on Care, Netherlands Institute for Care andWelfare, Utrecht. Philip Berman is Director, European Health ManagementAssociation, Dublin. E-mail: [email protected]. web: www.carmen-network.org
Nicoline Tamsma,Philip Berman andHenk Nies
“a range of EU policy
areas do have some
impact on the further
advancement of
integrated care’`

The European policy context
Health care and long-term care for olderpeople: tackling common challenges withinthe social protection agenda
The most immediate link to CARMEN’skey concerns emerged from the LisbonEuropean Council in 2000 and its follow-up with regard to the social policy agenda.In response to a Commission communica-tion,5 the Council stressed that social pro-tection systems needed to be reformed inorder to continue to provide quality healthservices in light of an ageing society.Subsequently, the Gothenburg Council(2001) asked for an orientation on the fieldof health care and care for older people,against the backdrop of the ‘open methodof coordination’. Building on the principleof subsidiarity, this method of workingallows Member States to tackle commonchallenges and problems, while at the sametime continuing to define their own nation-al strategy, and benefiting from experiencesand good practices of other Member States.
Since then, the issue of health care andlong-term care for older people has been atthe centre of a string of publications:
1. A report based on another CommissionCommunication6 (December 2001), sug-gesting EU member states should ensurethree broad objectives:
Access for all regardless of income orwealth.
A high level of quality of care.
Financial sustainability of care systems.
2. A joint report from the Commission andthe Council on supporting national strate-gies for the future of health care and carefor the elderly (March 2003), based oninformation provided by Member States onhow they deliver the objectives above .7
3. A European Parliament report confirm-ing the validity of the three key objectivesfor the modernisation of health care andlong-term care as well as the importance offurther structured cooperation betweenMember States.8
4. A Commission Communication defininga common framework to support MemberStates in the reform and development ofhealth care and long-term care using theopen method of coordination9 and propos-ing common objectives for health care pro-vision. The timeframe proposed for thisopen coordination process would see theCommission starting work on identifyingpossible indicators for joint objectivesbefore the end of 2004 and Member States
presenting medium-term policy objectivesby Spring 2005. This would then lead to aninitial series of development and reformstrategies in health care and long-term carefor the period 2006–2009.
Internal market policy and its consequencesfor services and patient mobility
Incorporating the freedom of individuals,goods, services, and capital, the EU internalmarket rules do impinge on health care andintegrated care provision as was clarified bynumerous rulings of the European Courtof Justice (ECJ).10 This led to the publica-tion of two different proposals from theCommission:
1. Parallel to the Communication on healthcare and long-term care, the Commissionpublished another Communication whichevolved out of the High Level Process ofReflection on Patient Mobility. It presentsa set of concrete proposals to addresspatient mobility as a consequence of theEU internal market.11 The twoCommunications complement each other.Together, they present an overall strategyfor developing a shared vision for Europeanhealth care and social protection systems.
2. A proposed Directive on services in theinternal market12 to provide a legal frame-work to eliminate obstacles to the freedomof establishment for service providers andthe free movement of services. Covering awide variety of services that theCommission considers as ‘economic serviceactivities’, it includes an article on theassumption of health care costs. The pro-posal would also reinforce the distinctionbetween hospital and non-hospital caremade by the ECJ* in recognising patients’rights to benefit from reimbursement in thecase of medical treatment dispensed inanother Member State, and would providea universal definition of hospital care acrossthe EU.
CARMEN’s recommendations for EUpolicy13
Overall comments
The Commission has initiated a processtowards the development of a shared visionfor European health care and social protec-tion service, which has great potential toenhance integrated care for older people.This potential should be maximised by abroad focus which includes perspectives onempowerment, prevention, social valuessuch as equity and solidarity, and the roleof informal carers. The shared visionshould appreciate the contribution of all
eurohealth Vol 10 No 234
OLDER PEOPLE
* See case law European Courtof Justice on the free move-ment of patients: Kohll (C-158/96), Decker (C-120/95), Smits andPeerbooms (C-157/99),Vanbraekel (C-368/98) andMüller-Fauré (C-385/99).
“the Lisbon European
Council stressed that
social protection
systems needed to be
reformed to continue
to provide quality
health services in an
ageing society”

elements of the health and social care sys-tem to improving services for older people,embracing whole systems service provision.A narrow focus on acute care only wouldbe a missed opportunity.
Given CARMEN’s commitment to putolder people in the centre of service devel-opment and delivery, its strong plea for thepromotion of older people’s positive con-tribution to society may come as no sur-prise. Older people should be seen as indi-viduals, not a uniform group; as assets tosociety, not a social burden. The Lisbonagenda is the EU’s most prominent stage totake on both economic and social chal-lenges. Recognising this, a good balancebetween economic and social objectives isessential in order to protect vulnerable citi-zens, support independence and achieve apositive outcome for older EU citizens inall Member States.
Tackling challenges with regard to healthcare and long term care
The suggested open method of coordina-tion is to support Member States’ nationalstrategies in tackling common challenges.Maybe one of the most prominent hurdlesto sustainable solutions for delivering carefor older people is the administrative,financial and organisational compartmen-talisation of health and social care systems.Country-specific problems tend to followthe dividing lines of these system compart-ments, with the division between social andhealth care being particularly prominentand the problems in the acute health caresector often taking centre-stage. MemberStates should be encouraged to establishmechanisms and incentives to work acrossthese two main pillars and their sub-sec-tions, and to stimulate policy developmentsthat encourage joint working and innova-tion at sector interfaces. Similarly, MemberStates should stimulate clear and coordinat-ed policy responsibilities across local,regional and national level.
National Action Plans (NAPs) set up byMember States to deliver common socialpolicy objectives should allow for theimplementation of activities that enable thepositive contribution of health and long-term care to other social policy areas, andvice versa. EU economic and social policyinstruments, such as the Structural Funds,should support further development of thewhole system of integrated care provision,including the development of services out-side hospital and residential settings.
Nationally, solutions should focus onestablishing a coherent system of services
with a range of attractive and suitableoptions for all older people, including vul-nerable people with multiple needs, regard-less of socioeconomic status, ethnicity, gen-der or lifestyle. Accessible, good qualitydomestic services and other forms of careprovided in the home setting should beavailable to ensure older people can contin-ue to live independently. Structural supportfor informal carers is an essential element inachieving overall objectives with regard toaccessible, good quality and financial sus-tainable long-term care. ‘It should includepractical, emotional and financial measures.
Other social policy themes
Next to the proposals on health care andlong-tem care, the broader European socialpolicy agenda includes issues such asemployment, pensions and social inclusion.All three of these are already subject to theopen method of coordination. The fourprocesses could well be streamlinedthrough delivery of the Lisbon agenda.This offers many opportunities for mutual-ly reinforcing policy measures to advancehealth care and care for older people.
With regard to employment, active mea-sures need to be taken to improve theimage, status, remuneration and work pres-sures in the care sector, to stimulateemployment and career opportunities inthese sectors and to encourage a sustainableworkforce. Measures designed to supportlonger working lives should take the posi-tion of older family carers into account.Their socioeconomic position should beprotected against repercussions in terms ofpension rights, income and/or social isola-tion.
In terms of social protection and inclusion,measures should be taken to prevent poor-er health among older people leading toimpoverishment and low income, which inturn may restrict access to care. If MemberStates introduce or increase co-paymentsand/or means testing as a cost-containmentmeasure in health system reform, thisshould not lead to poverty, social exclu-sion, unequal access, or increase of healthinequalities.
Pensions are a very important financialresource for older people. If older peopleare to pay more towards the costs of theircare, Member States should be encouragedto cordinate pensions and other forms offinancial social security on the one hand,and co-payment arrangements on theother. EU programmes aimed at tacklingsocial exclusion should facilitate projectsthat encourage social participation and
eurohealth Vol 10 No 2 35
OLDER PEOPLE
“active measures need
to be taken to
encourage a
sustainable workforce
in the care sector”

independence of older people and theirinformal carers.
Gender equality being a fifth key socialpolicy objective, older women’s health,financial and social resources may need spe-cific consideration. Compared to men, life-expectancy of women is higher and theycan expect to live more years in ill-health.Consequently, their need for health careand long-term care services will be higher.As women’s pensions and other financialresources are often less than those of men,women may be particularly vulnerable toadverse effects of cost-shifting from publicto individual budgets and the reduction ofpublicly funded standard care packages.
Internal Market
In following up the recommendationsemerging from the High Level Process of
Reflection on patient mobility and health-care, the focus should be on the whole sys-tem of health and social care, not on acuteand hospital care only. A limited focus willlose sight of many challenges posed byinternal market opportunities, includingthe increasing flow of older people seekingsemi-residential services abroad, and theincreasingly diverse group of people mov-ing across borders to offer their services inprivately purchased home care arrange-ments. The suggested High Level Groupon Health Services and Medical Careshould include experts and stakeholdersfrom the social care sector as well as thehealth care sector in order to oversee thewhole range of services that citizens cannow access abroad as a consequence ofEuropean Court of Justice rulings. It mightalso include representatives of older people,patients and carers.
For patients who have received part of theirtreatment abroad, measures have to betaken to ensure sufficient quality, access,and continuity of care. Case-managementand communication issues deserve particu-lar attention. Patients should not be deniedaccess to post-hospital care in their homecountry as a result of having received treat-ment in another country. TheCommission’s proposal for a directive onservices in the internal market would rein-force the distinction between hospital andnon-hospital care. Measures should betaken to guard against negative effects ofCommunity legislation on health systemcompartmentalisation, and on opportuni-ties for integration and innovation acrosssectors.
Future involvement from the CARMENnetwork and EHMACARMEN has been pro-active in linkingwith the Commission ever since the publi-cation of the Commission’s December 2001Communication6 and continued that dia-logue as the project progressed. While theCARMEN project as such is finished,through EHMA the thematic networkaspires to function as an instrument for theinvolvement of key stakeholders in furtherprogress made within the EU social protec-tion agenda both at national and EU level,and as a testing ground for common objec-tives and indicators should these be devel-oped through future collaboration process-es between Member States. The formula ofa thematic network has also proven to be aproductive tool for the exchange of goodpractices, which could again contribute tothe open method of coordination.
eurohealth Vol 10 No 236
OLDER PEOPLE
REFERENCES
1. Nies H, Berman PC (eds). Integrating Services for Older People: AResource Book for Managers. Dublin: EHMA, 2004.
2. Vaarama M, Pieper R (eds). Managing Integrated Care for Older People –European Perspectives and Good Practices. Helsinki: STAKES, forthcoming.
3. Banks P. Policy Framework for Integrated Care for Older People. London:Kings Fund, 2004.
4. Nies H. A European Research Agenda on Integrated Care for OlderPeople. Dublin: EHMA, 2004.
5. COM (1999) 347 final: A Concerted Strategy for Modernising SocialProtection.
6. COM (2001) 723 final: The Future of Health Care and Care for theElderly: Guaranteeing Accessibility, Quality and Financial Viability.
7. Council of the European Union. Joint Report by the Commission and theCouncil on Supporting National Strategies for the Future of Health Care andCare for the Elderly. Brussels: no. 7166/03, March 2003. Available athttp://europa.eu.int/comm/employment_social/soc-prot/healthcare/ elderly_en.pdf
8. European Parliament Committee on Employment and Social Affairs,Report A5-0098/2004 final, rapporteur Karin Jöns.
9. COM (2004) 304 final: Modernising Social Protection for the Developmentof High-quality, Accessible and Sustainable Health Care and Long-termCare: Support for the National Strategies Using the ‘Open Method ofCoordination’.
10. SEC (2003) 900: Commission Staff Working Paper. Report on theApplication of Internal Market Rules to Health Services: Implementation bythe Member States of the Court’s Jurisprudence.
11. COM (2004) 301 final: Communication from the Commission ‘Follow-upto the High Level Reflection Process on Patient Mobility and HealthcareDevelopments in the European Union’.
12. COM (2004) 2 final/3: Proposal for a Directive of the EuropeanParliament and the Council on Services in the Internal Market (presented bythe Commission).
13. Tamsma N. Advancing Integrated Care for Older People Through EUPolicy. Dublin: EHMA, 2004.
CARMEN has been supportedby the EuropeanCommission’s ‘Quality of Lifeand Management of HumanResources’ Programme, whichis part of DG Research’s 5thFramework Programme. Theauthors are solely responsiblefor the views expressed in thisarticle, which does not repre-sent the opinion of theCommunity.

eurohealth Vol 10 No 2 37
QUALITY
IntroductionThe ‘evidence based medicine’ movementhas changed attitudes, if not always thepractice, of clinicians. Many agree that theirpractice should be informed by researchabout treatment effectiveness, but mostalso recognise that they will need to com-pare the research conditions with those oftheir own setting to assess whether theycould expect similar results with theirpatients. Can they carry out the treatmentreported in the research in the same wayand are their patients sufficiently similar tothose selected for the research? Researchdoes not always transfer to all settings, butneeds to be translated.
The same judgements need to be made bypolicy-makers and managers when seekingto use research to inform their decisionsabout whether to introduce a policy ororganisational change. They need to assesswhether a change reported in the researchcan be applied in the same way in theirlocal situation, and if it were, would theresults be the same?
However, the little evaluation research intoorganisational and health systems changesoften fails to describe either the changemade or the local situational factors whichhelped or hindered implementation. Oftenvery few outcomes are reported, yet deci-sion-makers are interested in a number ofthe consequences of such changes.
Although policy-makers and managers’decisions will never be made only on the basis of research evidence, researchcould improve their decision-making.Organisational changes and reforms arebeing carried out in healthcare with verylittle reliable understanding of theirprogress and consequences. It is possiblethat large amounts of time and money arebeing wasted, and that these changes couldbe better informed by research. Evaluationcan strengthen democracy by holdingpoliticians and managers to account fordecisions and by enabling implementationof decisions.
There are challenges in evaluating complexchanges in healthcare and this in partaccounts for the lack of research in thisarea. This paper considers methods for car-rying out such research that could providesituationally-rich information allowing bet-ter informed decisions to be made. Itdescribes how medical research designshave been adapted, but also looks atresearch methods new to health care whichaim to understand how the context of thechange influences the change, rather than‘controlling-out’ the context. These designshelp policy-makers to translate changesmore effectively to their local setting andspeed the spread of changes likely to beeffective.
The need to evaluate complex socialinterventions‘Complex social interventions’ (CSIs)include hospital mergers or quality pro-grammes, external inspection processes, orintroducing diagnostic related group(DRG) funding for hospitals. These andothers are costly changes, but are increas-ingly used, often with little evidence ofeffectiveness. Evaluations of CSIs couldhelp policy makers to decide if such achange would improve healthcare and howbest to implement the change in their localsetting.1
Sophisticated evaluation designs have beendeveloped to evaluate treatments. Researchusing these designs is increasingly used byclinicians in their practice to decide the besttreatment for patients. These designs havealso been used to evaluate simple interven-tions to health care organisations, such as atraining programme.2 However, it is diffi-cult to apply these designs to evaluate com-plex social interventions: what are the chal-lenges, and are there methods which cangive the evidence which policy-makersneed?
The randomised controlled trialdesignHow do we know that lower costs perpatient, or improved quality are in fact pro-duced by a change carried out to get theseresults and not caused by something else,such as a new manager? Why not use meth-ods for treatment evaluations that controlfor these other factors?
Evaluating complex social interventions
John Øvretveit is Director of Research, The Karolinska Institute MedicalManagement Centre, Stockholm, and Professor of Health Policy andManagement, The Nordic School of Public Health, Gothenburg, and BergenUniversity Faculty of Medicine, Norway. E-mail: [email protected]
John Øvretveit
“Organisational
changes and reforms
are being carried out
with very little reliable
understanding of their
progress and
consequence”

When applied to treatments, the ran-domised controlled trial (RCT) designexcludes influences other than the treat-ment-intervention. This increases certaintythat any change to patients is due to theintervention rather that to something else,such as some patients taking other treat-ments at the same time. A RCT gives mea-sures of patient status before and after theexperimental intervention as well as mea-sures of another group of patients’ statusbefore and after they received the compari-son intervention. It is the researcher’s taskto prove that the difference is due to theintervention and not to something else,such as different types of patients in thetwo groups, or changes in the way theinterventions were applied. Randomisation,control and prospective design rule outother things which could explain any mea-sured before-after differences between theexperimental and control groups: thismakes it possible to control for factorsother than the treatment-intervention.
This design has been used successfully notonly to evaluate treatments to patients andservices, but also to evaluate some interven-tions to services. An example of an inter-vention to a service is a training pro-gramme, where service personnel ratherthan patients are the ‘target’. A RCT can beused to compare this training interventionto an alternative, such as no training. Wecan randomise service personnel to theexperimental intervention (training) and tothe control intervention (no training). Wecan select valid measures of the results oftraining so as to get data sensitive to thetraining and which does not register otherfactors. We can choose services that aresimilar so as to rule out differences in databetween the two groups that could becaused by other factors such as resources ortypes of service.
RCT for evaluating complex socialinterventionsRCTs can control for most other influencesor explanations with a careful study designand the cooperation of participating ser-vices. However it is not easy to use ran-domisation or control for many of themore complex social interventions for ser-vices which we need to evaluate.
DRG payment systems for hospitals, a hos-pital merger, or a hospital quality pro-gramme are complex because they are mul-tiple interventions: there is training butthere is also an intervention to inform orconsult personnel, an intervention tochange the work which people do, inter-
ventions to procedures and systems andmore. They are also social interventions intwo senses:
– They are interventions that change toadjust to changing conditions, they‘evolve’ rather than being ‘implemented’in a linear fashion.
– The organisations they are aimed at aresocial entities, constantly changing andinvolving sub-groups who interpret andrespond to changes in different ways.
In the language of sociology and politicalscience complex social interventions arecarried out by individuals and social groupswho interpret and adapt to their situation,they are not standardisable treatments.These ‘interventions’ also act on organisa-tions which do not respond like humanphysiology but which involve multiplegroups who interpret and respond to thechange differently. In addition the organi-sation is part of the surrounding social,economic, political and cultural environ-ment. The organisation’s interaction withthis environment affects the results of theintervention in a way which is different tothe way a patient’s environment affectstheir response to a drug or surgery.
These complex changes are interventions toservices that are widely used. Current man-agement wisdom is that the effects of theseinterventions are worth the costs of theintervention: but is this like thinking thatpatients with epilepsy are cured by blood-letting? Current medical wisdom is thatonly an RCT can discover if these interven-tions are effective, but it is not practical toallocate these interventions randomly to anexperimental group of hospitals and to acomparison group. The intervention itselfchanges over time and is not a standarddose, and the hospitals also change as aresult of other factors. Even if it is possibleto trial the intervention in some hospitalsand not in other similar hospitals, there aremany things we cannot control for, andwhich could explain any before-after dif-ferences between the two groups.
Control, or understand?Do these challenges mean that researchcannot assess whether social interventionslike DRG payment, mergers or hospitalquality programmes are effective? Thereare two schools of thought. First the‘quasi-experimentalists’, who take the RCTas the ideal. Randomisation might not bepossible, but we can try to get comparablegroups of personnel or organisations, those‘exposed’ to an intervention like a merger,
eurohealth Vol 10 No 238
QUALITY
“It is not easy to use
randomisation or
control for many of the
more complex social
interventions”

and those not exposed. We can try to stan-dardise the intervention by choosing orplanning mergers which are similar andcompare these with comparable pairednon-merger hospitals. We might also beable to design and carry out the studyprospectively rather than retrospectively.The second school of thought, the ‘socialevaluators’, argue that an RCT is not onlyimpractical, but undesirable. The followinggives an example of a social evaluation andthen explains the arguments against usingRCT design.
An example of a social evaluation
In 1994 six Norwegian hospitals intro-duced quality programmes as an experi-ment sponsored by the Norwegian MedicalAssociation to find out if ‘total qualitymanagement’ (TQM) was effective. I wasasked to evaluate this experiment. The hos-pitals ranged from a small 55 bed to a large800 bed teaching hospital. We could notrandomly allocate TQM to different hospi-tals, so I selected another six comparablehospitals and set about collecting data tofind out if the quality programmes pro-duced outcomes which were different inthe two sets of hospitals.
I soon abandoned this approach because itbecame clear that each of the six TQM hos-pitals was carrying out very different activ-ities in the name of TQM. Each had inter-preted this concept of TQM differently,and each were changing their programmesregularly, so that what was carried out wasnothing like what was planned.3
The approach I took was, first of all, todescribe the actual activities each carriedout which they called ‘TQM’, using theo-ries about how to implement TQM andtheir plans to guide data gathering for thedescription. With this description it wasthen possible to see more clearly what out-comes might be expected and to gather dataabout the changes which did happen. Overa four year period I gathered the views of across-section of personnel about what out-comes they expected and what had hap-pened, and also their views about whatcaused these outcomes, and compared thisacross the six hospitals. I also gathered dataabout hospital costs and patient outcomesand found differences, but could not besure these were due to the TQM pro-grammes and not to something else.
This study could not show conclusivelythat TQM was effective. What it did givewas the first description of how hospitalsinterpreted and carried through a qualityprogramme and the assessments of person-
nel about the results. It discovered impor-tant differences between the programmes.The comparisons found that personnelassessed as more successful those pro-grammes that had taken steps to involvemiddle managers and doctors. It found inall of the hospitals that better results wereachieved in those departments where mea-surement and project teams were used in aparticular way.
The limitations of RCTs for CSIsEven if a controlled trial design would havebeen possible, why would it have been lessdesirable than the ‘social evaluation’design? There are a number of argumentsof the ‘social evaluation’ school.4 RCTsonly measure a few limited outcomeswhich are suited to statistical calculationsfor assessing the probability of before andafter outcome differences being greaterthan chance. In evaluating social interven-tions we need to assess a broader range ofoutcomes, not just patient outcomes butthose for many different stakeholdergroups.
RCTs only assess outcomes. They do nothelp us understand the mechanisms orprocesses which produce the outcomes.When assessing social interventions we areinterested in which aspect of the interven-tion was the most ‘potent’, and in how andwhy it had any effect we may detect. Wecan make use of informed people who areinvolved in the change to theorise abouthow the intervention produces effects, orfails to do so. Because the intervention is asocial one, to a social organisation, and ifmany people hold the same views, thentheir views have an impact regardless ofwhether their views are ‘true’ or not.
RCTs standardise the intervention, eachpatient is exposed to the same interventionso that before and after differences couldnot later be attributed to individual treat-ments that were slightly different.However, it is not practical to standardisemost social interventions such as a merger,but, more importantly, not desirable to doso. Research suggests that some socialinterventions such as a merger or qualityprogramme are most effective when theconcept is adapted to the local situation,which includes adjusting the interventionas it progresses. Drug doses are adjusted topatients, but the adjustments of socialinterventions as they are applied to socialorganisations are of a different order. Withsocial interventions the planned ‘merger’ isnot the same as what actually happens. Thepoint is not to standardise the intervention,
eurohealth Vol 10 No 2 39
QUALITY
“some social
interventions such as a
merger or quality
programme are most
effective when adapted
to the local situation,
and adjusted as they
progress”

but to describe it as it unfolds and evolves.Standardising it makes it likely to fail.
RCTs try to control-out situational factors.The more that they do, then the more thefindings are thought to be generalisable toother settings. But with complex socialinterventions, the situational factors cannotbe separated and in one sense are an impor-tant part of the intervention. But this doesnot mean that the findings cannot be gener-alised to other settings because they are sosituationally-dependent? The point is notto control-out situational factors but tounderstand them. Social interventions likemergers are changed as they are carried out,not only to adjust to the ‘internal’ reactionsof personnel, but also to external changeslike changes in government or funding ornew laws. We can control-out these factorsby comparing similar organisationsexposed to the same changes in context, butwe are then less able to understand howand why those carrying out the interven-tion adapted it to the change in context.
The attribution problem for socialevaluators‘Social evaluators’ concentrate on describ-ing the complex intervention as it ‘unfolds’over time, rather than controlling the inter-vention by standardising it. They aim tounderstand which factors of the ‘situation’are important for the effectiveness of theintervention. Rather than controlling-outthese factors, they use informed partici-pants’ ideas about what these factors are, aswell as other more objective data to assessthe possible influence of these factors. Thiscan help others to decide if the interventionwould be effective in their local situationand which factors to pay attention to forcarrying-out the intervention successfully.
However, if ‘social evaluators’ do not usecontrol or randomisation, how can theyestablish if any of the apparent outcomes ofan intervention like a merger are, in fact,produced by the merger and not by some-thing else? These are some of the tech-niques used:
– A comparison group can be used to helprule-out context factors, like a change infunding explaining any discovered out-comes.
– A cross-section of informants can beused to collect data about what theythink are outcomes, and to collect theirideas about how to assess whether theseare the outcomes of the intervention andnot something else.
– Data can be collected on intermediate orshort-term outcomes, such as personnelreactions, which can more easily belinked to the intervention than patientor cost outcomes often distant from theintervention.
ConclusionsExpensive changes and interventions arebeing made to health care systems but withlittle knowledge about whether they areeffective. Policy makers need to know ifthese changes are effective elsewhere, andhow to carry through these changes if theydecide to do so. RCTs can be used to eval-uate some interventions, but many complexsocial interventions like mergers or struc-tural reforms cannot be evaluated using thisresearch design.
This does not mean that these changes can-not be evaluated at all. There are evaluationmethods which can provide decision-mak-ers with knowledge about how a complexchange was carried out and the results.‘Quasi experimental’ designs can tell usabout the effectiveness of some social inter-ventions. There are also ‘social evaluations’which give less certain findings about effec-tiveness, but a greater understanding abouta range of effects and about how theseeffects came about. They also give adescription of what is actually done tocarry out the intervention so that decision-makers do not confuse the concept or planwith what actually happened in a real situa-tion. Such studies also examine which situ-ational factors helped or hindered thechange and how the change was adjusted tothese factors as it was carried through overtime. This type of ‘real time’ action evalua-tion research can help make betterinformed policy and management decisionsabout whether and how to carry out achange.
eurohealth Vol 10 No 240
QUALITY
REFERENCES
1. Mattison, N. Putting policies in context –achieving and sustaining better health carequality. Eurohealth 2003;9(3):7–12.
2. Eccles M, Grimshaw J, Campbell M,Ramsay C. Research designs for studiesevaluating the effectiveness of change andimprovement strategies. Quality and Safetyin Health Care 2003;12:47–52.
3. Øvretveit J. Integrated QualityDevelopment for Public Healthcare. Oslo:Norwegian Medical Association, 1999.
4. Øvretveit J. Action Evaluation of HealthProgrammes and Change. A Handbook fora User Focused Approach. Oxford: RadcliffeMedical Press, 2002.
“‘real time’ action
evaluation research can
help make better
informed policy and
management decisions
about whether and
how to carry out a
change”

eurohealth Vol 10 No 2 41
INFORMED PATIENT
Development of the internet and its appli-cation to health care has opened up newpossibilities for patients to becomeinformed about their health and well being.Developments in digital and informationtechnologies in health care have alsoallowed doctors and researchers to generatemore information than ever before. Theimportance of e-health for the informedpatient is enormous and important fromseveral different perspectives because:
– Patients throughout Europe meet newchallenges in new therapies as well asnew knowledge regarding their diagno-sis.
– New knowledge is not always easy tounderstand or to apply.
– The existing health care system is notdesigned to meet this new situation.
The imperative to provide information forthe patient and what it means in practice isespecially acute in an organisation such asAgrenska that focuses on the needs of chil-dren and their families faced with rare dis-orders.
Each one of us has been, or is going to be, apatient at some point either because onewill have to look for help from a healthcare professional or a hospital due to illnessor because of a wish to improve health insearch of a better quality of life. All of ushave an interest in our own health, and weare always passively or actively looking forsomething that could improve it.
During the last decades, scientific opportu-nities and medical breakthroughs have hadan enormous impact on the quality andlength of life. More is to come and evenfaster than before. With the incredible bio-medical developments today, it is possibleto get a cure or a treatment somewhere onthis Earth for nearly any health condition.This does not mean that we can cure everyillness and restore health, but it means thatwe can improve health conditions to amuch greater extent than before.
Obstacles to overcomeThere are of course many obstacles thathave to be overcome and there is a lot of
new knowledge to be developed in order toreally cure illnesses. Among some of themost pressing is the need to:
– Get drugs faster to the patient.
– Provide safer and more targeted prod-ucts.
– Develop new ways of cooperationbetween the patient and many differentpartners, such as pharmaceutical compa-nies, government, academic, scientific orhealth professional organisations.
The possibilities are great but truly impos-sible to achieve without providing greaterinformation for patients in future. This isnot limited to greater individual responsi-bility and compliance alone. Futurepatients have to be much more closelyinvolved in stimulating research and facili-tating clinical trials through better andsmarter information technology directed topredicting risks and benefits. Finally, thereis a need to exchange information forpatients around the world in a trustworthyand secure way.
Although good in principle, we are still notin general in this situation today. Our taskis to develop many more situations andplaces where this interaction between thepatient and different partners can effective-ly take place. The interaction will not occurif we simply create a meeting or, send out asurvey, or talk with professionals.Information for the patient requires coop-eration in situations meeting certain stan-dards.
The Agrenska FoundationOne example of such a meeting place is theAgrenska Foundation in Sweden. Agrenskais dedicated to the provision of informationnot only for patients but also for theirentire families, and serves as an informationexchange for patients with specific diag-noses. Agrenska is focusing in particular onrare diseases in children and their families.Since the beginning of 1989 more than 3000families have participated in different diag-nosis-related family programmes. As thesediseases are rare, the need for informationis particularly intense. Moreover as theseconditions affect children, their impact onfamilies and society is that much more pro-found.
E-Health and the informed patient
Anders Olauson is President and Chief Executive Officer of the AgrenskaFoundation, Hovås, Sweden. E-mail: [email protected]
Anders Olauson
“there is a need to
exchange information
for patients around the
world”

It is within the Family programme atAgrenska that these interactions take place.Children already identified by the medicalsystem come to Agrenska with their par-ents and siblings because they all needinformation. Here meetings take placebetween many different partners, such asresearchers from pharmaceutical compa-nies, government representatives, academic,scientific or health professionals, and thepatients.
Together with Microsoft, Agrenska hasdeveloped a virtual platform on theInternet (www.agrenska.se/familyprogram)for use by the children and their families.They can use this either to exchange experi-ences and thoughts after their visit in a chatforum where they also can exchange infor-mation with the experts that they met dur-ing the visit. Children can also use a ‘pic-ture diary’ to exchange information withfriends and/or professionals.
This two-way interaction is very importantbecause information with respect to theconditions seen at Agrenska has to comedirectly from different actors. It is equallyvaluable that this information then goesback from the patient to the researchers, orto health care system professionals. Thebenefits of this programme are undoubted-ly recognised not only in Sweden but alsointernationally. This can be seen by theinterest from different institutions andcompanies worldwide. Among those whohave publicly acknowledged Agrenska’sapproach and confirmed the importance ofthe programme are the US NationalInstitutes of Health, The EuropeanOrganisation for Rare Diseases (Eurordis),a range of universities and hospitals inEurope, and patient organisations in Japan,the Middle East, and South Africa.
The lesson from these visits is two-fold:firstly the need is the same regardless ofwhere people live, and secondly this typeof a meeting place can be used in a varietyof different cultural and governmentalenvironments. Of course, without theinvolvement of Microsoft as an informationtechnology provider major obstacles wouldhave remained.
Lower costsA report prepared in 1997 by the School ofEconomics and Commercial Law inGöteborg has shown that the health carecosts with respect of children who had notgone through a tailored information familyprogramme were notably higher than thoseof treated children, SEK 35,200 per annumin comparison with SEK 13,300 per annum
respectively. This difference could beattributed to the fact that when comparedto the other families, informed families cru-cially knew several important facts:
– When they should seek medical care fortheir child.
– Where to go, and whom to ask for care.
– How they should proceed.
– When they did not have to go to thehospital because they could manage bythemselves.
This is the way an informed patient/personacts and behaves, and that is why costs tosociety are less than for uninformedpatients.
Fundamental questionsIn the final analysis, there are still manyfundamental questions to be asked beforedeclaring a universal preference forinformed patients. Who wants an informedpatient? Today we live in an individualisticsociety and there is a tendency for each oneof us to have to make decisions abouteverything from pensions to what we wantfrom our schools. So the answer may bethat we have already left an ‘uninformed’place for one where you have to beinformed in order to cope. However, thereare still some senior doctors in Europe whothink that it is totally wrong that the phar-maceutical industry has their own directcontacts with patient organisations.
How can a patient be informed? Thepatient can receive information from thestate, from patients’ organisations, fromdifferent companies who deliver services,and from other bodies based on science andgood standards. Must every patient be awell-informed patient? In my view, theanswer is no, and this is important from ademocratic point of view. Knowledgeshould never be that type of importantpower. What differentiates an informedpatient from an uninformed patient? Aninformed patient has a feeling of empower-ment as he or she is receiving more appro-priate treatment, has a better sense of well-being and ultimately a better quality of life.
Who will take the responsibility to changethe way healthcare services are organisedtoday, in order to meet the needs ofinformed patients? The only individualswith this kind of authority are politicians.If they do not take up the challenge, theirvoters will force them to, either directlythrough elections, or by the growing use ofservices run by private individuals or inde-pendent companies.
eurohealth Vol 10 No 242
INFORMED PATIENT
“costs to society are less
than for uninformed
patient”

News and information on the Dutch Presidency of the European Union.
eurohealth Vol 10 No 2 43
E-mail [email protected] to suggest websitesfor inclusion in future issues.
Dutch Presidency
www.eu2004.nl
Centre de Recerca enEconomia i Salut(CRES), Pompeu FabraUniversity, Barcelona
www.upf.es/cres
The Maltese Ministryof Health, The Elderlyand Community Care
www.health.gov.mt
The HealthcareCommission
www.healthcarecommis-sion.org.uk
The website provides a wide range of information on public health and health care services inMalta. Links are provided to other health related bodies on the island. Press releases, reports andinformation on healthy living are also provided. Most information is available in English althoughsome reports are only available in Maltese.
The Nuffield Institutefor Health, Universityof Leeds
www.nuffield.leeds.ac.uk
The Nuffield Institute for Health, conducts research in the areas of management, medicine, healthand social sciences, and also has a strong focus on linking evidence, policy and practice. As well asproviding information on research activities, and teaching programmes, a wide range of workingpapers, reports and other publications can be downloaded.
The Healthcare Commission is a new organisation that was launched on the 1st April 2004. Itexists to promote improvement in the quality of healthcare in England and Wales. In Englandonly this also includes regulation of the independent healthcare sector; separate bodies are respon-sible for these functions in Wales. Every NHS organisation in England is given a star rating fromzero to three, showing how it has performed against a range of indicators and targets. In additionto publishing clinical governance reviews (routine inspections of NHS organisations), and con-ducting investigations when serious problems arise within the NHS, independent reviews of pri-vate sector services are also produced, together with national NHS staff and patient surveys. TheCommission also produces an annual report for the UK Parliament on the state of healthcare inEngland and Wales. Themed reports including a recent review of national cancer care services isnow available online.
The Economics and Health Research Centre (CRES) is a special research centre of UniversitatPompeu Fabra founded in 1996. It undertakes a range of health policy, management and econom-ics research, with a strong multi disciplinary focus. The website provides access to working papersand other publications, in addition to providing information on events, activities and detailedstaff profiles. The website is available in Catalan, Spanish, and English.
The Association ofPublic HealthObservatories
www.apho.org.uk/apho
The Association of Public Health Observatories (APHO) has been established since June 2000. Itwas set up with the multiple aims of being a learning network for the 10 public health observato-ries in England and Wales and other users; to be a single point of contact for external partners; tobe an advocate for users of public health information; and to coordinate work across the publichealth observatories. Publications available on the website include reports on regional health indi-cators in the English regions. Information on contacts and expertise, work in progress and forth-coming events are also available.
The European Year ofEducation ThroughSport
www.eyes-2004.info
The Council of the European Union and the European Parliament made 2004 the European Yearof Education through Sport 2004 (EYES 2004). The main objective of the campaign has been tosensitise the European public to the importance of sport in an educational context as well as toincrease the significance of physical activities in school curricula. A wide range of information isprovided on activities and events in all official Community languages.
WEBwatch

eurohealth Vol 10 No 244
NEW PUBLICATIONSEurohealth aims to provide information on new publications that may be ofinterest to readers. Contact David McDaid [email protected] if you wish tosubmit a publication for potential inclusion in a future issue.
Towards the GlobalElimination of BrainDamage due toIodine Deficiency
Edited by B Hetzel, F Delange, J Dunn, J Ling, V Mannar, C Pandav
New Delhi, Oxford:Oxford UniversityPress, 2004
ISBN 0-195-67095-7
578 pages. Paperback
Review by Walter Holland.Emeritus Professor ofPublic Health, LSEHealth and Social Care,London School ofEconomics and PoliticalScience.
Iodine deficiency is the most common preventable cause of brain damage in the world today, withat least 2 billion at risk in 130 countries. This book chronicles the work of a dedicated group ofscientists who have been involved in research on this and also the essential dissemination, persua-sion and evaluation of appropriate policies for eliminating this scourge.
Iodine deficiency has been considered as a scourge of mankind since ancient times causing bothgoitre and brain damage at all ages, including for the foetus during pregnancy. People live in anenvironment where the soil has been leached of iodine due to flooding of river valleys or in hillyand mountainous areas by high rainfall and glaciation. This leads to iodine deficiency in all formsof plant life. Thus large numbers of people, particularly in Asia, live in areas where their diet isdeficient in a vital element required for the development of the thyroid hormones. In iodine defi-ciency the thyroid gland enlarges to form goitre, something recorded since 3,000BC. The recogni-tion of the relationship with brain damage is of more recent origin, and the introductory chapterchronicles the clinical, animal and biochemical and epidemiological studies that have been done todemonstrate this and other forms of iodine deficiency disorder (IDD). Various estimates are givenabout the magnitude of the problem, ranging from 1.6 to 2.2 billion people at risk. The effects, ineconomic terms are also described. There are also examples of anecdotal reports of the eliminationof IDD in the 1970s at village level in Indonesia, China and India.
IDD has been considered as a problem for developing countries, particularly in Asia, and obvious-ly the major international agencies targeted action in developing countries. However the problemin Europe was not neglected by the International Council of the Control of IDD.
Endemic goitre, often complicated by endemic cretinism, has been reported for centuries, especial-ly in mountainous areas in Switzerland, Austria, Italy and France. IDD has been entirely eradicat-ed in Switzerland, since 1990, due to the implementation of a salt iodisation programme, which hasbeen continually sustained. The impact of this programme has been noted by medicine, so thatIDD has not been considered an important problem for some years and become neglected. Yet in1999 it was considered by the WHO that 34 European countries were affected by IDD, with atotal population of 670 million of which 275 million were at risk. In 2002, the following countrieswere still considered deficient: Belgium, Denmark, France, Germany, France, Hungary, Italy,Ireland, Serbia and Montenegro, Romania, Slovenia, Spain and Turkey as well as many of thecountries previously comprising the Russian Federation.
It is shaming that iodine deficiency; the most common preventable cause of mental deficiency inthe world, is still so common in Europe. This is due to the lack of awareness and concern byhealth authorities, doctors and the public at large. This book demonstrates the great diversity oflegal, political, and logistic measures required in order to have an effective iodised salt programmein place to eliminate IDD and its health consequences.
The participants in IDD research and implementation adopted a ‘wheel model’ for their work, anexcellent model of what needs to be done if a disease is to be controlled. The outer ring is con-cerned with the population at risk, the prevalence of IDD, the salt economy, the health professionand public community groundswell education and training, resource allocation and assessment ofprevalence of IDD, urinary iodine and salt iodine levels as outcomes. The spokes comprise corre-spondingly situation assessment, communication, developing action plans, achieving political will,implementation of the programme and finally its evaluation.
The development of the steps that were taken to mobilise global concern with IDD and its controlby the involvement of the UN and its agencies, WHO and UNICEF, are fascinating. It is notoften that one reads a coherent narrative of the necessary steps required to mobilise the interna-tional community to take effective action to control a preventable condition. Perhaps the onlyother example is the eradication of smallpox. The difference with IDD is however, that industryhad to be involved, consumers persuaded and systems developed in order that people in veryremote, inaccessible regions could be reached.
This volume describes the measures taken in the various countries and regions and illustrates thecomplexity and different political, legislative, logistic as well as communication methods required.Although it is reckoned that almost 70% of households now have access to iodised salt and thatabout 80 million newborns are protected, with a saving of over one billion IQ points, there are still

eurohealth Vol 10 No 2 45
41 million unprotected newborns. This shows the continuing need to sustain progress made, tacklethe problem of countries backsliding in their iodised salt coverage and help and encourage saltproducers.
The story of IDD, so far, is a remarkable example of how epidemiological scientists can do bothgood science, and also develop and influence methods of prevention and control. It is a goodexample for teachers demonstrating the methods of disease control for a non-infectious condition.It illustrates the complexity and challenge of effective interventions based on good evidence andthe need for adaptability in different locations.
The book has many photographs and sketches by Anne Hetzel of the affected, as well as the areasin which work was done. For epidemiology it is both an example of how a dedicated group of sci-entists can work well together for a common goal and how one can introduce non-epidemiologicalmedical scientists into our field. This work is a fitting description of how an ‘ancient scourge’ canbe controlled.
This book brings together information from the Providing Integrated Health and Social Care forOlder Persons – Issues, Problems and Solutions (PROCARE) project in the EU Fifth FrameworkProgramme (Quality of Life and Management of Living Resources, Area “The AgeingPopulation and Disabilities”) that aims to help in defining the new concept of integrated healthand social care for older people in need of care by comparing and evaluating different modes ofcare delivery. The project will identify structural, organisational, economic and social-culturalfactors and actors that constitute an integrated and sustainable care system with enhanced out-comes for all actors involved.
This book gathers the achievements of the first project phase (2002) that consisted in a literatureoverview focusing on the question which of the variety of innovations in modes of organisation,finance and professional collaboration observed in Europe over the last decade have been themost successful and long-lasting ones. Thus, national reports from nine EU Member States(Austria, Denmark, Finland, France, Germany, Greece, Italy, the Netherlands and the UK) willbe presented by scholars from leading research and consulting agencies in these countries. Thenational reports follow a mutually agreed structure.
The publication is introduced by a general overview and a more theoretic article defining theissues at stake. It provides a general overview on European approaches towards integrated socialand health care services and policies that are to be developed to face the growing need of care inageing societies; furthermore, it provides indicators for successful approaches and models of goodpractice to overcome the ‘social-health-divide’ and a better understanding of the meaning of inte-grated services and coordination of social and health systems in the different countries. Finally,facts and figures about coordination at the interface between health and social care for older peo-ple as well as problems and solutions (‘lessons to learn’) concerning regulation and coordinationare exhibited by well-known scholars in social and health policy research.
Professor Adalbert Evers, from Justus-Leibig-University in Germany in reviewing the book hassaid that it’s strength “lies in the fact that it brings together what is usually separated: theoreticalreasoning and down-to-earth organisational model building, the presentation of illustrativenational peculiarities and of well-structured cross-national analysis, a reflection of the values thatare so important for the actors of change and sober empirical reports - for the use of a broadrange of professionals, scientists and policy makers.”
Contents
Introduction: Providing integrated health and social care for older persons – a Europeanoverview, Kai Leichsenring; Integrated health and social care for older persons: theoretical andconceptual issues, Andy M Alaszewski, Jenny Billings and Kirstie Coxon. National Reports:Providing integrated health and social care for older persons in Austria, Margit Grilz-Wolf,Charlotte Strümpel, Kai Leichsenring and Kathrin Komp; Denmark, Ellinor Colmorten, ThomasClausen and Steen Bengtsson; Finland, Paula Salonen and Riitta Haverinen; France – an old ideawith a great future, Michel Frossard, Nathalie Genin, Marie-Jo Guisset and Alain Villez;Germany, Günter Roth and Monika Reichert; Greece, Aris Sissouras, Maria Ketsetzopoulou,Nikos Bouzas, Evi Fagadaki, Olga Papaliou and Aliki Fakoura; Italy, Giorgia Nesti, StefanoCampostrini, Stefano Garbin, Paolo Piva, Patrizia Di Santo and Filomena Tunzi; TheNetherlands, Carine Ex, Klaas Gorter and Uschi Janssen; United Kingdom, Kirstie Coxon, JennyBillings and Andy M Alaszewski.
Public Policy and SocialWelfare Series, Volume28:
Providing IntegratedHealth and SocialCare for OlderPersons
A EuropeanOverview of Issuesat Stake
Edited by KaiLeichsenring and AndyM. Alaszewski
Aldershot:Ashgate,2004
ISBN 0-7546-4196-1
510 pages. Paperback
£27.50

eurohealth Vol 10 No 246
EU newsCOMPILED BY EUROHEALTH WITH ADDITIONAL INPUT FROM EUROHEALTHNET
Press releases and other suggested informationfor future inclusion can be e-mailed to the editorDavid McDaid [email protected]
Conference: Shaping the EUHealth Community
As part of the Presidency, a confer-ence, Shaping the EU HealthCommunity, was held in The Haguefrom 7–9 September attended by 440stakeholders in health care, includingrepresentatives of consumer groups,from all 25 EU Member States. Thefollowing themes were discussed.Public health and internal market As the European Union regulatesalcohol, tobacco and food, and asso-ciated services, such as advertisingand sales promotion, there is hugepotential for influencing health out-come through effective market legis-lation.
Cross border care Standardised information about pro-vision, quality, price and availabilityof care is needed.
eHealthICT is a tool to ensure the requiredlevel of information, choice andempowerment. A full vision of theintegration of eHealth into healthand social care is needed from theHealth Ministers of the EuropeanUnion.
Drugs and medical devicesMore transparency is needed in pre-scription, use and pricing of drugsand medical devices. Therapeuticadded value should be foremost forall parties concerned, i.e. industry,prescribers and consumers.
Health care in the local communityPrimary health care should be incor-porated in policy and decision mak-ing at the EU level. Therefore, indi-cators should be developed.
Long term carePublic campaigns for health promo-tion and healthy ageing are needed topostpone the dependency of theelderly.
Among the principle outcomes ofthe conference were a recommenda-tion that decisions taken byEuropean institutions should containa health impact assessment, and thatEuropean standards and codes arerequired to promote the quality ofhealth care. The conference also stat-ed that public campaigns are neces-sary to inform European citizensabout health promotion and healthyageing. The chair of the conference,Ms Iris van Bennekom, hailed theconference a success and wasdelighted about the willingness ofthe representatives of the Europeanhealth care sector to work togethertowards better health care in theEuropean Union.
Informal Health Council
The conference was followed by aninformal Health Council held inNoordwijk from 9–10 September.Ministers of Health of the MemberStates of the European Union,exchanged ideas on the theme ofHealth Care in an Ageing Society, a
Challenge for all EuropeanCountries. The subject was intro-duced by Professor NS Klazinga(Professor of Social Medicine at theAMC/University of Amsterdam).The ministers also took note of theconclusions of the conferenceShaping the EU Health Community.The meeting gave rise to a number ofobservations by the DutchPresidency. These included acknowl-edgment that ministers acrossEurope are concerned about thefinancial and social sustainability andefficiency of their health care sys-tems. Demographic ageing, theintroduction of new medical tech-nology and growing expectationsconcerning health care and healthcare services all play a role in thisdevelopment. While greater ageing isa sign of progress and success it wasnoted that this also presents chal-lenges. First, how can Member Statesensure that ageing citizens remainhealthy for as long as possible?Second, how can health care beorganised in such a way as to guar-antee that all will have access to nec-essary health care without overload-ing the labour market? Third, howcan health care systems be reformedin order to provide the next genera-tion with a financially feasiblemodel?
The meeting demonstrated thatwhile each country is pursuing itsown policy regarding these chal-lenges, there are similarities. In manycases, reforms of the health care sys-tem include combinations of: intro-ducing more financial incentives toimprove efficiency and productivitywhile respecting solidarity; introduc-
HEALTH UNDER THE DUTCH PRESIDENCY
The focus of health under the Dutch Presidency is on cooperation between Member States. The mantra of this work is therelationship between healthcare and adjacent areas of policy, such as agriculture and the environment. A wide range of issuesare being covered including: ageing populations, health and the internal market, infectious diseases, healthy foods, cross bor-der mobility of patients and professionals, information for patients, and issues around the environment and health. ThePresidency will also play an active role in the European Year of Education through Sport.
More information on the Dutch Presidency is available at:www.minvws.nl/en/themes/european_union_dutch_presidency/default.asp
Further information and presentations from the ‘Shaping the EU HealthCommunity’ conference are available at www.euhealthcommunity.org

eurohealth Vol 10 No 2 47
Research and Science: JanezPotocnik (Slovenia)Mr Potocnik is 46 and was educat-ed in Ljubljana. He was an eco-nomic analyst by profession beforebecoming director of the govern-ment office for European affairs in2000 and subsequently at the PrimeMinister’s Cabinet. He wasMinister for European Affairs from2002 until his nomination asCommissioner.
Emp loymen t , Soc ia l A f fa i r s &Equal Oppor tu in i t ies : V ladimirSpidia (Czech Republic)Mr Spidia is 53 and was educated inPrague, with a varied career includ-ing public administration. He waselected to the Parliament in 1996,and became Minister of Labourand Social Affairs in 1998 thenPrime Minister in 2002. Heresigned in spring 2004 and wasrecently nominated as EuropeanCommissioner to replace PavelTelicka, who will complete hisperiod of office in October.
Heal th & Consumer Protec t ion:Markos Kyprianou (Cyprus)Mr Kyprianou is 44 and was edu-cated at Athens, Cambridge andHarvard. He practised law inCyprus 1985–2003, specialising incompany law and taxation. MrKyprianou was elected to theHouse of Representatives threetimes from 1991 before becomingFinance Minister 2003-2004, whenhe was nominated to the EuropeanCommission.
In October the EuropeanParliament will question the pro-posed Commissioners in a series ofpublic hearings prior to voting onwhether to approve the new collegeof Commissioners as a whole.Provided the new Commissionersare endorsed they will then take uptheir positions on 1 November.
Profiles of all new Commissionersare available from:http://europa.eu.int/comm/commissioners/newcomm_en.htm
ing a more patient centred care sys-tem; and stimulating more personalresponsibility.
In order to keep society, healthy,active and productive the participa-tion of older people in society needsto be enhanced, evidence based poli-cies for chronic diseases need to bestimulated, and a new balance isrequired between personal and pub-lic responsibility in order to safe-guard affordable, accessible and sus-tainable health systems. The Dutchalso observed a common need toimprove cost awareness upstreamprevention strategies, and to investin primary and community basedcare while also stimulating integrat-ed care, medical innovation, healtheducation and the empowerment ofpatients. The Ministers agreed to theDutch Presidency initiating a meet-ing with members of the High LevelGroup on Health Services andMedical Care in an informal settingin addition to the regular meeting todiscuss the introduction of a perma-nent mechanism on health careissues in order to submit a proposalto the December 2004 Council.
The Informal Council was also oneof the final opportunities forCommissioner Byrne to set out hisperspectives on the way ahead. Inhis speech the Commissionerstressed the need to balance qualityimprovements with the need tomaintain core values and ensure sus-tainability. He commented that “ourresponse should focus on improvingthe quality of healthcare and healthpromotion, not by reducing solidar-ity and access to healthcare, nor bycreating financially unsustainablesystems.” He also recognised thecrucial role to be played by oldercitizens to continued economicgrowth stating that “active, healthyolder people are a valuable resourcefor society. We can project the pos-sible costs of increased healthcare,but we do not project the additionalcontribution that these people willmake to their families, to societyand to the economy at large.” TheHealth Council will meet formallyon 4 October and 6-7 December
Further information on the InformalHealth Council is available atwww.minvws.nl/images/future_challenges_tcm11-54749.pdf
APPOINTMENT OF NEW COMMISSIONERS
The incoming President of the European Commission, Jose Manuel DuraoBarroso, has announced the portfolios for the 25 new Commissioners due totake office from 1 November for the next five years. These include:
Tech Central Station Europe isoffering a prize of €2500 for thebest commentary piece by aEuropean on the theme, Puttingpatients first: Visions for EuropeanHealth Care. According to TCSEurope Editor, Craig Winneker,“Europeans endure long waits formedicines, treatment and surgeries– and pay high taxes for this sub-standard level of care. Patients lackchoice and access to the best medi-cines. European patients deserve21st century care and this contestseeks to engage Europe’s bestminds on how to improve theircountry’s health care system.”
The contest is open to allEuropeans and while submissionsmust be in English, special consid-eration will be given to originalthinking. The contest will also con-sider previously published pieceson this exact theme. Such submis-
sions must have been publishedwithin the previous 3 months and atranslation should accompany thepiece it was not originally inEnglish. Please submit to pieces byNovember 15 to HenrikRasmussen at [email protected] and include ashort personal biography as well asall relevant contact information.
Results of the contest will beannounced in December. The topfive commentaries will be publishedby www.techcentralstation.com.Authors will be compensated iftheir piece is selected for publica-tion. Pieces must not exceed 1,000words and will be judged by apanel consisting of TCS editors,Nick Schulz and Craig Winneker,and TCS host, James K Glassman.Tech Central Station is a news site,focusing on free markets and tech-nology.
AWARD ANNOUNCED FOR BEST COMMENTARY ON EUROPEANHEALTH CARE REFORM

eurohealth Vol 10 No 248
Europeans less inc l ined toexerc i se to p ro tec t t he i rhealth says Commission
2004 has been designated theEuropean Year of Educationthrough Sport. As part of the ini-tiative the European Commissionhas chosen to re-issue a 2003 sur-vey which shows that only one inthree EU-15 citizens engage insport on a weekly basis and only15% exercise three times a week.The Eurobarometer Survey inter-viewed 16,000 people over the ageof 15 from the 15 Member States.During the year the Commissionaims, through a series of initiativesacross Europe, to raise awarenessabout the beneficial links betweeneducation and sport. This willfocus on the key role that ahealthy lifestyle plays in reducingcardiovascular disease and otherlife-threatening problems. Toemphasise the importance of sportin everyday life, EU ministershave agreed to include sport in theEU Constitution. It was the firsttime ever that there has been anexplicit reference to sport in anEU treaty.
French public health law toshift from cure to preventionA proposal to amend France’s pub-lic health laws has gone through asecond reading in the Senate. One ofthe key innovations proposed in thetext is to shift the focus of thehealthcare system from treatment toprevention. Officials note thatFrance ranks low in Europe in pre-vention efforts and has a high rate ofpremature death, (i.e. death beforethe age of 65). Only 2% of theannual national health budget of€150 billion is devoted to preven-tion. The new law will be a signifi-cant step in increasing the nation’sinvestment in health education andprevention efforts. In addition, mea-sures targeting dangerous productshave been adopted, such as anamendment that will set a minimumthreshold for cigarette prices makingit impossible to have special offerstargeting new consumers.
More information at :www.senat.fr/dossierleg/pjl03-019.html
On 6 September it was announcedby the WHO Regional Committeefor Europe that the WHOEuropean Region is to have a sus-tainable strategy to face the largeand growing problem of non-com-municable diseases.
Over 300 delegates representing the52 Member States of the Regionhave decided to give high priorityto non-communicable diseases andto develop a comprehensiveEuropean strategy by the end of2006. The strategy is to target themain killer diseases in the Region,such as cancers, cardiovascular dis-eases, diabetes and respiratory dis-eases. It will also explore ways tocounter the risk factors responsiblefor their heavy and growing bur-den: tobacco use, alcohol abuse,raised blood pressure, raised cho-lesterol, overweight or obesity, lowfruit and vegetable intake, andphysical inactivity.
“The Member States’ very explicitsupport for this strategy shows thatthey are determined to take actionto limit the harm done by non-communicable diseases”, said DrMarc Danzon, WHO RegionalDirector for Europe. “Progress inthis area, and on tackling risk fac-tors as a whole, can only comefrom the combined efforts of indi-viduals and society as a whole”, headded. Of WHO’s six regions, theEuropean Region is the worstafflicted by non-communicablediseases, and their growth is star-tling. In 2002, they caused 86% ofdeaths and 77% of disease burden.According to WHO statistics, theleading non-communicable diseasesin the Region in 2002, in terms ofmortality, were cardiovascular dis-eases, cancers, respiratory disor-ders, digestive disorders and neu-ropsychiatric disorders. In terms ofburden of disease, the chief con-tributors were estimated to be car-diovascular diseases (23%), neu-ropsychiatric disorders (20%) andcancers (11%).
Across the Region, non-communi-cable diseases not only target indi-viduals, but also attack societies
and countries, placing extra strainon health-care systems and threat-ening economic and social develop-ment. They overwhelmingly affectthe poor. Mortality from cardio-vascular diseases, for instance, hasincreased at all ages in the newlyindependent states (NIS) over thepast decades. In 2000, the averagefigures for cardiovascular diseasemortality were three times higherthan those for the then EuropeanUnion. The Region’s poorer coun-tries face the double burden of ris-ing non-communicable diseaserates, as well as persistent commu-nicable diseases and inadequatehealth systems. People in lowsocioeconomic groups have twicethe risk of serious illness and pre-mature death of those in highsocioeconomic groups, partlyowing to poorer access to healthyfood and greater tobacco andharmful alcohol consumption.Most health-system resources go tonon-communicable diseases andthis trend will continue. A signifi-cant proportion of the total cost ofcare falls on patients and their fam-ilies.
Non-communicable diseases arelargely preventable. Dr GudjónMagnússon, Director, Division ofTechnical Support, ReducingDisease Burden, at the WHORegional Office for Europe said“There is a lot of action in differentcountries, by governments, donors,the private sector, nongovernmen-tal organizations and other groups,but we need these different playersto pool their knowledge and worktogether. That is the only way weare going to reduce the death andsuffering inflicted by non-commu-nicable diseases. A European strat-egy on non-communicable diseasescould be the beginning of a newunited fight to save the lives notjust of the citizens of today’sEurope, but of generations tocome.”
More information on non-commu-nicable diseases is available atwww.euro.who.int/mediacentre/20020617_1
HEALTH MINISTERS TO MAP OUT A PAN-EUROPEAN STRATEGY ONNON-COMMUNICABLE DISEASES BY 2006

What are the palliative careneeds of older people and howmight they be met?Many countries have ageing popula-tions. With coordinated care, morepeople could die at home if theywished, and with specialist palliativecare more patients and their familieswould benefit from a range of betteroutcomes. A new report from theHealth Evidence Network writtenby Elizabeth Davies from theDepartment of Palliative Care andPolicy at Guy’s, King’s and StThomas’ School of Medicine,London concludes that, althoughfurther research is needed, the morepressing issue is to put existingknowledge about palliative care intopractice and sustain the good prac-tices that already exist, throughoutthe health care system.
The report is available at www.who.dk/eprise/main/WHO/Progs/HEN/Syntheses/palliative/20040722_3
World Mental Health Day 2004World Mental Health Day 2004 willbe observed on 10 October. Thisyear’s theme is entitled “The rela-tionship between physical and men-tal health: co-occurring disorders.”
More information together withaccess to the the World Federation onMental Health’s Annual Report 2003can be found at www.wfmh.org
International conference – PROCARE: Providing IntegratedHealth and Social Care forOlder Persons – Facing theChallenges in EuropePROCARE is a two year interna-tional research project co-financedby the European Union’s FifthFramework Programme with theaim to promote the new concept ofintegrated health and social care forolder persons in need of care bycomparing and evaluating differentmodes of care delivery. PROCAREhas been carried out by a consortiumof ten organisations from nineEuropean countries. The results ofthis two year project will be pre-sented at the conference taking placefrom 21–23 October in Venice.
More information at:www.euro.centre.org/procare
What are the equity, efficiency,cost containment and choiceimplications of private health-care funding in westernEurope? Over the last 20 years the level ofprivate spending on health care hasrisen in many western Europeancountries, leading to concern aboutits impact. The main channels of pri-vate spending are private healthinsurance policies and cost-sharingschemes in public health systems. Anew report from the HealthEvidence Network written by SarahThomson and Elias Mossialos fromthe European Observatory onHealth Systems and Policies at theLondon School of Economics con-cludes that private sources of healthcare funding are often regressive andpresent financial barriers to access.They contribute little to efforts tocontain costs and may actuallyencourage cost inflation.
The report is available athttp://www.who.dk/HEN/Syntheses/hcfunding/20040629_3
Sixth Annual Conference onIntegrated Care This conference taking place atDublin Castle on 14–15 February2005 aims to bring togetherresearchers, policy makers and prac-titioners working with providers ofhealth and social care to exchangeknowledge and experiences on inte-grated care. The deadline for sub-mission of abstracts is 1 November2004.
Further information available atwww.integratedcarenetwork.org/conference2005/
Health in the EU from a DutchPerspectiveThe Dutch Presidency have pub-lished a document entitled ‘How dowe do, Health in the EU from aDutch Perspective’. This looks at arange of health issues: health status,health determinants, and health caresystems and compares the Dutch sit-uation with other Member Stateshealth situations.
This is available at www.minvws.nl/images/how%20do%20we%20do_tcm11-51837.pdf
Marc Danzon nominated to second term as WHO RegionalDirector for EuropeDr Marc Danzon has been nominat-ed to a second five-year term as theWHO Regional Director forEurope. Dr Danzon, a Frenchnational and the first representativeof France to lead a WHO region,announced in February this year thathe would run again. No candidateopposed him. Dr Danzon will for-mally begin his second term on 1February 2005. He called the vote onhis re-election an endorsement of theWHO Regional Office for Europe’scontinuing work “to supportMember States in better respondingto the health needs of their citizens”.
For his second mandate, Dr Danzonwill give priority to “helpingMember States to strengthen theircapacity to respond to health threats;continuing the fight against obesityand noncommunicable diseases; pro-viding health decision-makers withvalidated and accessible health infor-mation; and, of course, contributingto the global fight againstHIV/AIDS.”
More information atwww.who.dk/eprise/main/who/mediacentre/pr/2004/20040907_1
Europeans demand changes totheir healthcare systemsA study, entitled “Impatient forChange - European attitudes tohealthcare reform” published by TheStockholm Network reveal that 84%of respondents think that changes tonational health systems are urgent ornecessary. The desire for change isthe strongest among the working-age, taxpaying population of the EU.77 % of those surveyed believe thatpatients should be given more infor-mation about their illness and aboutthe quality of care provided by doc-tors and hospitals, including in othercountries.
It is available at www.stockholm-network.org/pubs/imp.pdf
eurohealth Vol 10 No 2 49
EuroHealthNet6 Philippe Le Bon, Brussels Tel: + 32 2 235 03 20 Fax: + 32 2 235 03 39Email: [email protected]
News in Brief