Embed Size (px)
Citation preview
Vogt-Koyanagi-Harada Syndrome
Laura S. Gilmore, MD
Department of Ophthalmology
November 12, 2004
Discussant: Leo Dominguez, MD
Case Presentation• CC: loss of vision and hearing
• HPI: 38 yo HF with 3 wk h/o progressively decreasing vision OD, irregular pupils. Seen by multiple MDs. Treated at onset for “allergies”, then by Ophtho in NM with PO prednisone at 80mg/day, PF and Atropine for about 1 week prior to presentation here.
• PMH: No arthritis, RA, lupus, DM, HTN. +HepC.
• POH: Poor vision OS since 10yo 2o trauma. No h/o glasses’ wear.
• ROS: +Tinnitus, hearing loss, ocular pain, photophobia, scalp and hair tenderness, L occipital HA, poor balance/vertigo, hair/lash/brow thinning, hypopigmentation of face/arms, back pain.
Physical Exam
• General: AAO, BP 110/61, pulse 53. Poor hearing, poor balance.
• VA: 20/150 OD, LP OS
• Pupils: 5 NR OU, irregularly shaped
• External: Thin brows, lashes OU; splotchy white patches of skin over face, forehead, arms
• SLE: KP OU; posterior synechiae OU; 4+C/F; 3+pigment on anterior capsule; 4+ vitreous cells
• Lens: 2+NSC/2+PSC OU
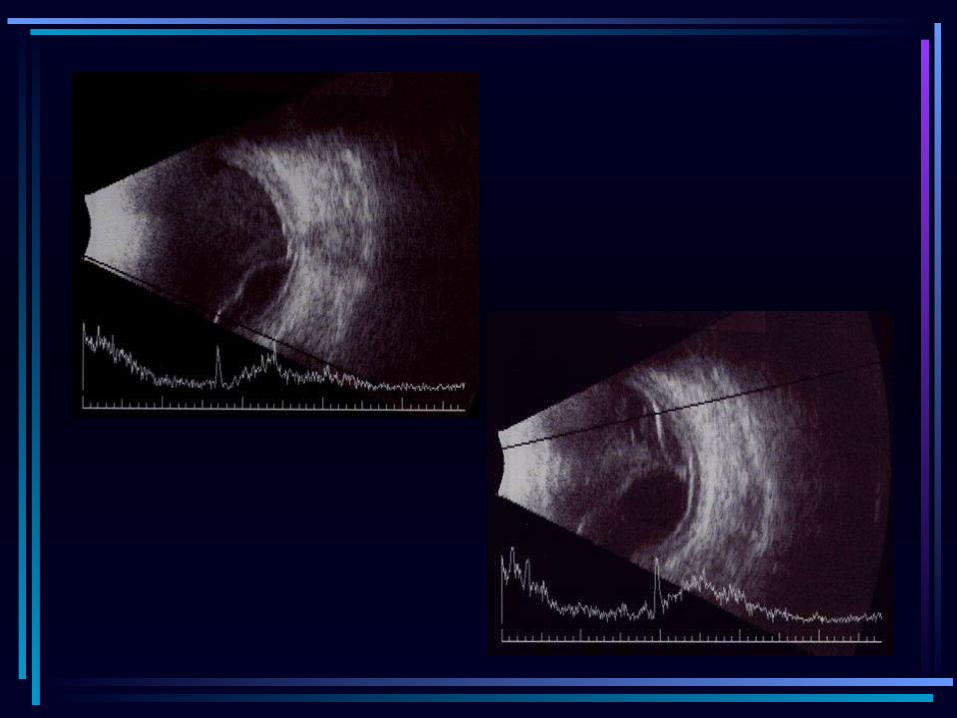
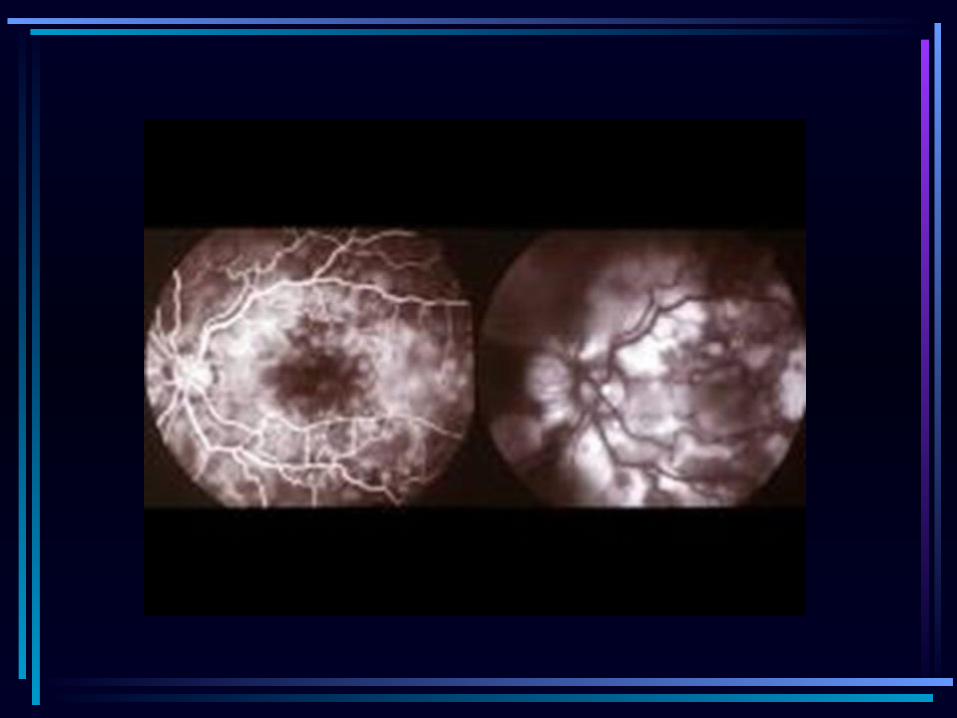
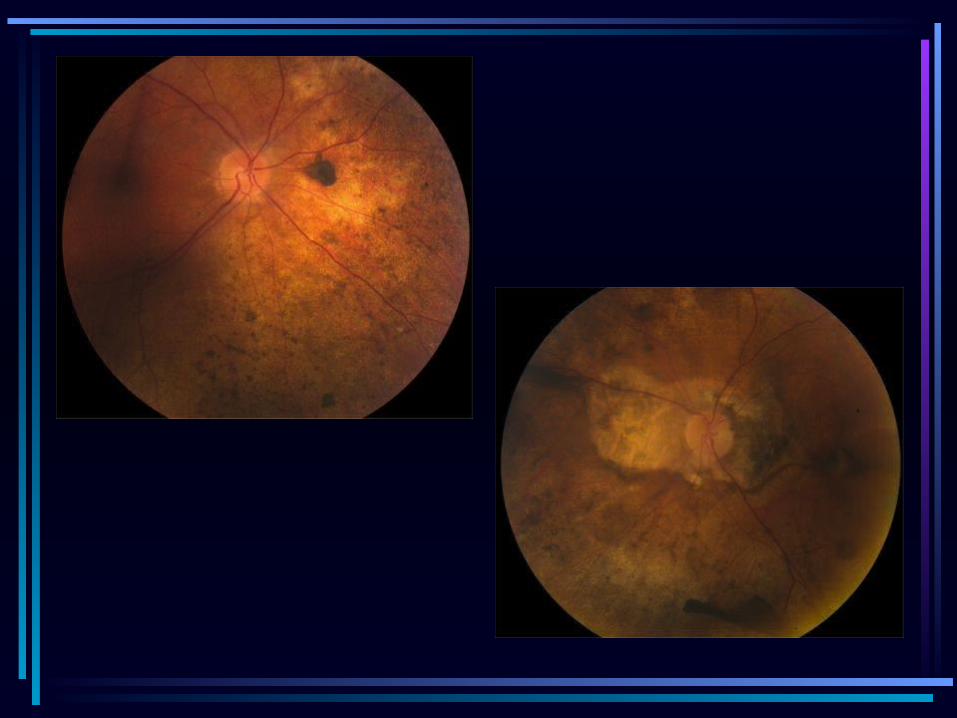
• B Scan: Serous RD OU; choroidal thickening; + vitreous cells

Differential Diagnosis
• VKH• Posterior scleritis• Uveal effusion syndrome • Harada's disease• Acute posterior multifocal placoid pigment
epitheliopathy• Sympathetic ophthalmia• Sarcoidosis
VKH• Uveoencephalitis• Extremely rare systemic disease of melanocyte-
containing organs• Characterized by bilateral uveitis with associated
cutaneous, neurologic, and auditory abnormalities• First described by Vogt in 1906 and Koyanagi in
1929 as anterior uveitis with poliosis, vitiligo, auditory disturbances (Vogt-Koyanagi syndrome)
• Harada reported a pt in 1926 with idiopathic uveitis affecting posterior segment, RD, and meningeal irritation
• Currently, VKH considered a single entity composed of variations of above symptoms
Etiology• Autoimmune response
- Reaction against antigen (tyrosinase or tyr-related protein?) shared by uveal, dermal, and meningeal melanocytes
- Circulating Ab against a retinal photoreceptor region- HLA-DR4 often present-commonly associated with other autoimmune diseases
• Viral reactivation, possibly EBV• Immunogenic predisposition
– Almost all cases are sporadic, with only rare familial cases
– But, susceptibility associated with specific HLA groups, particularly DRB*0405
Demographics
• Rare – No good data on frequency in US– Internationally, widely distributed
• Darker pigmented pts
• Range of presentation 10-52 years, maximum frequency in thirties
• Women affected more
Clinical Presentation, Phase One
• Prodromal (or meningeal)– Few days– HA, fever, photophobia, meningismus– Less common: gen muscle weakness,
hemiparesis, dysarthria, aphasia– Altered mental status, from mild confusion to
psychosis
Clinical Presentation, Phase Two
• Uveitic– Several weeks– When pt’s typically seek medical attention,
usually from Ophthalmologist– Bilateral blurred vision– Eye pain and irritation– Loss of vision– Tinnitus and dysacusis in 50%. May occur in
any of the 3 phases of VKH
Clinical Presentation
• Convalescent phase– Within 3 months of syndrome onset– Cutaneous signs
• Usually after onset of uveitis
• Have been reported years before any ocular sx
• Patchy alopecia
• Poliosis (in 90%) involving eyebrows, eyelashes, body hair and scalp
• Symmetrical vitiligo (in 63%) over head and trunk
Diagnosis• American Uveitis Society guidelines• No ocular trauma or surgery• At least 3 of following 4:
– B chronic inflammation of iris and CB– Posterior uveitis, including multifocal exudative RDs, and
disc hyperemia or edema– Neurological signs of tinnitus, neck stiffness, CN or CNS
dysfunction, cerebrospinal pleocytosis– Cutaneous findings of alopecia, poliosis, or vitiligo
• A-scan and B-scan• Multidisciplinary management• Consider LP for CSF analysis, FA, audiometry, skin
biopsy.
Treatment• Goal-reduce morbidity and prevent complications• Suppress initial intraocular inflammation
– Early and aggressive systemic steroids– 60-100mg PO QD– Slow taper over 3-6 months
• Unresponsive pts– Immunosuppression with azathioprine,
cyclophosphamide, or methotrexate
• Topical therapy– Steroid gtts– Cycloplegic-mydriatic gtts for sx relief
Prognosis• No mortality• Visual outcome depends on rapidity and
appropriateness of tx– Uncommon to have long term complications
• Reversible and irreversible vision loss• IOP elevation• Glaucoma• Cataracts
• Hearing almost always completely resolves• Cutaneous pigmentary changes usually permanent
Back to Our Case • Hospital Admission 7/11/03• IM, Rheumatology, Audiology, Gynecology• Labs:
– daily CBC and BMP, ESR, toxoplasma, ACE, FTA-ABS, RPR, ANA, PPD, Lyme titer, lupus anticoagulant, anticardiolipin Ab, anti-dsDNA, SSA Ab, SSB Ab, HLA-B27, hepatitis panel, HIV, VDRL, antiproteinase III, UA, antimyeloperoxidase, beta-HCG, AP/lateral CXR and LXR, CT head/orbits, MRI head/orbits
• Meds: – Solumedrol IV 1g/day per Rheum; PF gtt; atropine;
pepcid; azathioprine 100mg/day; tacrolimus, 2.5mg PO BID
Results
• MRI: – no inflammatory process in brain or
surrounding structures
• Labs: – ANA weakly positive, HepC +; all else
normal or negative, X-rays nl
• Audiology: – mild sensorineural hearing loss
Hospital Course• Improved hearing, balance, and visual acuity
throughout hospital stay
-VA 20/70 OD, LP OS
-no cells/1+flare OU
-decreased KP, vitreous cells
-DFE: improved view OU; inferior SRD OD, almost 360o SRD OS
• Discharged home at 1 week on PO Prednisone, Tacrolimus, Azathioprine, PF gtt, Atropine, Maxitrol ung
Relevant Clinical Course Since Discharge
• 7/18/03-Discharged home, s/p 1 week IV steroid therapy, aggressive immunosuppression
• 8/03-Timolol and Trusopt required for IOP 31, 34
• 10/17/03- 20/40 OD, CF @ 2ft OS, inflammation cleared, retina completely attached OU
• 11/03-began tapering Prograff, Azathioprine (Rheumatology)
• 12/03-began tapering PO prednisone and PF, d/c’d atropine
Clinical Course, Continued
• 7/04-3-4+Uveitic PSC OU
• 10/6/04-CE/PCIOL OD • 10/14/04-VA 20/30, very happy (with us)
• Immunosuppression low-dose now– Currently on prednisone 20mg PO QD,
azathioprine 50mg PO TID– Still requiring timolol and trusopt gtt
Conclusion
• Very rare
• Multidisciplinary treatment approach
• Early and aggressive immunosuppression with slow, prolonged taper required to improve outcome and decrease long-term complications
• Often have good outcomes
References• Choczaj-Kukula A, et al. Vogt-Koyanagi-Harada
Syndrome: eMedicine.com. Sept 2003.• Fattal D. Vogt-Koyanagi-Harada Syndrome
(VKH): summary and discussion of case presentation. Dept of Neurology, Baylor College of Medicine. 2001: www.bcm.tmc.edu/neuro1/index.html
• Islam SM, et al. HLA class genes in VKH disease. Invest Ophthalmol Vis Sci. 1994. 35: 3890-3896.
• Nussenblatt, RB, et al. Uveitis, Fundamentals and Clinical Practice. 1996. 312-324.
• Snyder DA, et al. VKH syndrome. Am J Ophthalmol. 1980. 90: 69-75.



![The Introspective House - Architects Registration Board · Mount Fuji Architects Studio - Tokyo (Masahiro Harada and Mao Harada)[3] Alphaville Architects - Kyoto (Kentaro Takeguchi](https://img.pdfslide.us/doc/110x75/5fe6fee18b960474295e1090/the-introspective-house-architects-registration-board-mount-fuji-architects-studio.jpg)

























