Embed Size (px)
Citation preview

Kidney International, Vol. 63, Supplement 85 (2003), pp. S44–S48
Vitamin D status and secondary hyperparathyroidism: Theimportance of 25-hydroxyvitamin D cut-off levels
CARLOS GOMEZ-ALONSO, MANUEL L. NAVES-DIAZ, JOSE L. FERNANDEZ-MARTIN,JOSE B. DIAZ-LOPEZ, MARIA T. FERNANDEZ-COTO, and JORGE B. CANNATA-ANDIA
Bone and Mineral Research Unit, Instituto Reina Sofıa de Investigacion; and Servicio de Bioquımica, Hospital Central deAsturias, Universidad de Oviedo, Spain
Vitamin D status and secondary hyperparathyroidism: The for measuring vitamin D, masking the effect of the afore-importance of 25-hydroxyvitamin D cut-off levels. mentioned factors and making the comparison between
Background. Serum 25-hydroxyvitamin D is the best indica- different populations difficult [3, 4].tor of vitamin D status. However, some controversy remainsWhen it comes to diagnosing vitamin D deficiency andregarding “normal” and “abnormal” values. This study’s aim
pinpointing exactly at what level it occurs, there is nowas to assess vitamin D status and prevalence of secondaryhyperparathyroidism. definitive consensus. Traditionally, vitamin D values be-
Methods. A random sample of 326 subjects (164 women and low 5–7 ng/mL induce osteomalacia, values lower than162 men, aged 68 � 9; range, 54 to 89) participating in the
10–12 ng/mL lead to secondary hyperparathyroidism andEuropean Vertebral Osteoporosis Study (EVOS) was used toosteoporosis, and levels above 18–20 ng/mL are consid-assess vitamin D status and secondary hyperparathyroidism.
Only those subjects who had never received any kind of treat- ered normal [5]. It has recently been proposed that levelsment for osteoporosis were included in this analysis. �40 ng/mL (�100 nmol/L) are desirable, that hypovita-
Results. Serum 25-hydroxyvitamin D levels were “deficient” minosis D occurs when the levels are between 20 and 40(�10 ng/mL) in 27% of subjects, “borderline” (10–18 ng/mL)ng/mL (50-100 nmol/L), vitamin D insufficiency occursin 40% of subjects, and “normal” (�18 ng/mL) in 33% of sub-when the concentration is between 10–20 ng/mL (25–50jects. The prevalence of secondary hyperparathyroidism (PTH
�65 pg/mL) according to 25-hydroxyvitamin D levels was 33% nmol/L), and vitamin D deficiency is seen with values(�10 ng/mL), 16% (10–18 ng/mL), and 12% (�18 ng/mL), re- lower than 10 ng/mL (�25 nmol/L) [6].spectively. There were no cases of secondary hyperparathyroid- The prevalence of vitamin D deficiency depends onism with 25-hydroxyvitamin D levels �40ng/mL. The indepen-
the cut-off point used, as well as the type of populationdent predictors for PTH were 25-hydroxyvitamin D and serumstudied. Therefore, a vitamin D deficiency was found increatinine in both sexes, but age was a predictor only in men.
Conclusion. These remarkable findings demonstrate the im- almost all of the chronic geriatric patients [7], and inportance of maintaining higher 25-hydroxyvitamin D levels to 57% of the American acute symptomatic patients [8].avoid stimulation of the parathyroid gland.
The prevalence of vitamin D deficiency was 36% of menand 47% of women in the European elderly population.Surprisingly, the most southern countries showed theThe vitamin D hormonal system consists of differentlowest levels [9], and, in women with postmenopausalmetabolites, ranging from cutaneous synthesis precur-osteoporosis, the deficiency prevalence ranged from 0%sors or dietary components, to the most active metabolite,in Singapore to 3.5% in the US, and slightly above 10%1,25-dihydroxyvitamin D, which acts upon the target or-in France and Spain [10].gan receptors [1]. The best indicator of vitamin D depos-
The objective of this study was to investigate the vita-its or status is the concentration of 25-hydroxyvitamin Dmin D levels and the prevalence of secondary hyperpara-[2]. Several factors determine vitamin D levels, includingthyroidism in a random study of the sector of our popula-factors that affect the skin’s synthesis of vitamin D throughtion at an age when they were most at risk from a clinicalultraviolet radiation, nutrition, and those which can mod-repercussion of vitamin D deficiency.ify vitamin D’s metabolism [2]. Moreover, there is a great
variability in both intra- and inter-laboratory methodsMETHODS
The study was carried out in Oviedo, a city in northernKey words: calcifediol, calcitriol, vitamin D deficiency, parathyroidhormone. Spain located at a latitude of 43�N, 400 meters above sea
level, and with a temperate climate (average temperature 2003 by the International Society of Nephrology
S-44

Gomez-Alonso et al: 25-Hydroxyvitamin D normal levels S-45
Table 1. General characteristics and biochemical data of the14�C), 1924 hours of sunlight per year, 900 mm of precipi-subjects included in the analysis
tation per year, and where it rarely snows or freezes.Men (N � 134) Women (N � 134)Three hundred and twenty-six people (164 women and
Age years 68�9 68�8162 men) between the ages of 54 and 89 who had beenHeight cm 165 �6 153 �6a
previously randomly selected from the Oviedo popula- Weight kg 76�10 67�11a
tion register to participate in the European Vertebral Menopause years — 49�5Dairy product intake cup/day 1.5 �1 1.7�1Osteoporosis Study (EVOS) [11] were included. In theCalcium mg/dL 9.4 �0.3 9.4�0.3fourth year of the study, a blood sample was drawn Phosphorous mg/dL 3.3 �0.4 3.6�0.4a
Creatinine mg/dL 1.1 �0.1 0.9�0.1aso that serum could be studied to determine variousAlkaline phosphatase 168�56 179�52parameters related to bone metabolism. All of the parti-25-hydroxyvitamin D ng/mL 17.2 �8.3 15.6�9.1b
cipants were Caucasian, self-ambulatory, and 99% lived Calcitriol pg/mL 45�18 37�12a
iPTH pg/mL 49�21 54 �24bin their own homes. The study took place during oneOsteocalcin ng/mL 5.3 �1.8 6.5�2.4a
year: 26% of the studies in spring, 14% in summer, 36%aP � 0.001in autumn, and 24% in winter. Other aspects relating to bP � 0.059
this study have been previously published [11, 12].In all subjects, a fasting blood sample was drawn first
thing in the morning. Once the serum was separated, itare shown in Table 1. The mean values of 25-hydroxyvi-was kept frozen at a temperature of �70�C until the analy-tamin D in the subjects excluded due to previous treat-ses were carried out. Serum calcium, phosphorus, creati-ment for osteoporosis were significantly higher com-nine, total alkaline phosphatase, and tartrate-resistantpared with the general sample (24.5 � 11.7 vs. 15.9 �acid phosphatase were determined by using an autoana-8.7 ng/mL; P � 0.001), without any difference in age orlyzer (Hitachi Mod. 717, Ratigen, Germany). The 25-the season in which blood was drawn.hydroxyvitamin D levels were determined by previous
The higher 25-hydroxyvitamin D levels were observedextraction with acetonitrile (IDS, Ltd., Bolton, UK),in the summer period—summer/autumn (19.4 � 10.3whose intra- and interassay coefficients of variation (CV)ng/mL) compared with the winter period—winter/were 5.2% and 8.2%, respectively.spring- (13.7 � 6.8 ng/mL; P � 0.001), without any sig-The 1,25-dihydroxyvitamin D levels were measurednificance in the differences observed between summerthrough radioimmunoassay (IDS, Ltd.); intra- and in-and autumn or winter and spring. A similar seasonalterassay CV were 6.5% and 9%, respectively. The intactpattern was observed in PTH (47 � 20 pg/mL comparedPTH and osteocalcin levels were measured using radio-with 55 � 23 pg/mL; P � 0.015) and alkaline phosphateimmunoassay methods (Nichols Institute, San Juan de(165 � 51 U/I compared with 178 � 55 U/I; P � 0.045)Capistrano, CA); intra and interassay CV were 2.6% andin summer and winter, respectively.5.8%, respectively, for PTH and 4.5% and 5.1%, respec-
The percentage of patients with insufficient levels oftively, for osteocalcin.
25-hydroxyvitamin D (�10 ng/mL) or acceptable levelsStatistical analysis was carried out using the SPSS Ver-
(�18 ng/mL) was notably different in winter comparedsion 8.0 package for Windows (Microsoft Corp., Red- with summer in those subjects aged less than 75. How-mond, WA, USA). The results are expressed as mean � ever, these differences were not present in those agedstandard deviation or percentages and were compared more than 75 (Table 2).using the Student t test, one way analysis of variance The prevalence of secondary hyperparathyroidism(ANOVA), or the Chi-square test as necessary. The cor- (PTH �65 pg/mL) was 18.5% of the men and 24.1% ofrelations were established through the Pearson coefficient. the women, a similar progression being noted as ageThe multivariate regression analysis was carried out follow- increased (Fig. 1). The PTH correlated with 25-hydroxy-ing the stepwise method. In every case, differences were vitamin D (r � 0.3; P � 0.01). Thus, 33% of the subjectsconsidered significant at a level of P � 0.05. with 25-hydroxyvitamin D levels �10 ng/mL showed hy-
perparathyroidism, contrasting with 13% of the individu-als with 25-hydroxyvitamin D �18 ng/mL (Fig. 1). It was
RESULTS observed that only values of 25-hydroxyvitamin D aboveThe following subjects were excluded from the study 30 (only one case of hyperparathyroidism) or 40 ng/mL
(N � 44) due to several reasons: 1 due to primary hyper- (no cases) guaranteed normal PTH values.parathyroidism, 1 for epilepsy treatment, 2 for severe The multivariate linear regression showed that the 25-chronic renal failure (serum creatinine �1.6 mg/dL), and hydroxyvitamin D levels (standard correlation coeffi-the rest for having had previous osteoporosis treatment. cient � � �0.29; P � 0.001), serum creatinine (� � 0.35;
P � 0.001), and sex (� � 0.28; P � 0.001, with r �The general characteristics of the 268 remaining patients

Gomez-Alonso et al: 25-Hydroxyvitamin D normal levelsS-46
Table 2. Seasonal 25-hydroxyvitamin D according to age expressed as percentage of subjects in each level
Winter/spring Summer/autumn
Age �10 ng/mL 10–18 �18 ng/mL �10 ng/mL 10–18 �18 ng/mL
�65 30% 42% 28% 13% 35% 52%65–74 40% 40% 20% 12% 46% 42%�75 27% 45% 27% 25% 50% 25%
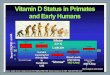
Fig. 1. Prevalence of secondary hyperpara-thyroidism (PTH �65 pg/mL) according tothe age and sex of the subjects (A ) and to the25-hydroxyvitamin D levels (B ).
0.40; P � 0.001) were independent predictors of PTH. In The 25-hydroxyvitamin D levels were 40% higher insubjects with excellent renal function—serum creatinine summer than in winter, a reflection of the differences in�0.8 and 1 mg/dL in women and men, respectively—no solar exposition. The mean winter values were below 15cases of secondary hyperparathyroidism were observed ng/mL, which is the value used as the defining limit forin individuals having 25-hydroxyvitamin D levels above deficiency by some authors [9, 24], supporting the limited18 ng/mL in men and 12 ng/mL in women. The indepen- capacity of vitamin D skin synthesis in winter in latitudesdent predictors of calcitriol were sex (� � 0.36; P � higher than 40�N [21]. The summer/winter difference was0.001), 25-hydroxyvitamin D levels (� � 0.22; P � 0.001), substantially higher than the 14% observed in the adultplasma creatinine (� � 0.24;P � 0.001), and serum cal- American population [19], and much lower than the 88%cium (� � 0.15; P � 0.08), with a global regression of differences observed in the infant Spanish populationcoefficient of r � 0.40; P � 0.001. at a latitude similar to our own, in which the summer
Concerning the bone remodeling markers, the inde- values were similar [13]. These differences probably re-pendent predictors of osteocalcin were PTH, sex, and flect a lesser nutritional contribution in our populationserum phosphorus (� � 0.23, 0.19, and 0.16, respectively; and a better response to cutaneous synthesis in infancy.r � 0.39, P � 0.001), and, in the case of alkaline phos- Spain had the second highest consumption of fish in thephate, excluding the cases with �GT �50 U/L, 25-hydroxy- world, but unlike countries in northern Europe, it isvitamin D (� � �0.14; r � 0.14, P � 0.03). generally consumed after being cooked. On the other
hand, dairy products are not fortified with vitamin D inSpain, its consumption is not as high as in other countries,DISCUSSIONand the consumption of polyvitamins is practically non-Although various studies on the Spanish [13–16], Eu-existent. These sociocultural factors could explain that,ropean [7, 9, 17, 18], or Caucasian population [2, 10, 19,when comparing the Europeans, the relationship be-20] have been published, for methodological, geographi-tween the 25-hydroxyvitamin D levels and latitude is thecal, or sociocultural reasons it is not always possible toinverse of that expected by solar radiation [7, 9, 10].extrapolate the results, or the results are incongruous.
The effectiveness of ultraviolet light in the skin synthe-Our study has the advantage of being a population-sis of vitamin D has been demonstrated in a similar waybased sample of both sexes, which includes the linksto the oral administration of vitamin D even in elderlybetween vitamin D and PTH and bone remodeling mark-patients [22]. But it has also been observed that, in pa-ers, and took place throughout one year. Subjects ex-tients with high sunlight exposure, the relationship be-cluded for previous treatment for osteoporosis had 50%tween vitamin D intake and 25-hydroxyvitamin D levelshigher mean levels of 25-hydroxyvitamin D than thosediminishes, perhaps due to a catabolism of vitamin Dincluded, probably due to interference from treatment
or the hygienic-dietary habit. caused by solar exposure. The skin’s melanin content,

Gomez-Alonso et al: 25-Hydroxyvitamin D normal levels S-47
which negatively influences the synthesis of vitamin D, people, the concentration of 25-hydroxyvitamin D neces-sary to achieve an adequate PTH level for a youngercan also contribute to conditioning lower levels of 25-
hydroxyvitamin D in black Americans [23], or in the population would be 40 ng/mL [6].With all of these considerations the results of our studyArab Mediterranean population [24], as in the southern
European population [2, 10], accentuating the nutritional indicate that the most appropriate 25-hydroxyvitamin Dlevels for our population at any time of year should bedeficits.
In our study, the percentage of the subjects with a 25- higher than 30 ng/mL. In our population above the ageof 55 years, the percentage of the vitamin D deficit usinghydroxyvitamin D deficit (�10 ng/mL) was between 30%
and 40%, in all age groups in the winter period. The the aforementioned cut-off point is above 90% in themost favorable period. This fact underlines the need todifferent recovery capacity in summer was notable.
While the deficiency prevalence decreased by a third in modify the dietary-hygienic habits of our population,or even recommend a policy of supplementation withthose aged younger than 75, in subjects older than 75,
there were no seasonal differences, suggesting a greater certain foods with vitamin D, as has been happening inother countries.capacity for skin synthesis in younger subjects and proba-
bly a lesser variation in the elder subject’s exposition tothe sun. The prevalence of the 25-hydroxyvitamin D ACKNOWLEDGMENTSdeficiency in aged subjects was similar to that which was Thanks to Daniel Alvarez Hernandez and Francesca Pieraccini for
their assistance in the preparation of this manuscript, and to BIOMEDfound in a previous population-based study [10] and lessand FIS for their economical support of the EVOS-EPOS study.than the elderly people with hip fractures [25].
The prevalence of secondary hyperparathyroidism was Reprint requests to Carlos Gomez Alonso, Servicio de MetabolismoOseo y Mineral, Instituto Reina Sofıa de Investigacion, Hospital Centralsimilar to that found in another study [23], and increasedde Asturias, C/Julian Claverıa s/n, 33006 Oviedo, Spain.with age, most likely due to the deterioration of renalE-mail: [email protected]
function and the decrease of the 25-hydroxyvitamin Dlevels. The relationship found between 25-hydroxyvi-
REFERENCEStamin D and PTH was similar to that found in other
1. Bouillon R, Carmeliet G, Daci E, et al: Vitamin D metabolismstudies with normal renal function [10, 16] or chronicand action. Osteoporos Int 8(Suppl 2):S13–19, 1998
hemodialysis [26]. 2. McKenna MJ: Differences in vitamin D status between countriesin young adults and the elderly. Am J Med 93:69–77, 1992In our study, serum creatinine and the substrate levels
3. Vieth R: Problems with direct 25-hydroxyvitamin D assays, and(25-hydroxyvitamin D) had a comparable influence onthe target amount of vitamin D nutrition desirable for patients
the PTH levels. The studies carried out on young people with osteoporosis. Osteoporos Int 11:635–636, 20004. Lips P, Chapuy MC, Dawson-Hughes B, et al: An internationalshowed the influence of renal function would be minimal
comparison of serum 25-hydroxyvitamin D measurements. Osteo-and the 25-hydroxyvitamin D references values for anporos Int 9:394–397, 1999
adequate regulation of PTH would be those that are 5. Vieth R: Vitamin D supplementation, 25-hydroxyvitamin D con-centrations, and safety. Am J Clin Nutr 69:842–856, 1999currently used. In our own aged subjects (those with
6. McKenna MJ, Freaney R. Secondary hyperparathyroidism in theexcellent renal function), there were no cases of hyper-elderly: Means to defining hypovitaminosis D. Osteoporos Int
parathyroidism when 25-hydroxyvitamin D values were 8(Suppl 2):S3–S6, 19987. Scharla SH. Prevalence of subclinical vitamin D deficiency inabove 18 and 10 ng/mL in men and women, respectively.
different European countries. Osteoporos Int 8(Suppl 2):S7–S12,The calcitriol regulation showed the similar behavior1998
of PTH. The analysis of bone remodeling markers dem- 8. Thomas MK, Lloyd-Jones DM, Thadhani RI, et al: Hypovitamin-osis D in medical inpatients. N Engl J Med 338:777–783, 1998onstrated that osteocalcin was conditioned by PTH val-
9. van der Wielen RP, Lowik MR, van den Berg H, et al: Serumues, as has been described in other studies [27], andvitamin D concentrations among elderly people in Europe. Lancet
alkaline phosphatase conditioned by 25-hydroxyvitamin. 346:207–210, 199510. Lips P, Duong T, Oleksik A, et al: A global study of vitamin DLooking at our results, the 25-hydroxyvitamin D val-
status and parathyroid function in postmenopausal women withues which guarantee PTH values below 65 pg/mL areosteoporosis: Baseline data from the multiple outcomes of raloxi-
higher than 30 (99%) or 40 (100%) ng/mL [28]. The 25- fene evaluation clinical trial. J Clin Endocrinol Metab 86:1212–1221, 2001hydroxyvitamin D values which guarantee normal PTH
11. O’Neill TW, Marsden D, Matthis C, et al: Survey response rates:values vary substantially from one study to another,National and regional differences in a European multicentre study
which probably reflects other factors, such as age, diet, of vertebral osteoporosis. J Epidemiol Community Health 49:87–93,1995and renal function. In this manner, values of 44 and 30
12. Gomez C, Naves ML, Barrios Y, et al: Vitamin D receptor geneng/mL in elderly Americans [20], 35 ng/mL in postmeno-polymorphisms, bone mass, bone loss and prevalence of vertebral
pausal women [16], 25 ng/mL in Lebanese women aged fracture: Differences in postmenopausal women and men. Osteop-oros Int 10:175–182, 199940 [24], and up to 12 ng/mL in the elderly French popula-
13. Docio S, Riancho JA, Perez A, et al: Seasonal deficiency of vitamintion would meet the aforementioned condition [29]. Ac-D in children: A potential target for osteoporosis-preventing strate-
cording to the regression between PTH and 25-hydro- gies? J Bone Miner Res 13:544–548, 199814. Aguado P, del Campo MT, Garces MV, et al: Alta prevalenciaxyvitamin D obtained from different studies, in elderly

Gomez-Alonso et al: 25-Hydroxyvitamin D normal levelsS-48
de deficiencia de vitamina D en mujeres posmenopausicas de una 22. Chel VG, Ooms ME, Popp-Snijders C, et al: Ultraviolet irradiationconsulta reumatologica en Madrid. Evaluacion de dos pautas de corrects vitamin D deficiency and suppresses secondary hyperpara-prescripcion de vitamina D. Med Clin (Barc) 14:326–330, 2000 thyroidism in the elderly. J Bone Miner Res 13:1238–1242, 1998
15. Quesada JM, Jans I, Benito P, et al: Vitamin D status of elderly 23. Harris SS, Soteriades E, Dawson-Hughes B: Secondary hyper-people in Spain. Age Ageing 18:392–397, 1989 parathyroidism and bone turnover in elderly blacks and whites. J
16. Mezquita-Raya P, Munoz-Torres M, Luna JD, et al: Relation Clin Endocrinol Metab 86:3801–3804, 2001between vitamin D insufficiency, bone density, and bone metabo- 24. Gannage-Yared MH, Chemali R, Yaacoub N, Halaby G: Hypo-lism in healthy postmenopausal women. J Bone Miner Res 16:1408– vitaminosis D in a sunny country: Relation to lifestyle and bone1415, 2001 markers. J Bone Miner Res 15:1856–1862, 2000
17. Bettica P, Bevilacqua M, Vago T, Norbiato G: High prevalence 25. Martinez ME, del Campo MT, Garcia JA, et al: Concentracionesof hypovitaminosis D among free-living postmenopausal women de vitamina D en pacientes con fractura de cadera en Madrid.referred to an osteoporosis outpatient clinic in northern Italy for Med Clin (Barc) 106:41–44, 1996initial screening. Osteoporos Int 9:226–229, 1999 26. Ghazali A, Fardellone P, Pruna A, et al: Is low plasma 25-
18. Chapuy MC, Preziosi P, Maamer M, et al: Prevalence of vitamin (OH)vitamin D a major risk factor for hyperparathyroidism andD insufficiency in an adult normal population. Osteoporos IntLooser’s zones independent of calcitriol? Kidney Int 55:2169–2177,7:439–443, 1997199919. Sherman SS, Hollis BW, Tobin JD: Vitamin D status and related
27. Brazier M, Kamel S, Maamer M, et al: Markers of bone remodel-parameters in a healthy population: The effects of age, sex, anding in the elderly subject: Effects of vitamin D insufficiency andseason. J Clin Endocrinol Metab 71:405–413, 1990its correction. J Bone Miner Res 10:1753–1761, 199520. Dawson-Hughes B, Harris SS, Dallal GE: Plasma calcidiol,
28. Cannata-Andıa JB, Gomez Alonso C: Vitamin D deficiency: Aseason, and serum parathyroid hormone concentrations in healthyneglected aspect of disturbed calcium metabolism in renal failure.elderly men and women. Am J Clin Nutr 65:67–71, 1997Nephrol Dial Tranpl 17:1–4, 200221. Webb AR, Kline L, Holick MF: Influence of season and latitude
29. Souberbielle JC, Cormier C, Kindermans C, et al: Vitamin Don the cutaneous synthesis of vitamin D3: Exposure to winterstatus and redefining serum parathyroid hormone reference rangesunlight in Boston and Edmonton will not promote vitamin D3
synthesis in human skin. J Clin Endocrinol Metab 67:373–378, 1988 in the elderly. J Clin Endocrinol Metab 86:3086–3090, 2001