Embed Size (px)
Citation preview

LETTER TO THE EDITOR
Vitamin B12 extensive thoracic myelopathy: clinical, radiologicaland prognostic aspects. Two cases report and literature review
Frederico Carvalho de Medeiros • Lucas Alverne Freitas de Albuquerque •
Renata Brant de Souza • Antonio Pereira Gomes Neto •
Paulo Pereira Christo
Received: 30 January 2013 / Accepted: 12 February 2013 / Published online: 7 March 2013
� Springer-Verlag Italia 2013
Abstract The myelopathy caused by vitamin B12 defi-
ciency is known as subacute combined degeneration. It is
rare, but a well known cause of demyelination of the dorsal
columns of the spinal cord. The magnetic resonance
imaging is characterized by an increased signal on
T2-weighted images involving the posterior columns of
cervical and thoracic cord. There have been few cases in
literature with extensive lesions (more than seven levels) of
the thoracic spinal cord. The clinical and radiological
improvements are possible if the replacement of vitamin
B12 is initiated precocious. We present two rare cases of
extensive thoracic myelopathy due to vitamin B12 defi-
ciency. The first is a young woman with complete clinical
recovery and important radiologic improvement after early
treatment. In addition, the second case is an older man with
partial response to the treatment. Those cases illustrate the
importance of considering vitamin B12 deficiency in any
patient, who presents with myelopathy.
Keywords Vitamin B12 � Deficiency � Subacute
combined degeneration � Magnetic resonance imaging �Atrophic gastritis � Extensive myelopathy
Dear Editor,
Vitamin B12 deficiency causes several pathological con-
ditions, including myelopathy, neuropathy and neuropsy-
chiatric disturbance. The specific spinal cord lesion caused
by vitamin B12 deficiency is rare, but a well-known con-
dition called subacute combined degeneration (SCD) [1–3].
There are few cases in literature with extensive thoracic
myelopathy (more than seven segments). We present two
rare cases of extensive thoracic myelopathy due to vitamin
B12 deficiency.
Case report 1
A 39-year-old woman, Afro-American, started a progres-
sive weakness and tingling in lower limbs. After 1 month
of the initial symptoms, she developed ataxic gait, sensitive
level at T8 segment and Romberg sign. Vibration and
proprioception were reduced in lower limbs. Laboratory
tests were remarkable only for macrocytic anemia: hemo-
globin of 7.1 mg/dL; the mean corpuscular volume was
100.0 fl; and decreased vitamin B12 level: 72 pg/ml (nor-
mal range 193–982 pg/ml). The serologic tests for HIV,
HTLV I and II, syphilis, Lyme and the inflammatory and
rheumatologic tests: unremarkable; cerebrospinal fluid:
normal; upper gastrointestinal endoscopy: severe fundic
atrophic gastritis. Magnetic resonance imaging (MRI)
revealed a symmetric and extensive hyperintensive signal
on T2WI at posterior columns from C7–T1 to T3–T11
F. C. de Medeiros (&) � L. A. F. de Albuquerque �R. B. de Souza � A. P. Gomes Neto � P. P. Christo
Department of Neurology and Neurosurgery, Santa Casa de Belo
Horizonte Hospital, Francisco Sales Avenue, number 1111,
4th floor, Belo Horizonte, MG 30150-221, Brazil
e-mail: [email protected]
L. A. F. de Albuquerque
e-mail: [email protected]
R. B. de Souza
e-mail: [email protected]
A. P. Gomes Neto
e-mail: [email protected]
P. P. Christo
e-mail: [email protected]
123
Neurol Sci (2013) 34:1857–1860
DOI 10.1007/s10072-013-1335-7
(Fig. 1a). These findings confirmed the diagnosis of SCD,
and after 3 months of intramuscular replacement of vita-
min B12, the patient presented complete clinical recovery,
and radiological improvement, keeping hyperintensive
signal on T2WI at posterior columns from T3 to T6
(Fig. 1b, c).
Case report 2
A 60-year-old man, Caucasian, stated to feel pain in lower
limbs. After 4 months, he presented paresthesia in hands and
feet. After 6 months since the initial pain, he presented
important limitation to walk. At neurological examination he
presented paraparesis 4?/5?; mild spasticity; sensitive level
at T12 segment; deep tendon reflexes were slightly hyper-
active on lower extremities; ataxic gait and Romberg sign;
Babinski sign was absent. Laboratory tests revealed pancy-
topenia: Hb: 6.6 g/dL, VCM: 115fL, platelets: 83.000 mm3,
white cells: 2,170 mm3. He presented low level of vitamin
B12: 55 pg/mL (normal range 193–982 pg/mL). The sero-
logic tests for HIV, HTLV I/II, syphilis, Lyme and the
inflammatory and rheumatologic tests and serum copper and
serum zinc: unremarkable; cerebrospinal fluid: normal;
upper gastrointestinal endoscopy: moderate chronic active
pangastritis, with gland atrophy. MRI revealed a symmetric
and extensive hyperintensity on T2WI at posterior and lat-
eral columns from T1 to T12 (Fig. 2). These findings con-
firmed the diagnosis of SCD. After 7 months since the first
symptoms, the vitamin B12 reposition was initiated. After
12 months of follow–up, the patient persisted with mild
paresthesia and gait ataxia.
The main symptoms of SCD are paresthesia, weakness,
stiffness, numbness or tingling of the limbs; sensory ataxia
that result in inability to walk in some patients; and
impaired vibration sensation. Babinski sign, and sensitive
level may be present [2–4]. The most consistent MRI
findings is symmetric hyperintensity on T2WI, owing
demyelination involving the dorsal columns, predomi-
nately in the lower cervical and upper thoracic region [1].
At sagittal images: there is a vertically oriented segment,
and at axial images: bilateral paired areas are seen as an
‘‘inverted V’’ or ‘‘inverted rabbit ears’’ [4].
There have been few cases reported in literature with
extensive myelopathy due to vitamin B12 deficiency [1, 2].
Fig. 1 a Thoracic spine MRI—sagittal T2WI image shows hyperin-
tense signal along posterior columns extending from T3 through T11.
Axial T2WI image demonstrates the symmetrical and bilateral lesion,
defined as ‘‘inverted V sign’’ or ‘‘rabbit ear reversed.’’ No evidence of
any compression on spinal cord. b, c Follow-up thoracic spinal
MRI—b sagittal T2WI image and c axial T2WI image obtained
3 months after treatment shows near total resolution of signal
abnormality along posterior columns
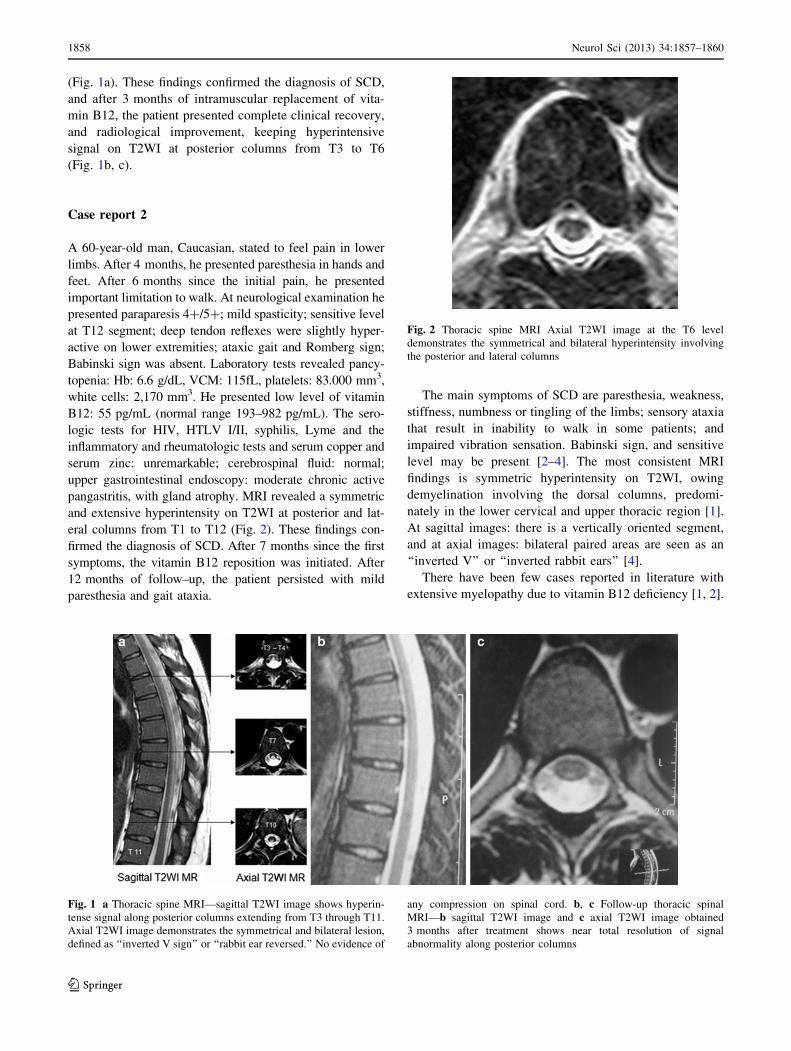
Fig. 2 Thoracic spine MRI Axial T2WI image at the T6 level
demonstrates the symmetrical and bilateral hyperintensity involving
the posterior and lateral columns
1858 Neurol Sci (2013) 34:1857–1860
123

Complete recovery as presented in our first case is even
more rare. In Table 1, we describe the well-documented
cases of extensive myelopathy and complete neurologic
recovery.
Vasconcelos et al. [7] performed a literature review
about SCD from 1968 to 2005. He found a total of 227
patients, but included only 57 well-documented patients.
He defined as extensive myelopathy when more than seven
spinal segments were affected. This cutoff point was
established because he observed that this was an inde-
pendent factor for worst prognosis. In his series, 24
patients presented extensive myelopathy. Only one of it, a
case of Wolansky et al. [5] presented complete clinical
recovery. Vasconcelos et al. [7] highlighted some other
clinical findings that were associated with worse outcome:
sensitive level, Romberg sign and Babinski sign. A factor
of good prognosis observed in this review of Vasconcelos
et al. [7] was age \50.
In our literature review, we found two other cases of
extensive myelopathy and complete neurologic recovery
(Table 1), besides Wolansky et al. [5]. All these cases were
in patients\50 years old, and all patients had the treatment
initiated in the first 4 months of symptoms. One patient
(Makdsi and Kadrie [6]) did not presented any factor of
worst prognosis. In the case of Wolansky et al. [5] (with
Romberg sign) and Rabhi et al. [2] (Babinski sign) at least
one factor was present. In our first case two factors: sensitive
level and Romberg sign were present, nonetheless we also
observed complete clinical recovery. We attribute this sat-
isfactory evolution to the precocity to treatment (1 month).
Our second case with partial treatment improvement pre-
sented multiple factor of unfavorable outcome:[50 years, late
treatment onset, Romberg sign and sensitive level. Those data
support the observation of Vasconcelos et al. [7] that the age
and precocity treatment are important factors to a favorable
prognosis.
Those two cases illustrate the importance of considering
vitamin B12 deficiency in any patient who presents with
myelopathy. The clinical improvement in SCD is related to
the severity of disease (length of myelopathy and symp-
toms), age and the precocity of treatment. Although not
specific for SCD, the MRI findings may be useful in
addition to the clinical assessment in monitoring the effi-
cacy of treatment.
References
1. Vide AT, Marques AM, Costa JD (2012) MRI findings in subacute
combined degeneration of the spinal cord in a patient with
restricted diet. Neurol Sci 33(3):711–713
2. Rabhi S et al (2011) Magnetic resonance imaging findings within
the posterior and lateral columns of the spinal cord extended fromTa
ble
1E
xte
nsi
ve
my
elo
pat
hy
du
eto
vit
amin
B1
2d
efici
ency
wit
hco
mp
lete
clin
ical
reco
ver
yaf
ter
trea
tmen
t
Pct
Au
tho
r(y
ear)
Ag
eS
exS
enso
ry
lev
el
Ro
mb
erg
Bab
insk
iC
ause
of
B1
2
defi
cien
cy
MR
IT
2-w
eig
hte
dT
ime
fro
mfi
rst
sym
pto
ms
to
trea
tmen
t
(mo
nth
s)
Cli
nic
al
imp
rov
emen
t
(mo
nth
s)
Rad
iolo
gic
al
imp
rov
emen
t
(mo
nth
s)
1W
ola
nsk
yet
al.
19
95
[5]
10
MN
oY
esN
oP
ern
icio
us
anem
iaH
igh
sig
nal
wh
ole
cord
0.5
To
tal
(3)
No
foll
ow
up
2M
akd
sian
dK
adri
e2
00
9
[6]
39
MN
oN
oN
oP
ern
icio
us
anem
iaH
igh
sig
nal
C3
–T
82
To
tal
(6)
To
tal
(6)
3R
abh
iet
al.
20
11
[2]
29
FN
oN
oY
esN
ot
iden
tifi
edH
igh
sig
nal
med
ull
ato
T1
1
4T
ota
l(2
)Im
pro
ved
4M
edei
ros
etal
.2
01
3
(th
isp
aper
)
39
FY
esY
esN
oC
hro
nic
atro
ph
ic
gas
trit
is
Hig
hsi
gn
alC
7–
T1
and
T3
–T
11
1T
ota
l(3
)S
lig
ht
hig
h
sig
nal
T3
–T
6(3
)
Pct
pat
ien
t,M
mal
e,F
fem
ale,
MR
Im
agn
etic
reso
nan
ceim
age
Neurol Sci (2013) 34:1857–1860 1859
123

the medulla oblongata to the thoracic spine in a woman with
subacute combined degeneration without hematologic disorders: a
case report and review of the literature. J Med Case Rep 5:166
3. Pittock SJ, Payne TA, Harper CM (2002) Reversible myelopathy
in a 34-year-old man with vitamin B12 deficiency. Mayo Clin Proc
77:291–294
4. Naidich M, Sam H (2005) Subacute combined degeneration.
Radiology 237:101–105
5. Wolansky LJ, Goldstein G, Gozo A, Lee HJ, Sills I, Chatkupt S
(1995) Subacute combined degeneration of the spinal cord: MRI
detection of preferential involvement of the posterior columns in a
child. Pediatr Radiol 25:140–141
6. Makdsi F, Kadrie T (2009) Sub-acute combined degeneration with
an initially normal level of vitamin B12: a case report. Cases J
2:6944
7. Vasconcelos OM, Poehm EH, McCarter RJ, Campbell WW,
Quezado ZM (2006) Potential outcome factors in subacute
combined degeneration: review of observational studies. J Gen
Intern Med 21:1063–1068
1860 Neurol Sci (2013) 34:1857–1860
123