Embed Size (px)
Citation preview
INFECTIOUS MYELOPATHY
DR.SARATH MENON.R, MD(Med.),DNB(Med.),MNAMS
DM RESIDENT,
DEPT. OF NEUROSCIENCES
AIMS,KOCHI.
INTRODUCTION
Infections and secondary inflammatory changes
play an important role
Direct neuronal invasion
Molecular mimicry
Myelopathy- spinal cord dysfunction of any
etiology ,intrinsic or extrinsic
PRESENTATION
Acute transverse myelitis
Acute flaccid paralysis- AHC, motor roots

APPROACH
History & physical examinations
Tempo of illness
Exposure
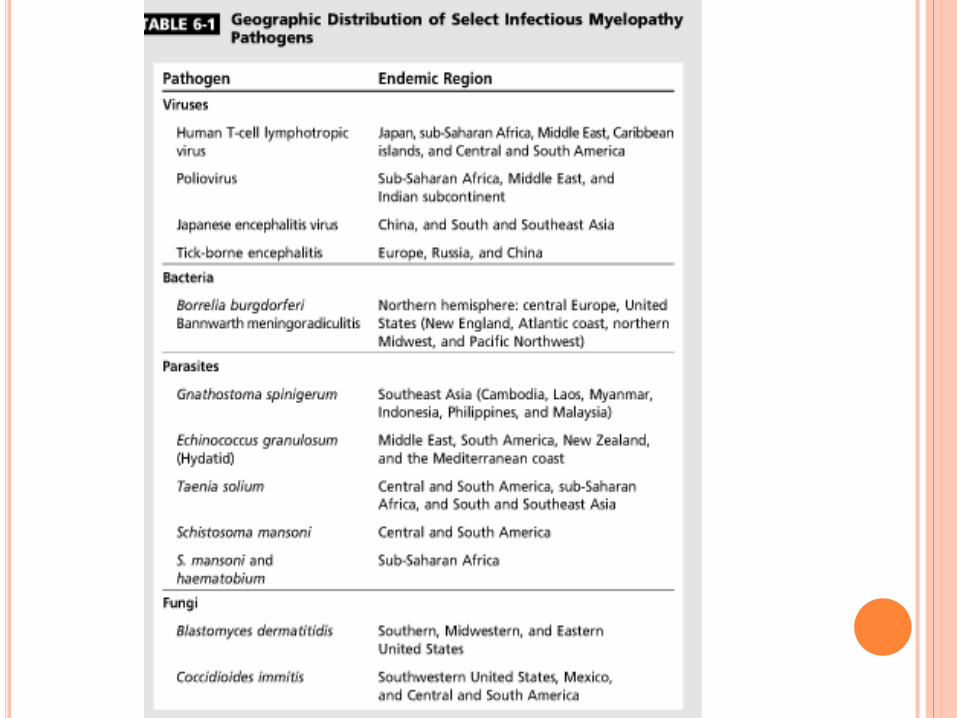
Demographic- endemicity
Host immune status
Ancillary test
Diagnosis & Rx
PARAINFECTIOUS ETIOLOGY
30 -60% infective myelopathy preceeded by
systemic infectious process
Molecular mimicry-
cross reactivity with host antigen in spinal cord
Usually 2-4 wks after infection
Dx- CSF IgG index,OCB
Serology & specific antigen in csf /serum
Rx-
Iv steroid
Refractory cases- IVIG,cyclophosphamide or
rituximab.
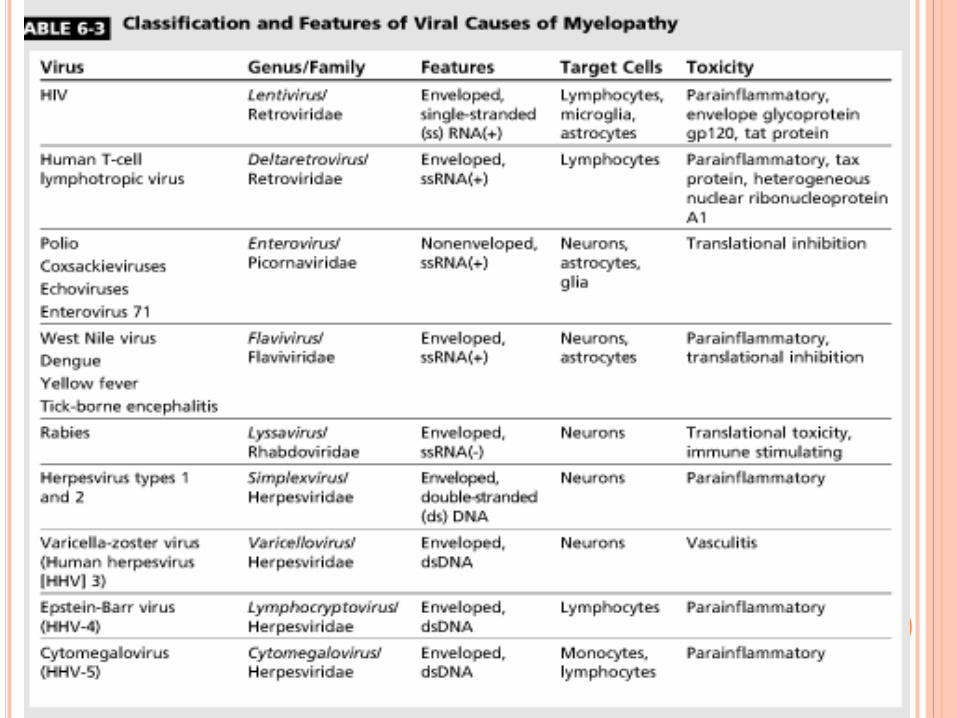
CAUSATIVE AGENTS
Viral
Bacterial
Parasitic
Fungal


RETRO VIRUSES- HIV
CNS – lymphocytes,microglia
Crosses BBB
Neurotoxicity by viral proteins
Chronic pro inflammatory state
CD4 < 200- HIV – vacuolar myelopathy
HIV –VACUOLAR MYELOPATHY
Slow progressive,painless myelopathy
LL weakness,gait difficulties,spasticity,erectile
dysfunction,mild paresthesia
Urge incontinence,urgency- later
Impaired proprioception
LL disproportionately affected.
Diagnosis of exclusion in HIV + pts.
Acute presentation,spinal level ,prominent pain ,UL
prominently involved- alternate diagnosis
D/D- oppurtunistic infection,neoplasms,VB12 def.
Imaging-
Usually normal.
Spinal cord atrophy
Findings similar SACD
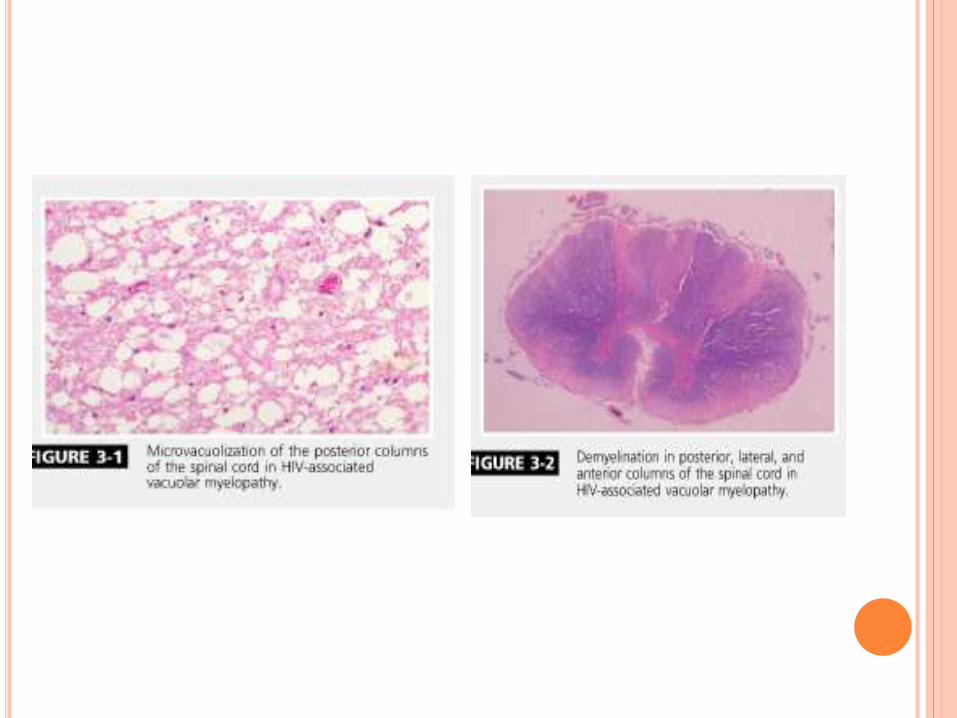
Microscopy-
spongy,vacuolation of myelin
lipid laden macrophages
Rx-
HAART reduced incidence
No response to ART,B12 or IVIG,steroids
13
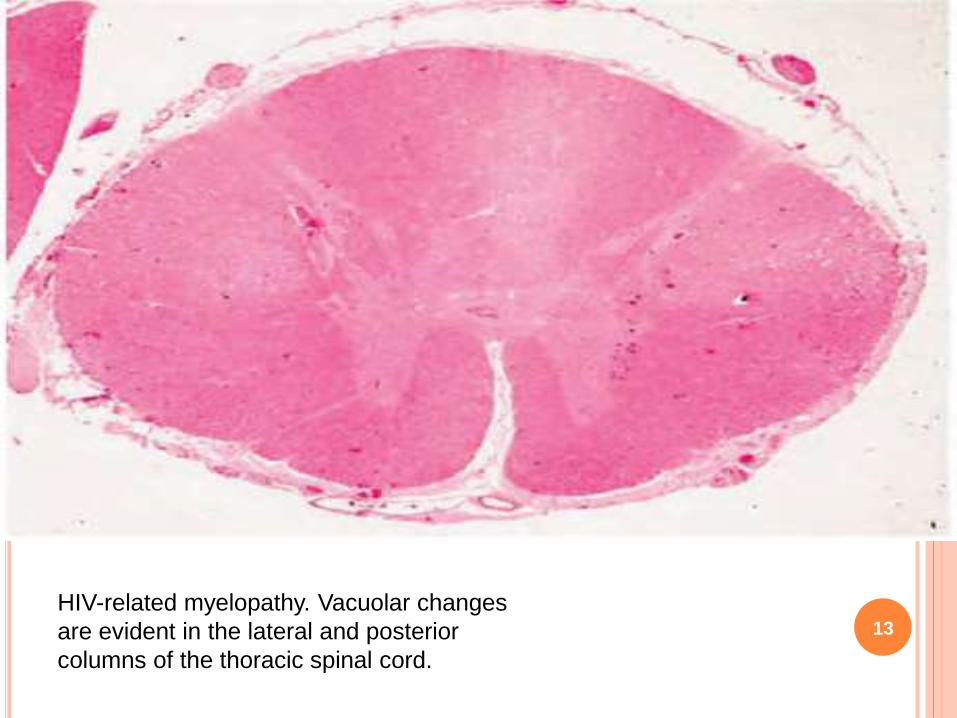
HIV-related myelopathy. Vacuolar changes
are evident in the lateral and posterior
columns of the thoracic spinal cord.

HTLV-1 (HAM/TSP)
4% HTLV-1 will develop
Female predominance
CD8 + Tcell neurotoxicity or molecular mimicry
Clinical features
- insidious ,slow progression
- LL spasticity
- prominent bladder/bowel involvement
- UL weakness insignificant
Diagnosis
- Clinical,demographic,serology
- csf- lymphocytic pleocytosis,OCB+
Confirmation- Western blot
PCR- peripheral blood- distinction & viral load
Imaging
-Focal T2 Hyperintensity in lower cervical cord
-contrast enhancement+
- close d/d to MS
- cervical/thoracic cord atrophy
TREATMENT
No effective clinical trials to date.
Steroids
INF-alpha, cyclosporine,azathioprine- effective
early – limited evidence
HAART
ENTEROVIRUSES
Ubiquitous RNA virus
Produce acute flaccid paralysis
Poliovirus
- AHC affection
- Subsaharan Africa,middle east,Indian subcontinent
- Fever,menigismus,asymmetric flaccid paralysis of LL
proximal > distal over 2 days
- Post polio syndrome
- Slow progressive recrudescence
- Severity of initial disease
ENTEROVIRUS 71- EV 71
AFP similar to polio
Asia –pacific
Children
Fever ,rash – paralysis over 3-5 days
Mri= T2 hyperintensity in lower brainstem,cerebellum
CSF- lymphocytic pleocytosis
No specific rx
IVIG -tried

FLAVIVIRUS- WEST NILE VIRUS
Polio-like paralysis
Mosquito vector
Fever—myelitis—over 2-8 days
Flaccid paralysis, respiratory,bladder +
Risk factor
Age > 50 yrs,immunosuppression
WNV – directly affect AHC
21
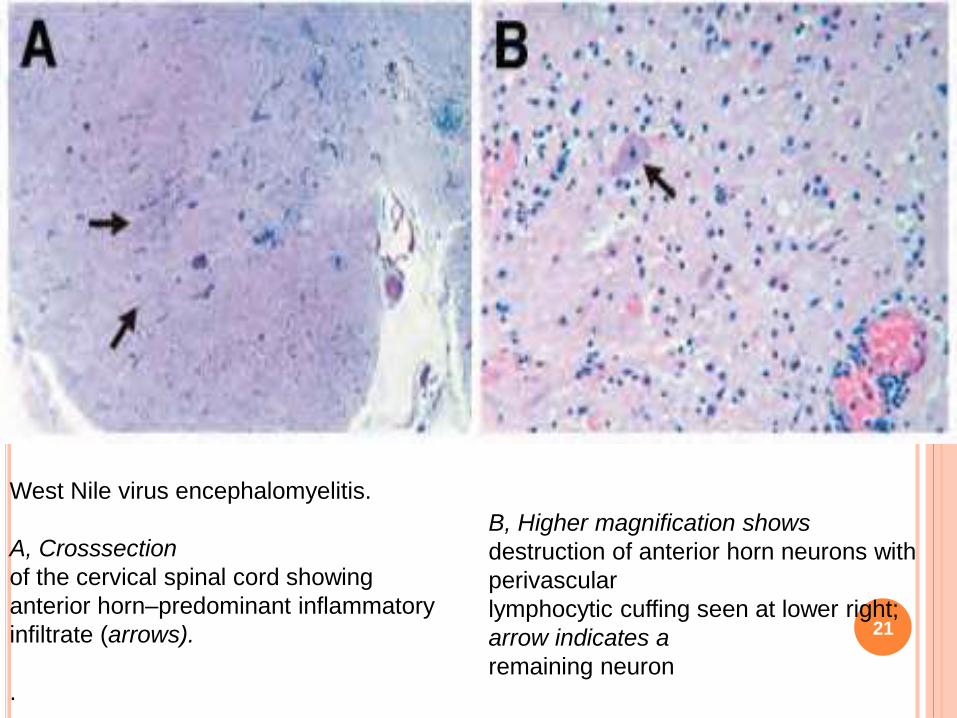
West Nile virus encephalomyelitis.
A, Crosssection
of the cervical spinal cord showing
anterior horn–predominant inflammatory
infiltrate (arrows).
.
B, Higher magnification shows
destruction of anterior horn neurons with
perivascular
lymphocytic cuffing seen at lower right;
arrow indicates a
remaining neuron

Diagnosis
-peripheral leukocytosis,thrombocytopenia,transaminitis
CSF- PMN /mononclear pleocytosis,elev.protein,sug-nl
- IgM –sensitive/specific
- serology
-Spinal cord imaging-normal
- Rx
- Supportive,no specific
- anecdotal- steroids

RABIES
2/3rd –furious/encephalitic,1/3rd –dumb/paralytic
Paralytic-
GBS like presentation—encephalopathy—death
Considered in exposure to animal bite esp.bat
PCR- Skin biopsy from nape of neck-specific
Serology
Virus amplification from skin,saliva,CSF
Supportive rx.
Prophylaxis

HERPES VIRUSES-HSV1&2
HSV1 &2 – myelitis
HSV-2 related myelitis-adults
Elsberg syndrome-reactivation of HSV-2
inflammation in dorsal roots + spinal cord = radiculomyelitis
C/f :
- subacute lower extremity weakness may ascend
- Numbness or tingling in lumbosacral dermatome
- Urinary retention
Acute necrotising myelopathy- severe form seen in
immunocompromised
Flaccid paraplegia+ areflexia
Diagnosis
- CSF-lymphocytic pleocytosis with raised protein
Necrotizing myelitis- PMN leukocytosis
CSF-PCR amplification of DNA
Imaging
- Spinal cord edema
- T2 hyperintensity+CE of radicular roots & cord
Rx
- Iv acyclovir x 14 days f/b oral acyclovir /valacyclovir
- Steroids –role uncertain
- Complete recovery is posssible
- 20% cases,recur

VZV
Myeloradiculitis on reactivation-immunocompromised
Necrotising vasculitis + demyelination
Zoster preceeds, cases with no rash
Asymmetric paraparesis + sensory loss- days to wks
CSF-
Mononuclear pleocytosis ,elevated protein
Anti-VZV IgM assay in CSF-sensitive
PCR- rapid
Imaging- T2 hyperintense in cord = dermatome
Rx
iv acyclovir + steroids
CMV
Imunocompromised- HIV – CD4<100cells/microL
Lumbosacral polyradiculomyelitis-
supf.meningitis-> nerve roots & spinal cord
Necrotizing myelitis
Imaging-
cord edema+root edema+ CE
meningeal thickening+clumping of roots
CSF-
PMN pleocytosis+elev.protein+ low sugar
Rx
IV ganciclovir+ foscarnet
Poor prognosis
EBV
Children / young adults
Immunocompromised –transplant
Spectrum – aseptic meningitis
meningoencephalitis
cranial/peripheral neuritis
GBS & myelitis
Myelitis- 2-3 weeks after primary infection
flaccid paraparesis,sensory level,bladder+
CSF-
mononuclear pleocytosis,elev.protein,sugar-nl
Serology –EBV DNA
CSF-EBV DNA PCR
Imaging-
T2hyperintensity+ce+nerve thickening
Rx
- Acyclovir-little effect on clinical course
- steroids

BACTERIAL- SYPHILIS
Meningovascular-cord infraction-endarteritis-rare
Tabes Dorsalis
Post antibiotic era- less incidence
c/f-
subacute/chronic – sensory ataxia+
loss of vibration,joint position
lancinating pain+
hyperreflexia,charcot joint,AR pupil
Imaging-
cord atrophy
non enhancing T2 hyperintensity-posterior cord
SYPHILIS-OTHER FORMS OF MYELOPATHY
Hypertrophic pachymeningitis
Spinal cord Gumma
AHC
Syingomelia
Aortic aneurysm –sec AHC
Charcot vertebra-cord compression
SYHILITIC MENINGOMYELITIS
Current era, most common spinal cord d/s
Men-25-40 yrs
Avg.6yr after infection
Progressive spastic ,asymmetric paraparesis
Imaging-
T2 hyperintensity central cord +CE

DIAGNOSIS & RX
Peripheral serology+ CSF evaluation
VDRL & RPR- sensitive in early
TP-FAB- specific
CSF- mild inflammatory
- VDRL,FAB
Rx
Inj.Penicillin aqueous -12-24 mu q4h x 10-14 days
Jarisch-Herxheimer reaction
(iv steriods-premptively)
LYME DISEASE
Ixodes tick-endemic North America,Europe,Asia
Erythema migricans-initial lesion
Classic triad- facial palsy,aseptic meningitis,painful
radiculitis
Bannworth synd.-acute transverse myelitis-painful
Chronic,progressive myelopathy- other form
Diagnosis
-clinical history
-ELISA/Western blot
-CSf- Lyme specific IgM
-MRI- T2 hyperintensity+CE-root,meninges
Rx-
IV Ceftriaxone-14-28 days+ steroids
TUBERCULOSIS
MC myelopathy- Pott’s disease
Vertebral venous system
Anterior segment of thoracic & lumbar spine-collapse
Other forms-
- intramedullary/intradural tuberculomas-
(S/A myelopathic symptoms).
- granulomatous myeloradiculitis-
(rapid progressive rad.pain,paresthesia,flaccid
weakness,babinski+ ,bladder+)
- spinal artery vasculitis+ cord infarction
- ADEM
- Cord compression- vertebre,granulating tissue
DIAGNOSIS
CSF- lymphocytic pleocytosis,low sugar,very high protein
AFB,TB cultures
Mantaux test- + in 40%
MRI (Pott’s)–T1 hypo +T2 hyper +CE
Vertebre collapse+ cord compression
Granulomatous myeloradiculitis-
CE+ meningeal thickening +spinal roots
Tuberculomas-
CE+ T1 hypointense ring +T2 hyperintense central

RX
2 month HRZE/S+ 7-10 Month HR
Vertebral disease- surgical option
Lumbar disease-better prognosis

PYOGENIC BACTERIA
Vertebral osteomyelitis- collapse+ epidural abscess
Intramedullary abscess- hematogenous seeding+
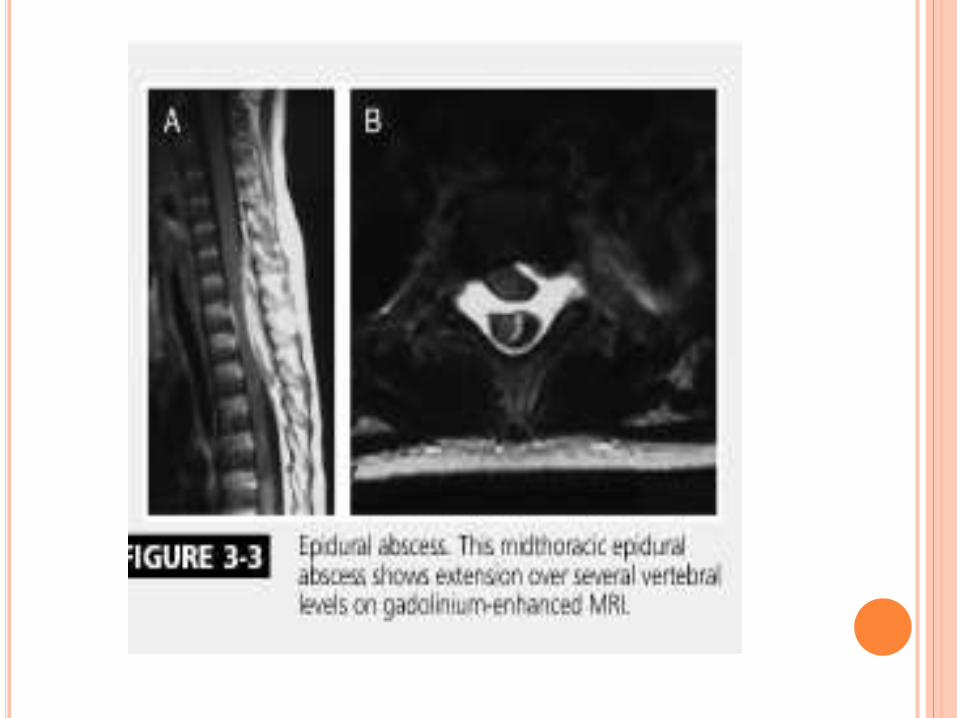
Epidural abscess
- osteomyelitis- hematogenous
- Local soft tissue,viscera,instrumentation ant.epidural
- Direct seeding- post.epidural
- Risk factors+
- Thoracic +
C/F-
- Focal back pain+ muscle spasms
- Fever
- MC- S.aureus > Streptococcus > GNB
Diagnosis-
ESR,CRP
Blood culture-+ 60%
Imaging
LP –contraindicated
Rx
- Drainage
- Iv antibiotics

OTHER BACTERIAL MYELOPATHY
Bartonella- myelitis & Brown –Sequard syndrome
Whipple disease-
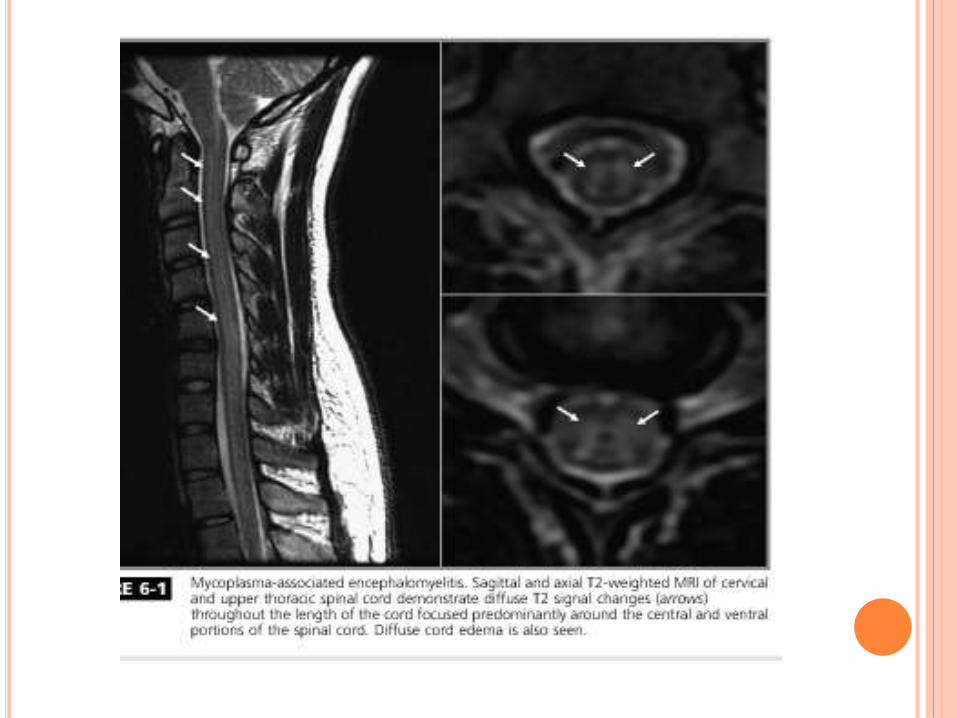
Parainfectious-
Mycoplasma
Pertussis
PARASITIC MYELOPATHIES
Schistosomiasis
Central America & Africa
Retrograde migration of eggs ffrom portal system to
epidural venous plexus
Subacute- low back ache- paraparesis-sensory level-
bladder/bowel++
T11 –L1 & Cauda equina
MRI-
-Cord enlargement
- intramedullary T2 hyperintensity
- lower thoracolumbar cord,conus,cauda CE
DIAGNOSIS
3 features
-Lower spinal cord or cauda
-Evidence of infection(ova in stool/urine,rectal
biopsy,serology)
-Exclusion of other causes
Peripheral Serology- ELISA,IF
CSF tests specific- Monoclonal antibodies or PCR
Tissue biopsy- gold standard
(avoided in CNS disease).

RX
Praziquantel
Concurrent steroids
Rarely, decompression- medically refractory
OTHER PARASITES
Toxoplasma gondii-
-Advanced HIV
-Parenchymal + spinal cord mass lesions
-Peripheral IgG+
- CSF-PCR(spf)
Rx-
pyrimethamine + sulfadiazine /clindamycin
folinic acid
NEUROCYSTICERCOSIS
1.2 %-5.8% cases involve spinal cord
Subarachnoid
Subarachnoid cysts migrate from basal cisterns
75% cases – intracranial NC
Csf- high proten + eosinophilia
Rx
- albendazole + steroids
- rarely,decompression.

HYDATID CYST-ECHINOCOCCUS
Spinal rare
Vertebrae,extradural or paraspinal
Cysts in other sites+
Large- mass effect,bony destruction,inflammatory
response
Imaging-cysts
Serology
Rx-
albendazole
surgical
Recurrence- norm
OTHER PARASITES
Gnathostoma spinigerum
Angiostrongylus cantonensis

FUNGAL CAUSES
Immunocompromised
Aspergillus,cryptococcus
Spinal myelopathy
- epidural abscess
- c/c arachnoiditis
- intramedullary granulomas
- frank myelitis
- vasculitis + cord infarction.



APPROACH
Clinical –
- Onset- Acute vs Subacute Vs Chronic
- Progression
- Painful vs painless
- Sensory level
- Bladder/Bowel+
CSF analysis
Imaging

ACUTE FLACCID PARALYSIS
Polio
Enteroviruses
West NileV
Leukomyelitis-(Acute)
Herpes
CMV
Borellia- rare
EBV
Rabies
LEUKOMYELITIS (SUBACUTE-CHRONIC)
Treponema
Mycoplasma
Tuberculosis
HIV/HTLV-1

Thank you