Virtually Possible: The Use of Technology in the Treatment Of
Diabetes
Virtually Possible: The Use of Technology in the Treatment Of
DiabetesCheryl B. Masters, PhD, Jerry Nymberg, MD, Mark Robinson,
MD, Andrea Cochran, PhD, Wes Teeter, MA, LPCCabarrus Family
MedicineCarolinas Healthcare System
Collaborative Family Healthcare Association 15th Annual
ConferenceOctober 10-12, 2013 Broomfield, Colorado U.S.A.
Session #B5b Saturday, October 12, 2013Collaborative Family
Healthcare Association 12th Annual ConferenceFaculty Disclosure We
have not had any relevant financial relationships during the past
12 months.
CFHA requires that your presentation be FREE FROM COMMERCIAL
BIAS. Educational materials that are a part of a continuing
education activity such as slides, abstracts and handouts CANNOT
contain any advertising or productgroup message.
The content or format of a continuing education activity or its
related materials must promote improvements or quality in health
care and not a specific propriety business interest of a commercial
interest.
Presentations must give a balanced view of therapeutic options.
Use of generic names will contribute to this impartiality. If the
educational material or content includes trade names, where
available trade names for products of multiple commercial entities
should be used, not just trade names from a single commercial
entity. Faculty must be responsible for the scientific integrity of
their presentations. Any information regarding commercial
products/services must be based on scientific (evidencebased)
methods generally accepted by the medical community.
Collaborative Family Healthcare Association 12th Annual
ConferenceStudy SummaryStudy question: Will video-enhanced home
monitoring devices increase patient access (and improve outcomes)
to a diabetes care team embedded in a patient centered medical
home?Study population: Total enrollment of 119 poorly-controlled
diabetic patients (HbA1c > 9%)Study sites: CFM-Kannapolis,
CFM-ConcordStudy duration: 3 month intervention and 3 month
follow-upDiabetes Care Team: care manager, nutritionist, clinical
psychologist, and clinical pharmacist3 Baseline
DataConcordKannapolis 2012 DataConcordKannapolisNumber of Active
Patients 13, 1059, 579Office Visits35, 08327, 347MDs (n)95ACPs
(n)22Residents (n)66NCQA PCMH Level 33Total Diabetics (n)1069908%
of A1c > 911.1 %11.1%4Frequently Cited Barriers To Glycemic
ControlTransportationFinancial resourcesMood disordersLimited
knowledge about diabetes
Gatchel & Dordt (2003) Clinical Health Psychology and
Primary Care5ObjectivesParticipants will identify the relationship
between mood, stress and diabetes.Participants will describe the
prominent psychosocial obstacles to diabetes
management.Participants will identify the advantages of virtual
services as a platform for diabetes management.
Include the behavioral learning objectives for this
sessionCollaborative Family Healthcare Association 12th Annual
ConferencePatients Randomized to Three GroupsGroup 1Group 2Group
3Usual care from PCPNo cost to access diabetes care teamNo care
managerUsual care from PCP Care managerNo cost access diabetes care
teamCare manager coordination of diabetes care team servicesUsual
care from PCP Care managerVirtual access to diabetes care team
using video-enhanced home monitoring devicesFace Time via
iPadHoneywell home monitor transmissions of glucose, BP and
weight
7 Baseline DemographicsGroup 1Group 2Group 3 N413940Age
(mean)48.650.951.6Female %59%67%45% Race:WhiteAfrican
AmericanLatino281212514031908Group 1Group 2Group 3A1c11.210.911.3SD
for A1c1.61.31.9Glucose (Office)246270231Weight
(male)255234221Weight (female)221203213Total
Cholesterol190202175Triglycerides271258226Baseline Glycemic Control
Mean by Group9DID Virtual Technology Improve Access?Changes in
Access to the Team Patients Seen Before the Study Patients Seen
During the Study
At least one visit to nutritionist 47 81At least one visit to
pharmacist 23 77At least on visit to behaviorist 2 5611Number of
Visits with all DCT Disciplines by 3 MonthsDisciplineGroup 1Group
2Group 3Pharm, Nutr, and Behav521 21 *CM, Pharm, Nutr, Behav2817CM,
Pharm, and Nutr71220* Main study outcome Note: 100% saw their PCP
at study entry
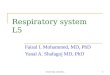
Visits by Discipline After 3 Months(FT is the number of FaceTime
Visits)
(41 FT)(52 FT)(46 FT)(12 FT)Did Technology Improve Glycemic
Control?
Improvements in Glycemic Control
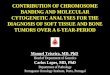
15Was Depression or Stress Related to Diabetes?
What Percentage of Patients Screened Positive for
Depression?
35%32%17Did PHQ-9 Scores Improve with Treatment?18Top 10
Stressors (Holmes & Rahe)ChristmasPersonal injury/illnessChange
in financial stateChange in eating habitsChange in health of family
memberDeath of close family memberSexual difficultiesChange in
social activitiesChange in sleeping habitsDeath of close
friend19Holmes & Raye by GroupHolmes &Raye Group 1 Group 2
Group 3Total ScoreMean
(standarddeviation) 89.46
(95.38) 123.69
(134.70) 102.70
(96.96)Score