Embed Size (px)
Citation preview
Tendon injuriesTendon injuries
Robert Spławski MD, PhDPaweł Surdziel MD, PhDRobert Spławski MD, PhDPaweł Surdziel MD, PhD
Department of Traumatology and Hand SurgeryDepartment of Traumatology and Hand Surgery
University of Medical SciencesUniversity of Medical Sciences in Poznan in PoznanUniversity of Medical SciencesUniversity of Medical Sciences in Poznan in Poznan
Head of Department:Head of Department:Prof. Władysław ManikowskiProf. Władysław ManikowskiHead of Department:Head of Department:Prof. Władysław ManikowskiProf. Władysław Manikowski
Historical notesHistorical notes
Tendon surgery is as old as surgery Tendon surgery is as old as surgery itselfitself
2698 BC – Yu-Fu2698 BC – Yu-Fu460460BC – HippocratesBC – Hippocrates280 BC – Herophilos 280 BC – Herophilos fromfrom Chalkedon Chalkedon129-199 – Galen129-199 – Galen980-1037 – Avicenna980-1037 – Avicenna1641- Ambrosius Pare1641- Ambrosius Pare1880 - Nikoladoni1880 - Nikoladoni1881 – Gluck1881 – Gluck1882 – Henck1882 – Henck
Historical notesHistorical notes
Historical notesHistorical notes
Hippocrates – if injury of Achilles tendon occurHippocrates – if injury of Achilles tendon occurs it would s it would cause acute fever, convulsins etc.cause acute fever, convulsins etc.Avicenna - tenth century strongly advocated tendon sutureAvicenna - tenth century strongly advocated tendon sutureWorld War I and II stimulated the development of modern World War I and II stimulated the development of modern hand hand surgerysurgery
Tendon Tendon cconsistonsistss of : of :• Cells – fobroblastsCells – fobroblasts• Extracellular matrixExtracellular matrix mainly collagen fibers, mainly collagen fibers, elastinelastin fibers fibers ground substance ground substance (proteoglicans, glycosaminoglycans, (proteoglicans, glycosaminoglycans,
structural proteins, plasma proteins and other small molecules)structural proteins, plasma proteins and other small molecules)
CollagenCollagen
typI – composed of three chains typI – composed of three chains 70% glicine, 15% proline and 15% hydroxyproline70% glicine, 15% proline and 15% hydroxyproline
Collagen molecules are combined in a right-handed tripleCollagen molecules are combined in a right-handed triplehelix. helix. The sThe stabilisation between helixs tabilisation between helixs is maintain is maintain by by hydrogens bonds.hydrogens bonds.
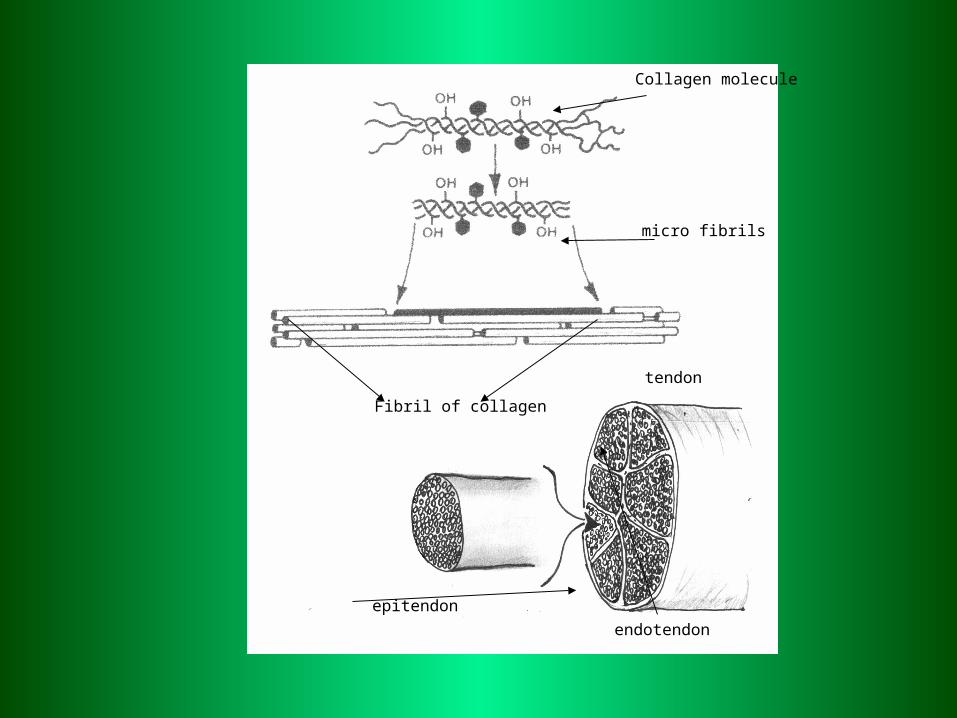
Collagen molecule
micro fibrils
Fibril of collagen
tendon
epitendon
endotendon
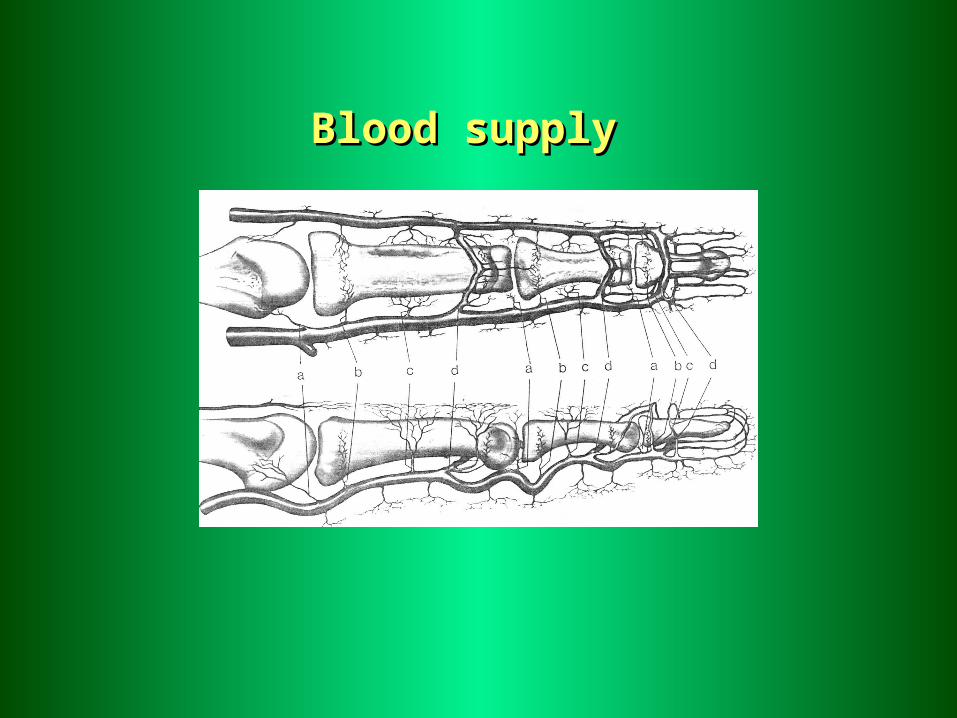
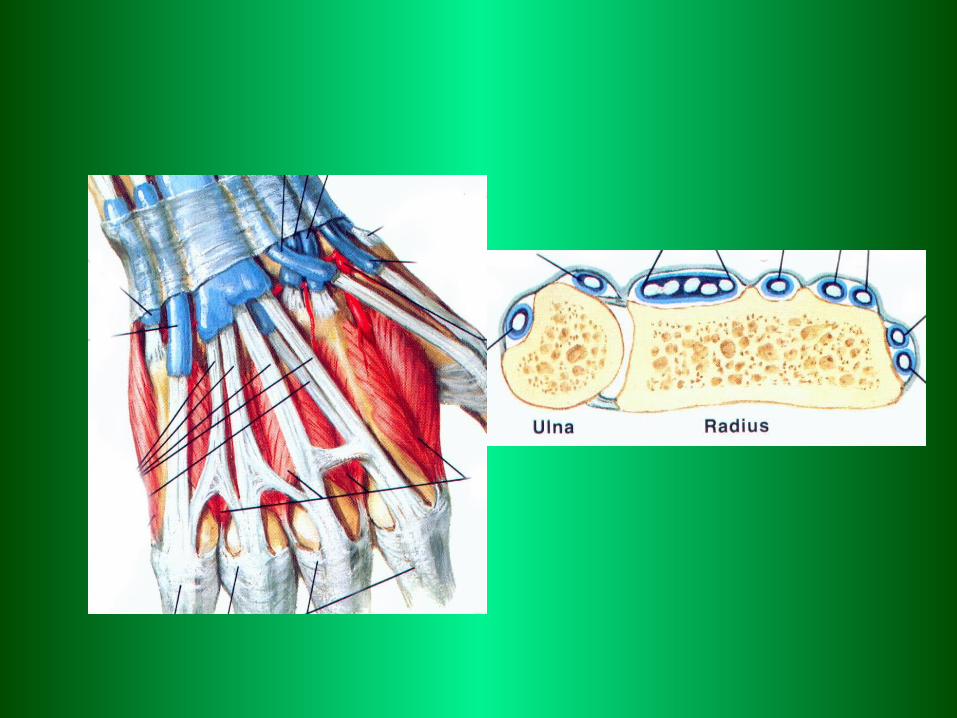
Blood supplyBlood supply
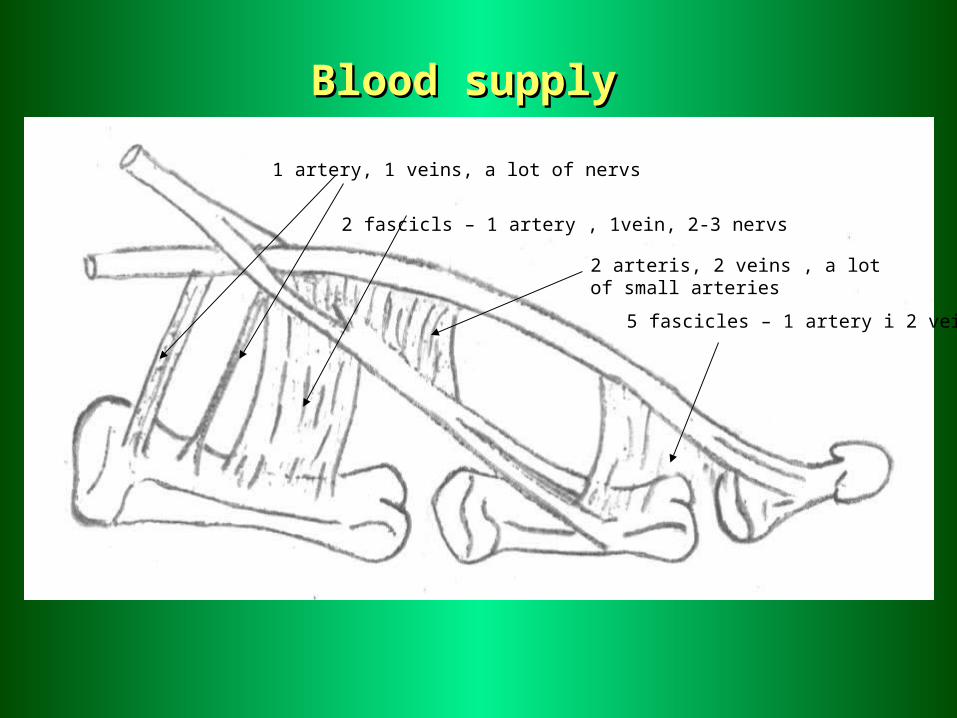
1 artery, 1 veins, a lot of nervs
2 fascicls – 1 artery , 1vein, 2-3 nervs
2 arteris, 2 veins , a lot of small arteries
5 fascicles – 1 artery i 2 veins
Blood supplyBlood supply
Blood supplyBlood supply
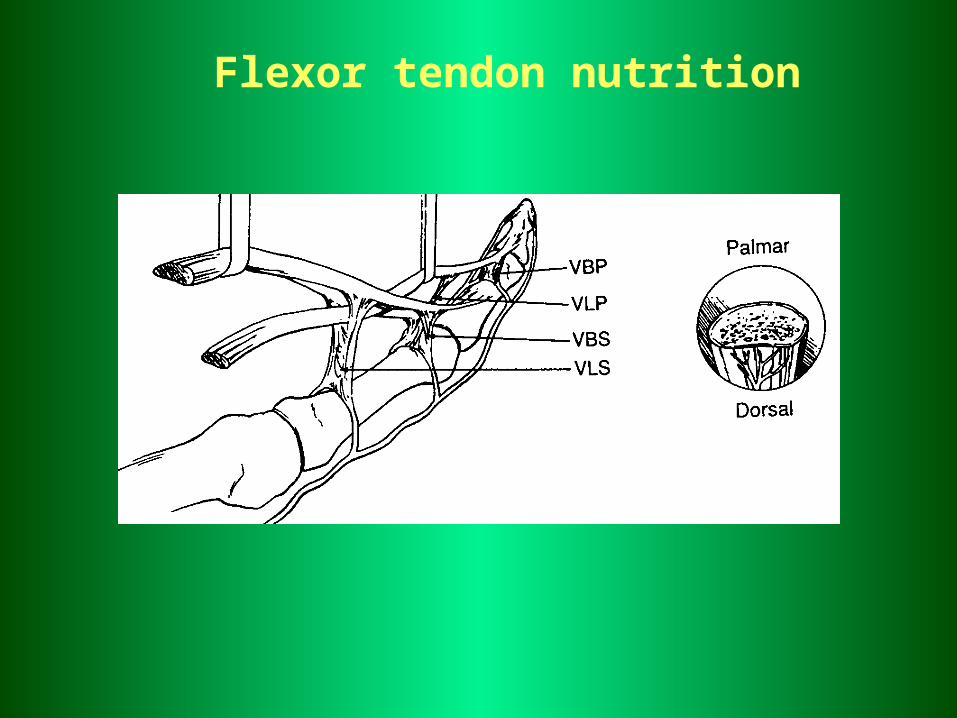
Flexor tendon nutrition
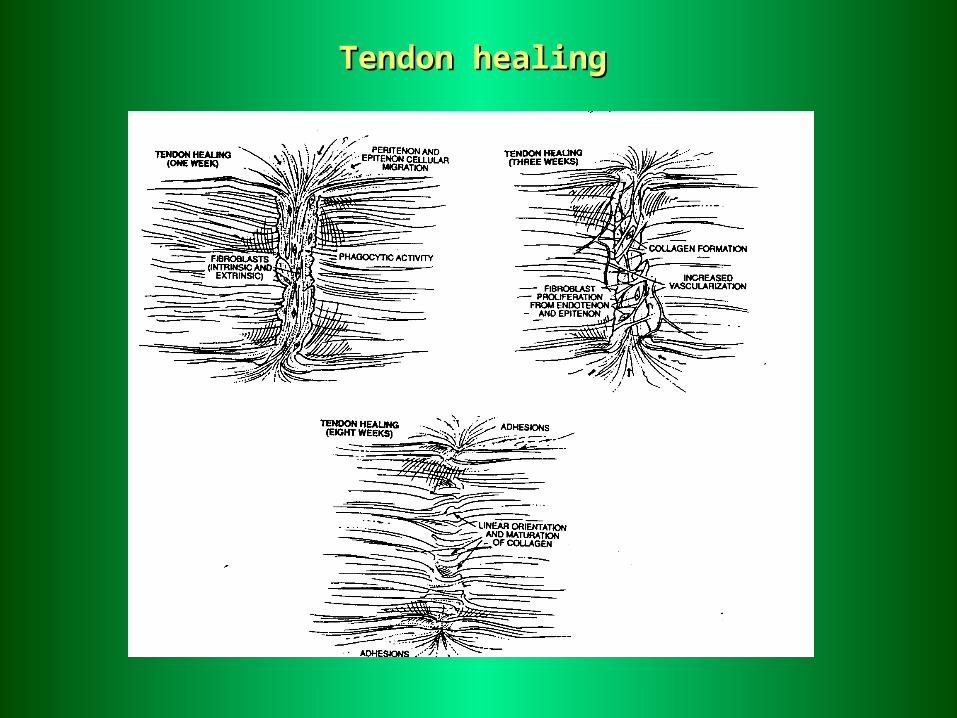
Tendon healingTendon healing
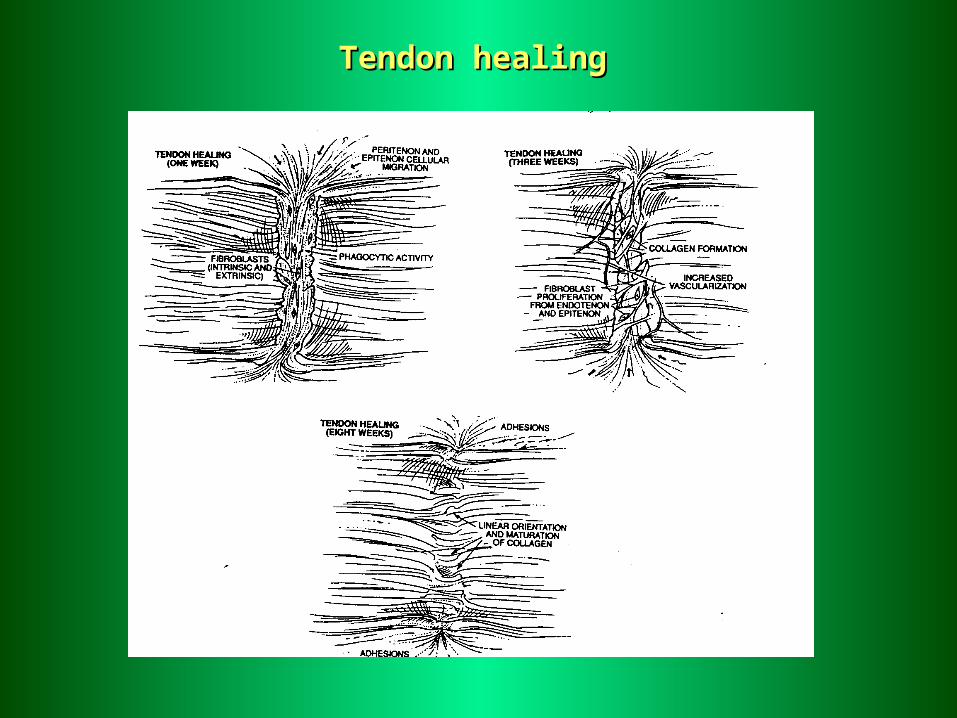
Tendon healingTendon healing
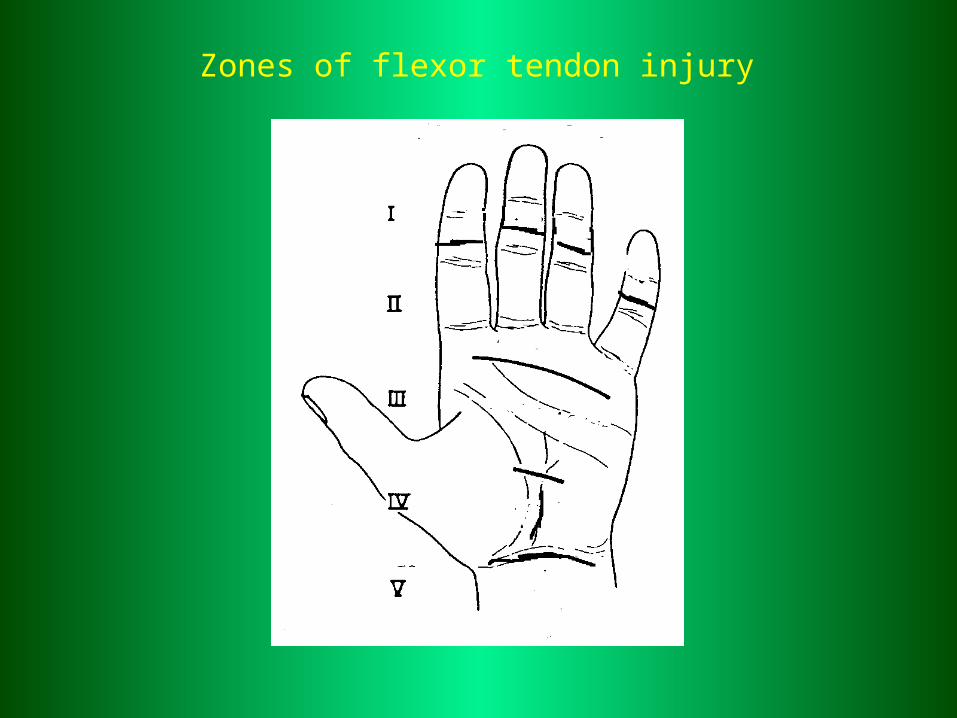
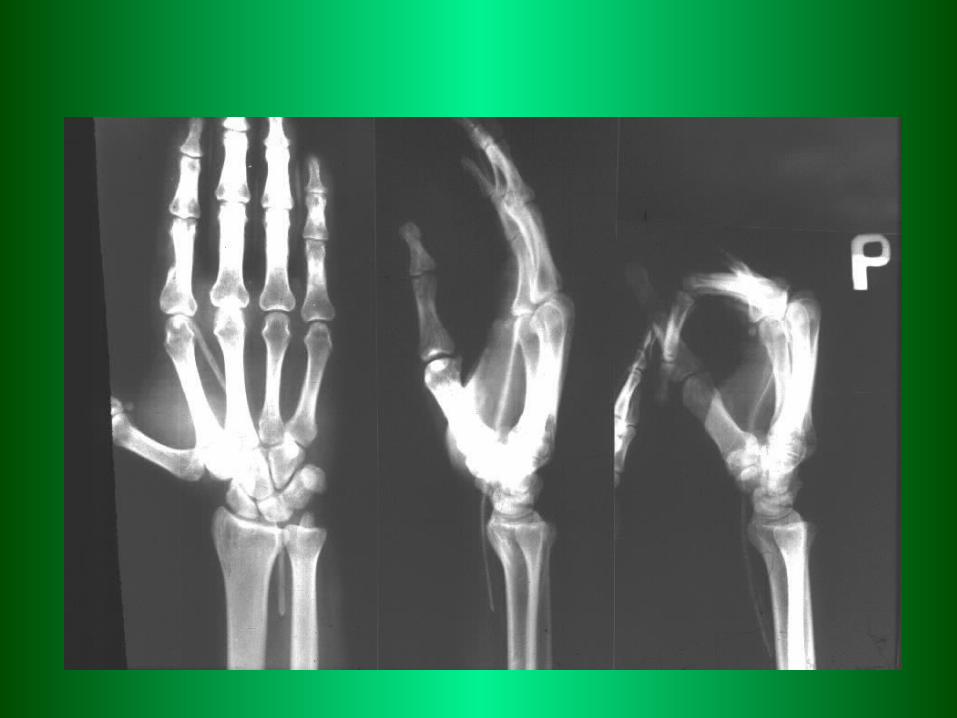
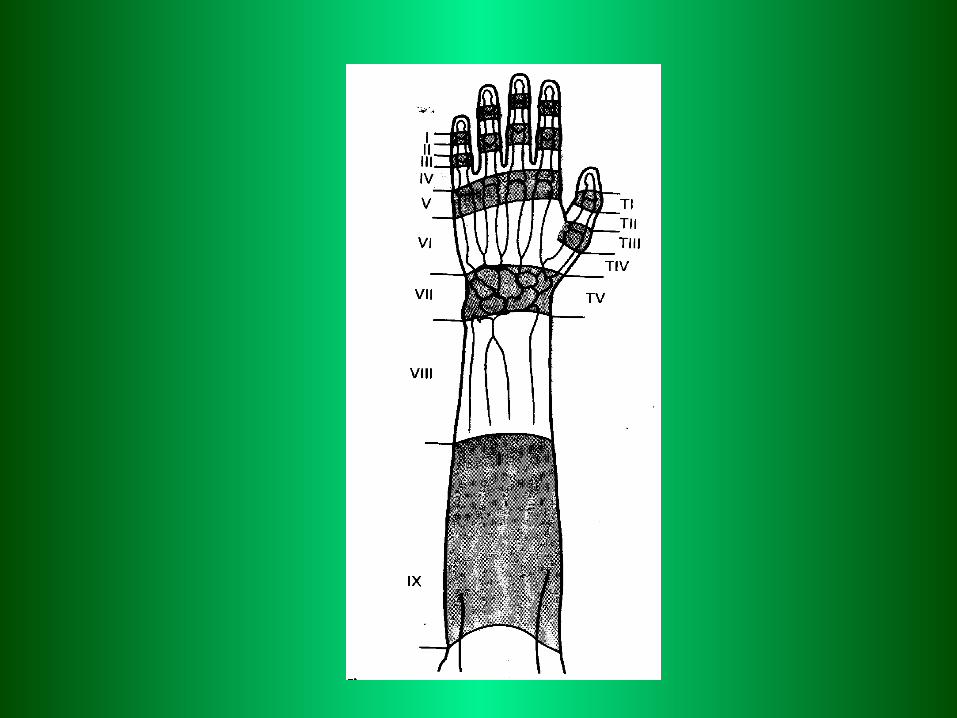
Zones of flexor tendon injury
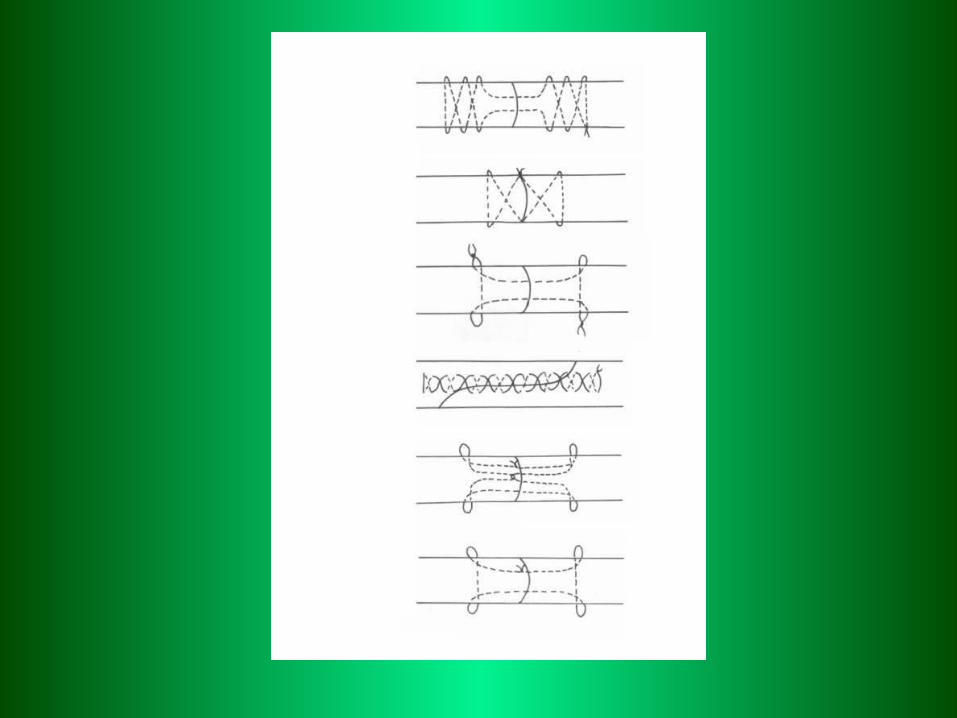
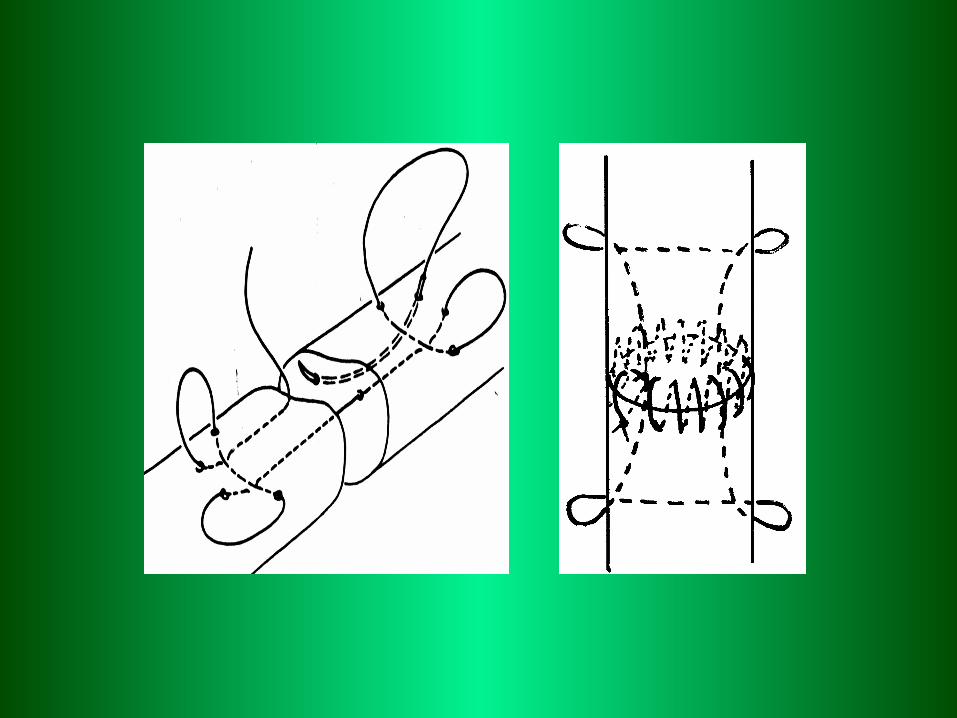
Primary flexor tendon suturePrimary flexor tendon sutureDelayed flexor tendon sutureDelayed flexor tendon suture
Secondary repair /late reconstruction/Secondary repair /late reconstruction/- - one stage tendon reconstructionone stage tendon reconstruction- - two stage tendon reconstructiontwo stage tendon reconstruction
TreatmentTreatment
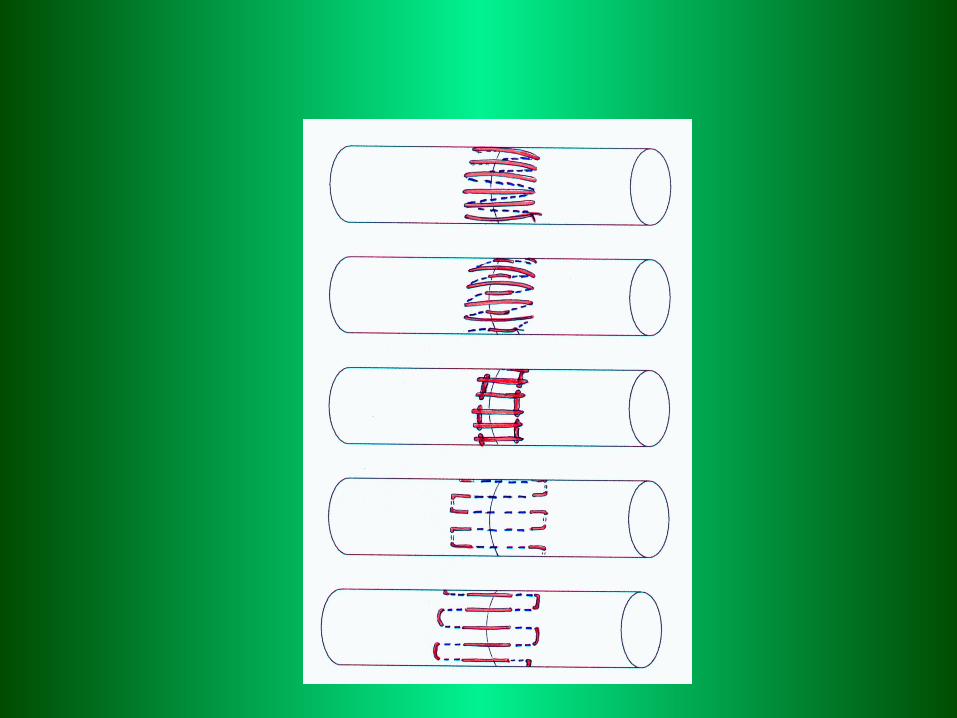
Zone I Reinsertion after avilsion injuryReinsertion after avilsion injuryEnd to end sutureEnd to end suture
Zone II End to end sutureEnd to end suture
Zone III End to end sutureEnd to end suture
TreatmentTreatment
1.1. Active extension-Active extension-ppassive flexion assive flexion Kleinert Kleinert method method ooff rehabilitation rehabilitation
2.2. Controlled passive motion -Controlled passive motion -Duran-HouserDuran-Houser method method /active motion after 5 weeks//active motion after 5 weeks/
3.3. Controlled active motion methodControlled active motion method..
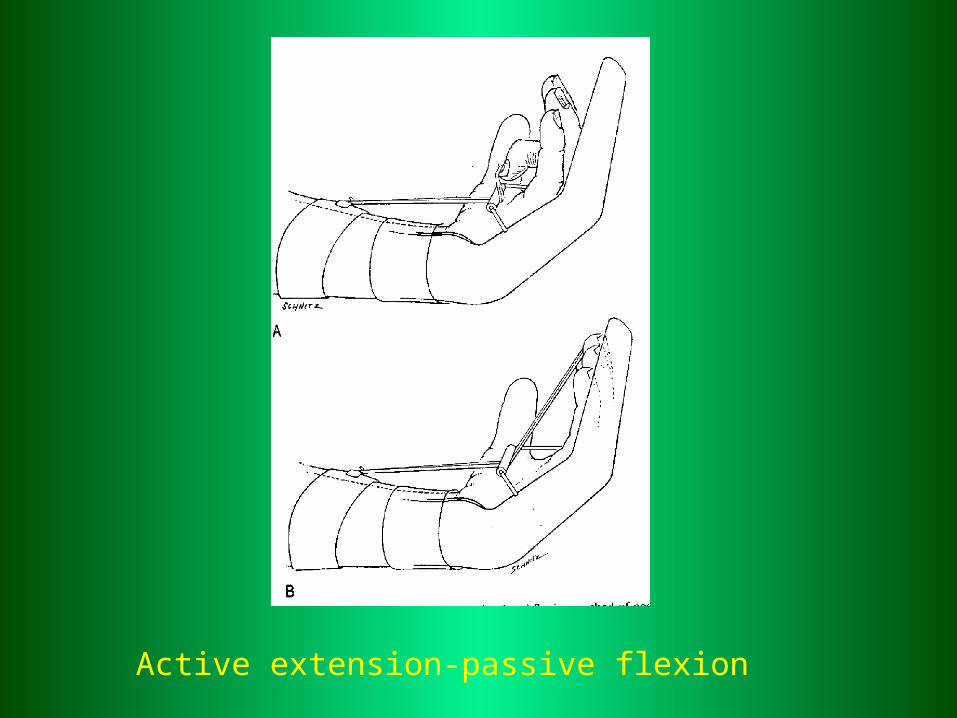
Active extension-passive flexion

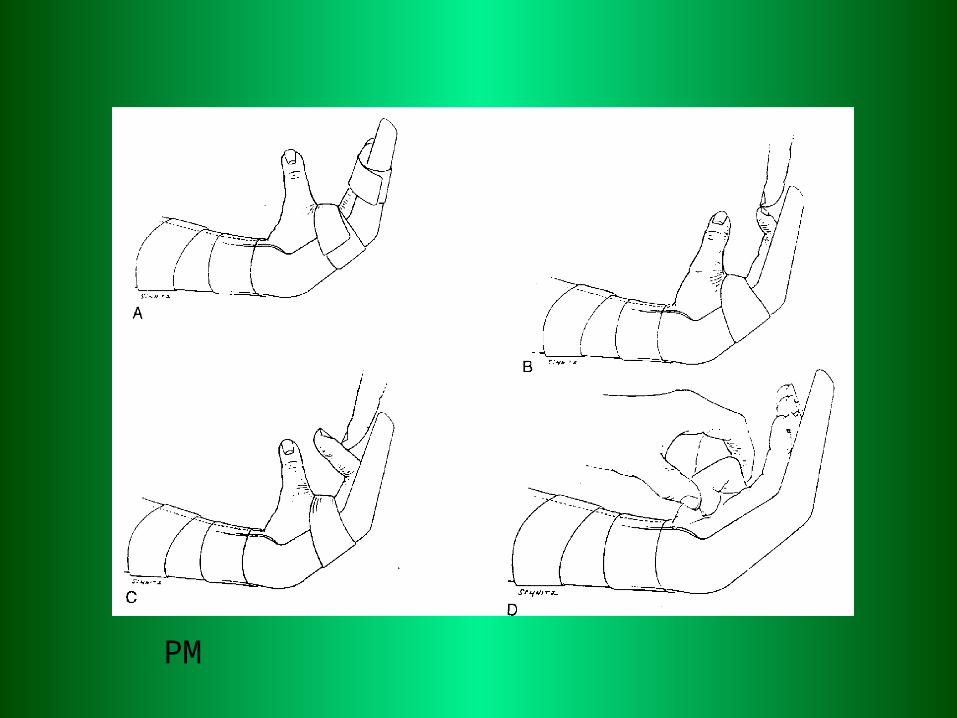
PM
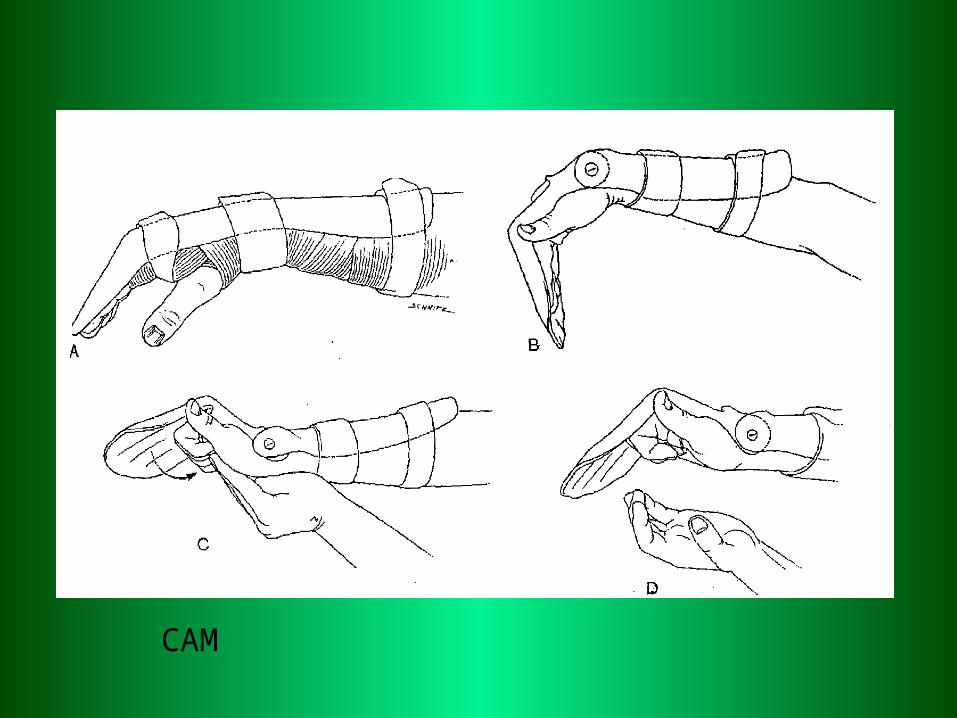
CAM
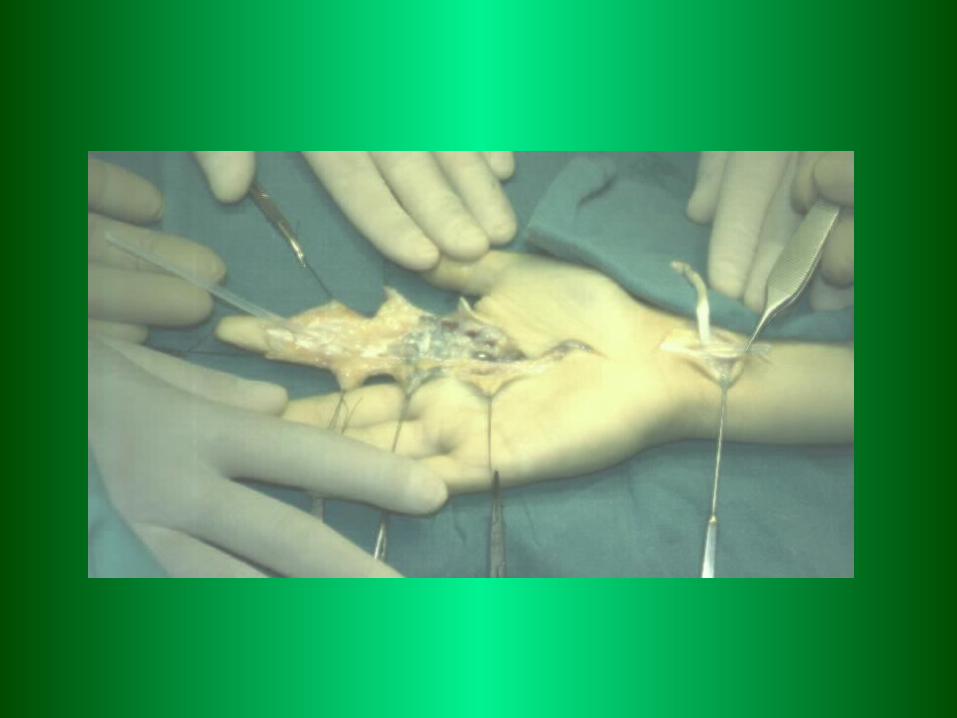
Tendon reconstructionTendon reconstruction
Primary end to end tendon suture. To 3-4 weeks.Primary end to end tendon suture. To 3-4 weeks.Secondary - staged techniquesSecondary - staged techniques
single stage – good conditionssingle stage – good conditions
two stage – after complicated injuristwo stage – after complicated injuris1-st stage – endoprothesis1-st stage – endoprothesis2-nd stage – tendon graft.2-nd stage – tendon graft.
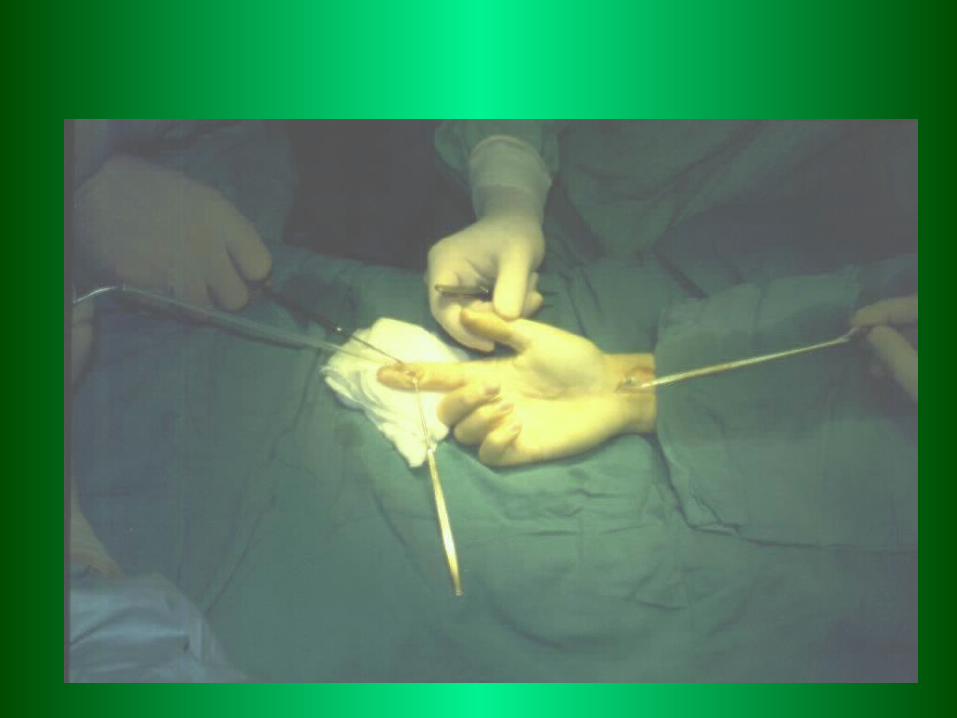
Secondary Secondary tendon tendon repairrepair
1.1.One stage reconstruction One stage reconstruction FTG /free tendon graft/ FTG /free tendon graft/
1.1. Bunnel1.1. Bunnel graft zone graft zone I-III I-III I° wg Boys`aI° wg Boys`a
1.2. Matev 1.2. Matev graft zone graft zone I-VI-V
1.3. 1.3. Interposition graftInterposition graft III-V III-V
2. TFTI (temporary flexor tendon implant)2. TFTI (temporary flexor tendon implant)
2.1. 2.1. ShortShort graft graft I-IIII-III
2.2. 2.2. LongLong tendon graft tendon graft I-VI-V

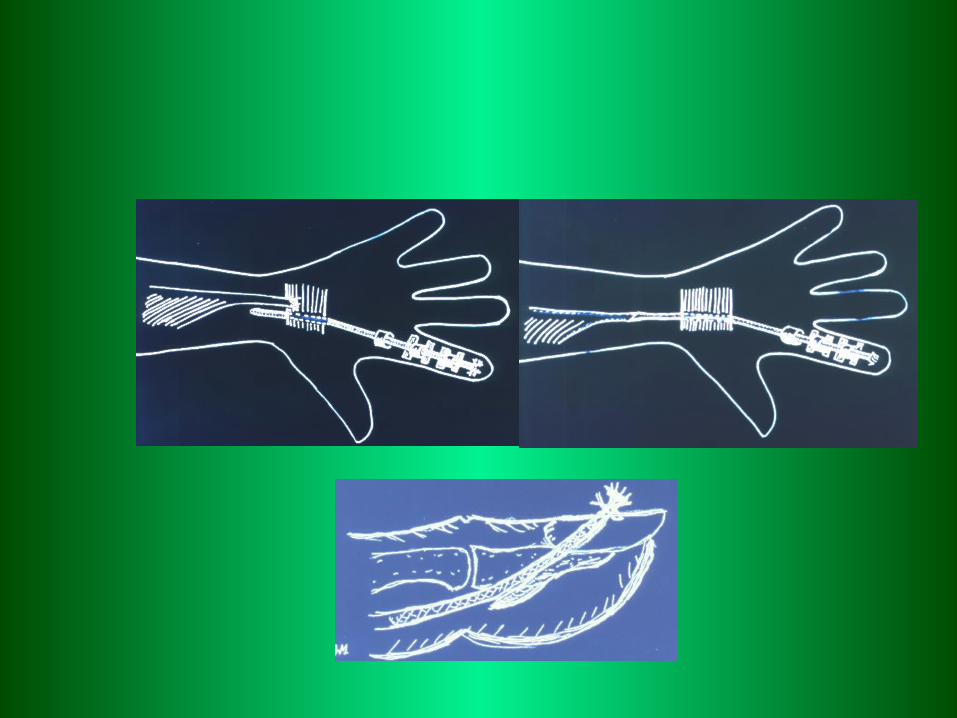
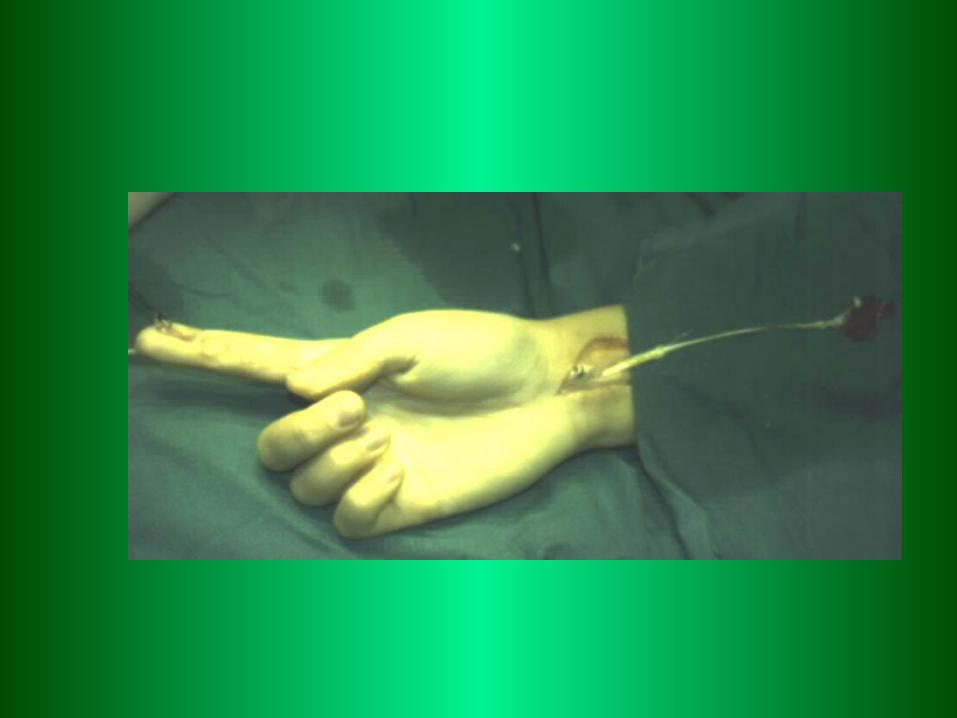
Tendon reconstructionTendon reconstruction
Tendon graftsTendon grafts
Short – zone 1-3Short – zone 1-3Long – zone 1-5Long – zone 1-5












Prostowniki
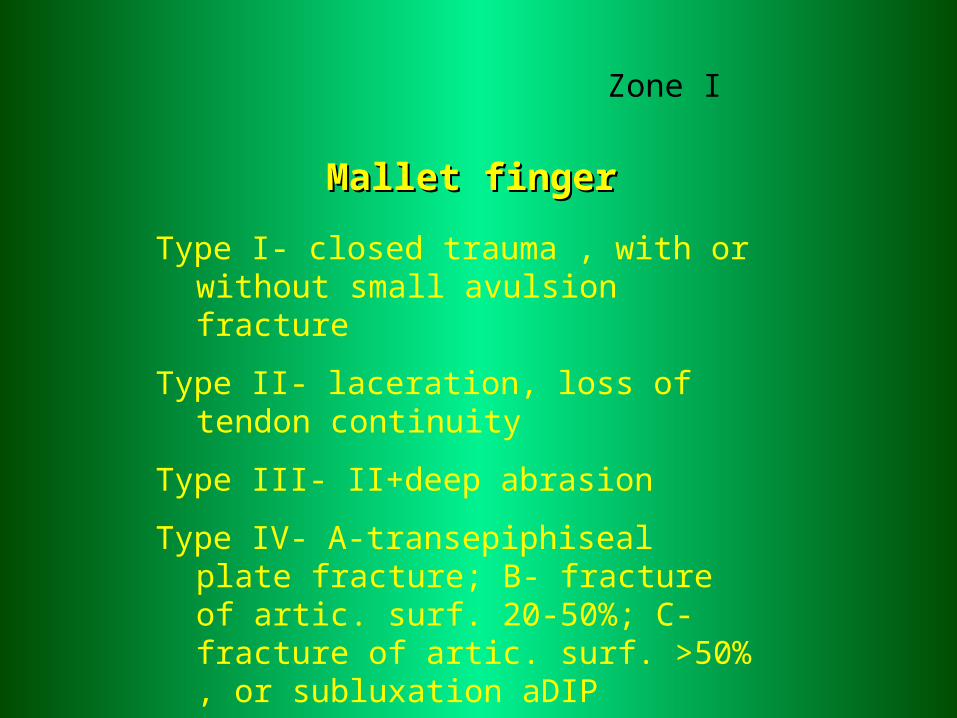
Mallet fingerMallet finger
Type I- closed trauma , with or without small avulsion fracture
Type II- laceration, loss of tendon continuity
Type III- II+deep abrasion
Type IV- A-transepiphiseal plate fracture; B- fracture of artic. surf. 20-50%; C- fracture of artic. surf. >50% , or subluxation aDIP
Zone I
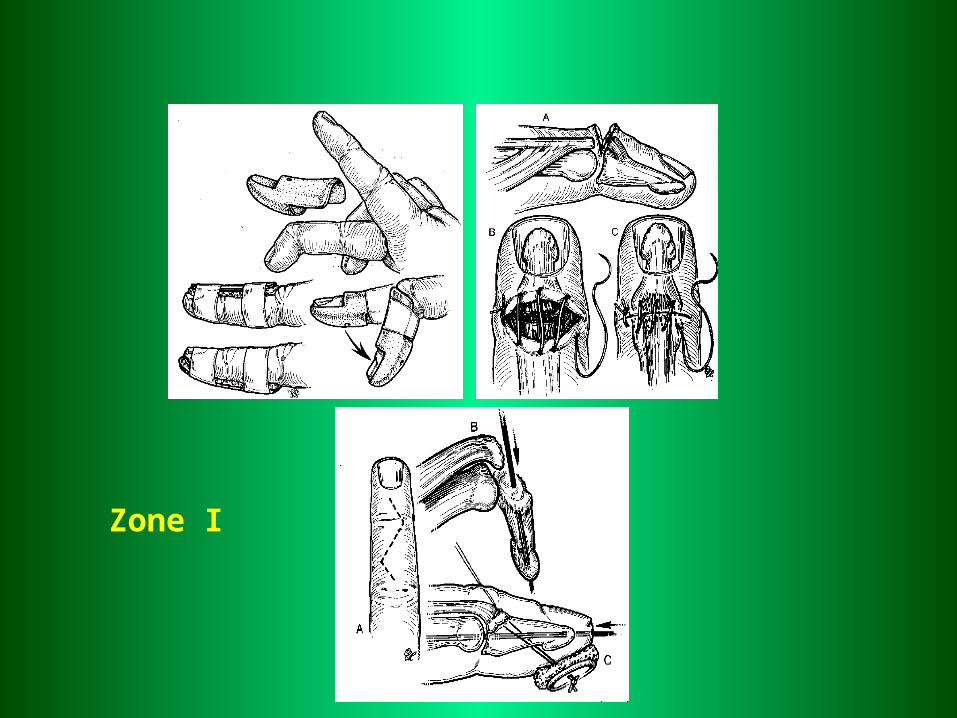
Zone I
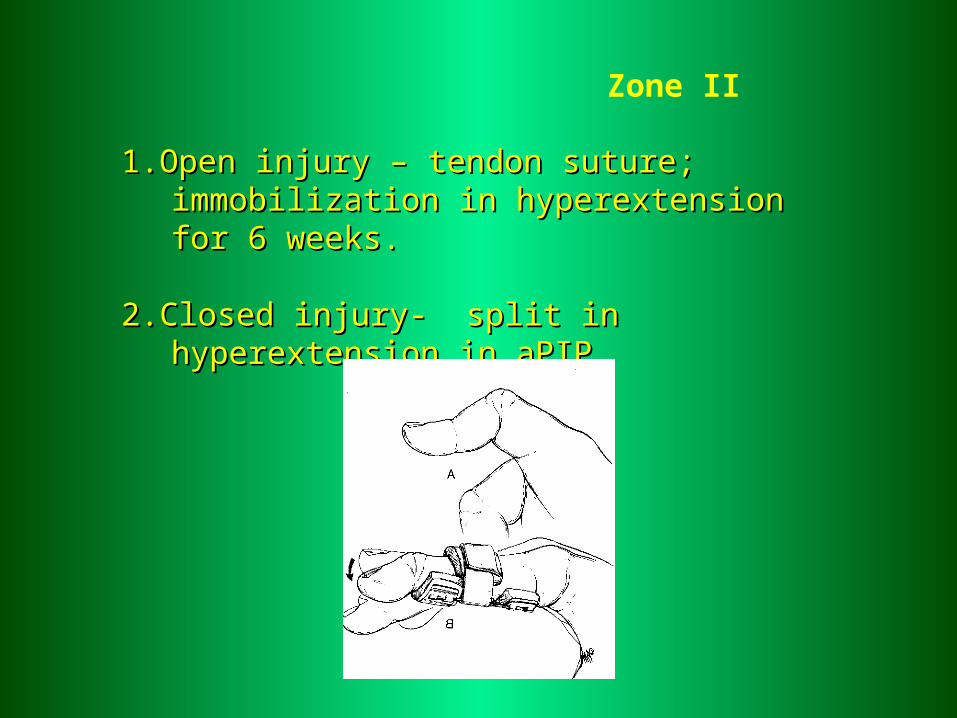
Zone II
1.1.Open injuryOpen injury – – tendon suturetendon suture; ; immobilization in immobilization in hyperextension for 6 weekshyperextension for 6 weeks..
2.2.Closed injury- Closed injury- split in hyperextension insplit in hyperextension in aPIP aPIP
Zones III, IV,V
Open injury:- tendon suture, immobilization aPIP 0° to 5-6 weeks -
exercise- Zone V – wrist immobilization in flexion 40°. MP joints in
flexion 10-20°.
Closed injury:- splint for 6 weeks
Zones VI-IX
End to end tendon suture.Immobilization – wrist in hyperextension 40-45° for 4-5 weeks
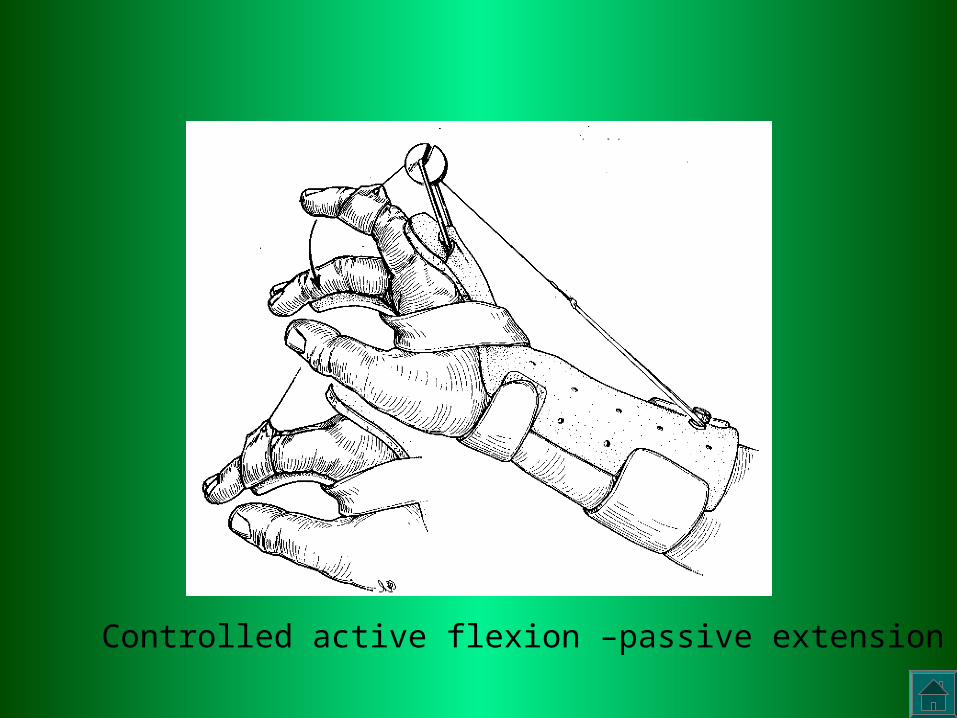
Controlled active flexion –passive extension