Embed Size (px)
Citation preview

Virtual Clinics
From women’s health to pre-operative assessment
Setting up & sustaining virtual clinics
28th April 2017
2017
Stephen Radley MD FRCS FRCOG
Urogynaecologist
Director of Research Jessop Wing
Sheffield Teaching Hospitals NHS FT
Director of R&D, ePAQ Systems Ltd
An NHS spin-out technology company

Understanding service virtualization: Where to start?
Case study: Virtual clinics: From Gynaecology to Pre Op Assessment
Understanding service virtualization: The theory
Tools and pathways
Where to start? Lessons from our virtual clinics
Developing a web-based ‘Virtual Clinic’ in Urogynaecology
The benefits of virtual clinics for ‘sensitive’ conditions
Practicalities and a walk through how the clinic works in practice

Understanding service virtualization: The theory
Virtual Clinic Provision of remote or non-face to face medical care, utilizing communication media
e-Health Healthcare practice supported by electronic processes & communication
Cybermedicine / Telemedicine Use of internet / electronic media to deliver medical services
(e.g. consultations & prescriptions)
Remote transmission of data
(e.g. images, results & assessments) supporting health care
Cyber Clinician Medical professional providing consultation via the Internet

Tools and pathways
Face to face… Post… Telephone… Internet… Cloud… Mobile
Retail, travel, financial services…… …healthcare

Pathways
NHS England
Technology Enabled Care Services: TECS Resource for commissioners
‘Maximise value of TECS for patients, carers, clinicians, health economy’
Defined as…
Telehealth, Telecare, Telemedicine, Telecoaching, Self-care
Aiming to…
Improve long-term conditions: convenient, accessible & cost effective
www.england.nhs.uk/ourworld/qual-clin-lead/tecs

Value & Burden: Virtual Clinics
Appropriate, accessible, practical
Is it clinically useful to patients & clinicians?
Can it be used in different settings?
How does it impact on patient care?
What is the cost - benefit to patients, society & providers?

80.471.4
59.3 58.4
39.0
11.1
0%
20%
40%
60%
80%
100%
would
recommend
would
undergo
again
subjective
improvement
or cure
no GSI normal
urodynamic
study
subjective
cure
The ‘Science’ of Outcomes Assessment

Symptoms vs Investigations
(BFLUTS): "Does urine leak before you can make it to the toilet?"
0%
20%
40%
60%
80%
100%
Never
(n=6)
Some- times
(n=20)
Occas-
ional
(n=32)
Most of
time
(n=27)
All the
time (n=10)
% w
ith d
etr
usor
overa
ctivity
Ambulatory
Urodynamics
Standard
Urodynamics

Bristol female urinary
tract symptoms - Q
Birmingham
bowel & urinary
tract - Q
Sheffield prolapse
symptoms - Q
Female sexual
function index
ICS
Male
Pelvic Floor
Assessment (PAQ)
Questionnaires
Developing a web-based ‘Virtual Clinic’ in Urogynaecology

Why an electronic
questionnaire ?
Burden
Value (interactive, simple & easy, help pages)

Radley S et al. Development & validation of a questionnaire for the
assessment of bowel symptoms in women. BJOG 2002
Radley SC et al. Computer interviewing in urogynaecology. BJOG 2006

ePAQ – Pelvic Floor
Structure
• Introductory pages
• Questionnaire dimensions (up to 120 items)
Urinary
Bowel
Vaginal
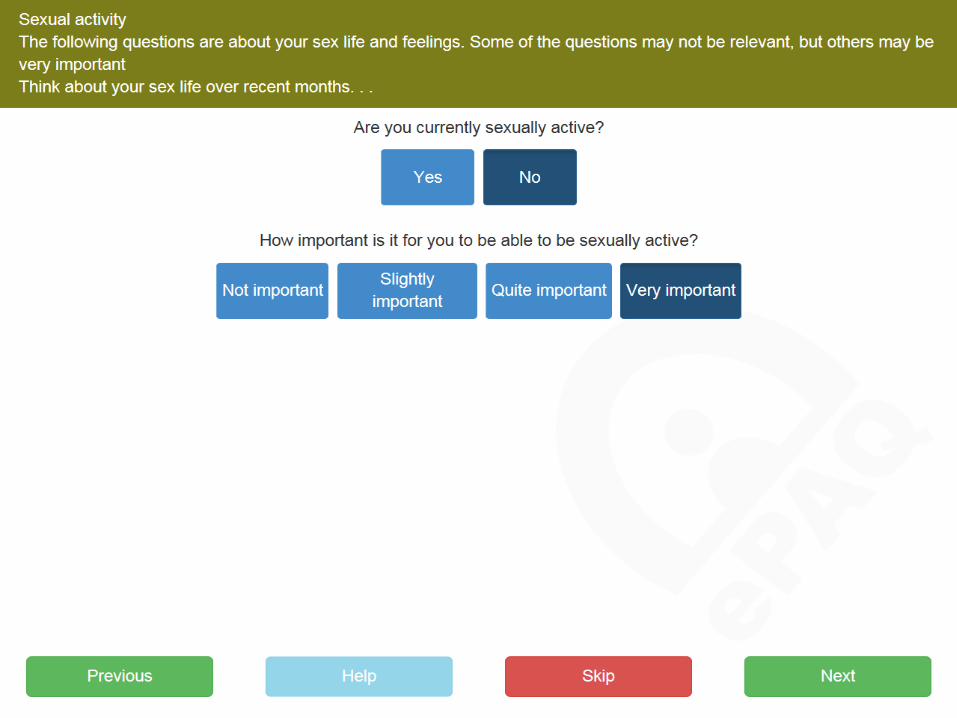
Sexual
• Analysis, summary, printed report
Interactive &
optional
dimensions

ePAQ – Pelvic Floor
A questionnaire for clinical use





















Would you recommend this service
to Friends & Family?
2 year data – Follow up patients
N %
Extremely likely 445 66
Likely 173 26
Neither likely nor unlikely 35 5
Unlikely 7 1
Extremely unlikely 12 2
Total 672
‘Likely’ or ‘Extremely likely’ 92


ePAQ-PF Summary report

ePAQ – MPH (Menstrual, Pain, Hormonal)

Symptoms
Impact
ePAQ Detailed report
(Lower Urinary Tract Symptoms)
QoL

29 year old, Pakistani, Non-English speaking
Schizophrenia
Not examined
MSU -ve
Solifenacin 5mg

Routine clinical care

The Virtual Clinic

2006 survey of ePAQ users in urogynae clinic
• 80% of under 50s had internet access
• 45% of over 50s had internet access
95% of those with home internet access…
‘Would have liked to have used system before coming to clinic’

The Virtual
Clinic
Name Tel Time
Anna Smith AS1234 078212344 14:00
Beryl Jones BJ8765 0114 3098909 14:10
Connie Lewis CL2345 0114 3897890 14:20
Diane Cole DC4567 07989997654 14:30
Edna Rose ER3847 07635668234 14:49
Fiona Groves FG2783 0114 3897890 14:50
Greta Holmes GH1783 0114 3897890 15:00
Heidi Hill HY7896 0114 3897890 15:10
Ida France TA1256 0114 3897890 15:20
Joanne Davies JD3456 0114 3897890 15:30
Kay Somers KS2365 07885668234 15:40
Lisa Tandy LY5698 0757 3897890 16:00
Margaret Smith MS3452 0114 3897890 16:10
Nora Bates NB2344 0114 3897890 16:20
Orla Charles OC3567 07835668234 16:30
Penelope Roper PR5702 07835668234 16:40
Rose Doyle RD5098 07835668234 16:50
Selena Bird SB8090 07835668234 17:00
Tina Moores TM3409 07835668234 17:10
Ursula King PL0987 07835668234 17:20
Violet Bonnett VB0934 07735668239 17:30

Benefits of virtual clinics for sensitive conditions
• Disclosure, discussion & shared decision making 1
• Embedded outcome measures (PROMs & PREMs) 2
• Avoiding clinician bias 3
• Engagement, enablement, empowerment 4
1. Schussler-Fiorenza et al. Using an electronic pelvic floor questionnaire to increase discussion rates of urinary incontinence in primary care: an RCT. (In Press)
2. Black et al Relationship between patient reported experience (PREMs) and patient reported outcomes (PROMs) in elective surgery. BMJ 2013
3. Black et al. Impact of surgery for stress incontinence on morbidity: cohort study. BMJ 1997
4. Dua et al: Understanding women’s experiences of electronic interviewing during the clinical episode in urogynaecology: A qualitative study. IUGA Journal 2013

Patient comments…
I preferred answering the more embarrassing questions via the questionnaire than
face to face
Knowing that an examination was out of the question put me more at ease
Phone consultation excellent, relaxed & stress free
Thorough & informative way of doing things
I didn’t have to worry about childcare
Helped express my problems enormously
Helped focus on urgent and relevant problem
Made me realise the extent of my problem
Helped talk at ease about my problems
It was really easy to use
Good, enjoyable, easy and quick!
Good idea, well done!

0%
10%
20%
30%
40%
50%
Strongly
agree
Mostly agree Neither
agree nor
disagree
Mostly
disagree
Strongly
disagree
'The questionnaire was helpful during my clinic visit'

Disclosure Prevalence of coital incontinence in urogynaecology clinics
Author(s) Number of women Outcome measure Prevalence
Moran et al, 1999 2153 Direct questioning 10.6%
Serati et al, 2008 132 Direct questioning 11.6%
Madhu et al, 2015 11689 Direct questioning 11.8%
Monsterrat et al, 2008
633
KHQ
36.2%
Bekker et al, 2009 136 Non-validated Q 56%
El Azab, 2011 90 Non-validated Q 66%
Jha et al, 2012 480 ePAQ-PF 60%
Gray et al, 2016 2312 ePAQ-PF 47%

Practicalities How the clinic works
1) Standard appointments booking system
Patient preference choice, patient information
2) www.epaq-voucher.co.uk
Arranged via OPD / Ward staff / Secretary
3) Monthly clinic: 20 x 10 min appointments
5 – 15 min, supported by correspondence, notes & ePAQ
4) Outcomes
Letter to GP + ePAQ report / ePAQ progress report
Letter to patient
Information leaflets
Follow up
Discharge
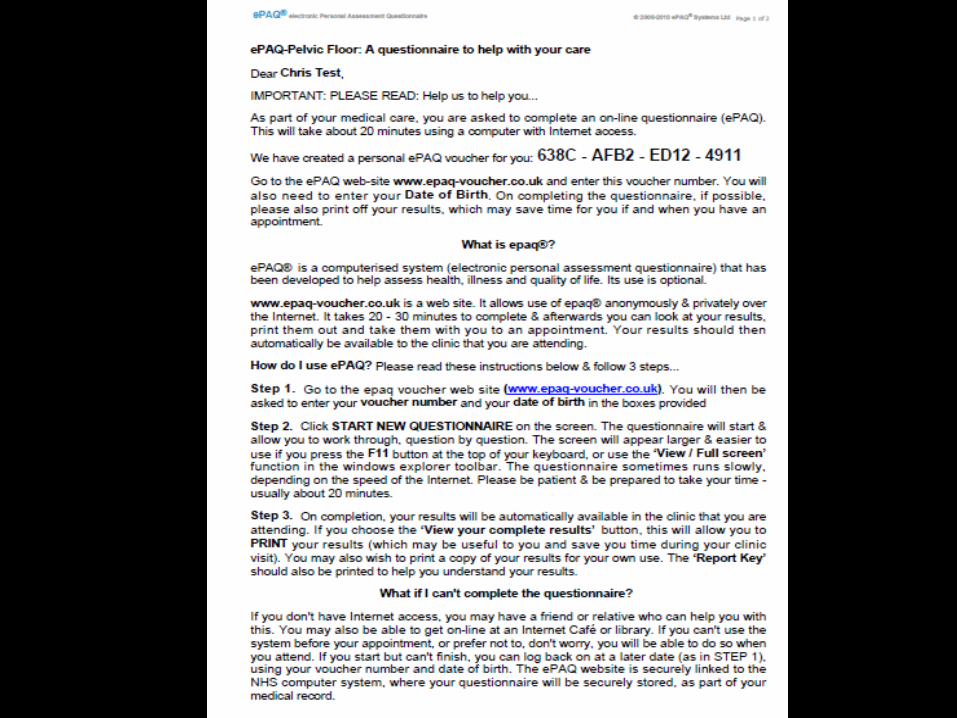

https://start.epaq.co.uk
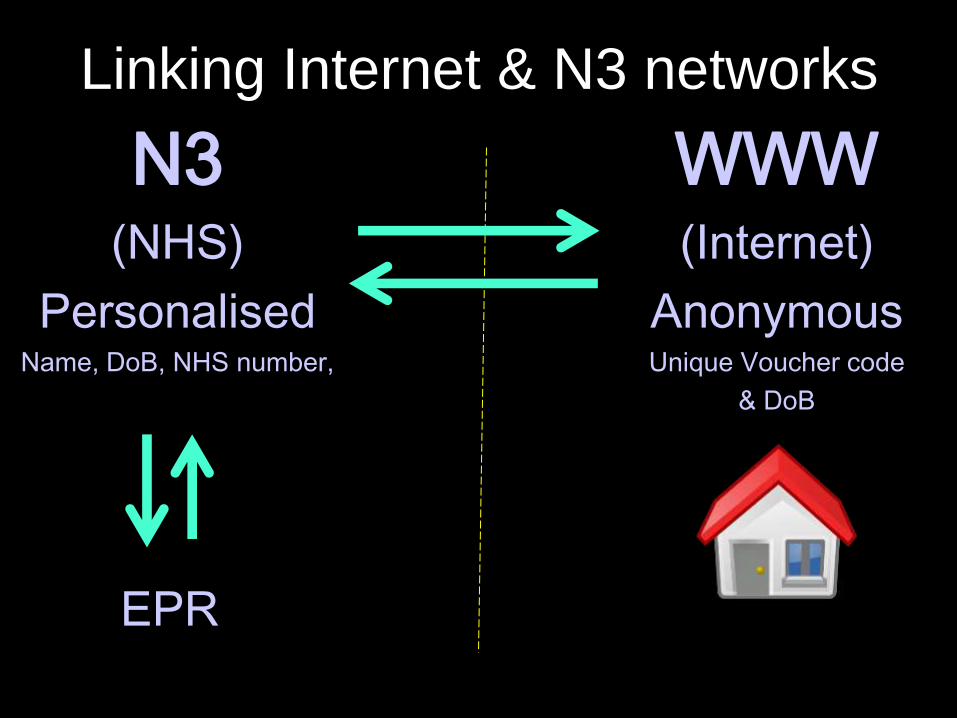
Linking Internet & N3 networks
N3 (NHS)
Personalised Name, DoB, NHS number,
WWW (Internet)
Anonymous Unique Voucher code
& DoB
EPR

Users
Manchester
Liverpool
Sheffield
Birmingham
Newcastle
Derby
Leeds
South Tees
Southport
Ormskirk
Scotland (S Ayr)
Italy (Milan)
Ire (Dublin)
100,000+
Colorectal, Urology, Physiotherapy,
Urogynaecology, Nurse Specialists

0
20
40
60
80
100
U P&S Voiding OAB SUI U QOL
Incontinence surgery: TVT pre and post op mean
ePAQ urinary domain scores (n=54)
pre op mean
post op mean
Effect size: SUI = 2.4 U-QoL = 2.2

Mean waiting time between referral & VUC: 28 days
(range 7 - 46)
Primary complaints
Stress incontinence (79%)
Overactive bladder (50%)
Prolapse (27%)
Bowel problems (24%)
Sexual dysfunction (24%)
VUC Outcomes (first 50 patients)

79% Treatment planned or initiated
39% Referred to physiotherapy
44% Scheduled urodynamics
12% Clinic follow-up
8% Referred to another clinic
Virtual Clinic:
First 50 patients

Positive aspects (0 = worst, 100 = best possible)
Communication (PEQ)
84 (SD = 16)
Value (QQ-10)
77 (SD 16)
Negative aspects (0 = best, 100 = worst possible)
Barriers (PEQ)
15 (SD = 15)
Burden (QQ-10)
25 (SD = 16)
Virtual Clinic: Satisfaction Data

0%
10%
20%
30%
40%
50%
Strongly
agree
Mostly agree Neither
agree nor
disagree
Mostly
disagree
Strongly
disagree
'The questionnaire was helpful during my clinic visit'

0
20
40
60
80
100
Disagree
completely
Disagree So-so Agree Agree
completely
'I felt taken care of'%

Evaluating the impact of a ‘virtual clinic’ on the quality
and cost of patient care in urogynaecology: An RCT
Jones GL, Radley SR, Jacques RM, Wood HJ, Brennan V, Dixon S.
195 Women: New patient referrals to
urogynaecology clinic

Resource Cost per patient
(Intervention) (£) N = 27
Cost per patient (control) (£)
N = 30
Mean Difference (£)
95% CI Lower
95% CI Upper
P-value
Cost of Consultations
Consultation cost1 29.35 69.52 -40.17 - - -
Cost of software 2.40 2.40 0 - - -
Cost of computer N/A 0.25 -.25 - - -
Total consultation costs per pt
31.75 72.17 40.42 - - -
Direct costs 6/12
GP Visits 41.22 35.33 5.89 -25.29 37.06 .654
Practice nurse 0.94 2.13 -1.18 -3.77 1.41 .063
Appointments 251 188 62.67 -87.02 212.36 .405
Surgery 330 286 44.88 -353.35 442.97 .822
Other professionals
Physio 5 5 .05 -7.58 7.68 .989
Nurse 4.5 2 2.49 -5.48 10.45 .534
Consultant 8 14 -6.35 -23.22 10.51 .454
Total direct costs 641 532 108.37 -346.93 563.67 .635
Indirect costs 6/12
Personal expenditure (£)
24 16 7.9 -6.04 21.84 .261
Loss of productivity 443 481 -37.81 -847.04 771.42 .926
Total indirect costs 467 497 -29.91 -839.47 779.66 .946
Total costs per pt 1,140 1102 38.04 -1119.34 1196.03 .948
RCT: New patient referrals in urogynaecology

Resource Cost per patient
(Intervention) (£) N = 27
Cost per patient (control) (£)
N = 30
Mean Difference (£)
95% CI Lower
95% CI Upper
P-value
Cost of Consultations
Consultation cost1 29.35 69.52 -40.17 - - -
Cost of software 2.40 2.40 0 - - -
Cost of computer N/A 0.25 -.25 - - -
Total consultation costs per pt 31.75 72.17 £40 (56%) - - -
Direct costs 6/12
GP Visits 41.22 35.33 5.89 -25.29 37.06 .654
Practice nurse 0.94 2.13 -1.18 -3.77 1.41 .063
Appointments 251 188 62.67 -87.02 212.36 .405
Surgery 330 286 44.88 -353.35 442.97 .822
Other professionals
Physio 5 5 .05 -7.58 7.68 .989
Nurse 4.5 2 2.49 -5.48 10.45 .534
Consultant 8 14 -6.35 -23.22 10.51 .454
Total direct costs 641 532 108.37 -346.93 563.67 .635
Indirect costs 6/12
Personal expenditure (£)
24 16 7.9 -6.04 21.84 .261
Loss of productivity 443 481 -37.81 -847.04 771.42 .926
Total indirect costs 467 497 -29.91 -839.47 779.66 .946
Total costs per pt 1,140 1102 38.04 -1119.34 1196.03 .948
RCT: New patient referrals in urogynaecology

Mean difference between groups & 95% CI for post consultation PEQ scores
(positive mean difference indicates the intervention group has a better score)

Summary of RCT Findings Virtual Clinic does appear to positively improve patient experience of consultation, particularly communication Virtual clinics may prove beneficial in overcoming barriers, improving emotional wellbeing and enhancing communication Significant difference between the duration of consultations (Approx 50% shorter) and associated consultation costs Patient selection & tariffs important factor in cost / benefit Follow-up care, Long-term conditions

Other applications
ePAQ-PO
(Pre Op Assessment)
ePAQ-Vascular
(NIHR ScHARR)

ePAQ-PO
Summary Report





Walk-in Pre Operative Assessment
• 2 sites (NGH & RHH)
• 12 touchscreens
• Support worker
• POA nurse
• 5 long day service…

ePAQ-PO implementation in Sheffield Teaching Hospitals 2015 - 2016

‘The questionnaire helped with communication’
%

‘Willing to use again’
%

Comments
‘Very impressed with the online system has it was quick and easy to complete’ ‘I thought the questionnaire was easy to complete and very thorough’ ‘The questionnaire was far too long and had nothing to do with my condition’
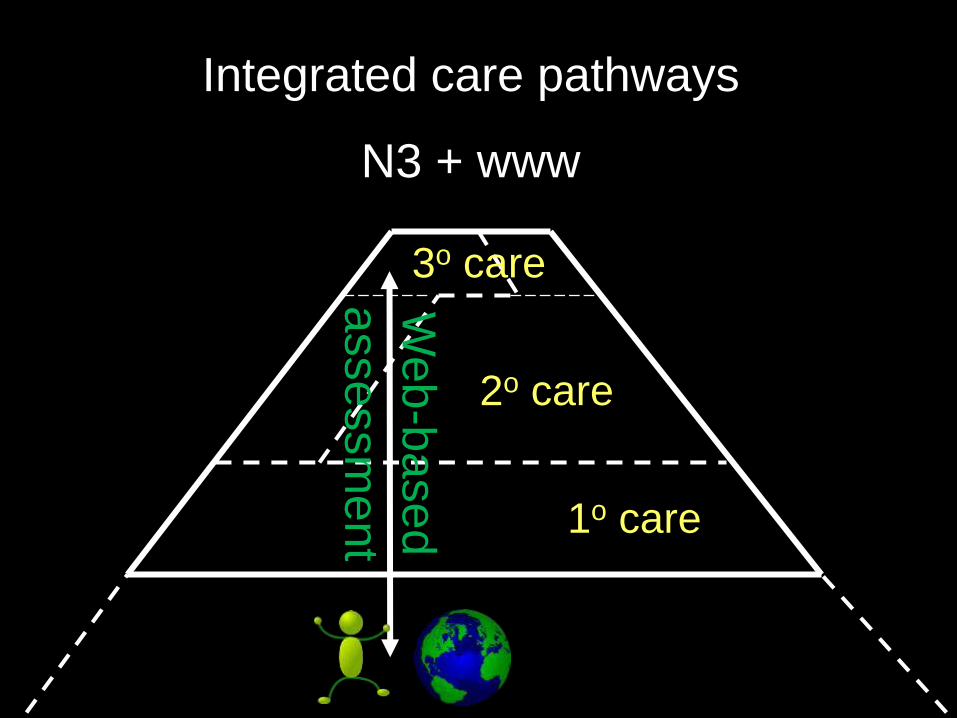
Integrated care pathways
N3 + www
1o care
2o care
3o care
Web
-based
assessm
ent

Home
Internet
Standardisation
Clinical governance
Screening
& Triage
Secondary care
Web-based assessment
Supporting patient-centred, integrated healthcare
Clinical assessment
Primary care
Research, Audit
Service evaluation
Appraisal,
revalidation,
Accreditation
Appointments

Where to start? Lessons from our virtual clinics
Consider: patients, clinicians, management & managing change
Champions: Staff / Colleagues / Managers / Stakeholders
Funding: Business case / Grants
Industry / Commissioners
Integration with e-systems…
Its not all about the money….
….but

Thank You
Computer interviewing in urogynaecology: concept, development and psychometric testing of an electronic pelvic floor assessment questionnaire (e-PAQ) in primary and secondary care. Radley et al. BJOG, 2006
Increasing Discussion Rates of Incontinence in Primary Care: A Randomized Controlled Trial. Sophia Miryam
Schussler-Fiorenza Rose et al. Journal of Women’s Health. Volume 24, Number 11, 2015 The use of free text items in electronic questionnaires to record patients’ concerns, goals and questions relating to
their condition. Gray et al. Proceedings of BSUG. Int Urogynecol J. 2015 QQ-10: An instrument to measure face validity and feasibility of questionnaire use in healthcare. Moores K, Jones G, Radley SC. Int J Quality in Health Care. 2012 Prolapse surgery and sexual function. Dua A, Jha S, Farkas A, Jones GL, Radley SC. International Urogynecology
Journal. (Oct 2011) Effect of posterior colporrhaphy on anorectal function. Dua A, Jha S, Farkas A, Jones GL, Radley SC. International
Urogynecology Journal. (2011) Quality of life measurement & electronic assessment in urogynaecology. Dua et al. The Obstetrician &
Gynaecologist (2011) Factors affecting the outcome of TVT. Jha S et al. European Journal of Obs Gyn Repro Biol (2008) Responsiveness of ePAQ-PF. Jones GL et al. Int Urogynecol J Pelvic Floor Dysfunct. (2008) Impact of TVT on Sexual function. Jha et al. Int Urogynecol J Pelvic Floor Dysfunct. (2008) Electronic pelvic floor symptoms assessment: tests of data quality of ePAQ-PF. Jones GL et al. Int Urogynecol J Pelvic
Floor Dysfunct. (2008)

Pre-Operative Assessment Patient-completed, preoperative web-based anaesthetic assessment questionnaire (electronic Personal Assessment Questionnaire Pre-Operative) Development and validation. Iain M. Goodhart, John Andrzejowski, Georgina Jones, Mireille Berthoud, Andy Dennis, Gary Mills and Stephen Radley. Eur J Anaesthesiol 2016; 33:1–8 An evaluation of factors influencing the assessment time in a nurse practitioner-led anaesthetic pre-operative assessment clinic. R. H. Hawes, J. C. Andrzejowski, I. M. Goodhart,3 M. C. Berthoud and M. D. Wiles. Anaesthesia 2015; doi:10.1111/anae.13340 Electronic Personal Assessment Questionnaire Pre-Operative: Patient experience and face validity of an interactive, electronic questionnaire for the preoperative assessment of patients due to undergo general anaesthesia: Goodhart I, Andrzejowski J, Berthoud M et al. British Journal of Anaesthesia 2012; 109: 655- 668 How valid are patient-reported height and weight using an interactive computerised pre-operative assessment questionnaire (ePAQ-PO)? Andrzejowski, JC. Goodhart, IM ; Berthoud, M ; Radley, SC ; Hawes, RH. British Journal Of Anaesthesia, 2013 May, Vol.110(5), pp.861-861

![PROPOSED 2018 - floridadep.gov Region - DRAFT... · Docme COLL!qoL COLL!qoL luJ go COLL!q L nouucello -OLLI neao 00 L CCGC!I COLL!qoL IVX Lorue COLL!qoL ash 01] q so LL!qoL u BIAq](https://img.pdfslide.us/doc/110x75/5aa619db7f8b9ae7438e63bc/proposed-2018-region-draftdocme-collqol-collqol-luj-go-collq-l-nouucello.jpg)