Embed Size (px)
Citation preview

Virginia C. Li, PhD, MPHProfessor of Community Health Sciences
Health Promotion (Green)
The combination of educational and environmental supports for actions and conditions conducive to health

An Ecological View on Health Promotion-Intrapsychological factors-Interpersonal processes-Institutional factors-community factors-public policy

Health Promotion in Community Health promotion actions means:-create supportive environment-strengthen community action-develop personal skills-reorient health services-build healthy public policy


Health Education
Any combination of learning experiences designed to facilitate voluntary actions conducive to health

Principles of Health Education-principle of educational diagnosis-hierarchical principle-principle of cumulative learning-principle of participation-principle of situation specificity-principle of multiple methods-principle of individualization-Feedback principle-principle of intermediate target

Deaths due to Tobacco Use• In the 20th century, the tobacco epidemic
killed 100 million people worldwide. • During the 21st century it could kill one billion.
• Tobacco causes 1 in 10 adult deaths worldwide
• WHO 2002
• And ……


Smoking Prevalence Among U.S. Adults, 1955–2007(as a percent of population, 18 years of age and older)
Year Overall population
Males Females Whites Blacks
1955 — 56.9% 28.4% — —
1965 42.4% 51.9 33.9 42.1% 45.8%
1970 37.4 44.1 31.5 37.0 41.4
1980 33.2 37.6 29.3 32.9 36.9
1990 25.5 28.4 22.8 25.6 26.2
2000 23.3 25.7 21.0 24.1 23.2
2002 22.5 25.2 20.0 23.6 22.4
2003 21.6 24.1 19.2 22.7 21.5
2004 20.9 23.4 18.5 22.2 20.2
2007 20.8 23.9 18.0 21.9 23.0
Source: U.S. Centers for Disease Control and Prevention. Web: www.cdc.gov.


Declines in U.S. Cigarette Consumption 1990-2005

Dimensions of the Anti-smoking Movement1) Epidemiological research2) Mass media2) Interpersonal communications
3) Advocacy /Legislation

Dimensions of the Anti-smoking Movement : EpidemiologySurgeon Generals Report - 1964 - smoking linked to lung cancer , heart disease
Continuing research - quitting improves health, nicotine addictive
Continuing research - second hand smoke kills, health of persons in smoke free zones better

Dimensions of the Anti-smoking Movement: Mass Media
1971 ban on TV/Radio cigarette ads Warning signs on cigarette packs Change in behavior of public figures Many visible /viable anti-smoking efforts
Publicity about epidemiological findings

Dimensions of the Anti-smoking Movement: InterpersonalEarly 1980’s Increase # anti-smoking clinics
Increase expectations/social pressure not to smoke
Increase awareness of preventive health behaviors

Dimensions of the Anti-smoking Movement: Advocacy/LegislativeLate 1980’s : Government regulations
about smoke-free environmentsAdvocacy groups push policy changes
at all levels: higher taxes on cigarettesCorporate anti-smoking policiesInsurance companies-no smokersLawsuits- get big tobacco

Types of Smoking Control Programs-Worksite Control Programs
-Worksite Control Policies-School Based Control Programs-Community Based Control Programs-Physician/Clinic Based Control Programs-Policy-Based Smoking Programs-Economic-Based Smoking Programs

Policy and Environmental Interventions -clean indoor air
-restricting tobacco advertising and promotion-restricting use access to tobacco-comprehensive school health programs-price/excise taxesAdditional interventions-insurance premium differentials-reimbursement for smoking cessation-differential hiring of smokers-litigation as policy

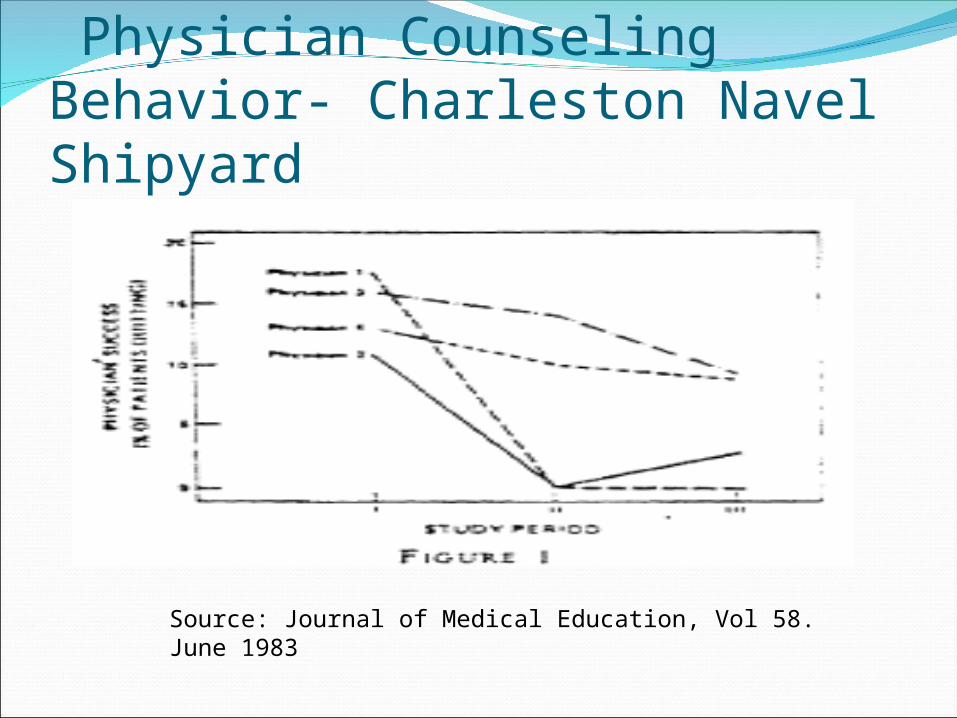
Physician Counseling Behavior- Charleston Navel Shipyard
Source: Journal of Medical Education, Vol 58. June 1983

Physician Counseling Behavior- Baltimore Family Planning Clinics
Source: Journal of Medical Education, Vol 58. June 1983

Healthy People 2010 Objectives Increase to at least 905 the proportion of internists and family
physicians who routinely advise cessation and provide assistance, follow up, and document charts for all their tobacco-using patients.
Percentage of Clinicians
1992Routinely providing service to 81-100% of patients Inquiry about tobacco use Internists
75% Family physicians
59%Discussion of strategies to quit Internists
50% Family physicians
45%

Anti-smoking Movement: California(1999)
Late 80’s- Prop 99 -taxes fund anti smoking efforts
Funds spent - smoking rates come down Early 90’s : Wilson re-appropriates funds Campaign stalls ( mid 90’s)- smoking rates
go up especially among youth , minority members
Attorney General forced to join law suit against tobacco companies

Mass Settlement Agreement (1998)
Holds tobacco companies accountable for their actions
Pays restitution to 46 states for health care costs incurred from tobacco-caused illnesses
Also exempted the companies from private tort liabilities regarding harms caused by an use of tobacco. In exchange, companies agreed to:Curtail certain marketing practicesPay, in perpetuity, various amount payments to the
states to compensate for some of the medical costs Dissolve the tobacco industry groups- Tobacco
Institute, Center for Indoor Air Research,Council for Tobacco Research

Family Smoking Prevention and Control Act (June 11, 09)
Initiated by Waxman, signed by B Obama, opposed by GW Bush
Allow FDA to lower the amount of nicotine in tobacco products
Ban candy flavorings that appeal to kids
Block misleading labels such as “low tar” and “light”
Tobacco companies will be required to cover their cartons with large graphic warnings

Tobacco use is the leading preventable cause of death in the world!
WHO 2003
….Tobacco is the only legally available consumer product which kills people when it is used entirely as intended.
Oxford Medical
Companion
(1994)

Tobacco Industry at WorkToday’s teenager is tomorrow’s potential regular consumer, and the overwhelming majority of smokers first begin to smoke while still in their teens.
Philip Morris Internal Document (1981)

Teenagers – advertising targetWhile sports is by far the best avenue to attract, sample, and influence our core target smokers, it is not the only way. International movies and videos also have tremendous appeal to our young adult consumers in Asia.
Philip Morris Internal Document (1990)

THE Layout of the Market outside U.S.
Within the total market, there are areas of strong growth, particularly in Asia and Africa.…It is an exciting prospect.
British American Tobacco Internal
Document (1990)

Cigarette Production, Exports, and Domestic Consumption—United States, 1990–2004

Export The U.S. is the world’s largest exporter of
cigarettes, and for many years burgeoning exports offset declines in domestic consumption.
However, export volume that peaked at 243 billion pieces in 1996 has fallen to an estimated 170 billion in 1999.
Cigarette exports are falling as U.S. manufacturers transfer production of cigarettes to overseas sites to reduce costs and as consumption declines in some of the major U.S. export markets as anti-smoking activity increases.

Foreign Draw

PUFFED UPPhilip Morris Readies Global Tobacco Blitz Division Spin off Enables Aggressive Product Push;
High Tar Smokers in AsiaNew Products:
Marboro Mix 9- a high nicotine and high tar cigarette (introduced in Indonesia in July 2007)
Marboro Filter Plus- sold in South Korea, Russia,
Kazakhstan, UkraineMarboro Intense- a quick nicotine hit sold in
TurkeyHeatbar- hand held electronic device emits less
smoke than regular cigaretteMarboro Wides- extra thick cigarettes Wall Street Journal (1/29/2008)


Global Youth Tobacco SurveyCountry National survey or
jurisdiction where survey conducted
Surveyyear
Proportion currently using any tobaccoproduct [%]a
Males (95% CI)
Females (95% CI)
Brazil Rio de Janeiro 2005 17.2 (14.0 - 21.0)
15.7 (12.3 - 19.8)
Czech Republic
National 2002 35.5 (31.5 - 39.7)
33.6 (29.8 - 37.5)
Hungary National 2003 28.0 (23.8 - 32.7)
26.9 (23.2 - 30.9)
Bulgaria National 2002 28.6 (24.5 - 33.0)
39.2 (34.3 - 44.4)
Russian Federation
National 2004 30.1 (26.6 - 33.8)
24.4 (21.5 - 27.6)
India National 2006 17.3 (14.5 - 20.4)
9.7 (7.2 - 12.8)
Indonesia
National 2006 24.1 (19.0 - 30.1)
4.0 (3.0 - 5.4)
Malaysia National 2003 40.0 (34.6 - 45.7)
11.5 (9.4 - 13.9)
Pakistan Islamabad 2003 12.4 (9.2 - 16.5)
7.5 (5.4 - 10.2)
Mexico Mexico City 2003 29.4 (25.0 - 34.1)
24.8 (18.8 - 32.1)
Source: WHO REPORT ON THE GLOBAL TOBACCO EPIDEMIC, 2008


Missing in Tobacco Control Policies
Tobacco CROP SUBSTITUTION