Embed Size (px)
Citation preview
Vinnitsa National Pirogov Memorial Medical University
vertebral osteochondrosis
Head of the Department of Traumatology and Orthopedics MD, Professor Vladimir Fischenko
vertebral osteochondrosis
This is the most severe form of degenerative – dystrophic spinal diseases caused by pathological changes in the intervertebral discs . Over time , in this process involved between the small vertebral
joints , vertebral bodies and ligaments of the spine. Degree of pathological changes is determined by
morphological and functional features of the intervertebral discs .
The incidence over the age of 50 years up to 90% , currently there is a trend towards younger
osteochondrosis - and it occurs at the age of 16 - 20 years. Certain extent osteochondrosis associated
with physical transfer loads and is more common in people who are engaged in heavy physical labor
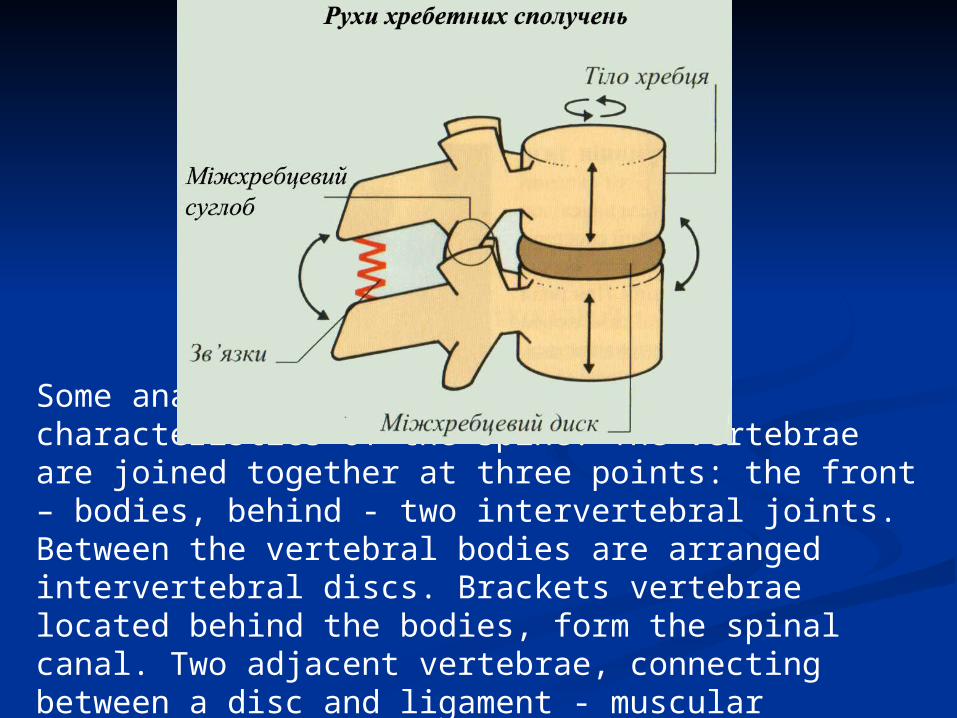
Some anatomical - physiological characteristics of the spine. The vertebrae are joined together at three points: the front – bodies, behind - two intervertebral joints. Between the vertebral bodies are arranged intervertebral discs. Brackets vertebrae located behind the bodies, form the spinal canal. Two adjacent vertebrae, connecting between a disc and ligament - muscular apparatus, form a single anatomical - functional complex - vertebral segment.
Intervertebral disc firstly connects the vertebrae together , and secondly, provide mobility therebetween , and thirdly, a good absorber that prevents trauma to the vertebral bodies during movement. Intervertebral discs give your spine flexibility, elasticity and mobility , as well as the ability to withstand significant physical activity . Intervertebral disc consists of two plates of hyaline bordering with closing plates adjacent vertebral bodies gelatinous nucleus pulposus and annulus fibrosus.
A gelatinous kernel is a capsule, whose walls are formed collagen fibers ; the capsule is filled with so - called chondrites gelatinous consistency containing the cartilage cells . This structure provides flexibility to the kernel . Fibrous ring of intervertebral disc is composed of bundles of connective tissue in the center of the loose and tight at the periphery ; front and side sections drive a few extend beyond the vertebral bodies. The anterior longitudinal ligament is adherent to the vertebral bodies and freely spreads through the disk . Posterior longitudinal ligament is involved in the formation of the anterior wall of the spinal canal , thrown loosely over the bodies of the vertebrae and fused with the rear surface of the disk .
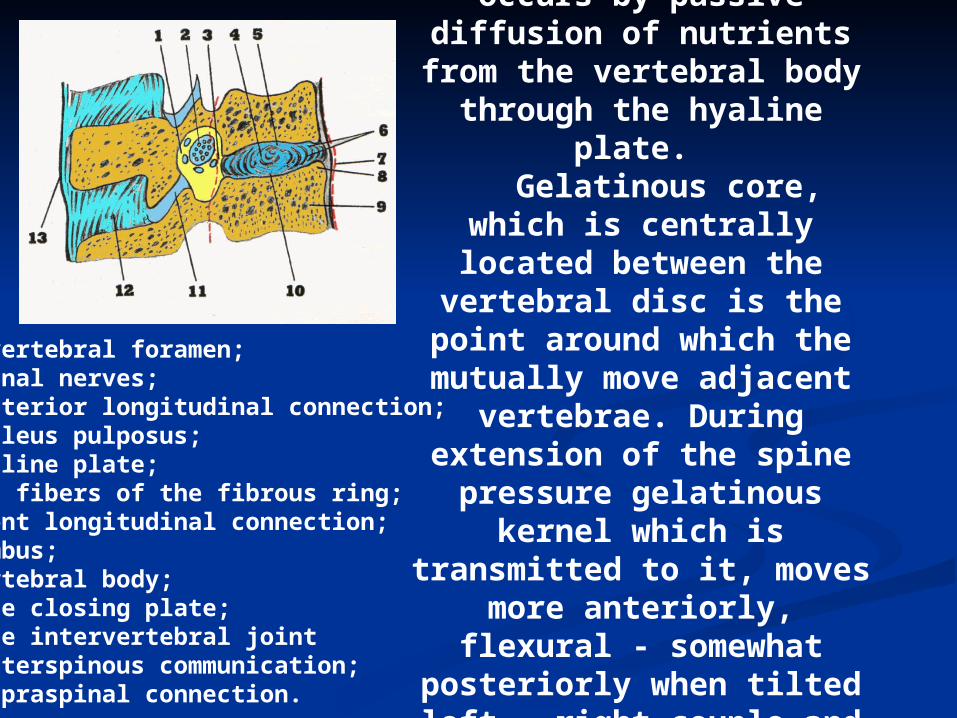
Trophism of the disk occurs by passive
diffusion of nutrients from the vertebral body
through the hyaline plate. Gelatinous core, which is centrally located
between the vertebral disc is the point around
which the mutually move adjacent vertebrae.
During extension of the spine pressure gelatinous
kernel which is transmitted to it, moves
more anteriorly, flexural - somewhat posteriorly when tilted left - right couple and vice versa.
Intervertebral foramen; 2. Spinal nerves; 3. Posterior longitudinal connection; 4. Nucleus pulposus; 5. Hyaline plate; 6. The fibers of the fibrous ring; 7. Front longitudinal connection; 8. Limbus; 9. Vertebral body; 10. The closing plate; 11. The intervertebral joint 12. Interspinous communication; 13. Supraspinal connection.
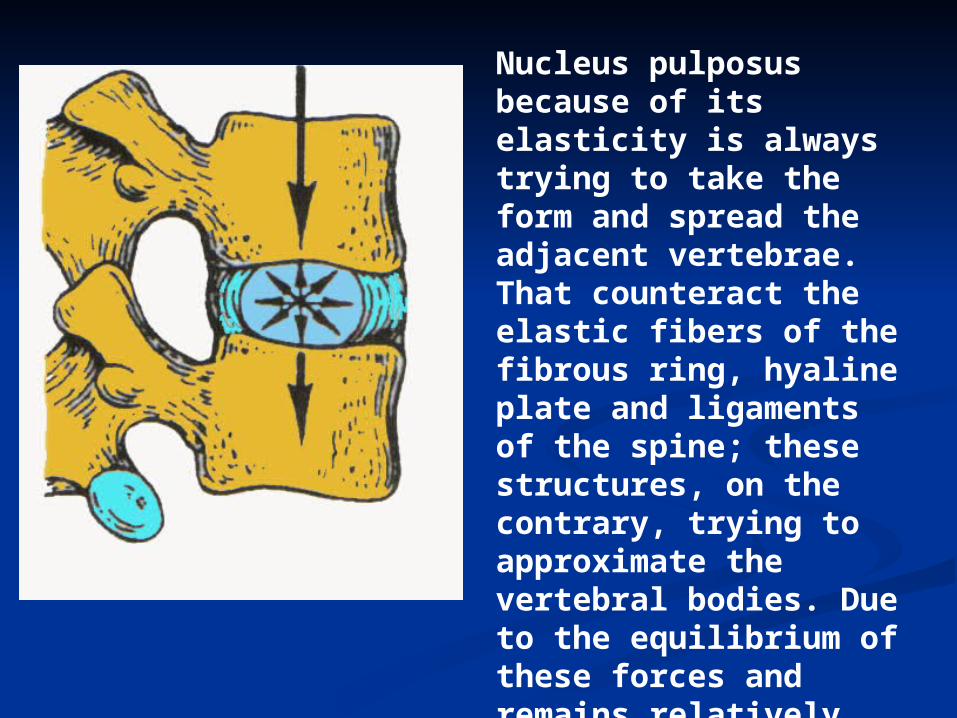
Nucleus pulposus because of its elasticity is always trying to take the form and spread the adjacent vertebrae. That counteract the elastic fibers of the fibrous ring, hyaline plate and ligaments of the spine; these structures, on the contrary, trying to approximate the vertebral bodies. Due to the equilibrium of these forces and remains relatively constant intervertebral slots
The etiology of osteoarthritis finally clarified to date. Some authors relate the appearance of the disease with an infectious factor, especially against the background of frequent hypothermia . Traumatic factor occurs in the majority of patients engaged in heavy physical labor of developing osteoarthritis , undoubtedly contributes to the corresponding spine injury . At the young age of osteochondrosis of the thoracic spine often occurs secondarily as a consequence osteochondropathy anterior divisions of the vertebral bodies - the so - called Scheuermann 's Mau disease.
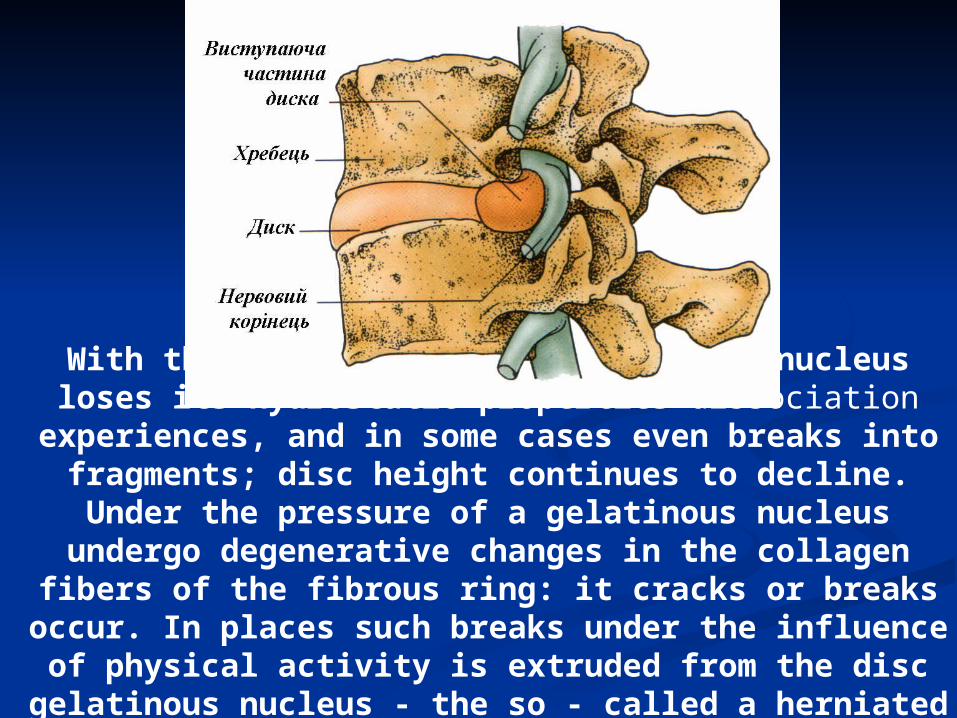
With the progression of a gelatinous nucleus loses its hydrostatic properties dissociation experiences,
and in some cases even breaks into fragments; disc height continues to decline. Under the pressure of a gelatinous nucleus undergo
degenerative changes in the collagen fibers of the fibrous ring: it cracks or breaks occur. In places
such breaks under the influence of physical activity is extruded from the disc gelatinous
nucleus - the so - called a herniated disc.
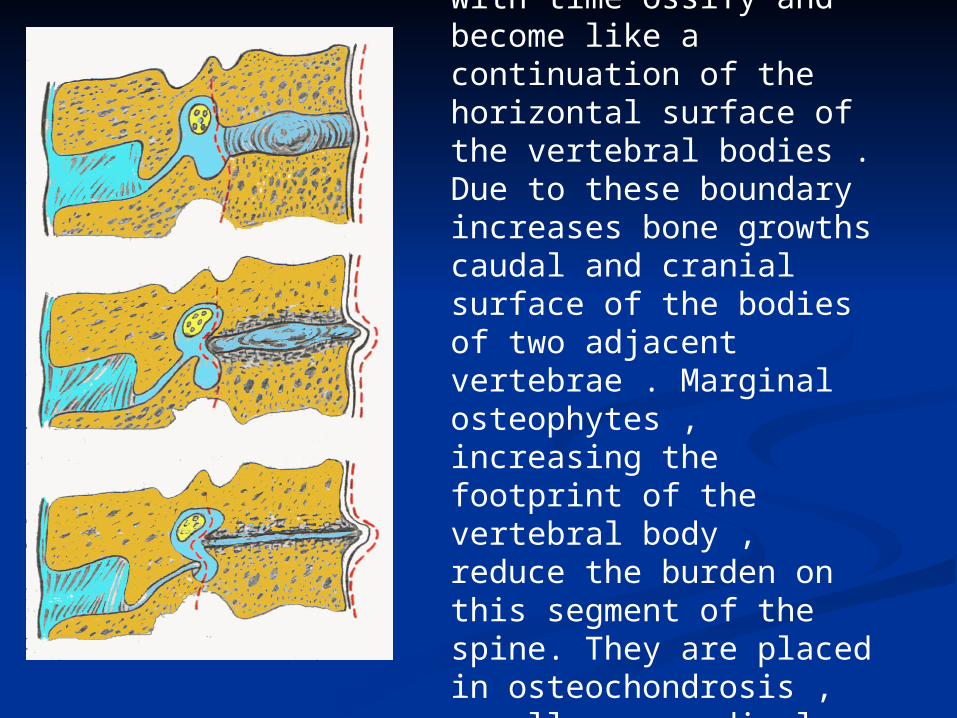
Broken pathologically altered gelatinous core fibers of the fibrous ring occupy a horizontal position , with time ossify and become like a continuation of the horizontal surface of the vertebral bodies . Due to these boundary increases bone growths caudal and cranial surface of the bodies of two adjacent vertebrae . Marginal osteophytes , increasing the footprint of the vertebral body , reduce the burden on this segment of the spine. They are placed in osteochondrosis , usually perpendicular to the axis of the spine and never coalesce with each other.
With the defeat of C3-C4 disc pain localized in the shoulder girdle, the heart, there is degeneration of the
posterior group of muscles in the neck; possible to change the tone of the
diaphragm muscle - while there are hiccups, flatulence.
Defeat disc C4-C5 causes pain in the shoulder and upper arm; there is a
weakness of the deltoid muscle, hypoesthesia on the outer surface of
the shoulder. Degenerative changes in the C5-C6
disc accompanied by pain, which runs from the shoulder girdle on the outer
surface of the shoulder and forearm to 1-2 fingers, with malnutrition and
decreased reflexes m. biceps brahii.
Defeat disc C6-C7 accompanied by the propagation of pain on the outside and back of
the shoulder and forearm to the third finger with gipoesteziya and decreased reflexes m.
triceps brahii. With osteochondrosis disc C7-Th1 pain
extends along the inner surface of the arm and forearm to 4-5 fingers marked hypoesthesia in these areas, malnutrition m. adductor policis
and m. fleksor policis longus.
Vegetatively - degenerative syndrome in osteochondrosis of the cervical spine is
manifested in the form of cervical diskalgia syndrome anterior scalene muscle , shoulder - scapular periarthritis, syndrome " shoulder - hand" , vertebral artery syndrome , visceral
cardiac syndrome - the so-called " cervical angina ."
Cervical diskalgia accompanied by constant or episodic (as lumbago ) pain in the neck . Pain -
intense, worse after sleep and sharp turns of the neck. Holds the voltage back of the neck muscles
and their callous rigidity. When you hear the crunch of movements ; notes deletion cervical
lordosis , forced the head position of the slope in the direction of the affected disk.
When symptom m. skalenus anterior register voltage eponymous muscle, while the pain
extends from the neck to the head and the type brachialgia - down to the chest, the inner
surface of the shoulder, forearm and wrist to 4 and 5th fingers, so comes malnutrition anterior
scalene muscle. Parallel marked vascular disorders such as swelling of fingers, cyanosis,
decrease in skin temperature of the upper extremity; inclination of the head in the
opposite direction or a show of hands causes the disappearance of the pulse.
Leverage - scapular periarthritis occurs in 23 % of cases. It manifests itself in the form of aching pain in the shoulder joint , with the transition to and shoulder girdle . Diversion
hands above 90 gr. Causes difficulties ; gradually acquires the development of the shoulder girdle muscle atrophy . On radiographs of the shoulder joint markedly local osteoporosis, sometimes you can see the site of calcification m. supraspinatus.
Syndrome " shoulder - hand" Steynbrokera described in 1948 as vegetatively - dystrophic
process , which is closely linked with the shoulder - scapular periarthritis , with shoulder pain combined with pain in the wrist . Occurs as swelling of the fingers , it is difficult mobility in
her joints , leather fingers - smooth, pale - cyanotic , its temperature is lowered. this development becomes muscle wasting and
atrophy of the hand of the palmar aponeurosis . radiographs revealed diffuse osteoporosis bones
of the hand and the humeral head .
Artery syndrome spine ( a.vertebralis ) was first described in 1925 in Barre in the pathogenesis of the syndrome is in first place in the direction of expansion of osteophytes intervertebral foramina , usually disk-level C4-C5 and C5-
C6 , thus there is compression of the spine and sympathetic plexus vertebral artery stenosis . This leads to poor circulation in the cerebellum, brainstem , and
occipital lobes of the brain and the clinical picture appears so - called vertebral - basilar insufficiency . There are headaches that start in the neck and then apply to the
parieto - temporal area. They begin , usually in the morning and increases sharply when moving neck. Sometimes accompanied by pain cochle - vertebral
disorders such as nausea or vomiting, feeling the noise in the head , ringing in the ears , synchronously with puls .
There are so-called " fly " before the eyes, pain in the eyes . It is also possible violation of swallowing , or foreign
body sensation in the throat. Difficulties in the diagnosis of vertebral artery syndrome occur in patients with
hypertension , menopausal neurosis , severe atherosclerosis .
Visceral disorders in osteochondrosis of the cervical spine in the form of cardiogenic syndrome was first described in 1929; arise due to pathological impulses coming from the cervical sympathetic ganglia through the upper, middle and lower
cardiac nerves to the myocardium. Briefly on the differential. the diagnosis of this syndrome
and angina:
─ Pain in osteochondrosis of the cervical spine are localized mainly in the shoulder girdle and between the shoulder blades
with the transition to the heart area, and angina - mostly behind the sternum radiating to the arm, shoulder blade;
─ osteochondrosis by changing the position of the head, hands, pain aggravated by coughing and angina - no.
─ duration of pain in osteochondrosis to 2 hours. , Angina - up to 30 min. ;
─ therapeutic effect of nitroglycerin in osteochondrosis absent, and angina - yes;
─ osteochondrosis no ECG changes, angina , these changes are present ;
─ osteochondrosis range of motion in the cervical spine - limited , and movements themselves are often accompanied by a
characteristic crunch ;
─ osteochondrosis palpable tension and soreness marked paravertebral muscles of the cervical spine ; pain arises in the
percussion of the spinous processes . If angina is not observed .
There is some restriction of mobility of the thoracic , due to the presence of 12 pairs of
ribs, 10 of which are connected to the sternum and the front form the thorax . This
leads to a relatively smaller than in other portions , traumatic thoracic intervertebral
discs. Physiological thoracic kyphosis facilitates the distribution of the load on the front and side surfaces of the disks , so back osteophytes and herniated discs are relatively
rare . For osteochondrosis of the thoracic characteristic so - called hernia SHmorlja
arising from protrusions gelatinous nucleus in adjacent vertebral body to break records
hyaline degenerative changes of the intervertebral disc . Keely Shmorlja
diagnosed radiographically as rounded areas vertebral bone loss , surrounded by strip
sclerosis at closing plates vertebrae.
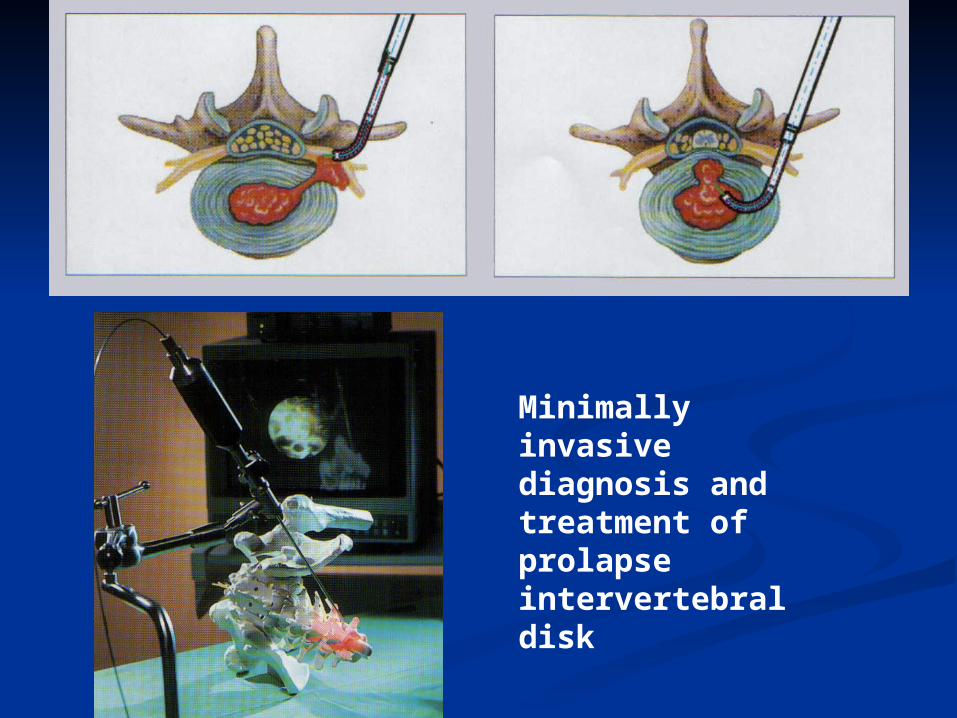
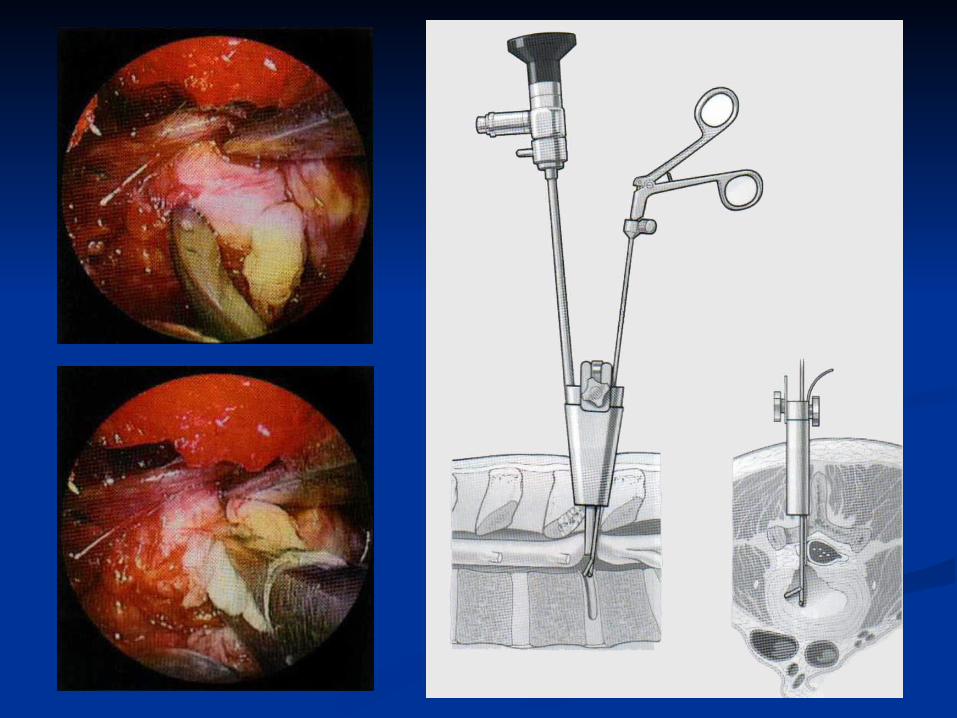
Minimally invasive diagnosis and treatment of prolapse intervertebral disk