Embed Size (px)
Citation preview

Vilnius National Conference for Drug Control, 5 November 2009
EU-Dap/Unplugged:EU-Dap/Unplugged:
an effective school-based program an effective school-based program
for drug use prevention among adolescentsfor drug use prevention among adolescents
Federica Vigna-Taglianti EU-Dap study
Piedmont Centre for Drug Addiction EpidemiologyOED Piemonte, Torino
A.Avogadro University, Novara
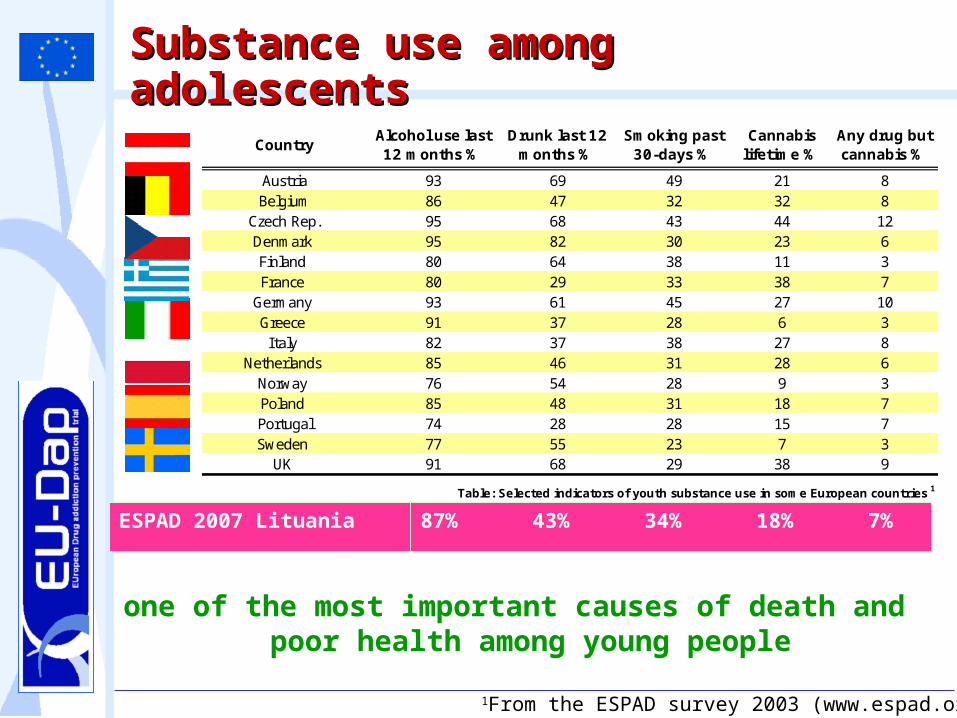
1From the ESPAD survey 2003 (www.espad.org)
one of the most important causes of death and poor health among young people
Substance use among Substance use among adolescentsadolescents
ESPAD 2007 Lituania
CountryAlcohol use last 12 months %
Drunk last 12 months %
Smoking past 30-days %
Cannabis lifetime %
Any drug but cannabis %
Austria 93 69 49 21 8Belgium 86 47 32 32 8
Czech Rep. 95 68 43 44 12Denmark 95 82 30 23 6Finland 80 64 38 11 3France 80 29 33 38 7
Germany 93 61 45 27 10Greece 91 37 28 6 3Italy 82 37 38 27 8
Netherlands 85 46 31 28 6Norway 76 54 28 9 3Poland 85 48 31 18 7Portugal 74 28 28 15 7Sweden 77 55 23 7 3
UK 91 68 29 38 9
Table: Selected indicators of youth substance use in some European countries 1
87% 43% 34% 18% 7%
Prevention interventions are a good public health strategy to reduce the burden of disease due to substance addiction
Prevention Prevention
Prevention strategies:
1. universal prevention targeted to general population as well as to specific
unselected populations (schools, family, community)
2. selective prevention targeted to subsets of the population identified as
having a higher risk of drug use than average
3. indicated prevention which targets those who have already taken drugs and
are considered to be at risk of becoming addicted
Effective PreventionEffective Prevention
No clear evidence is available on effective selective and indicated interventions (ok: family interventions)
Among universal interventions, school-based comprehensive social influence programs are effective
• the effectiveness of interventions is scarcely evaluatedscarcely evaluated
• only few interventions are effectiveeffective
However,
There are evidences that some interventions can make harm (information only, mass-media for drugs)
Negative results: “US Media Campaign”In the US, the effectiveness evaluation of a recent
big mass-media campaign "National Youth "National Youth Anti-Drug Media CampaignAnti-Drug Media Campaign"" (with messages (with messages on TV, radio, andon TV, radio, and newspapers, andnewspapers, and internet internet bannersbanners),), targeted to 12-18 years old youngs and their parents, showed clear “boomerang” effects:
- 3% increase in marijuana usemarijuana use in 14-16 years old youngs
- increase of positive attitudes, intentions to use and first users of marijuana among youngs more exposed to messages (Jacobsohn)
- boomerang effect on peers marijuana useboomerang effect on peers marijuana use
Why effective programs
Why is that important to apply effective programs
2. Ado2. Adollescents are involvedescents are involved (<18 years)
1. Primary prevention intervention: • the target population is healthyhealthy, our aim is
to prevent a risk behaviour (use of drugs) in a population where most people are non-non-usersusers
• the target population did not ask for an intervention
We are responsibWe are responsiblle for adoe for adollescents who start escents who start using drugs because of the interventionusing drugs because of the intervention
Social skills
Normative educationKnowledge
Comprehensive Social Comprehensive Social Influence (CSI) Influence (CSI)
ApproachApproach
CSI approachCSI approach
Development of personal and social skills
Knowledge on risks and consequences of use
Modification of wrong perception of peers and adults substance use and social acceptability
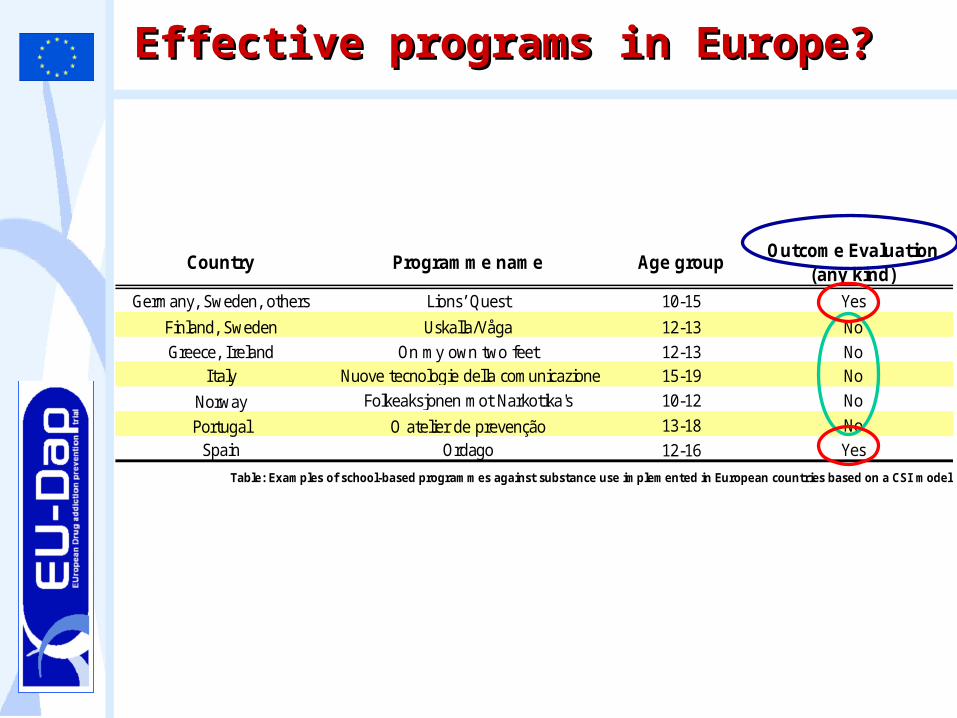
Country Programme name Age groupOutcome Evaluation
(any kind)Germany, Sweden, others Lions’ Quest 10-15 Yes
Finland, Sweden Uskalla/Våga 12-13 NoGreece, Ireland On my own two feet 12-13 No
Italy Nuove tecnologie della comunicazione 15-19 No
Norway Folkeaksjonen mot Narkotika's 10-12 No
Portugal O atelier de prevenção 13-18 NoSpain Ordago 12-16 Yes
Table: Examples of school-based programmes against substance use implemented in European countries based on a CSI model
Effective programs in Europe?Effective programs in Europe?
Characteristics of the EU-Dap Characteristics of the EU-Dap triatriall
Experimental study:
- Cluster Randomized Controlled trial
Funded by the European Community - Public Health Program
Involving 9 centers in 7 European Countries9 centers in 7 European Countries Conceived by an international expert group Supported by EMCDDA
Main aims:• to build a School-based European Prevention
Program (“UnpluggedUnplugged”)• to evaluate the efficacy of the program
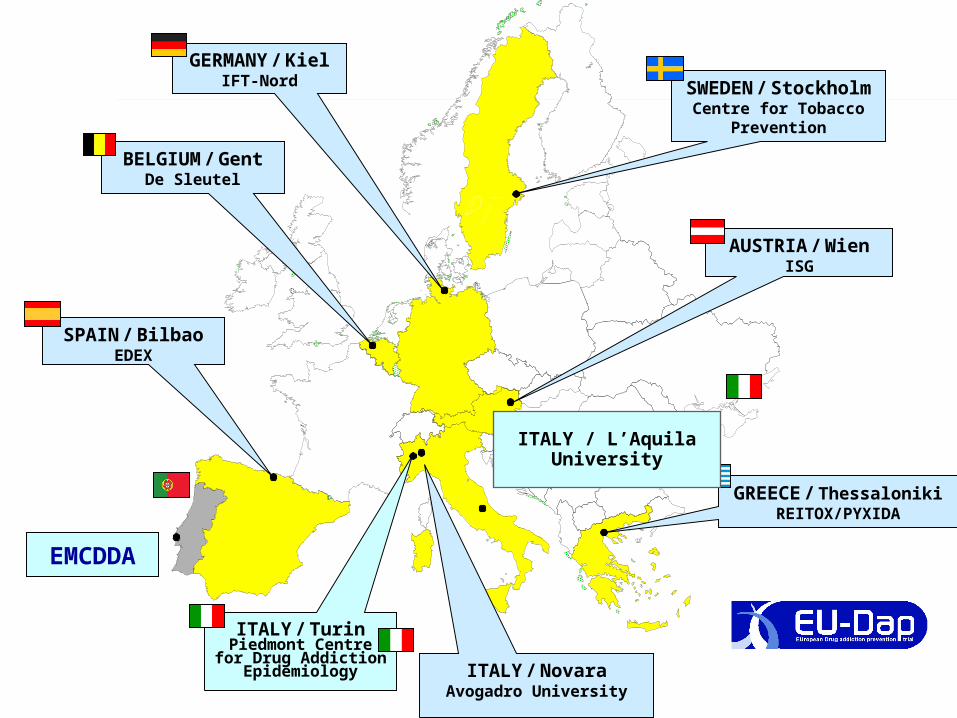
SWEDEN / StockholmCentre for Tobacco
Prevention
SPAIN / BilbaoEDEX
GREECE / ThessalonikiREITOX/PYXIDA
AUSTRIA / WienISG
GERMANY / KielIFT-Nord
BELGIUM / GentDe Sleutel
ITALY / TurinPiedmont Centre
for Drug Addiction Epidemiology
EMCDDA
ITALY / NovaraAvogadro University
ITALY / L’AquilaUniversity
““Unplugged”Unplugged”
• the program is based on a Comprehensive Comprehensive Social Influence Social Influence approach
• It includes the following components– Social skills– Personal skills– Knowledge– Normative education– (resistance education, indirectly)
• It is administered by teachers trained in a 3-days course
• It is made by 12 units, 1 hour each
• It is designed for 12-14 years old students
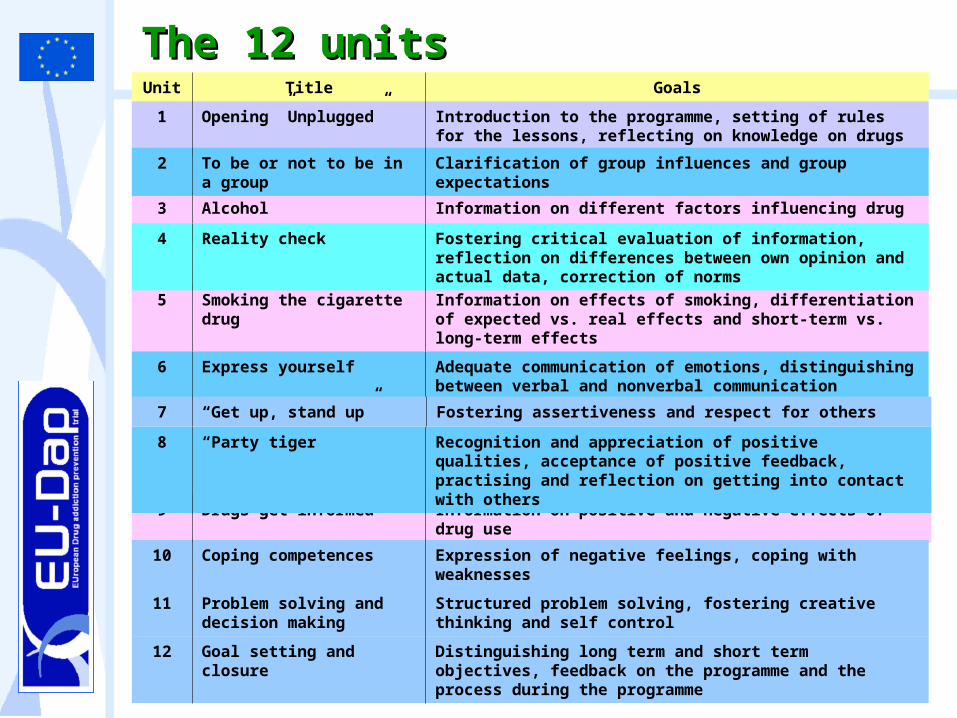
The 12 unitsThe 12 units Unit Title Goals
1 Opening ”Unplugged” Introduction to the programme, setting of rules for the lessons, reflecting on knowledge on drugs
3 Alcohol Information on different factors influencing drug use
5 Smoking the cigarette drug
Information on effects of smoking, differentiation of expected vs. real effects and short-term vs. long-term effects
9 Drugs-get informed Information on positive and negative effects of drug use
2 To be or not to be in a group
Clarification of group influences and group expectations
4 Reality check Fostering critical evaluation of information, reflection on differences between own opinion and actual data, correction of norms
6 Express yourself Adequate communication of emotions, distinguishing between verbal and nonverbal communication
8 “Party tiger” Recognition and appreciation of positive qualities, acceptance of positive feedback, practising and reflection on getting into contact with others
7 “Get up, stand up” Fostering assertiveness and respect for others
10 Coping competences Expression of negative feelings, coping with weaknesses
11 Problem solving and decision making
Structured problem solving, fostering creative thinking and self control
12 Goal setting and closure
Distinguishing long term and short term objectives, feedback on the programme and the process during the programme
Evaluation: enrollmentEvaluation: enrollment
• 7079 students participated in the baseline baseline surveysurvey (November 2004)
• The program (“Unplugged") was administerd between November 2004 and February 2005 in the intervention arms
• 6604 (93%) students participated in the first first follow-up surveyfollow-up survey (May 2005), 3 months (at least) after the end of the program
• 5812 (82%) students participated in the second follow-up surveysecond follow-up survey (May 2006), 15 months (at least) after the end of the program
Self completed anonymousanonymous questionnaire on use of substances, attitudes, knowledge…
– most items retrieved from EDDRA data bankEDDRA data bank– identical for all countries
Procedures for the surveysProcedures for the surveys
Linkage between pre- and post-test by a self self generated codegenerated code based on fixed data (some letters from name of parents, date of birth..)
the reliabilityreliability was tested in a pilot study (Galanti 2006, Preventive Medicine)
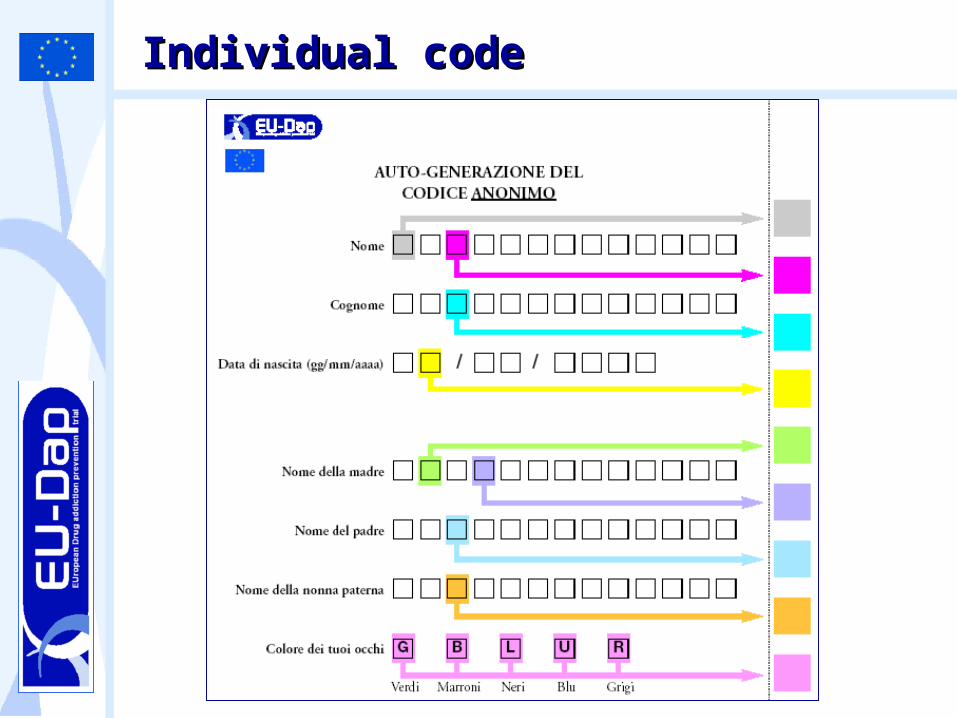
Individual codeIndividual code
The questionnaireThe questionnaire
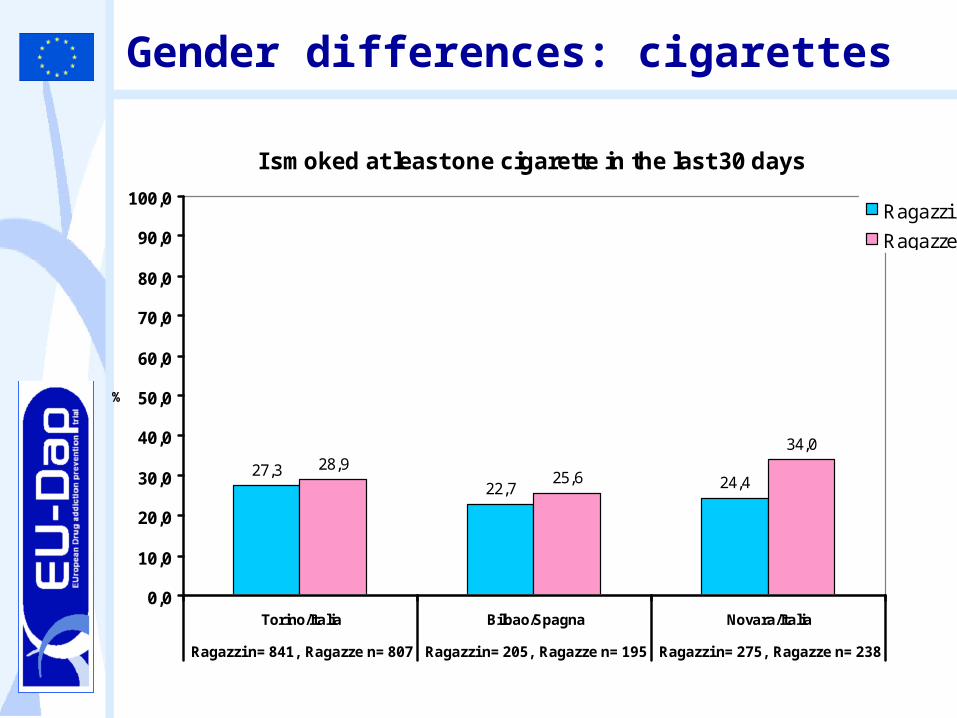
Gender differences: cigarettes
I smoked at least one cigarette in the last 30 days
27,322,7 24,4
28,925,6
34,0
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
100,0
Torino/Italia Bilbao/Spagna Novara/Italia
Ragazzi n= 841, Ragazze n= 807 Ragazzi n= 205, Ragazze n= 195 Ragazzi n= 275, Ragazze n= 238
%
Ragazzi
Ragazze

Drunkenness episodes
I've been drunk at least ONCE in the last 30 days
11,917,3
10,57,6
18,410,9
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
100,0
Torino/Italia Bilbao/Spagna Novara/Italia
Ragazzi n= 841, Ragazze n=807
Ragazzi n= 205, Ragazze n=195
Ragazzi n= 275, Ragazze n=238
%
RagazziRagazze
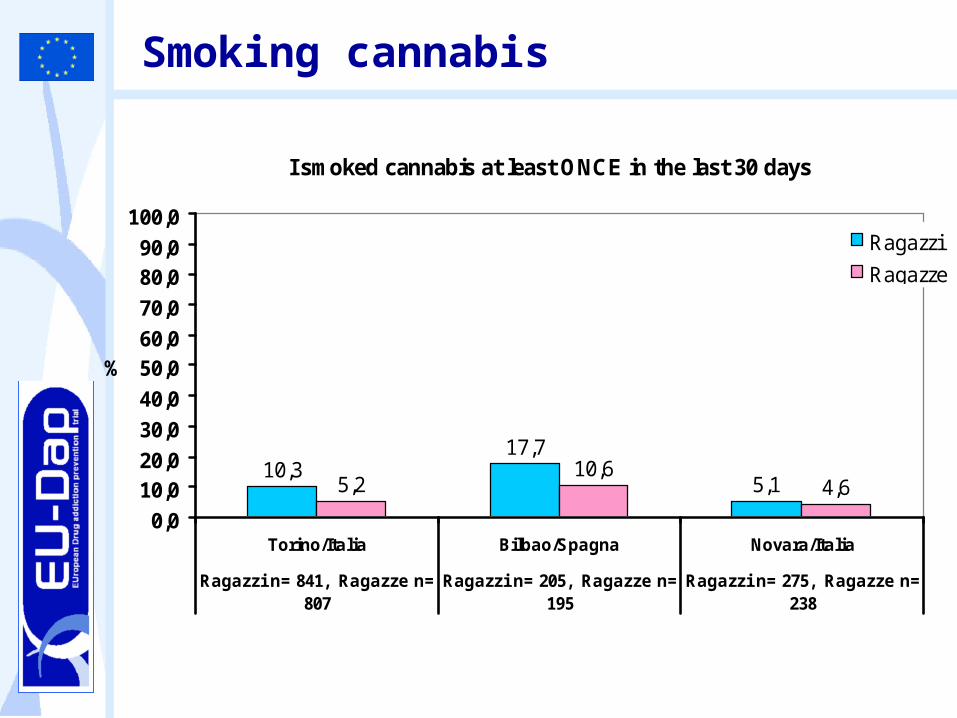
Smoking cannabis
I smoked cannabis at least ONCE in the last 30 days
10,317,7
5,15,210,6
4,6
0,0
10,020,0
30,0
40,0
50,060,0
70,0
80,090,0
100,0
Torino/Italia Bilbao/Spagna Novara/Italia
Ragazzi n= 841, Ragazze n=807
Ragazzi n= 205, Ragazze n=195
Ragazzi n= 275, Ragazze n=238
%
Ragazzi
Ragazze
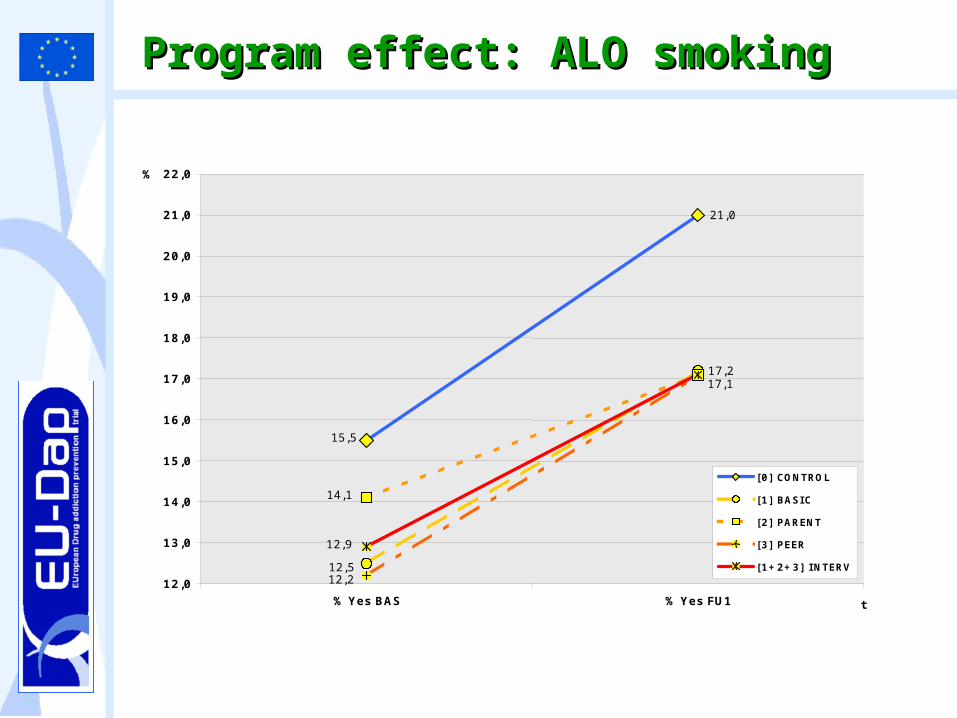
Program effect: ALO smokingProgram effect: ALO smoking
21,0
17,2
15,5
12,5
14,1
12,2
17,1
12,9
12,0
13,0
14,0
15,0
16,0
17,0
18,0
19,0
20,0
21,0
22,0
% Yes BAS % Yes FU1 t
%
[0] CONTROL [1] BASIC [2] PARENT [3] PEER [1+2+3] INTERV
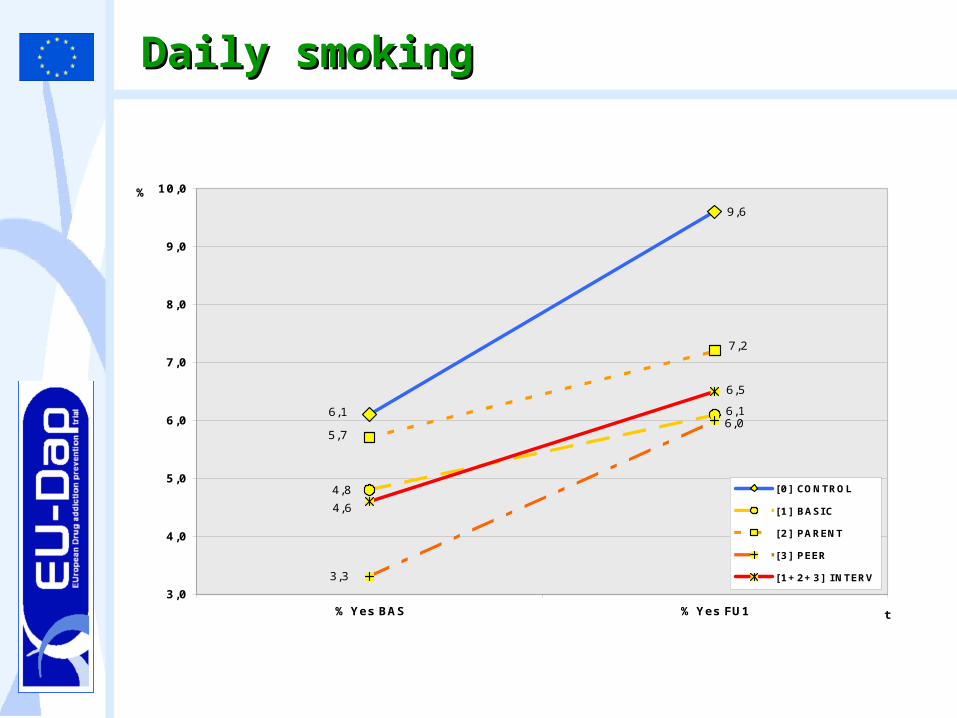
Daily smokingDaily smoking
9,6
6,1 6,1
4,8
7,2
5,7 6,0
3,3
6,5
4,6
3,0
4,0
5,0
6,0
7,0
8,0
9,0
10,0
% Yes BAS % Yes FU1 t
%
[0] CONTROL [1] BASI C [2] PARENT [3] PEER [1+2+3] I NTERV
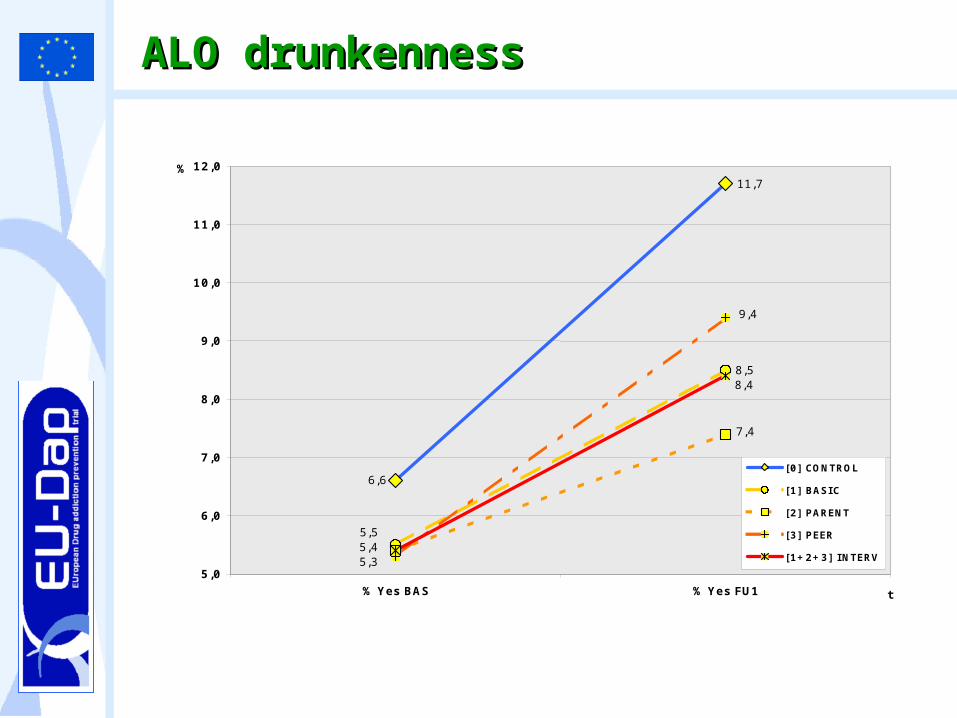
ALO drunkennessALO drunkenness
11,7
8,5
6,6
5,5
7,4
5,3
9,4
8,4
5,4 5,0
6,0
7,0
8,0
9,0
10,0
11,0
12,0
% Yes BAS % Yes FU1 t
%
[0] CONTROL [1] BASI C [2] PARENT [3] PEER [1+2+3] I NTERV
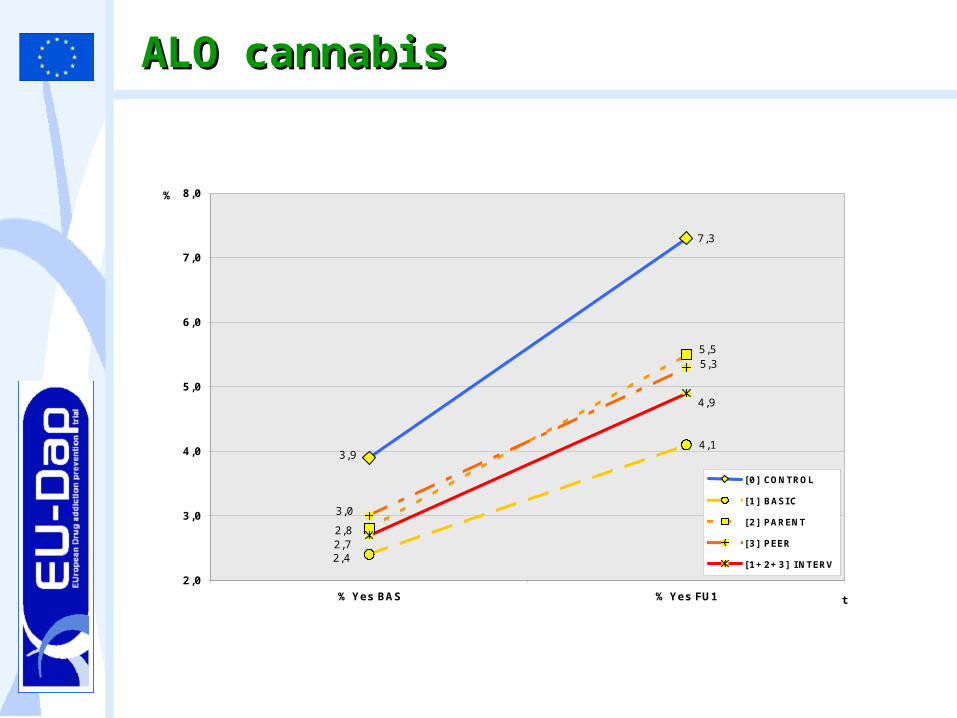
ALO cannabisALO cannabis
7,3
3,9 4,1
2,4
5,5
2,8
5,3
3,0
4,9
2,7
2,0
3,0
4,0
5,0
6,0
7,0
8,0
% Yes BAS % Yes FU1 t
%
[0] CONTROL [1] BASI C [2] PARENT [3] PEER [1+2+3] I NTERV

Adjusted statistical analysisAdjusted statistical analysis
• A Multi-Level model was used to:
– Adjust for the cluster effect cluster effect (cluster RCT: the unit of the randomization is the class, but the unit of the analysis is the student)
– Take into account the differences in the differences in the prevalence of use among centersprevalence of use among centers
– Take into account the differences in the differences in the prevalence of use among arms prevalence of use among arms (the controls show higher prevalences of use at the baseline)
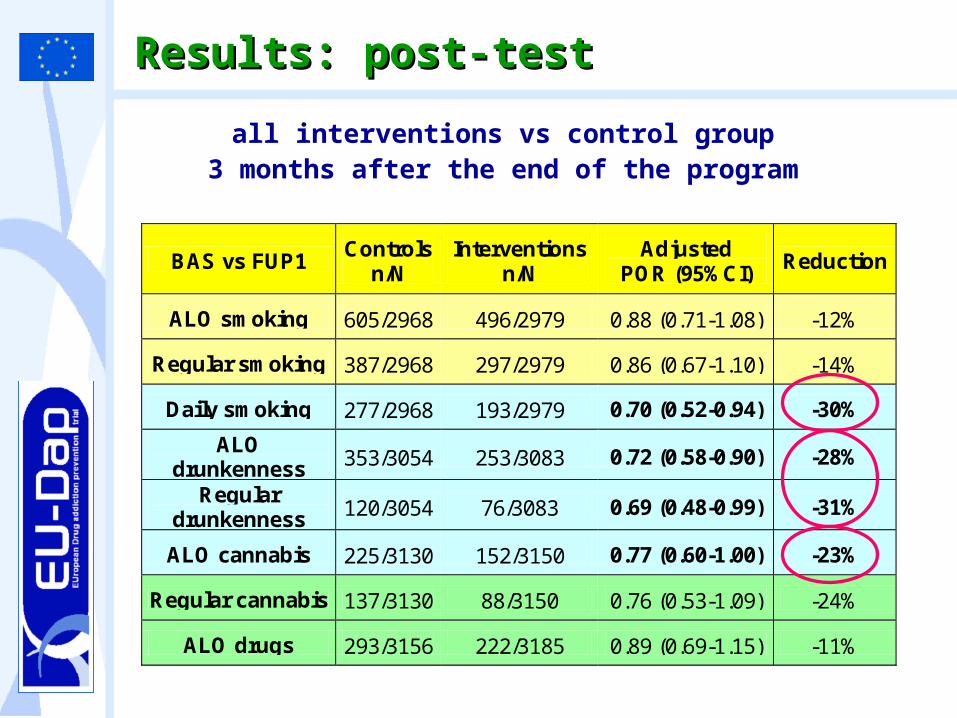
Results: post-testResults: post-test
all interventions vs control group 3 months after the end of the program
BAS vs FUP1 Controls
n/N Interventions
n/N Adjusted
POR (95%CI) Reduction
ALO smoking 605/2968 496/2979 0.88 (0.71-1.08) -12%
Regular smoking 387/2968 297/2979 0.86 (0.67-1.10) -14%
Daily smoking 277/2968 193/2979 0.70 (0.52-0.94) -30%
ALO drunkenness 353/3054 253/3083 0.72 (0.58-0.90) -28%
Regular drunkenness 120/3054 76/3083 0.69 (0.48-0.99) -31%
ALO cannabis 225/3130 152/3150 0.77 (0.60-1.00) -23%
Regular cannabis 137/3130 88/3150 0.76 (0.53-1.09) -24%
ALO drugs 293/3156 222/3185 0.89 (0.69-1.15) -11%
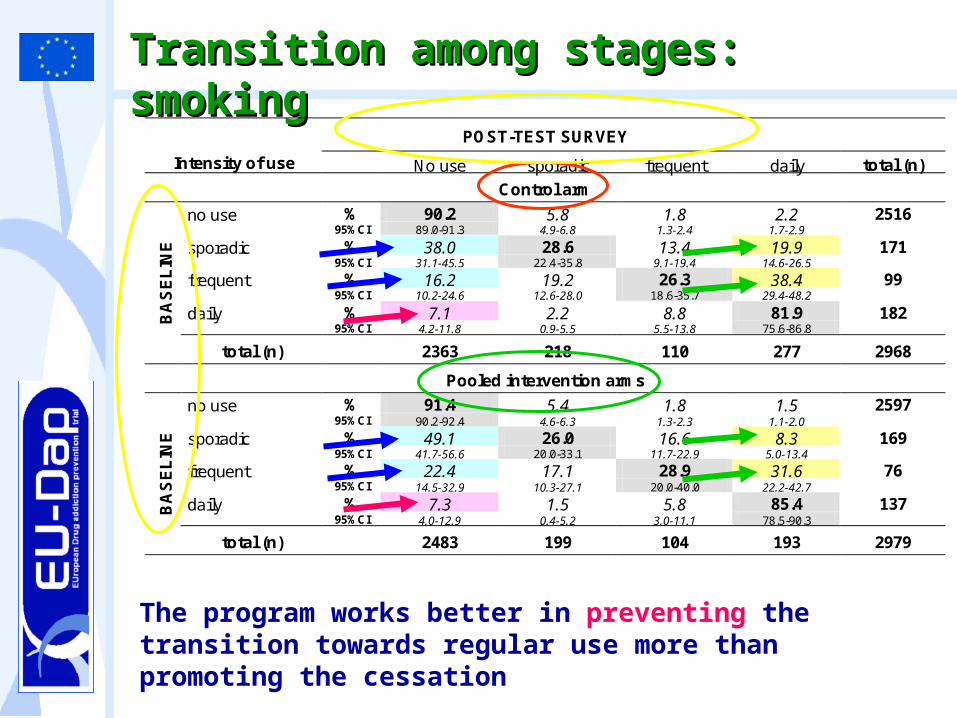
The program works better in preventing the transition towards regular use more than promoting the cessation
Transition among stages: Transition among stages: smokingsmoking
POST-TEST SURVEY
Intensity of use No use sporadic frequent daily total (n)
Control arm
no use % 90.2 5.8 1.8 2.2 2516 95%CI 89.0-91.3 4.9-6.8 1.3-2.4 1.7-2.9
sporadic % 38.0 28.6 13.4 19.9 171 95%CI 31.1-45.5 22.4-35.8 9.1-19.4 14.6-26.5
frequent % 16.2 19.2 26.3 38.4 99 95%CI 10.2-24.6 12.6-28.0 18.6-35.7 29.4-48.2
daily % 7.1 2.2 8.8 81.9 182 95%CI 4.2-11.8 0.9-5.5 5.5-13.8 75.6-86.8 B
AS
EL
INE
total (n) 2363 218 110 277 2968
Pooled intervention arms
no use % 91.4 5.4 1.8 1.5 2597 95%CI 90.2-92.4 4.6-6.3 1.3-2.3 1.1-2.0
sporadic % 49.1 26.0 16.6 8.3 169 95%CI 41.7-56.6 20.0-33.1 11.7-22.9 5.0-13.4
frequent % 22.4 17.1 28.9 31.6 76 95%CI 14.5-32.9 10.3-27.1 20.0-40.0 22.2-42.7
daily % 7.3 1.5 5.8 85.4 137 95%CI 4.0-12.9 0.4-5.2 3.0-11.1 78.5-90.3 B
AS
EL
INE
total (n) 2483 199 104 193 2979
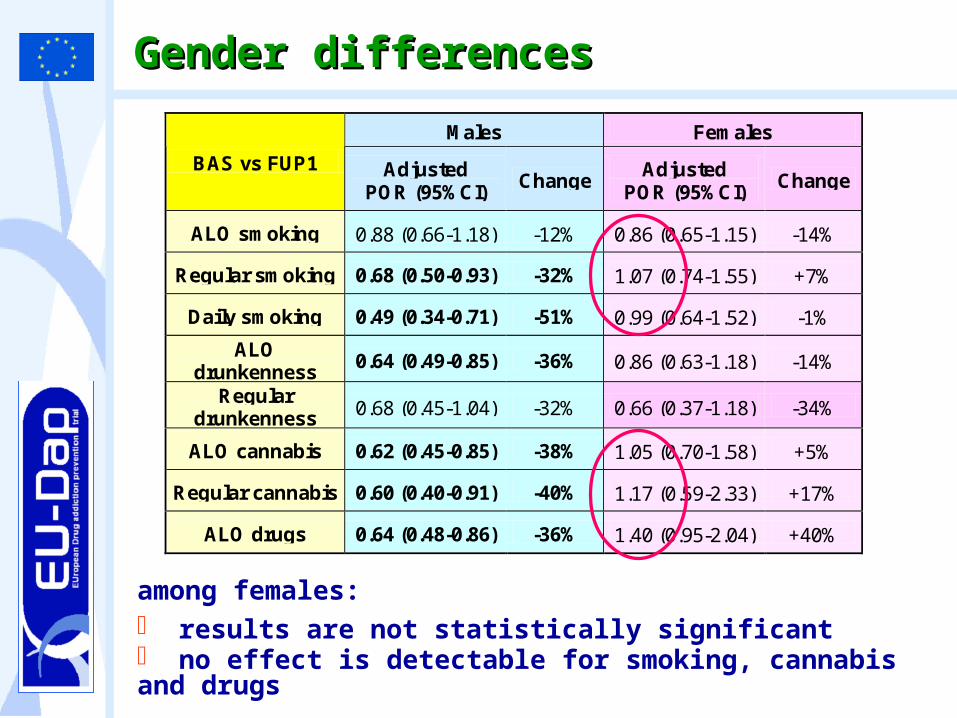
Gender differencesGender differences
among females: results are not statistically significant no effect is detectable for smoking, cannabis and drugs
Males Females
BAS vs FUP1 Adjusted POR (95%CI)
Change Adjusted
POR (95%CI) Change
ALO smoking 0.88 (0.66-1.18) -12% 0.86 (0.65-1.15) -14%
Regular smoking 0.68 (0.50-0.93) -32% 1.07 (0.74-1.55) +7%
Daily smoking 0.49 (0.34-0.71) -51% 0.99 (0.64-1.52) -1%
ALO drunkenness
0.64 (0.49-0.85) -36% 0.86 (0.63-1.18) -14%
Regular drunkenness 0.68 (0.45-1.04) -32% 0.66 (0.37-1.18) -34%
ALO cannabis 0.62 (0.45-0.85) -38% 1.05 (0.70-1.58) +5%
Regular cannabis 0.60 (0.40-0.91) -40% 1.17 (0.59-2.33) +17%
ALO drugs 0.64 (0.48-0.86) -36% 1.40 (0.95-2.04) +40%
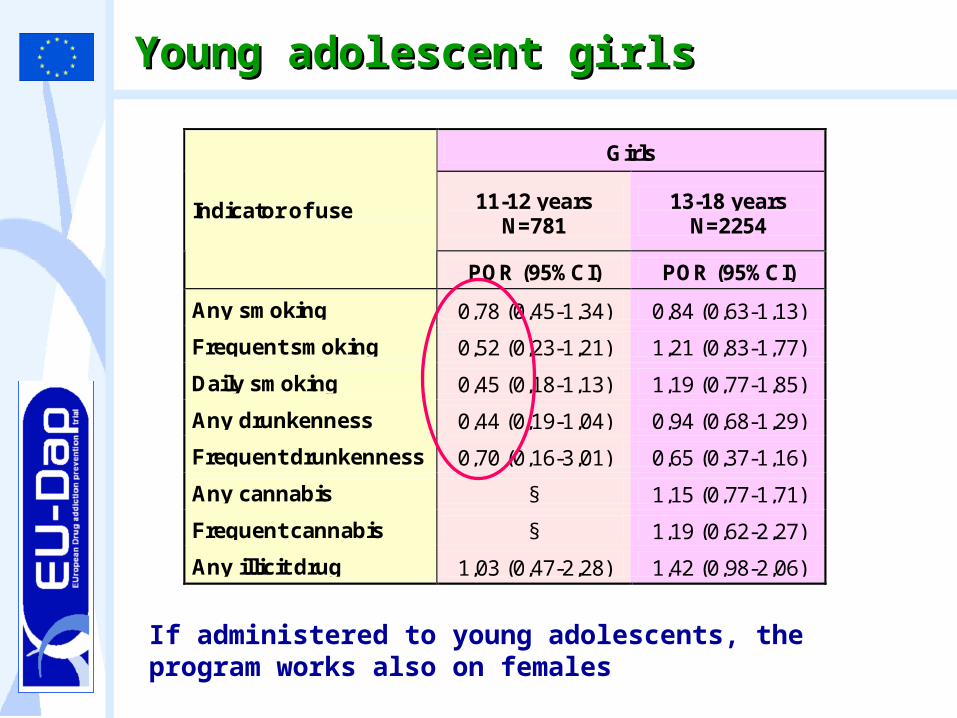
Young adolescent girlsYoung adolescent girls
If administered to young adolescents, the program works also on females
Girls
11-12 years N=781
13-18 years N=2254
Indicator of use
POR (95%CI) POR (95%CI)
Any smoking 0,78 (0,45-1,34) 0,84 (0,63-1,13)
Frequent smoking 0,52 (0,23-1,21) 1,21 (0,83-1,77)
Daily smoking 0,45 (0,18-1,13) 1,19 (0,77-1,85)
Any drunkenness 0,44 (0,19-1,04) 0,94 (0,68-1,29)
Frequent drunkenness 0,70 (0,16-3,01) 0,65 (0,37-1,16)
Any cannabis § 1,15 (0,77-1,71)
Frequent cannabis § 1,19 (0,62-2,27)
Any illicit drug 1,03 (0,47-2,28) 1,42 (0,98-2,06)
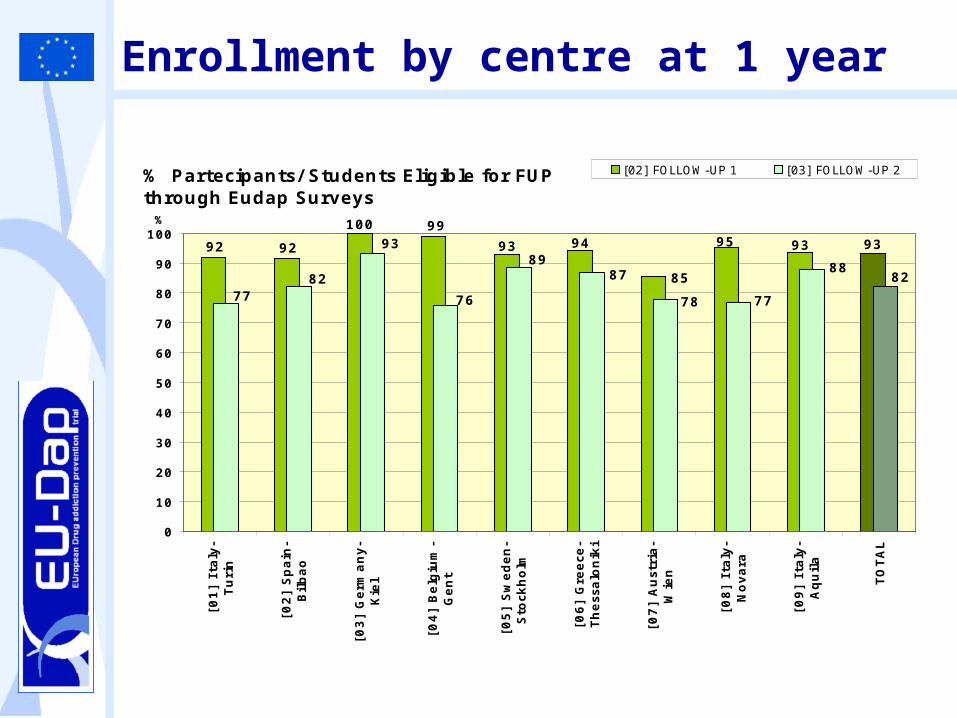
Enrollment by centre at 1 year
% Partecipants/ Students Eligible for FUP through Eudap Surveys
939395
85
9493
99100
9292
7782
93
76
89
77
8882
78
87
0
10
20
30
40
50
60
70
80
90
100
[01
] It
aly
-Tu
rin
[02
] S
pain
-B
ilbao
[03
] G
erm
an
y-
Kie
l
[04
] B
elg
ium
-G
en
t
[05
] S
weden
-S
tockh
olm
[06
] G
reece-
Th
essalo
nik
i
[07
] A
ustr
ia-
Wie
n
[08
] It
aly
-N
ovara
[09
] It
aly
-A
qu
ila
TO
TA
L
%
[02] FOLLOW-UP 1 [03] FOLLOW-UP 2
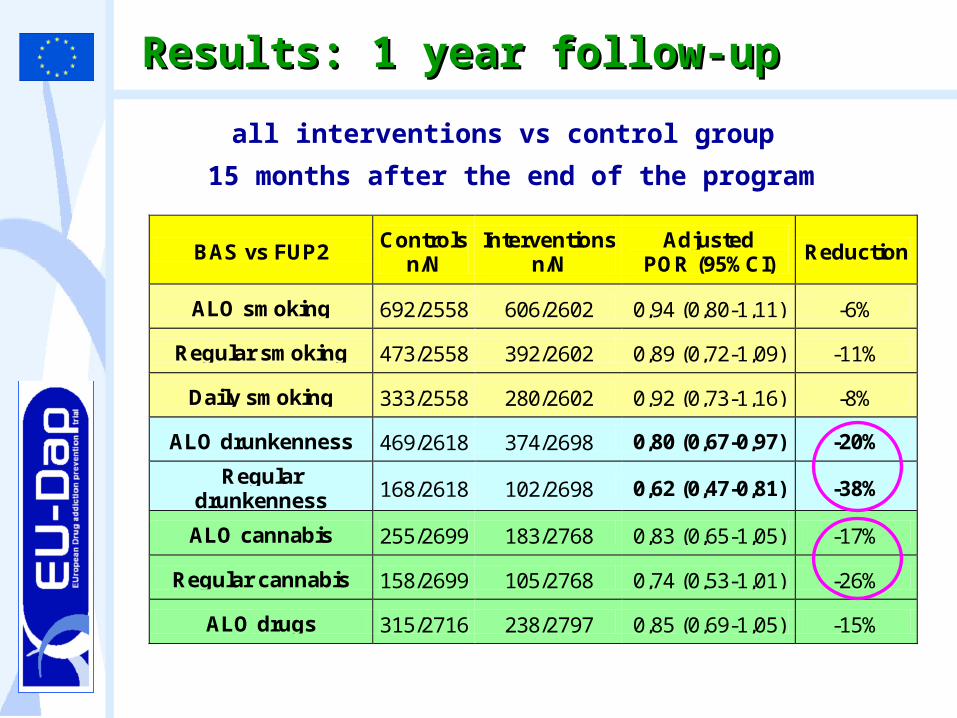
Results: 1 year follow-upResults: 1 year follow-up
all interventions vs control group
15 months after the end of the program
BAS vs FUP2 Controls
n/N Interventions
n/N Adjusted
POR (95%CI) Reduction
ALO smoking 692/2558 606/2602 0,94 (0,80-1,11) -6%
Regular smoking 473/2558 392/2602 0,89 (0,72-1,09) -11%
Daily smoking 333/2558 280/2602 0,92 (0,73-1,16) -8%
ALO drunkenness 469/2618 374/2698 0,80 (0,67-0,97) -20%
Regular drunkenness 168/2618 102/2698 0,62 (0,47-0,81) -38%
ALO cannabis 255/2699 183/2768 0,83 (0,65-1,05) -17%
Regular cannabis 158/2699 105/2768 0,74 (0,53-1,01) -26%
ALO drugs 315/2716 238/2797 0,85 (0,69-1,05) -15%
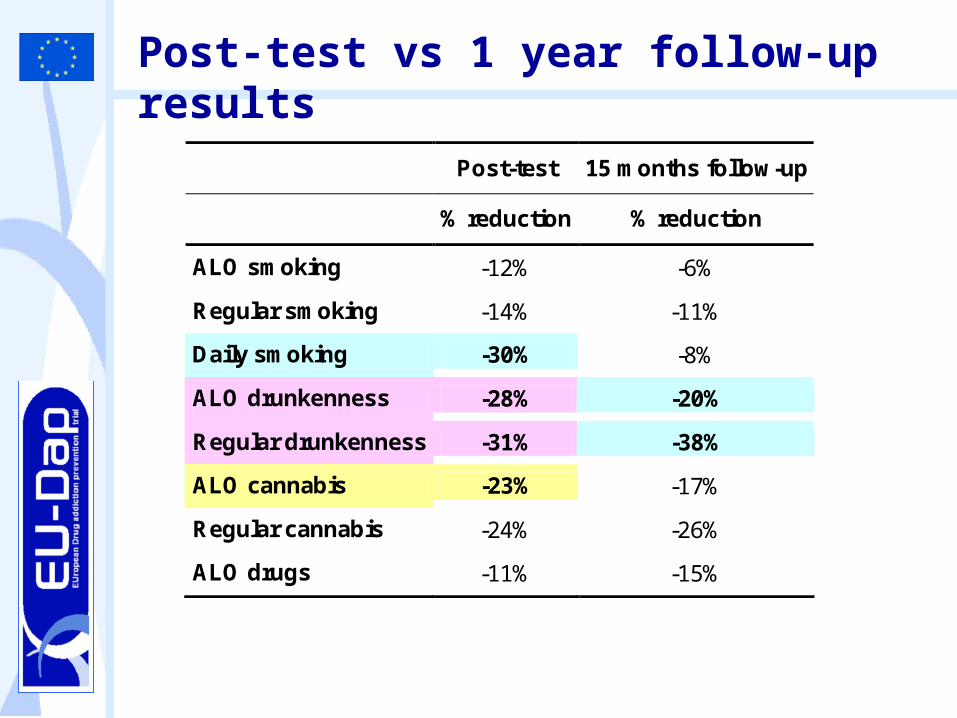
Post-test vs 1 year follow-up results
Post-test 15 months follow-up
% reduction % reduction
ALO smoking -12% -6%
Regular smoking -14% -11%
Daily smoking -30% -8%
ALO drunkenness -28% -20%
Regular drunkenness -31% -38%
ALO cannabis -23% -17%
Regular cannabis -24% -26%
ALO drugs -11% -15%
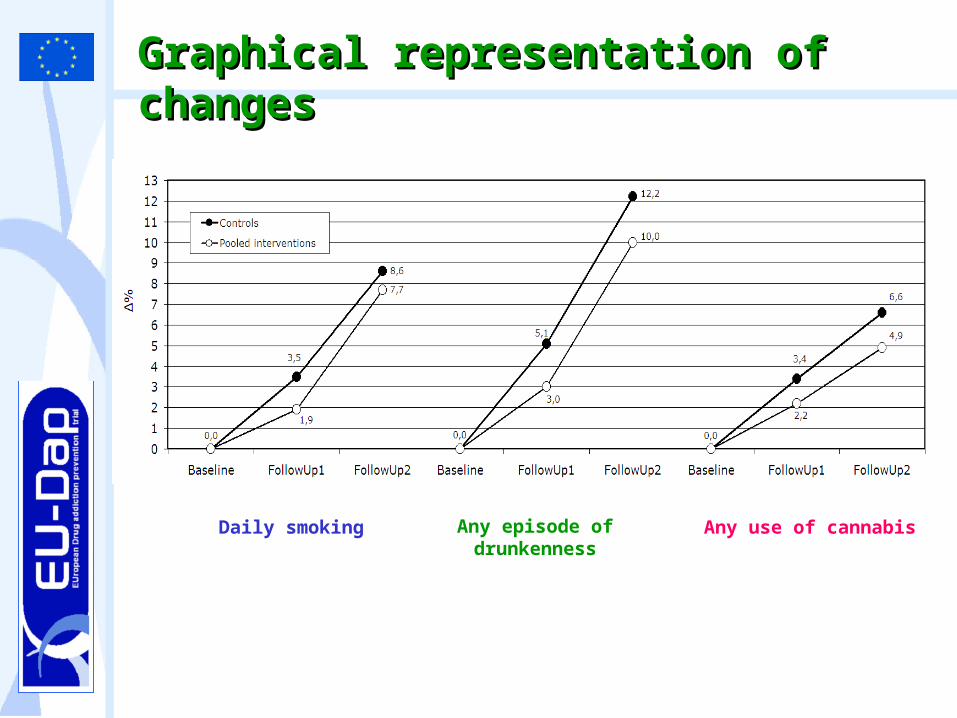
Graphical representation of Graphical representation of changeschanges
Daily smoking Any episode of drunkenness
Any use of cannabis
Conclusions on the effectConclusions on the effect
The statistical analysis shows that UnpluggedUnplugged is effective in reducing use of drugs, alcohol and cigarettes at the post-testand the results are maintained for alcohol alcohol (and cannabiscannabis) at 1 year follow-up
The program works better in preventing the usepreventing the use more than promoting cessation
Since there are gender differencesgender differences in the effectiveness, it is recommended to administer the program to early adolescents (less than 14 years old)

Implementation of UnitsImplementation of Units
Experimental version of the Unplugged program
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12
Core Units
% c
lass
es
Partial
Complete
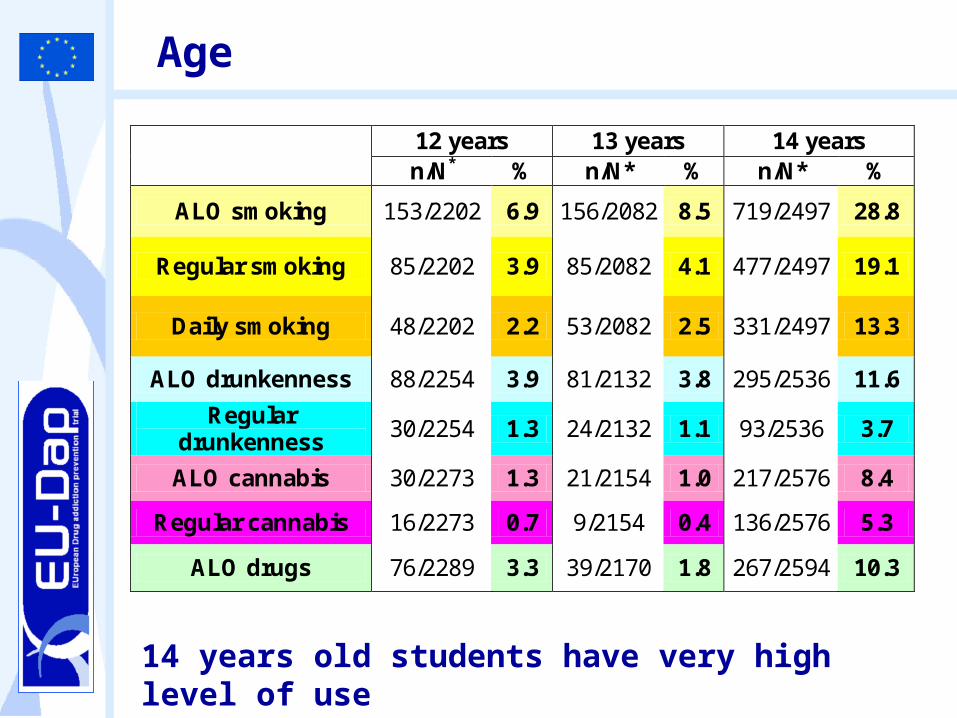
Age
12 years 13 years 14 years n/N* % n/N* % n/N* %
ALO smoking 153/2202 6.9 156/2082 8.5 719/2497 28.8
Regular smoking 85/2202 3.9 85/2082 4.1 477/2497 19.1
Daily smoking 48/2202 2.2 53/2082 2.5 331/2497 13.3
ALO drunkenness 88/2254 3.9 81/2132 3.8 295/2536 11.6
Regular drunkenness
30/2254 1.3 24/2132 1.1 93/2536 3.7
ALO cannabis 30/2273 1.3 21/2154 1.0 217/2576 8.4
Regular cannabis 16/2273 0.7 9/2154 0.4 136/2576 5.3
ALO drugs 76/2289 3.3 39/2170 1.8 267/2594 10.3
14 years old students have very high level of use
The Guide is a tool for
a. Policy makers (Chapter 1)
b. Headmasters (Chapter 2)
c. Teachers (Chapter 3)
to disseminate and implement CSI programs in the schools
Practical tools are provided in each chapter to choose, plan, implement and evaluate the implementation of the program
Suggestions for implementationSuggestions for implementation
Steps to followSteps to follow
• Ministry of Education mandate, promote and/or coordinate
• School autonomy to choose to implement a CSI programme
• Regional authorities promote and coordinate
• Schools use consultative processes which involve teachers, parents & pupils
• Motivated teachers to lead or manage the programme
• Schools have an established tradition of prevention activities or have set a mission statement or goal to do so
Conducting an environment assessment
GETTING STARTED
SEE T
OO
L N
. 1
Cri
teri
a t
o c
on
sid
er
wh
en
ch
oosin
g a
CS
I p
rog
ram
Gu
ide:
Ch
ap
ter
2G
uid
e:
Ch
ap
ter
2
The environment attitude towards tobacco/alcohol and substance use and towards prevention interventions has to be considered (post-pone/create)
Steps to followSteps to follow
• Engage parents to support the programme.
• Investigate funds available from the Ministry, Region, School Budget.
• Ensure materials for teachers and students are available.
Gathering resources to implement a CSI programme
IMPLEMENTING
SEE T
OO
L N
. 2
Tip
s fo
r ra
isin
g
fun
ds
Getting organized to implement a CSI programme
• Schedule and organize the programme’s implementation on the school calendar.
•Support Teachers’ continuing education in legislation. Allow teachers to attend training, should it be available, or organize a training for teachers by allowing those that have taught prevention programmes to act as trainers. S
EE T
OO
L N
. 3
Org
aniz
e a
teac
her
tr
ain
ing
Gu
ide:
Ch
ap
ter
2G
uid
e:
Ch
ap
ter
2
Steps to followSteps to follow
• Teachers can adopt the role as trainers.
• Teachers are motivated to accurately implement all sessions of the programme in the foreseen sequence.
• Parents are interested in the continuation of prevention activities and ask the school to annually implement them
• Adopt the programme to take place as core curriculum within one or more subjects.
• Funding by Ministry set aside for implementation.
• Surveil the program’s implementation and suggest how to improve upon it.
Maintaining quality in CSI programmes
SUSTAINING
SEE T
OO
L N
. 4
Co
nd
uct
a q
ual
ity
con
tro
l as
sess
men
t
Gu
ide:
Ch
ap
ter
2G
uid
e:
Ch
ap
ter
2
Sustaining the implementation of the program across years is important (inequalities/context/effectiveness)
Ongoing activities
In 2006, the EC funded a second phase of the project (EU-Dap2EU-Dap2), aimed to the dissemination of effective prevention programs
PolandPoland and Czech RepublicCzech Republic joined the project as new implementing countriesthe GuideGuide to successful implementation of CSI to successful implementation of CSI curricula in schoolscurricula in schools has been published
www.eudap.net
PublicationsPublications on the effect of the program are now available on Pubmed/International Journals
New projectsNew projects are ongoing with the collaboration of Mentor Foundation
Mentor Lithuania is involved… together with Russia, Romania, Croatia and Kyrgyzstan