Embed Size (px)
Citation preview

26. Diagnosis?
a. Monomorphic VT (MMVT)b. Polymorphic VT (PMVT)c. MMVT degenerating into PMVTd. Atrial fibrillation with WPW syndrome
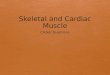
The correct answer is ‘C’- MM VT degenerating into PM VT.The first 3 QRS complexes are the same. After that (see lead aVF) there is transition towidely changing, irregular QRS complexes. First one should look into the clinical profile.This was a 72 year old man with an old myocardial infarction, moderate LV dysfunction,no reversible ischemia and recent unexplained syncope. The VT shown here was inducedduring an EP study. The PMVT soon degenerated into VF (Fig. 1b); this was terminated bydefibrillation (Fig. 1c).Fig. 1b: MMVT → PMVT → VF

Fig. 1c: Defibrillation terminates VF, followed by bradycardia (normal sinus rhythm returnedwithin a few seconds)
The highly probable cause for the syncope was a transient ventricular arrhythmia. The patientwas at high risk for sudden death. He therefore received an ICD (implantable cardioverter-defibrillator)
27. 48 yr. old lady, recent re-do mitral valve replacement. Shifted to room. Hadsyncope, following which this ECG was recorded.
Likely cause of syncope?

a. Torsade de pointesb. Bradycardiac. Hypotensiond. Atrial fibrillation with rapid ventricular rate
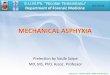
The correct answer is ‘A’ - TdP.The basic rhythm is atrial fibrillation (almost appearing like atrial flutter in lead V2) with a slowventricular rate. The T waves are inverted in leads I, II, aVL, aVF and prominently so in leads V3-V6.Importantly, the QT interval is markedly prolonged, measuring at least 600 ms in lead V4.PVCs are seen coming towards the end of the T wave (note the last PVC is before the end of the Twave). Such R-on-T PVCs, coming during the vulnerable phase (latter half of repolarisation) areominous in the setting of QT prolongation.Fig. 2b: Soon after shifting back to ICCU…
Torsade de pointes! (TdP)Later, the QT remained normal.QT prolongation after valve surgery should prompt a search for the following factors:• Hypokalemia• Hypomagnesemia• Amiodarone use for atrial fibrillation• Hypothermia• Aggressive diuretic use• Antibiotics known to prolong QTFig. 2c: I.V. Magnesium given, isoprenaline infusion started… The ventricular rate has picked up,the QT has normalised

28. 17 yr. old girl
a. SVTb. VT with VA dissociationc. Preexcited tachycardiad. None of the above
The correct answer is ‘D’ – None of the aboveThere is a regular wide QRS tachycardia @ 180/min. The QRS shows a qR pattern (RBBB-like)in lead V1. The rS pattern in V6 in this setting favours VT. This diagnosis is strengthened by thenorthwest axis of -100 0 (dominant broad R in aVR).The P waves can be picked out carefully in lead III (Fig. 3b).
29. 65-year-old man with a “heart attack” several years ago

The rhythm is:
a. Sinus tachycardiab. Atrial tachycardiac. VT with AV dissociationd. VT with retrograde conduction
The correct answer is ‘a’The T waves in lead II are peaked indicative of positive P waves, suggesting sinus tachycardia.The ECG at normal heart rate recorded later was as follows:
This showed that this was a regular LBBB-type wide QRS tachycardia.In wide QRS tachycardia in a patient with an old MI, the diagnosis is VT, until proved otherwise. Thiscase was an exception to the rule.
30.39 yr. old obese lady. Recurrent low feeling with fatigue.

There is:a. Sinus node dysfunctionb. AV blockc. Both A and B
The correct answer is ‘a’ – Sinus node dysfunction (SND)The ECG shows a long sinus arrest of 3.6 seconds. During this, no P wave is seen. Otherwise,there is bradycardia. Every P wave is connected with a normal PR interval. Hence, there is noAV block. The symptoms are most likely because of SND. Hence an ‘atrial-based pacemaker’seems necessary.A 24-hour Holter and a treadmill stress test are useful for decision-making in borderline cases.Figure 1 (a) shows the ECG after a permanent pacemaker. The patient had 1:1 AV conductionwhen atrium was paced upto 180 bpm. Hence, an AAIR pacemaker was implanted with reliefof symptoms.All the complexes here show a pacing spike prior to the P wave. In one complex, the pacingstimulus is seen only in lead V2 (↓) because of respiratory variation causing difference in pacingspike amplitude.Fig 1 A

31.27 year old man. 3 episodes of rapid palpitations with near-syncope/syncope. WideQRS tachycardia documented. Currently he is on amiodarone and metoprolol.
a. Supraventricular tachycardia (SVT) with left bundle branch block (LBBB)b. Idiopathic Right ventricular outflow tract (RVOT) VTc. Arrhythmogenic right ventricular dysplasia (ARVD)
2The correct answer is ‘c’ – ARVDThe ECG above shows a regular wide QRS (QRS=135 ms) tachycardia @ 170 bpm. The markedfluctuation in the T waves in long lead II along with the occasional ‘P’ waves (*) strongly suggest VAdissociation.Moreover, the LBBB like morphology, the negative QRS in V1 along with right axis deviation (QRSaxis=120°) is another hall-mark of VT arising from the RVOT.

The sinus rhythm ECG is abnormal, with T inversion in V1-V3 and low limb lead voltages. This isconsistent with ARVD. Sinus bradycardia and PR prolongation could be because of anti-arrhythmicdrugs. This patient’s echocardiogram showed a mildly dilated RV with outpouchings. The cardiac MRIconfirmed these findings.This patient is at high risk of sudden death and syncope and needs an ICD.
32. 75 yr. old lady with 2 yr. H/O recurrent rapid palpitations, occasionally with syncope
a. SVTb. VTc. S VT and VT
The correct answer is ‘a’ – SVTTop panelThe upper strip shows onset of tachycardia with a PAC (*) along with a prolonged PR interval. After thisduring the “tachycardia” (ventricular rate 96 bpm) a P’ wave is seen exactly between 2 QRS complexes.Note that these QRS complexes have a prominent R’ in the first channel () which is not seen duringsinus rhythm. this R’ strongly suggests an additional P wave.Bottom panel

There is a transition to a faster wide QRS tachycardia. Note that the RR durations are now exactly half.Thus, the SVT showed 2:1 AV conduction which changed to 1:1 AV conduction with rate-related bundlebranch block.This SVT is most likely slow-fast AV nodal re-entry tachycardia.
The arrowheads are of equal length
33. 45 yr. old man; unexplained syncope. Brother had died suddenly
Examination, echocardiogram normal. What next?a. Holterb. Coronary angiographyc. E P studyd. ICDThe correct answer is ‘d’ – ICD.The limb leads show an indeterminate QRS axis and PR prolongation (240 ms). Lead V1 andV2 suggest an incomplete RBBB pattern along with marked convex ST elevation. This is aclassical Type I Brugada pattern. In view of the ‘malignant’ history, this patient has Brugadasyndrome and is at a high risk of SCD due to VT/VF. Unfortunately, there is no reliable testto prognosticate and there is no effective drug therapy. Therefore, an ICD (preferably dual

chamber in view of AV delay) becomes mandatory.However, the patient and his family requested if any further studies could be done to be certainabout the diagnosis. Therefore, provocative testing with IV flecainide was performed along withan EP study. Such maneuvers do have a reasonable positive predictive value. Figure 1a showsthe gross QRS widening with flecainide, along with easy inducibility of VF. Subsequently, thepatient underwent a dual-chamber ICD implantation.
34. 48 yr. old man. Asymptomatic. “Routine” stress test….Figure 2

Figure 2a

a. Artifactual traceb. Sinus tachycardia with LBBBc. SVTd. VT
The correct answer is ‘b’There is an increase in the ventricular rate to 166 bpm with exercise along with widening of the QRScomplex, The QRS resembles the LBBB pattern and has a sharp initial downstroke in lead V1. WhileP waves are not clearly seen, careful observation in lead II suggests that the P wave merges with thedownslope of the T wave.Artifactual waveforms are not uncommon with ‘Linked Median’ software manipulation as seen in manystress test machines. These are done to make the ECG look free of noise but, are a distortionand should be avoided. The typical exercise-induced VF has a RVOT origin with LBBB-like pattern (butwith a slow downstroke in lead V1) and right axis deviation.The simplest way to confirm the diagnosis of rate-related LBBB would be to observe that the onset andtermination of LBBB occurs in conjunction with a change in heart rate. Figure 2b shows that as the heartrate settles, the LBBB disappears.Figure 2b 30 seconds later…

35. A pacemaker was implanted several years ago…

a. Single chamber (VVI) pacemaker, retrograde P wavesb. Dual chamber pacemaker (P sensed, QRS paced)c. None of the above
The correct answer is ‘c’The ECG shows constant ventricular pacing. The pacemaker artifacts are best seen in leads V1 and V6.There is one P wave seen before each QRS complex. These P waves are positive in leads I, II, V4, V5and V6. Hence, these are normal P waves. Retrograde P waves would be inverted in lead V2. The PRinterval is constantly changing which cannot happen with a dual-chamber pacemaker (except in the raresituation with marked sinus tachycardia which exceeds the programmed upper rate).Hence, this is a single chamber VVI pacemaker which is functioning normally. Coincidentally, the sinusrate is similar to the pacing rate. Since, no P wave is conducted, the indication for pacing must have beenAV block.
36. 65 yr. old lady. Recent PAMI for anterior MI. Needed ventilator and IABP. 1st day of mobilisation

a. Artifactb. Monomorphic VTc. Polymorphic VTd. S VT with aberrancy
The correct answer is ‘a’The difference in pattern between the two leads helps in discerning out the artifact which was mimickinga tachycardia. The QRS complex can be detected in the leads which are synchronously manifested ascompared to the artifactual complexes.

41.
This ECG shows:a. Atrial fibrillationb. CHBc. Idioventricular rhythmd. All the above

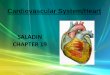
The correct answer is ‘d’ – All of the aboveThere is a slow ventricular rate (35 bpm). The RR intervals are regular but the QRS complex is wide(150 ms- see annotations in lead V2).
There are deep symmetrical T wave inversions in inferior and precordial leads. No normal P waves areseen. There is a clear atrial fibrillation.In atrial fibrillation, a slow regular ventricular rate can only be the result of complete heart block. Thewide QRS complexes originate in the ventricular myocardium.
43. 19-year old with history of palpitations and a syncopal episode.

This ECG shows:a. Polymorphic VTb. Atrial fibrillationc. Monomorphic VT
The correct answer is ‘b’ – Atrial fibrillationThe basal ECG shows a hint of pre-excitation as evidenced by a borderline short PR intervalin lead V4 and a hint of a delta wave. The arrhythmia is fast, broad and irregular. The RRinterval varies markedly. There are two types of QRS complexes in the ECG: (1) those whichare predominantly negative in leads V2 and V3 showing rS (*) and (2) those which show amonophasic R wave as shown by a # mark. A polymorphic ventricular tachycardia would havebeat-to-beat variation in the QRS complexes. A monomorphic VT would never be so irregular.In this case, the very rapid ventricular rate is because of conduction down two accessorypathways. The WPW pattern during atrial fibrillation becomes much more marked because AVnode is refractory during rapid rates. In sinus rhythm, however, the AV nodal conduction maskspartly the WPW pattern.

44. Uncontrolled HT. Pacemaker implanted for bradycardia a few years ago.Patient now comes with ill-health and dyspnea.
Likely cause for symptoms:a. Ischemiab. Renal failurec. Pacemaker malfunction
The correct answer is ‘b’- Renal failureThe QRS complexes are all paced. They are extremely wide measuring 280 ms.The P waves bear no relation to the QRS complexes. Hence, we are talking of single chamberventricular pacing. The P waves is distinctly abnormal as seen in lead C1 (V1). This suggests abiatrial abnormality. The P wave abnormality could be because of ventricular dysfunction andenlargement because of long-standing uncontrolled hypertension.The T waves are extremely tall and peaked. The height measures almost 18 mm in C3 (V3)

and the peaked nature is best seen in lead C2 (V2). Ventricular pacing does give wide QRScomplexes. However, these are typically in the range of 140-180 ms, depending on the site ofpacing and the size of the heart. A QRS complex of 280 ms is distinctly unusual for ventricularpacing. Secondary T wave change opposite to the QRS complex is expected with ventricularpacing. However, the peaked nature is distinctly abnormal. Also, the amplitude is too high forsecondary T wave changes. This ECG picture along with the clinical scenario suggests that thepatient is having a metabolic problem. Hyperkalemia is the most important cause for this Twave abnormality. If one then evaluates this retrospectively, then the QRS widths suggestingmyocardial delay is also a feature of sever hyperkalemia.Narrowing of QRS after correction of hyperkalemia
The next ECG after correction of hyperkalemia shows marked reduction in the QRS widths to about 120ms. The T waves also become much lower measuring only 8 mm in lead V3. The P wave abnormality isstill seen suggesting residual ventricular abnormality.
49. A 22 yr. old male; asymptomatic nationally competitive tennis player

This ECG shows:a. Mobitz type 1 AV block (Wenckebach)b. Mobitz type 2 AV blockc. Intermittent AV blockd. SA exit block
The correct answer is ‘a’ – Mobitz type 1 AV block (Wenckebach)There is clearly progressive PR prolongation followed by a blocked P wave. The Holter stripsshown below did not show in any higher grades of AV block. Repeatedly, AV Wenckebachwas seen.
At other times during the Holter there was 1:1 AV conduction even upto a heart rate of over101 bpm.

During stress test, he walked for 15 minutes on standard Bruce protocol without symptoms;the ventricular rate increased to 130 bpm.All the above information put together suggests a ‘vagally mediated’ AV nodal Wenckebach.In this athlete it is physiological, asymptomatic and not requiring any treatment. He wasallowed to continue his playing career with precautions of avoiding dehydration and fasting.
50.A 62 yr. old lady with diabetes, hypertension, Creatinine 3.9; comes with heaviness in chest…
This ECG shows:a. LBBBb. Acute MIc. Both A and Bd. None of the above
The correct answer is ‘c’ – LBBB and Acute MIThe ECG shows wide QRS complex of 140 ms, which confirms the LBBB pattern in lead V1(C1). The QRS axis is -300 and the PR interval is normal.In addition to this, there is ST elevation in V6.In the presence of LBBB, secondary ST-T changes are the rule. These ST-T changes are ina direction opposite to the QRS complex. However, in this ECG, despite the R wave in V6,there is concordant ST elevation. This clinches the diagnosis of acute MI. Therefore, in this

instance, one can diagnose LBBB with AMI, especially with the associated clinical profile.This patient was give IV heparin along with other medication. After the chest heavinesssettled, the ECG the next day (shown below) shows resolution of the ST segment in leadV5 (C5) and V6 (C6), along with the appearance of R wave in lead V5 (C5). This evolutionsuggests reperfusion.
The next day, the patient again had chest discomfort. The ECG now seen below showsreappearance of ST elevation in V5 and V6, suggesting re-infarction.
52. A 53 yr. old lady with effort dyspnea. At start of stress test….
3 minutes of exercise. Tiredness. The profile suggests:

This ECG shows:a. Ischemiab. AV nodal blockc. Infranodal blockd. None of the above
The correct answer is ‘c’ – Infranodal blockCareful observation of ECG during exercise shows that there is deformation of the T wavewhich has become pointed in lead II suggesting the presence of 2:1 AV block. This is confirmedby pointed T wave lying exactly between the midpoint of the 2 surrounding p waves.Ischemia is unlikely as there are no ST segment changes. The T wave changes have occurredbecause of superimposed P waves. In any case, ischemia does not produce isolated AV blockon exercise.Any AV block which comes or worsens on exercise, has to be ‘Infranodal block’ as AV nodalconduction improves with exercise. This patient therefore needs a pacemaker.
55. A 45-year-old man with severe chest pain

This ECG suggests:a. Proximal LAD occlusionb. R CA occlusionc. L eft main critical stenosisd. A cute Pericarditis
The correct answer is’ d’ – Acute pericarditisExcept leads aVR and V1, all leads show ST elevation. Also, there is ST depression in leadaVR. Close scrutiny shows the ST elevation to be “concave upward”, best seen in lead V5;however, this is only a supportive criterion for the diagnosis.Acute pericarditis causes inflammation of the epicardium resulting in repolarizationabnormalities of both atria and ventricles. In ventricles, it results in ST elevation which isseen in most of the leads and in atria as repolarization occurs during the PR segment. Thecurrent of injury causes PR segment elevation in aVR and depression in other leads. In acutepericarditis, PR and ST segment change directions. In conclusion, aVR may show PR elevationwith ST segment depression where as other leads show PR depression with ST elevationThe ECG after 3 days (below) showed complete normalization.

59. 68-year-old lady. Fatigue and recurrent near-syncope
This ECG shows:a. Sinus arrestb. Intermittent AV blockc. APC with concealed conductiond. SA exit block
The correct answer is ‘a’ – Sinus arrestThere are several long pauses, of variable duration. The longest one is 4.2 sec. Duringthese pauses, no P waves are seen. The pauses are not exact multiples of the P-P interval.Hence these are not SA blocks. The pauses are terminated by escape junctional or low atrialdepolarisations. A sinus arrest is more than 3 sec long- hence this is the correct diagnosis.These strips are during night time (see carefully the time mentioned), when the patient was

asleep. Hence in asymptomatic individuals with a high vagal tone, this could even be a normalvariation. In this patient, however, the associated symptoms of bradycardia made a pacemakerimplantation necessary. Since the AV nodal conduction was normal, an AAIR pacemaker wasimplanted. The paced ECG is displayed below.
ECG - 4A small pacing artifact precedes each P wave. There is also a solitary PVC. The patient wasasymptomatic after this.
60. 60-year-old man. Old anterior MI 6 months ago. Coronary Angio then had shown an ectasia of the LAD artery. This time he came with recent chest pain with collapse
This ECG shows:a. SVT with aberrancyb. Ventricular tachycardiac. AFib with fast ventricular rate

d. None of the aboveThe correct answer is ‘b’ – Ventricular tachycardiaThe ECG shows a regular wide QRS tachycardia. The QRS complexes are monomorphic.Unless proved otherwise, a wide QRS tachycardia in subjects with a history of MI must beconsidered a ventricular tachycardia. Moreover, one can even discern AV dissociation inlead V1.Monomorphic VT in coronary artery disease is due to an underlying scar of an old MI.