Embed Size (px)
DESCRIPTION
VHA and Indian Health Service: Access for American Indian & Alaska Native Veterans. Women Veterans. VHA and Indian Health Service: Access for American Indian & Alaska Native Veterans. VA Health Services Research and Development Service, ACC 03-304. B. Josea Kramer, PhD - PowerPoint PPT Presentation
Citation preview


B. Josea Kramer, PhDVA Greater LA Healthcare System Geriatric Research Education Clinical Center
Bruce Finke, MDIndian Health ServiceActing CMO, Nashville AreaElder Health Consultant
VA Health Services Research and Development Service, ACC 03-304
VA Greater Los Angeles Healthcare System InvestigatorsElizabeth Yano, PhD Debra Saliba, MD, MPH Stella Sarkisyan, MPH, MSW Donna Washington, MDLaurence Z. Rubenstein, MD, MPH
Overview: “VHA and IHS: Access for American Indian and Alaska Native Veterans”
Objectives:• Describe AIAN veterans’ health needs • Describe use of VHA and IHS• Inform interagency planning efforts
Photo: Maxine Judkins
Methods:• Administrative data• Organizational survey• Focus groups• Expert panel
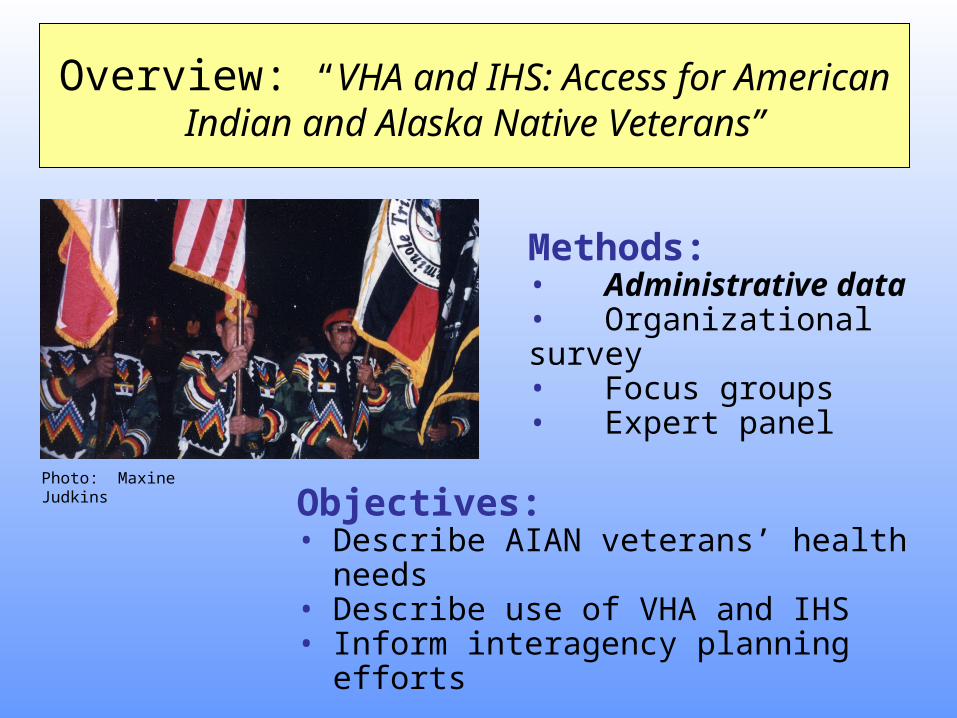
VHA IHS
Service states 50 35
States with hospitals 50 13
Entitlement
Background: VHA-IHS Memorandum of Understanding, 2003VHA and IHS resources
Overview: “VHA and IHS: Access for American Indian and Alaska Native Veterans”
High rates of military participation
BackgroundAmerican Indian Alaska Native Female Veterans
Many AIAN women are eligible for care from IHS and VHA
• Little is known about AIAN women• health needs• use of VHA and IHS
Overview“Federal healthcare for AIAN women veterans”
• Demographic and health characteristics
• Use of VHA and/or IHS care• Strategies for closer alignment
of federal resources
Minnie Spotted Wolf WWII – Marine Reserve Corps
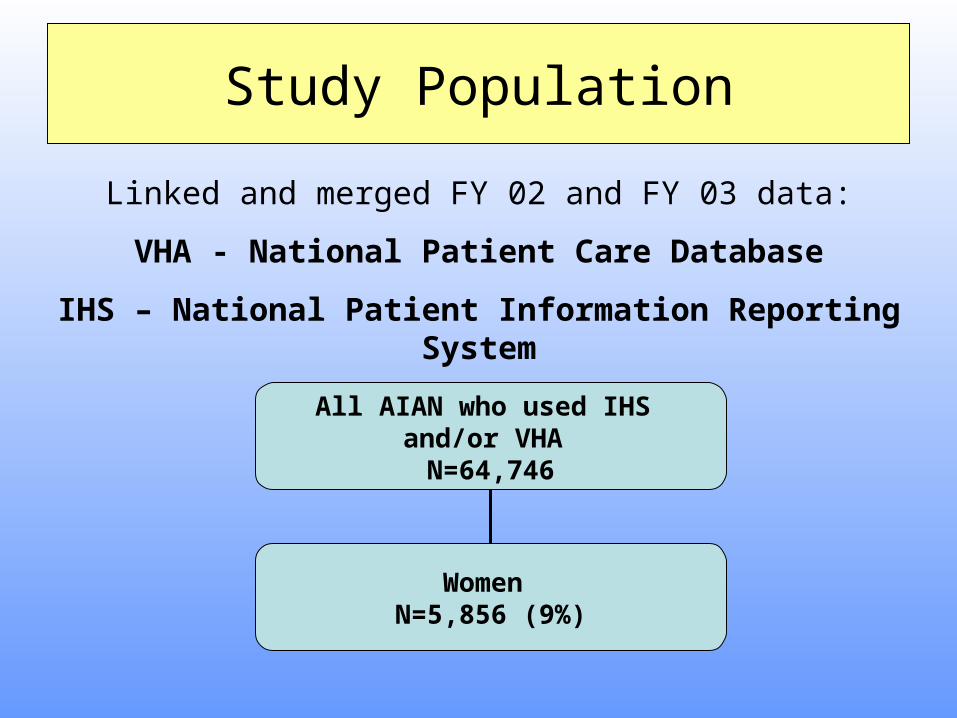
Study Population
All AIAN who used IHS and/or VHA
N=64,746
Women N=5,856 (9%)
Linked and merged FY 02 and FY 03 data:
VHA - National Patient Care Database
IHS – National Patient Information Reporting System
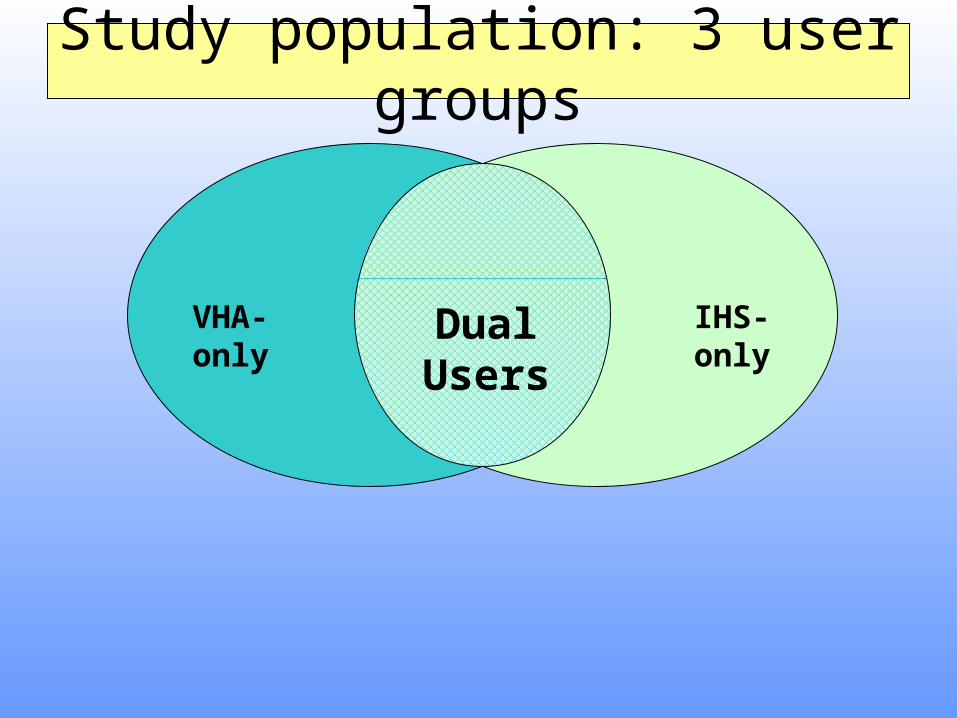
Study population: 3 user groups
VHA-only IHS-onlyDual Users
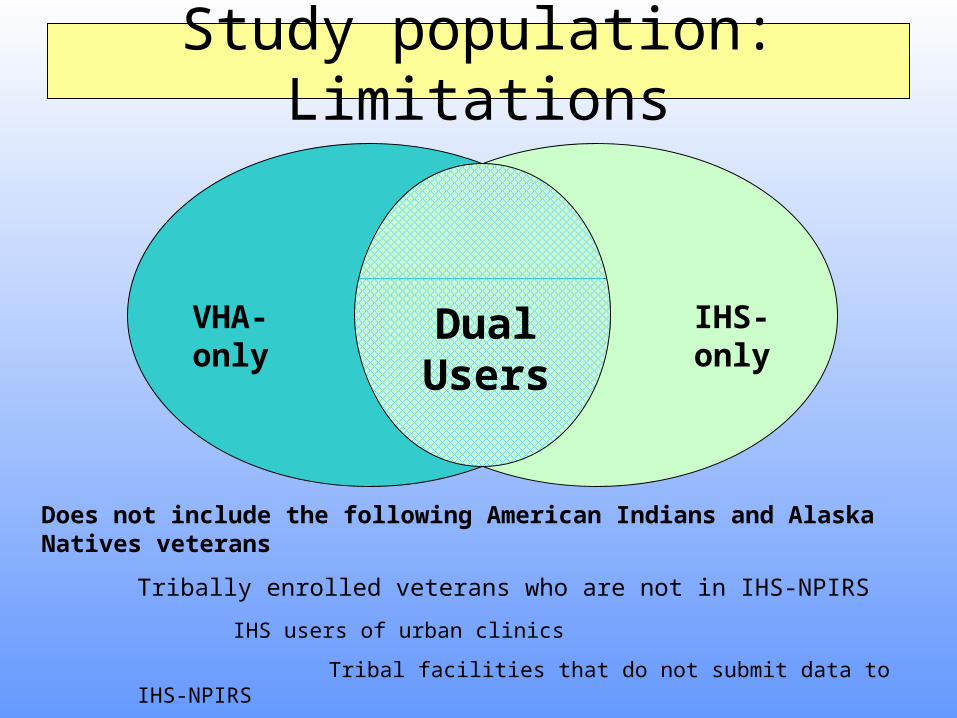
Study population: Limitations
VHA-only IHS-onlyDual Users
Does not include the following American Indians and Alaska Natives veterans
Tribally enrolled veterans who are not in IHS-NPIRS
IHS users of urban clinics
Tribal facilities that do not submit data to IHS-NPIRS
IHS-only users may under-report veterans
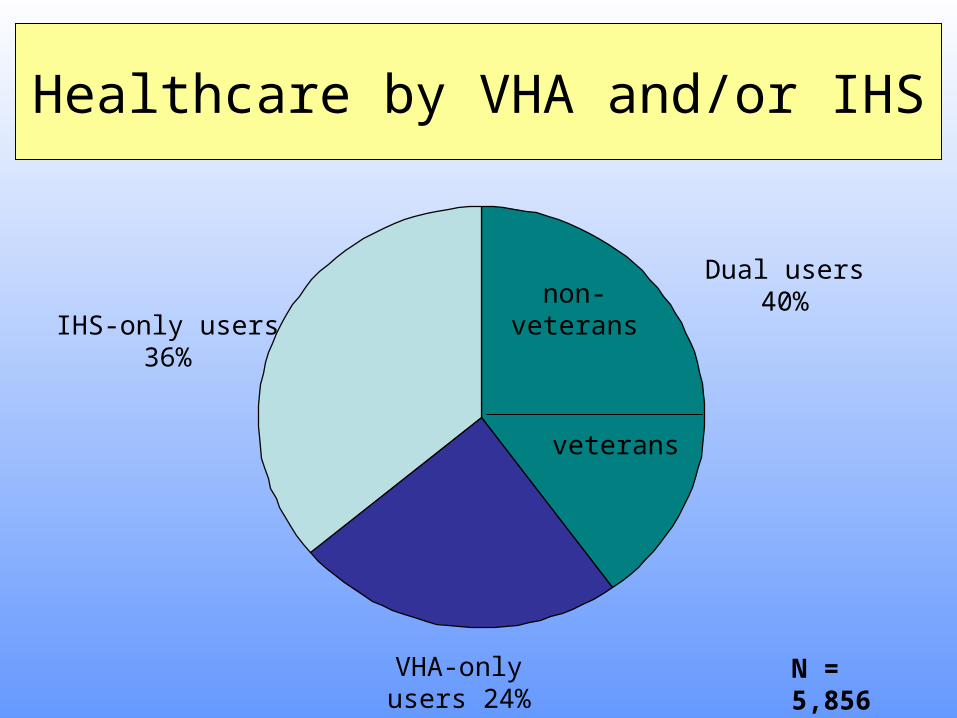
Healthcare by VHA and/or IHS
non-veterans
veterans
IHS-only users 36%
VHA-only users 24%
N = 5,856
Dual users40%
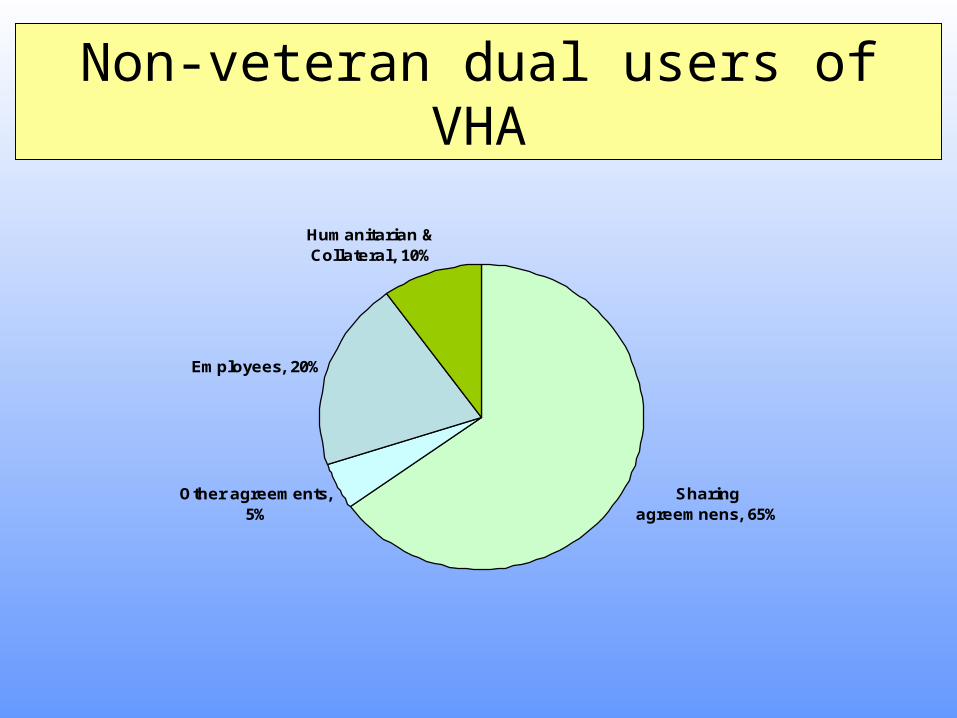
Non-veteran dual users of VHA
Sharing agreemnens, 65%
Other agreements, 5%
Employees, 20%
Humanitarian & Collateral, 10%
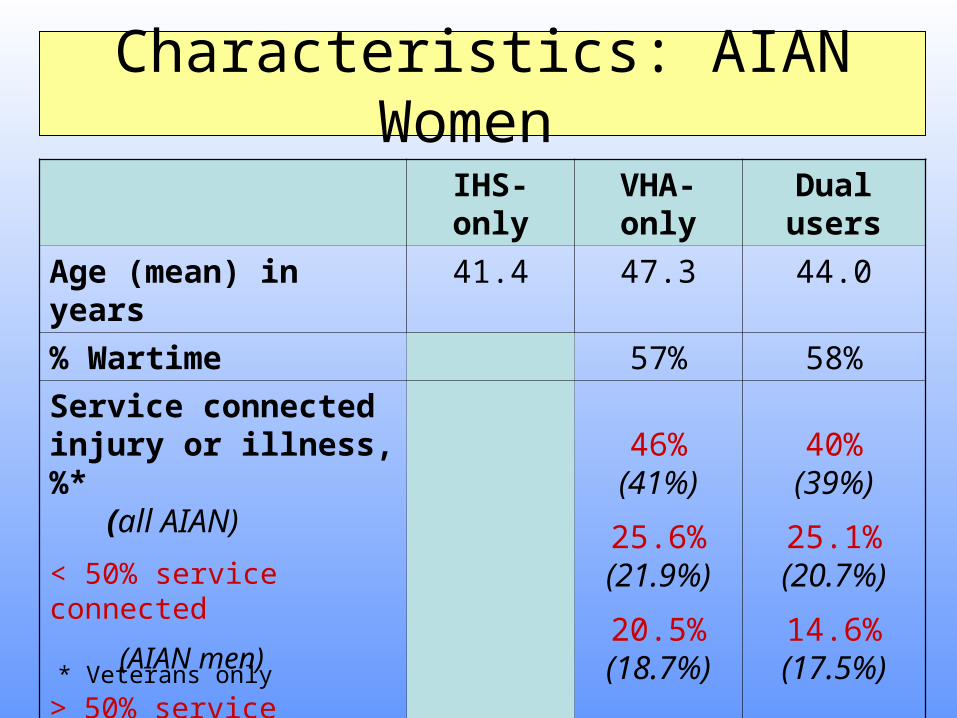
IHS-only VHA-only Dual users
Age (mean) in years 41.4 47.3 44.0
% Wartime 57% 58%
Service connected injury or illness, %* (all AIAN)
< 50% service connected
(AIAN men)
> 50% service connected
(all AIAN)
46%
(41%)
25.6%(21.9%)
20.5%(18.7%)
40%(39%)
25.1%(20.7%)
14.6%(17.5%)
Characteristics: AIAN Women
* Veterans only
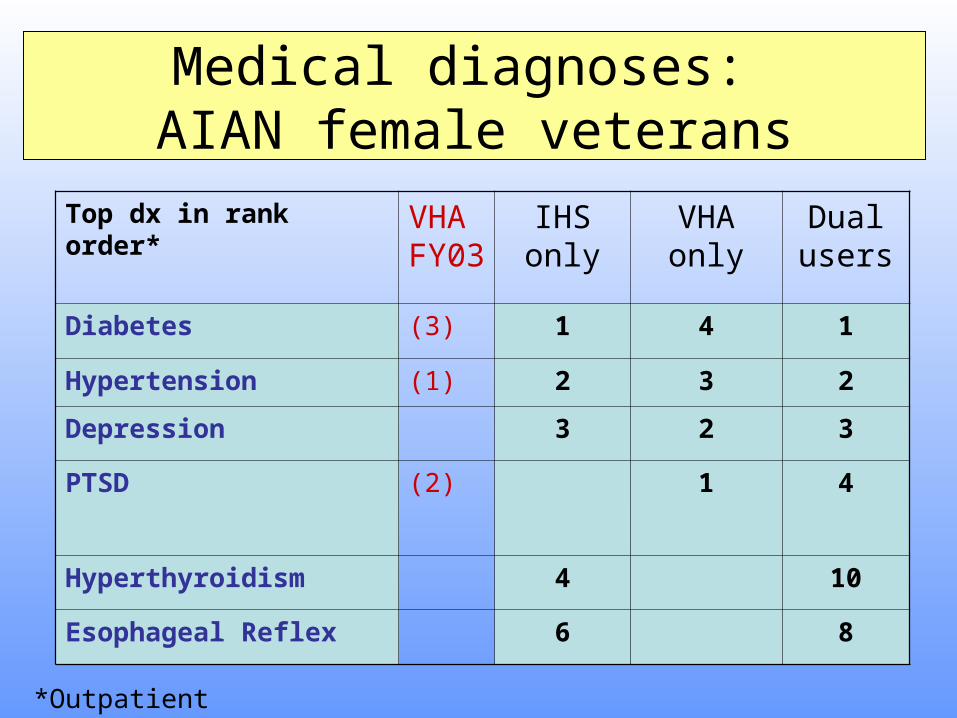
Medical diagnoses: AIAN female veterans
*Outpatient
Top dx in rank order* VHA FY03
IHS only
VHA only
Dual users
Diabetes (3) 1 4 1
Hypertension (1) 2 3 2
Depression 3 2 3
PTSD (2) 1 4
Hyperthyroidism 4 10
Esophageal Reflex 6 8
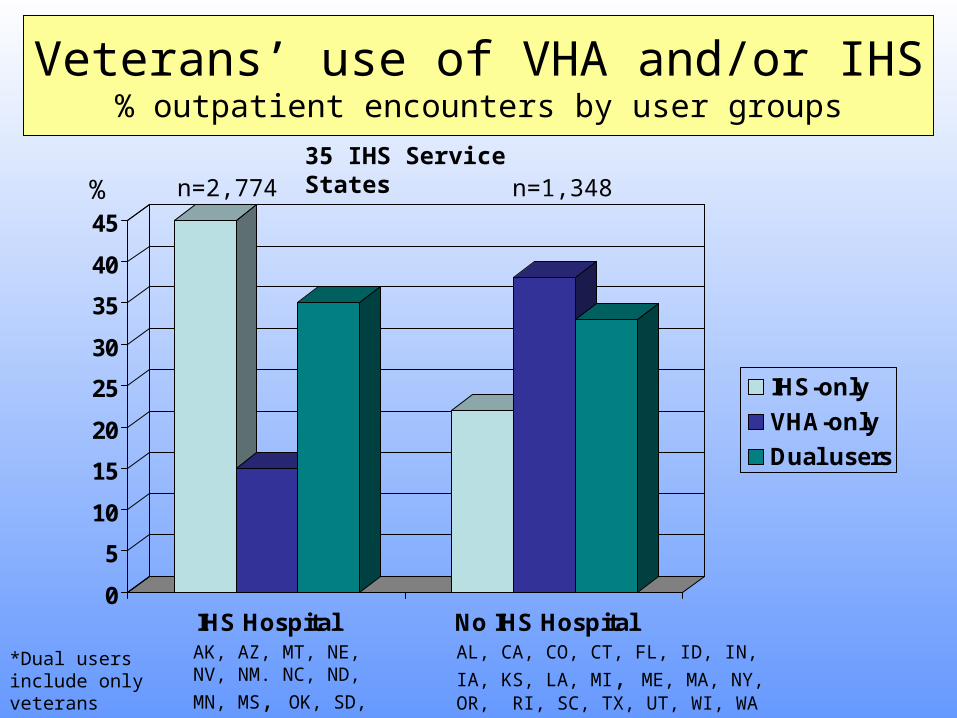
Veterans’ use of VHA and/or IHS% outpatient encounters by user groups
0
5
10
15
20
25
30
35
40
45
IHS Hospital No IHS Hospital
IHS-only
VHA-only
Dual users
n=2,774 n=1,348
AK, AZ, MT, NE, NV, NM. NC, ND, MN,
MS, OK, SD, WY
AL, CA, CO, CT, FL, ID, IN, IA, KS,
LA, MI, ME, MA, NY, OR, RI, SC, TX, UT, WI, WA
%
*Dual users include only veterans
35 IHS Service States
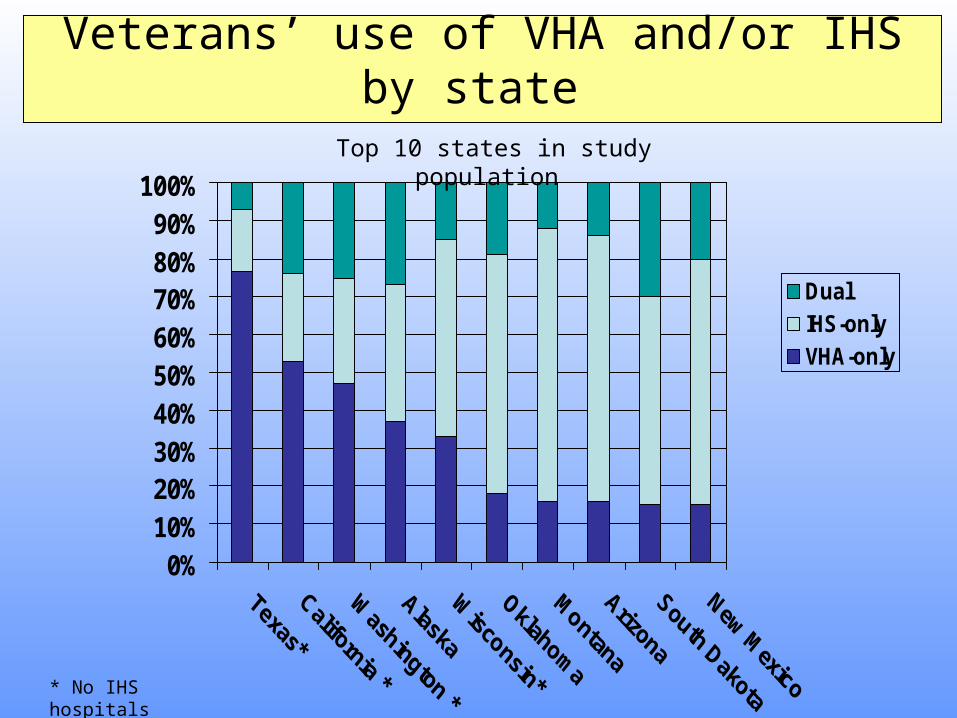
Veterans’ use of VHA and/or IHS by state
0%10%20%30%40%50%60%70%80%90%
100%
DualIHS-onlyVHA-only
* No IHS hospitals
Top 10 states in study population
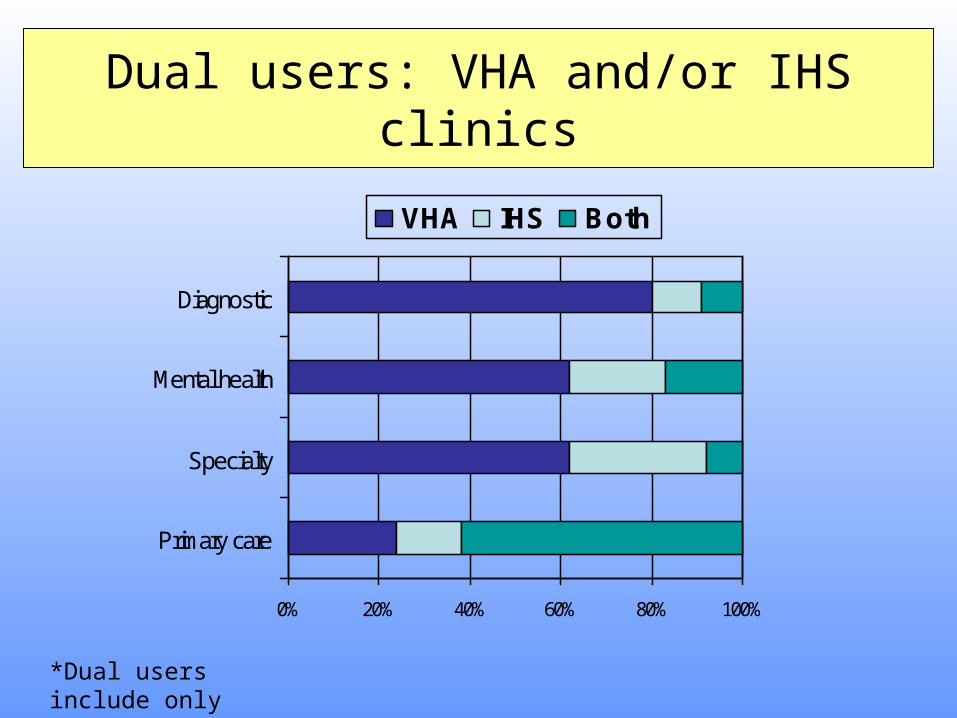
Dual users: VHA and/or IHS clinics
0% 20% 40% 60% 80% 100%
Primary care
Specialty
Mental health
Diagnostic
VHA IHS Both
*Dual users include only veterans
• High rate of service connected injuries and illness.
• PTSD, hypertension, diabetes & depression are prevalent conditions.
• Utilization patterns of VHA and/or IHS vary by location and by clinical resources.
• There is potential for overlaps in care for veterans who use both VHA and IHS.
Summary
Policy Implications:
• Expanding VHA care to all eligible female AIAN veterans would not require new types of services.
• Strategies for closer alignment of VHA and IHS may vary in recognition of utilization patterns.
• Coordination mechanisms should be established to reduce the potential for fragmentation of care for all dual users of VHA and IHS.
Policy Implications
Misty Warren, ChoctawNaval Test Parachutist
Mary Cornfield, Seneca Desert Shield/Storm
Cora Sinard, OneidaWWI – Army Nurse
Eva Mirabel, TaosWWII Air Corps
Janet Malcolm, OneidaViet Nam Era, Army Corps
Honoring American Indian women veterans