Embed Size (px)
Citation preview
1
VF00102
Mid-Trial Update
July 2017
VF00102 is a blinded study. All data presented are provisional and subject to formal statistical analysis.

222
• The information contained in the presentation is not intended to be an offer for
subscription, invitation or recommendation with respect to shares in any jurisdiction.
• No representation or warranty, express or implied, is made in relation to the accuracy
or completeness of the information contained in this document or opinions expressed in
the course of this presentation. The information contained in this presentation is subject
to change without notification.
• This presentation contains forward-looking statements which can be identified by the
use of words such as “may”, “should”, “will”, “expect”, “anticipate”, “believe”, “estimate”,
“intend”, “scheduled” or “continue” or similar expressions. Any forward-looking
statements contained in this presentation are subject to significant risks, uncertainties,
assumptions, contingencies and other factors (many of which are outside the control of,
and unknown to Factor Therapeutics Limited, and its officers, employees, agents or
associates), which may cause the actual results or performance to be materially
different from any future result so performed, expressed or implied by such forward-
looking statements.
• There can be no assurance or guarantee that actual outcomes will not differ materially
from these statements. The photographs of clinical subjects used in this presentation
are illustrative of medical conditions associated with potential applications of VF-001
(formerly marketed as VitroGro®). Actual clinical results may vary from those shown.
• Relevant images accessed under Creative Commons.
Disclaimer
2

3
VF00102 Mission
A Phase IIb study in venous leg ulcers designed to enable
clear decision-making :
• Phase III go/no go in the US
• Business development / partnerships / M&A
• CE Mark submission in Europe (second pivotal trial)
4
Strategy
Based on analysis of the previous VitroCARD study:
• Highly selective, focused on patients most likely to benefit
➢ “Margolis 1” (moderately severe ulcers)
• Receive standard care before randomisation
➢ To exclude placebo (spontaneous) responders
• Both wound closure and pain reduction endpoints
• Includes a quality of life (QoL) survey to pave the way forEU payer discussions
5
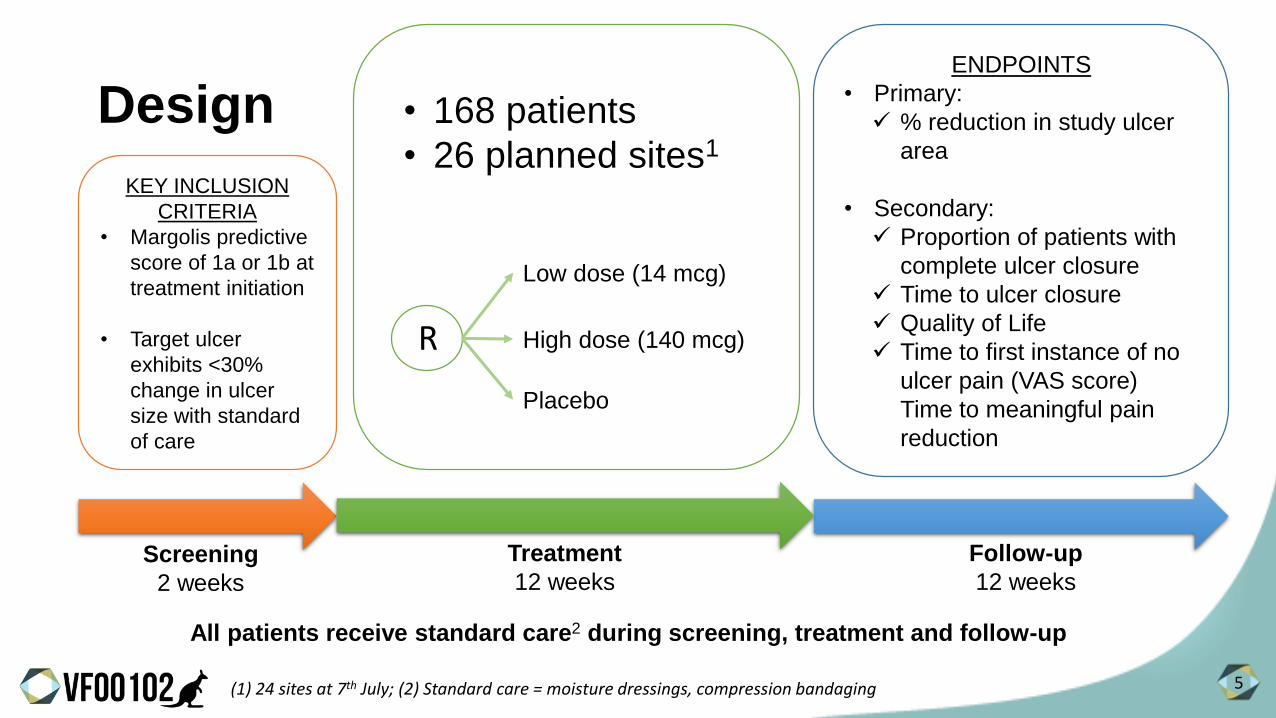
KEY INCLUSION
CRITERIA
• Margolis predictive
score of 1a or 1b at
treatment initiation
• Target ulcer
exhibits <30%
change in ulcer
size with standard
of care
Screening
2 weeks
(1) 24 sites at 7th July; (2) Standard care = moisture dressings, compression bandaging
• 168 patients
• 26 planned sites1
Treatment
12 weeks
ENDPOINTS
• Primary:
✓ % reduction in study ulcer
area
• Secondary:
✓ Proportion of patients with
complete ulcer closure
✓ Time to ulcer closure
✓ Quality of Life
✓ Time to first instance of no
ulcer pain (VAS score)
Time to meaningful pain
reduction
Follow-up
12 weeks
All patients receive standard care2 during screening, treatment and follow-up
Design
Low dose (14 mcg)
High dose (140 mcg)
Placebo
R
6
Pain
• Prior experience with VF001 suggested a marked reduction in pain by 3 weeks, particularly in patients who healed well
• This is both difficult and important to evaluate in a trial:
➢ Requires that patients are not on localised pain management therapy
➢ Requires a placebo that is “identical” to the treatment in all respects
➢ Opens the door to a completely different set of partnerships if successful (i.e. pharma companies with an interest in pain management, rather than wound care)
7
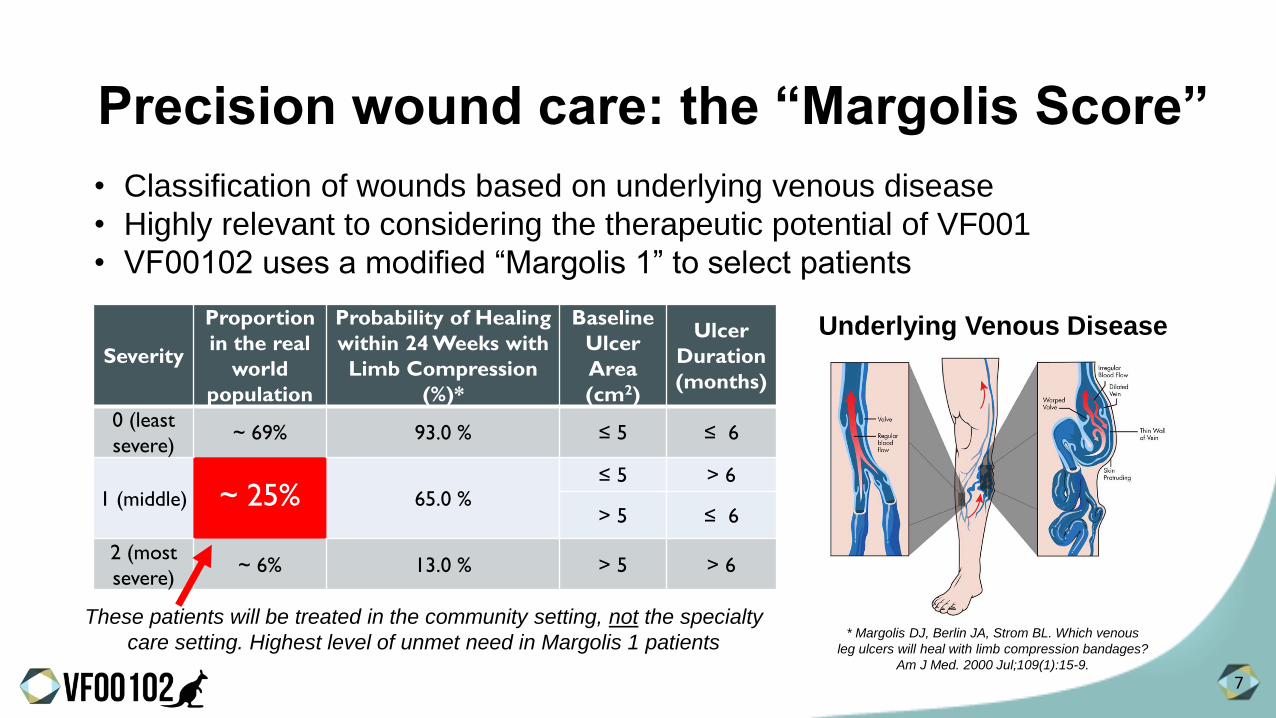
Precision wound care: the “Margolis Score”
• Classification of wounds based on underlying venous disease
• Highly relevant to considering the therapeutic potential of VF001
• VF00102 uses a modified “Margolis 1” to select patients
Severity
Proportion
in the real
world
population
Probability of Healing
within 24 Weeks with
Limb Compression
(%)*
Baseline
Ulcer
Area
(cm2)
Ulcer
Duration
(months)
0 (least
severe)~ 69% 93.0 % ≤ 5 ≤ 6
1 (middle) ~ 25% 65.0 %≤ 5 > 6
> 5 ≤ 6
2 (most
severe)~ 6% 13.0 % > 5 > 6
* Margolis DJ, Berlin JA, Strom BL. Which venous
leg ulcers will heal with limb compression bandages?
Am J Med. 2000 Jul;109(1):15-9.
Underlying Venous Disease
These patients will be treated in the community setting, not the specialty
care setting. Highest level of unmet need in Margolis 1 patients

8
Trial experience to date
> 280 patients pre-screened> 450 patient visits
• Sites are actively seeking patients, high level of engagement from most sites participating in the study
• Pre-screening is helping to focus on the population of interest
• As sites become familiar with the protocol, their patient selection improves
➢ Reflected in the screen fail rate observed to date
• Patient compliance is extremely high, with only one withdrawal
• Current focus is to work with the less active sites
9
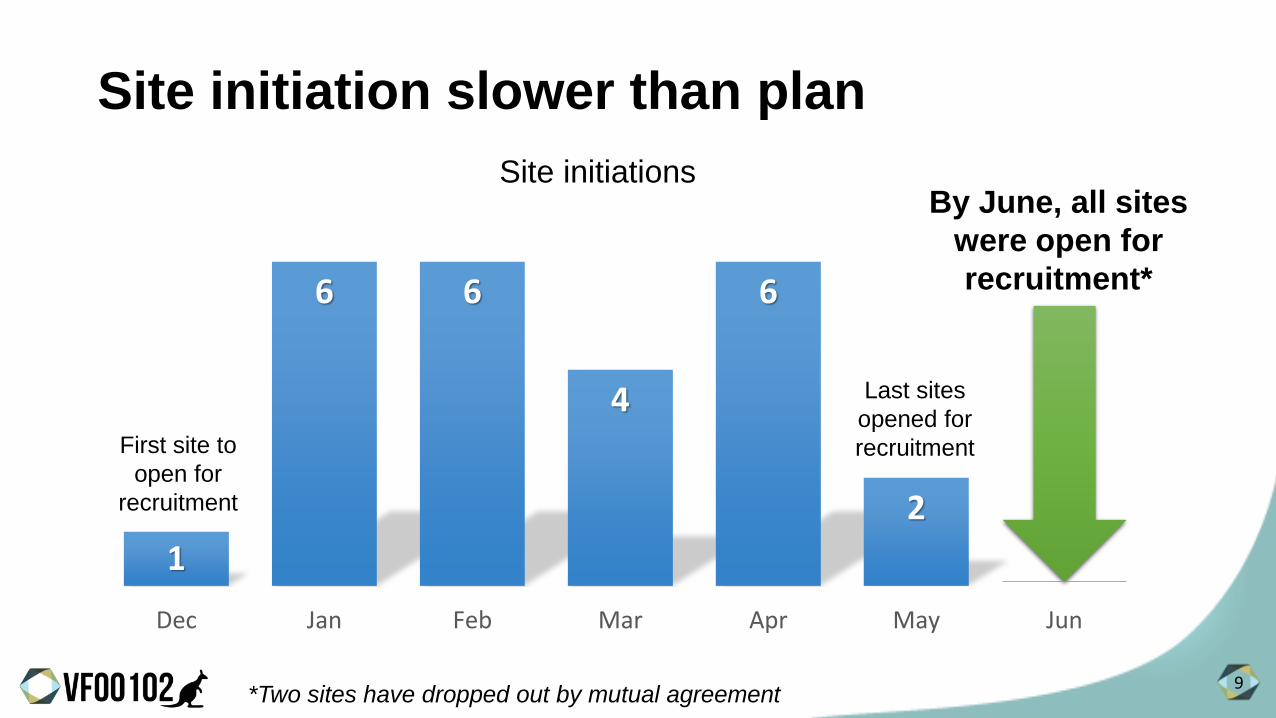
Site initiation slower than plan
1
6 6
4
6
2
Dec Jan Feb Mar Apr May Jun
First site to
open for
recruitment
Last sites
opened for
recruitment
By June, all sites
were open for
recruitment*
*Two sites have dropped out by mutual agreement
Site initiations
10
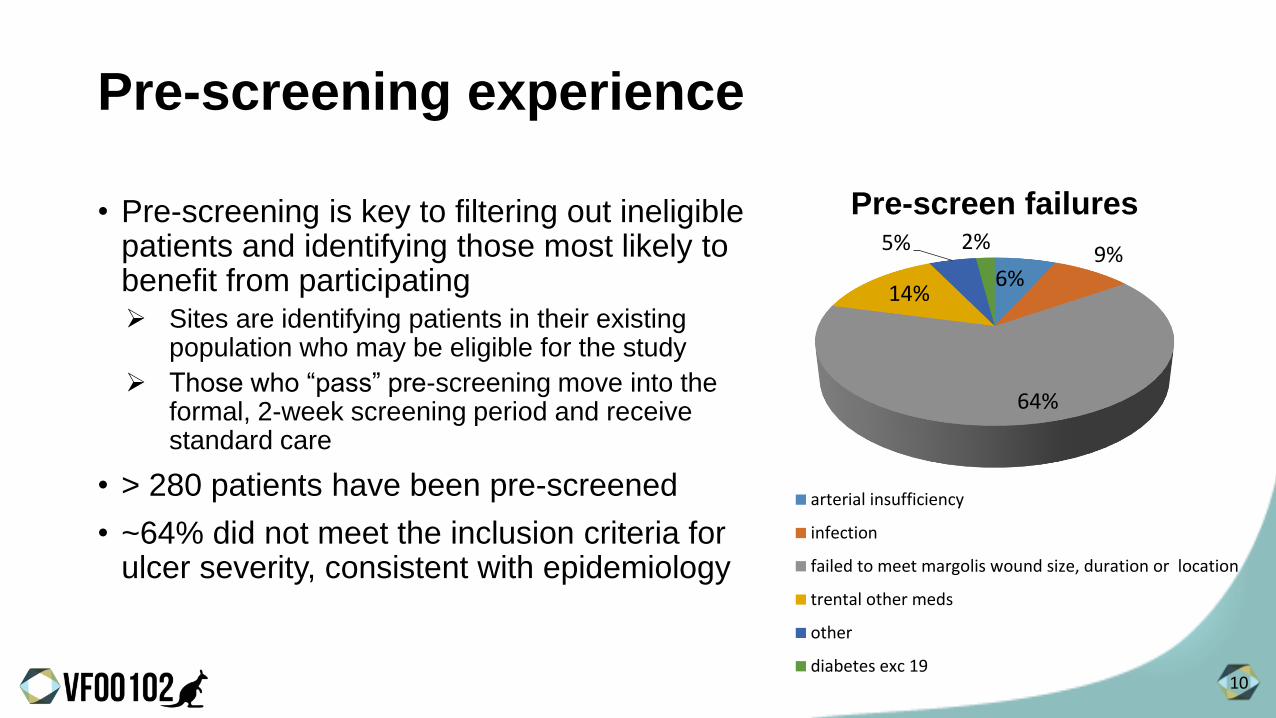
Pre-screening experience
• Pre-screening is key to filtering out ineligible patients and identifying those most likely to benefit from participating➢ Sites are identifying patients in their existing
population who may be eligible for the study
➢ Those who “pass” pre-screening move into the formal, 2-week screening period and receive standard care
• > 280 patients have been pre-screened
• ~64% did not meet the inclusion criteria for ulcer severity, consistent with epidemiology
6%9%
64%
14%
5% 2%
Pre-screen failures
arterial insufficiency
infection
failed to meet margolis wound size, duration or location
trental other meds
other
diabetes exc 19

11
Screen failure rate profile
• As sites get up to speed and understand the protocol, screen fail rates drop quickly
• Training and more rigorous pre-screening is delivering the expected number of screen failures: ~20%
0%
10%
20%
30%
40%
50%
60%
Dec/Jan Feb Mar Apr May
Percent screen fail

12
0
1
2
3
4
5#2
5
#24
#23
#22
#21
#20
#19
#18
#17
#16
#15
#14
#13
#12
#11
#10 #9 #8 #7 #6 #5 #4 #3 #2 #1
Screened/mth
Randomised/mth
Mostly
Academic
Mostly
Vascular/SurgicalMostly Wound Care /
Podiatry Clinics
Successful sites:
• Have been open longer
• Have quickly screened after initiation
- Typically wound / podiatry clinics
Overview of performance: site-by-site
Sites ranked by time to first patient screened
Patients
/site/m
thsin
ce S
IV
13
Site characteristics
• Wound care / podiatry sites : recruiting well➢ Some excellent performing sites
➢ Many are now bringing in a patient / month or better
➢ Will eventually be commercially important for VF001
• Vascular / surgical sites see typically more severe patients➢ Have generally struggled to recruit patients effectively
➢ Broader recruitment strategies (advertising, targeting referral clinics / GPs) required
➢ Watching very closely
• Academic / university medicine sites➢ Are expected to be very good recruiters (have great patient reach)
➢ Are simply slow to get up and running because of internal IRB* processes
*IRB = Institutional Review Board or “ethics approval”

14
0
20
40
60
80
100
120
140
160
180
200
220
6-Jan-17 6-Feb-17 6-Mar-17 6-Apr-17 6-May-17 6-Jun-17 6-Jul-17 6-Aug-17 6-Sep-17 6-Oct-17 6-Nov-17 6-Dec-17
Actual Screened Actual Randomized Withdrawn April est. Rand April est. Screen
Target 210 screened
Target 168 randomized
Limit 25 withdrawals
(PAREXEL) (PAREXEL)
Recruitment growing but behind CRO forecast
15
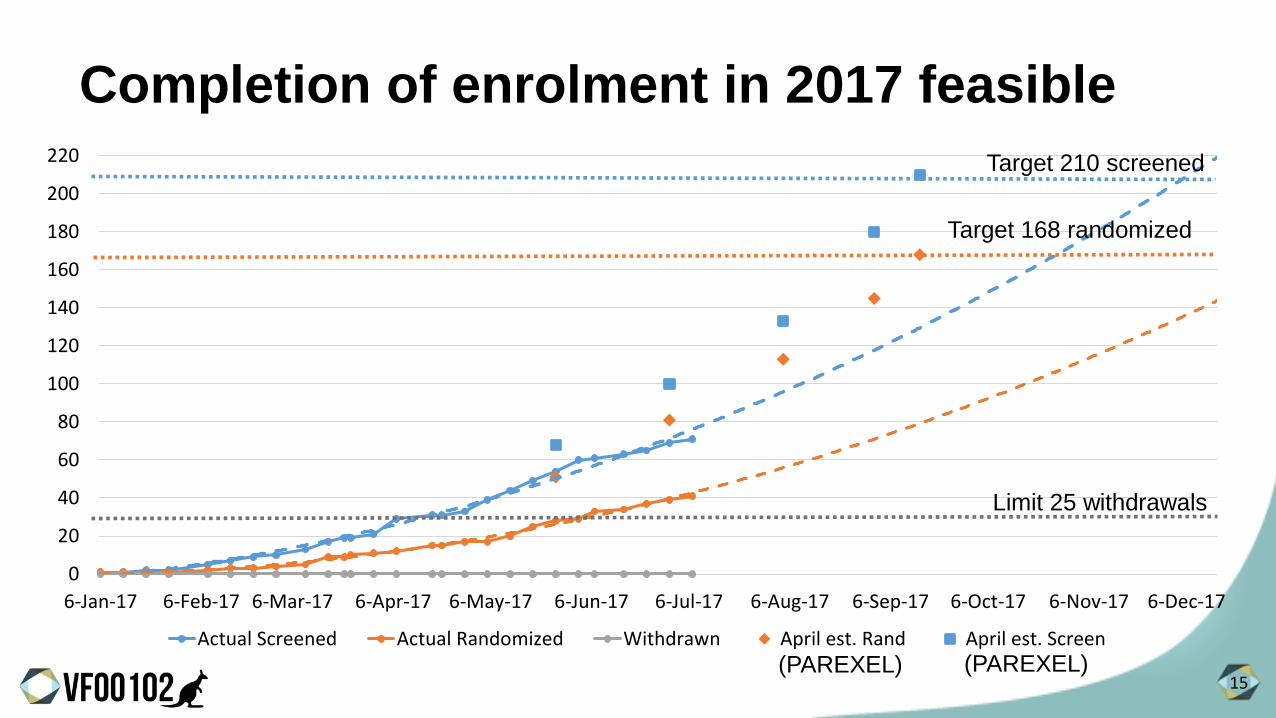
0
20
40
60
80
100
120
140
160
180
200
220
6-Jan-17 6-Feb-17 6-Mar-17 6-Apr-17 6-May-17 6-Jun-17 6-Jul-17 6-Aug-17 6-Sep-17 6-Oct-17 6-Nov-17 6-Dec-17
Actual Screened Actual Randomized Withdrawn April est. Rand April est. Screen
Target 210 screened
Target 168 randomized
Limit 25 withdrawals
Completion of enrolment in 2017 feasible
(PAREXEL) (PAREXEL)
16
Recruitment growth is not linear
• Q2 enrolment was more than double Q1 with only one additional site recruiting
• Several sites have yet to make a contribution to the study and are being actively managed (additional training, site visits, advertising)
• Academic sites (5) have only just gone online (IRBs) but are expected to be able to significantly contribute to the study
• Sites that have been active for 3 months have far greater recruitment rates than sites that have been active for less time➢ i.e. it takes time for sites to get comfortable with the protocol
➢ This is not a “simple” trial
17
Are patients’ ulcers healing?
• 28 patients have already been treated to at least Treatment Visit 6 (T6)
• 59% currently show a 50% or greater reduction in wound area
• Although the trial is not yet fully recruited and the data are blinded, this is encouraging as a “quality check” ➢ Because these are patients with fairly hard to heal ulcers
➢ Because the inclusion criteria for the trial ensures that these are “chronic” wounds that are less likely to spontaneously heal without treatment
• Only one serious adverse event (SAE) reported to date (not attributed to the treatment)
18
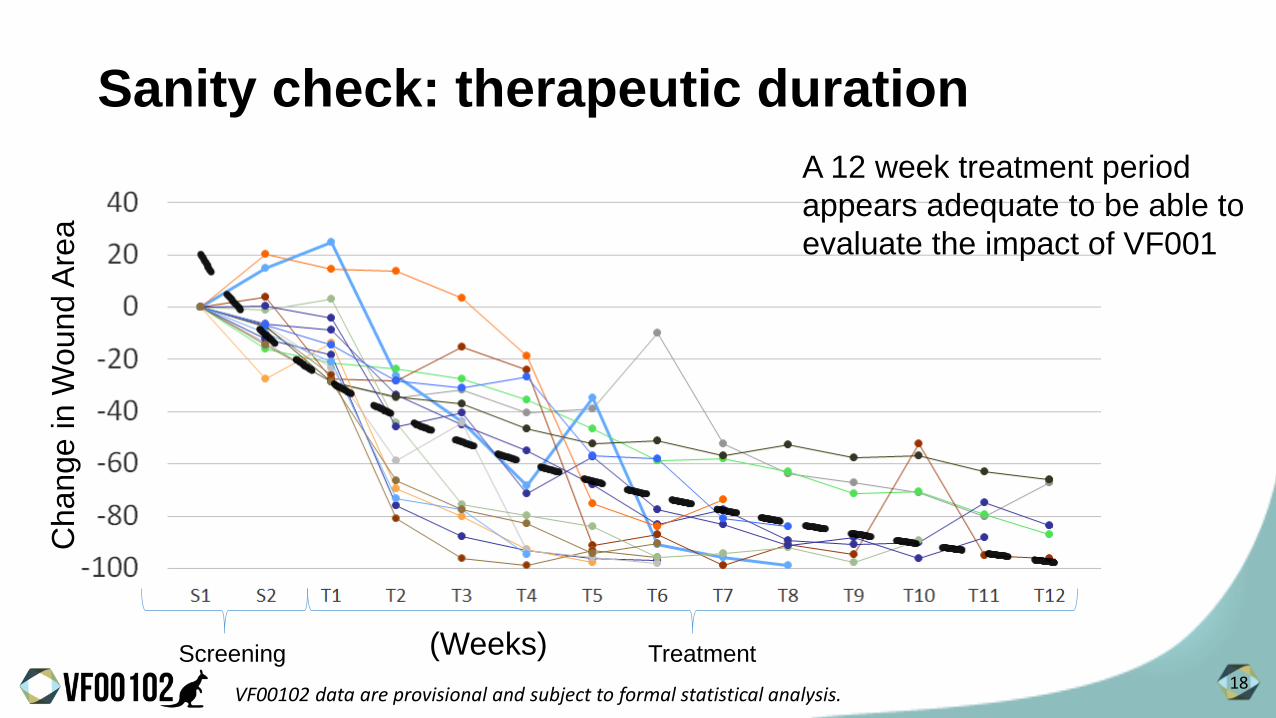
Sanity check: therapeutic duration
A 12 week treatment period
appears adequate to be able to
evaluate the impact of VF001
Screening Treatment
Change in W
ound A
rea
(Weeks)
VF00102 data are provisional and subject to formal statistical analysis.

19
0
20
40
60
80
100
120
0 2 4 6 8 10 12
% o
f In
itia
l Wo
un
d A
rea
Week
Sanity check: healing trajectory sensible
0
20
40
60
80
100
120
0 2 4 6 8 10 12
% o
f In
itia
l Wo
un
d A
rea
Week
VitroCARD – “Margolis 1” subset
VF00102 inclusion/exclusion criteria appear to be selecting a population whose overall healing trajectory is similar to patients in the VitroCARD study with “Margolis 1” ulcers
VF00102 data are provisional and subject to formal statistical analysis.

20
Major trial risks
Risk Mitigation Comments
Timely Enrolment Active management of under-
performing sites
Academic sites expected to have a significant
impact over the next quarter
Site Performance Replacement/ augmentation
of poor performers
We have qualified 6 additional sites and will
bring online if necessary
PAREXEL (CRO)
Acquisition
Senior-level dialogue /
assurances. In discussion
with backup CROs
Parexel acquired by private equity group
(Pamplona Capital) in June 2017. Cost cutting
measures likely, headcount impact
Screen failure rate Control of screening
“allowance” to under-
performing sites
Screen failure seems to be stable and in line
with plan but we are watching closely. Can
prioritize recruitment to higher quality sites
Seasonal impact -
summer
Monitoring closely Difficult to know if seasonal impact. VLUs
usually occur more often in summer

21
Concluding remarks
• A sophisticated trial that is progressing well
• This is a unique trial design that is the first of its kind – precision medicine
• Significant quarter-on-quarter enrolment improvement
• ~16 highly-engaged sites that are performing well (out of 24). Plenty of room for
improvement. Expecting a boost from the academic sites coming online
• Carefully watching site quality and screen failure rates
• Despite delays in getting sites launched, still targeting to complete
recruitment this year
VF001





























