Embed Size (px)
Citation preview

Dian Yu, class of 2016
Vestibular System

Chris Cohan, Ph.D.Dept. of Pathology/Anat SciUniversity at Buffalo
1. Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation?
2. Describe the vestibular apparatus, the 2 vestibular organs, and their unique sensory receptors
3. Describe the 1st and 2nd order neurons in vestibular pathways
4. Describe the pathways mediating vestibular perception and reflexes
5. Understand the importance of vestibular tests for clinical assessment
6. Describe: 1) acoustic neuroma and its the symptoms 2) benign paroxysmal positional vertigo
http://neuroscience.uth.tmc.edu/s2/chapter10.htmlhttp://neuroscience.uth.tmc.edu/s2/chapter11.html
Objectives

A 70 year-old woman complains of several episodes of dizziness for the past month. Symptoms: •when she awakens in morning and rolls over, she feels like room is spinning
• lasts about 20 sec, but sometimes nausea/vomiting
• brief periods of dizziness when she stands or shakes her head. Has caused her to fall.
• No change in hearing or ringing in ears

VESTIBULAR SYSTEM
• What is vestibular sensation• Where are vestibular sensory organs• How is vestibular info used by the CNS• What are clinical implications of vestibular
stimulation and vestibular lesions.

• Induced by head motion or change in head position
FUNCTIONS Deficits1. Perception of head movement/head position.
• Reflexive control of:2. Posture and balance - ability to stand upright3. Head position - head upright on shoulders4. Eye-head coordination - vestibulo-ocular reflex5. Autonomic Centers
Vestibular Stimulation
vertigo
falling
tilting
nystagmus
nausea

All sensory systems have pathways for perception and reflexes.
In the vestibular system, REFLEXES
dominate
Vestibular reflexes provides important tool for testing brainstem function.

Inner Ear

Vestibular Apparatus
Perilymphatic SpaceBony and Membranous
Labyrinth

Vestibular Apparatus2 Vestibular Organs:
• Semicircular Canals• Utricle and Saccule

Vestibular ReceptorsIn semicircular canals, sensory epithelium is the crista ampullares
duct
ampulla
cupula
crista
ampulla cupula

Vestibular Receptors
In the utricle/saccule, the sensory epithelium is Macula
Macula
Otolithic Membrane
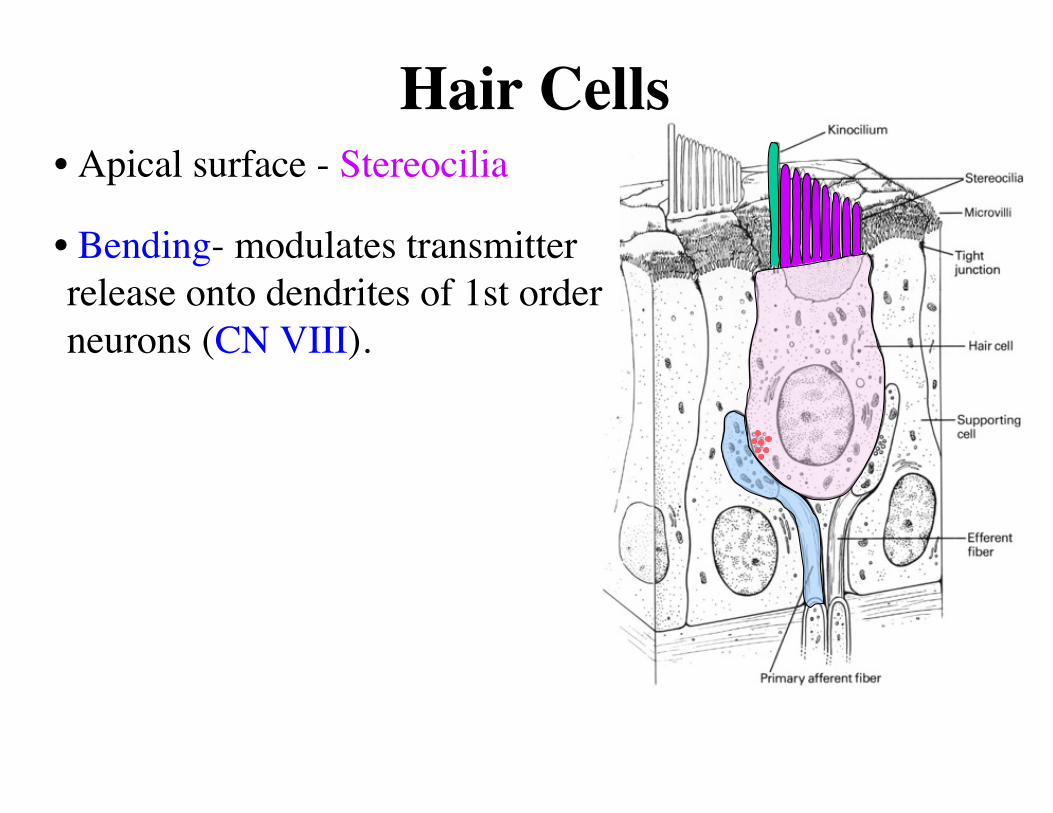
Hair Cells• Apical surface - Stereocilia
• Bending- modulates transmitter release onto dendrites of 1st order neurons (CN VIII).

Vestibular Structures
• First-order neurons
• in vestibular ganglion
• Bipolar neurons
dendriteaxon

Vestibular Structures
CN VIII enters brainstem at cerebello-pontine angle –
location of:
cerebellum, pons, medulla, CN VII, CN VIII

Vestibular Structures
S
I
LM
To cerebellumSecond-order neurons:
• the 4 vestibular nucleiin caudal pons/rostral medulla
• cerebellumaxons travel in inferior cerebellar peduncle
S
I
L
M
nodulus flocculus
Both the vestibular nuclei and cerebellum are REQUIRED for vestibular function

Damage to the vestibular nuclei –lateral area of caudal pons and rostral medulla
or
flocculus/nodulus of cerebellum
causes
generalized vestibular symptoms!! - falling, wide-based gait, nystagmus, nausea, vertigo
Lesions of Vestibular Structures

Vestibular Pathways
VestibularNuclei
VPL Parieto-temporal cortex
Vestibular disruption/lesions cause vertigo (feeling of movement).
1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers

Maintaining Balance
i. Vestibular system - required• vertigo has over-riding effect
ii. Visual system - provides external reference
iii. Proprioception - info about the body rather than head.
eg after spinning it is difficult to maintain upright posture using vision or proprioception
Romberg Test
1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers

2. Posture/Balance• strong excitation to extensor
muscles - counter gravity and maintain posture/balance.
• Ipsilateral tract – supports posture on same side. LVST
Lateral vestibulospinal tract
Lesions cause falling to same side.
Vestibular Pathways1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers

3. Head Position• Visual perception is aided by upright head position
• Vestibular stimuli during a fall forward, activate neck extensors to protect the head.
MVST
Medial vestibulospinal tractcontrols neck muscles
Vestibular Pathways
• Lesions cause altered head posture/head oscillation.
1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers

4. Eye-Head Movements• vestibulo-ocular reflex
MLF
Head rotation induces compensatory movement of the eyes in the opposite direction to maintain visual fixation.
Vestibular Pathways
• Lesions cause nystagmus.
1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers
VI
III
vest nuc

5. Autonomic Centers in rostral medulla
• Chemoreceptive trigger zone
• Vomiting center in Lateral RF
Vestibular Pathways
• Lesions cause nausea/vomiting.
1. Perception2. Posture and balance3. Head position4. Eye-head coordination5. Autonomic Centers

Effects of Vestibular Stimulation•Vertigo – perceived motion
in absence of movement•Loss of Balance/Falling•Nystagmus (spontaneous or induced forms)
•Nausea/Vomiting
MLF
LVST
MVST
Nystagmus may be ongoing or evoked by an eye movement.

1. Head rotation - Oculocephalic Reflex(Doll’s Eye Maneuver)
® conjugate eye movements
2. Caloric Test – cold or warm water infused into external auditory meatus
® conjugate eye movements(see https://www.youtube.com/watch?v=H4iQkFUgG6k)
3. Rotation in Barañy Chair (conscious)• see Dr Baizer’s handout
Stimulating/Testing the Vestibular SystemTests irritability and intact pathway

Doll’s Eyes ManeuverIn a comatose patient, moving the head from side to side or up and down causes the eyes to move in the direction opposite to head movement due to stimulation of the semicircular canals. These movements are known as Doll’s Eyes. This result indicates intact brainstem pathways. With brainstem damage, the eyes move in the direction of head movement (absent oculocephalic reflex).
In a conscious patient, when the same maneuver is done, the direction of eye movement depends upon whether the subject’s eyes are fixated on an object. Typically, fixation is not the case and the eyes move with the head.

Clinical Importance of Brainstem ReflexesCASE: On returning home from shopping, a wife finds her 59 year-old husband unconscious on the floor. He has no pulse. After calling 911, she begins CPR. When Mr. T arrives in the ED, he is in ventricular fibrillation. Spontaneous circulation is eventually restored, but Mr. T remains comatose. After 3 days in coma, his wife asks about her husband’s condition and the probability of a good outcome.How assess extent of CNS damage/function in unconscious patient
1. Somatosensory Evoked Potential2. Corneal reflex3. Pupillary Constriction Reflex4. Oculocephalic Reflex or Caloric Test

• Recognize vestibular symptoms• Source may be peripheral or CNS• When CNS, typically multiple
symptoms indicate lesion in• vestibular nuclei or• vestibular areas of cerebellum
• More localized lesions (eg MLF) produce more specific symptoms.
MLF
LVST
MVST
Vestibular System Lesionsto cortex

Acoustic Neuroma
A benign, slow-growing tumor of schwann cells in CN VIII. It may involve CN V and CN VII also.

Case SolutionA 70 year-old woman complains of several episodes of dizziness for the past month. Symptoms: • when she awakens in morning and rolls over, she feels like room is spinning
• lasts about 20 sec, but sometimes nausea/vomiting
• brief periods of dizziness when she stands or shakes her head. Has caused her to fall.
• No change in hearing or ringing in ears

Case Solution• 1. What does she mean by dizziness?
• 2. Relatedness of spinning room, nausea, falling, no hearing and ringing in ears?
• 3. What causes this condition?
vertigo
Symptoms of vestibular over-stimulation
Benign Paroxysmal Positional Vertigo

Benign Paroxysmal Positional Vertigo• non-progressing condition with brief periods of
severe vertigo – sudden change in head position
• Risk Fac: idiopathic/aging, head trauma, infection
• Pathophys: Dislodged otoconia move into semicircular canals to stimulate crista abnormally
• Treatment: Otolith Repositioning Procedure• surgery
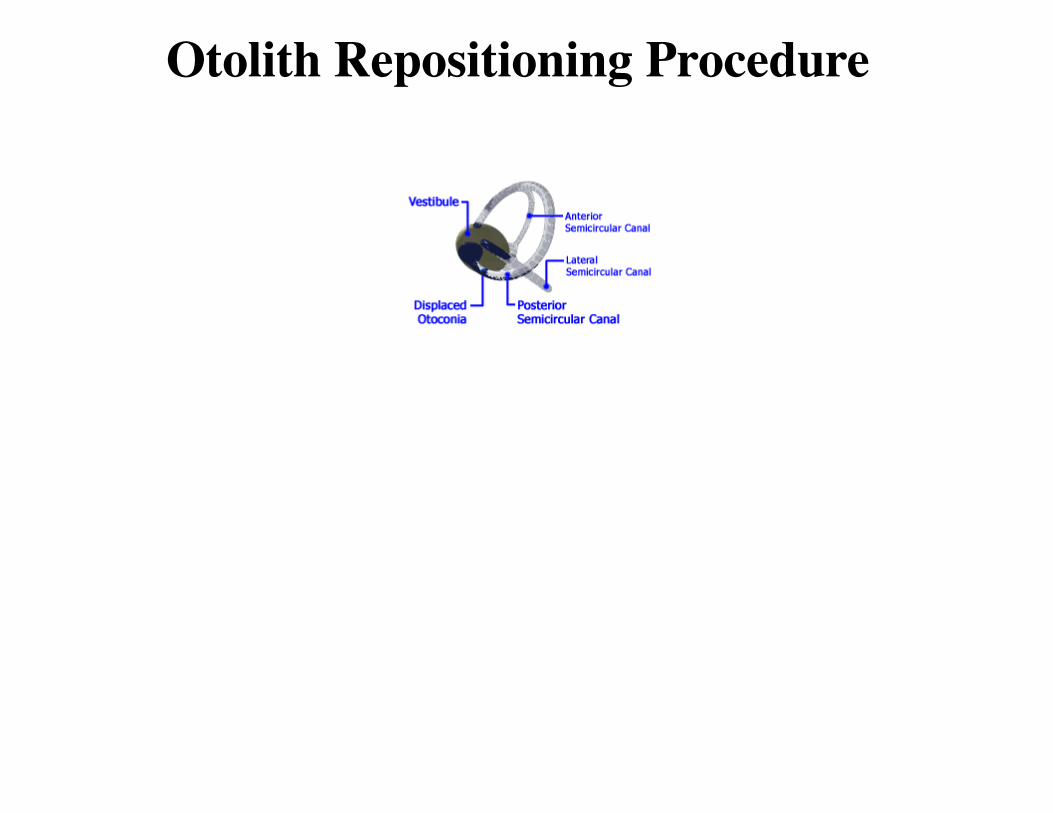
Otolith Repositioning Procedure