Embed Size (px)
Citation preview

Dan Gold, DO Assistant Professor of Neurology, Ophthalmology,
Neurosurgery, Otolaryngology – Head & Neck Surgery, Emergency Medicine
The Johns Hopkins University School of Medicine
Clinical Evaluation of Vestibular and Auditory Function

Outline • The labyrinth
• Semicircular canals • Otoliths • Cochlea
• Evaluation of labyrinthine function • Bedside • Laboratory
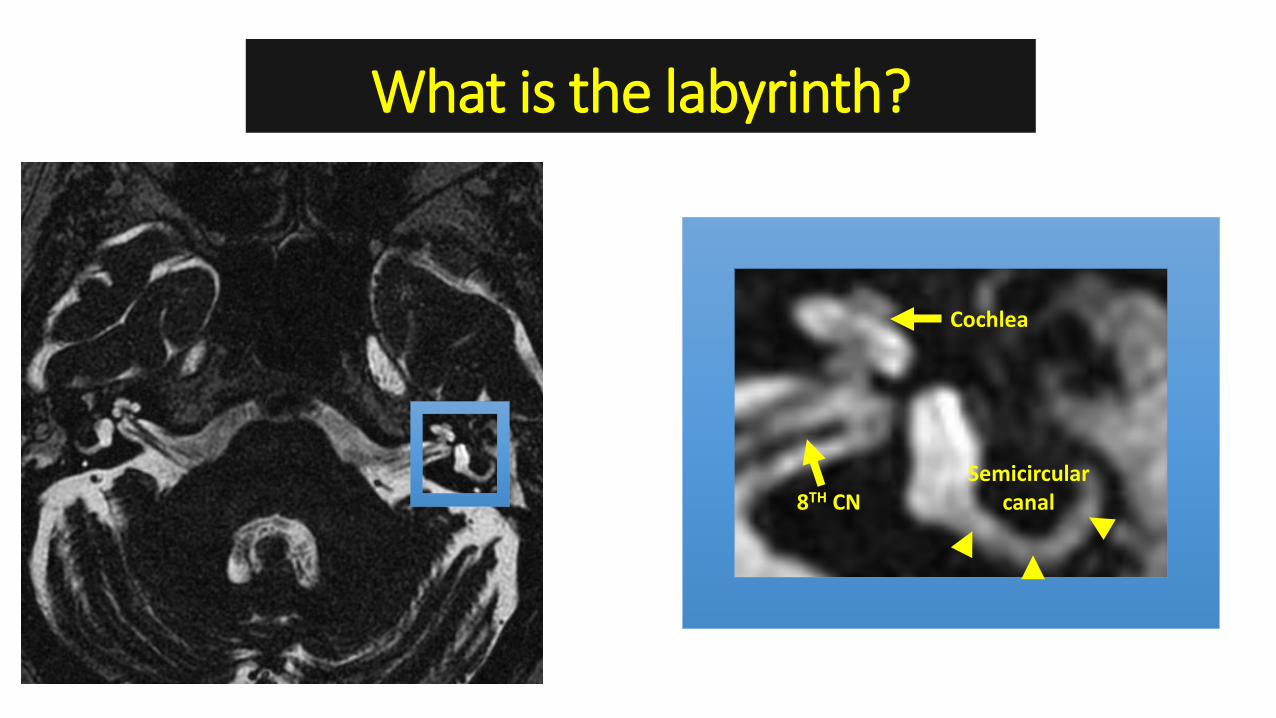
What is the labyrinth?
Cochlea
Semicircular canal 8TH CN

The Labyrinth 1) Semicircular Canals – angular acceleration 2) Otoliths – linear acceleration 3) Cochlea – hearing
Gold DR, et al. Repositioning maneuvers for BPPV. Curr Treat Options Neurol 2014 Smartphone App – aVOR, Liberty information Technology

Symptoms of Vestibular Disease (semicircular canals &/or otoliths)
• Vertigo • The sensation of self-motion (of head/body) when no self-motion is occurring
or the sensation of distorted self-motion during an otherwise normal head movement (a balance sensation)
• Dizzy • The sensation of disturbed or impaired spatial orientation which does not
necessarily include a false or distorted sense of motion (a balance sensation) • Unsteadiness
• Feeling of being unstable while seated, standing, or walking without aparticular directional preference (a balance sensation)
• Oscillopsia • The false sensation that the visual surround is oscillating (a visual sensation)
Bisdorff, A. R., J. P. Staab and D. E. Newman-Toker (2015). "Overview of the International Classification of Vestibular Disorders." Neurol Clin 33(3): 541-550.

SEMICIRCULAR CANALS
• Vestibulo-Ocular Reflex (VOR) • Bedside evaluation
• Head impulse test (HIT) • Dynamic visual acuity • Head-shaking
• Laboratory evaluation • Video HIT • Calorics • Rotational chair testing
Gold DR, et al. Repositioning maneuvers for BPPV. Curr Treat Options Neurol 2014

VOR Function

What does the VOR do?
• Why do the eyes move at all? • To see clearly, different movements must be possible
Loss of the VOR
“Most of us have experimented with motion pictures at home. This experience can be used to illustrate the sensations of the patient with damage to the vestibular apparatus. Imagine the results of a sequence taken by pointing the camera straight ahead, holding it against the chest and walking at a normal pace down a city street. In a sequence thus taken and viewed on the screen, the street seems to careen crazily in all directions, faces of approaching persons become blurred and unrecognizable and the viewer may even experience a feeling of dizziness or nausea. Our vestibular apparatus normally acts like the tripod and smoothly moving carriage on which the progression’s motion picture camera is mounted. Without these steading influences, the moving picture is joggled and blurred.”

Bilateral Vestibular Loss

The VOR The Semicircular Canals

The VOR Endolymph Flow
Stereocilia project into a gelatinous cupula deflection of cupula deflects stereocilia action potentials
Redrawn & modified from: http://pages.jh.edu/strucfunc/strucfunc/Academics_files/Della%20Santina%20and%20Carey%20Lecture%20notes%20-%20Struct%20Func%20ME%20580-625%202014.pdf

R L
EXCITATORY (AmpulloPETAL) R HC - Increased
Firing Rate
INHIBITORY (AmpulloFUGAL)
L HC -Decreased Firing Rate
Turn head right… …Increased firing rate ipsilaterally (R); decreased contralaterally (L)

The VORVisually-Enhanced VOR
VOR (Slow and Fast) https://collections.lib.utah.edu/details?id=187678

SEMICIRCULAR CANALS • Bedside evaluation of the VOR
• Head impulse test (HIT) - https://collections.lib.utah.edu/details?id=187678 • Dynamic visual acuity - https://collections.lib.utah.edu/details?id=1307318 • Head-shaking - https://collections.lib.utah.edu/details?id=187675

VOR Dysfunction

SCC Imbalance (left-sided lesion)
Dynamic SCC imbalance – ABNORMAL HEAD IMPULSE TEST (HIT)

SCC Imbalance (left-sided lesion)
Static imbalance Relatively higher
firing rate on Right (brain
thinks head is turning right)
Static imbalance Decrease in firing
rate on Left
Static SCC imbalance - NYSTAGMUS Arrows point in the direction of the
vestibular slow phase

SEMICIRCULAR CANALS • Laboratory testing
• Video HIT - https://collections.lib.utah.edu/details?id=1306744 • Calorics - https://collections.lib.utah.edu/details?id=1306740 • Rotary chair testing - https://collections.lib.utah.edu/details?id=1306742

Test When to Order Strengths Weakness
Caloric Testing (usually included in battery of
videonystagmography [VNG]/ electronystagmography [ENG]
testing)
Video Head Impulse Test (vHIT)
• To quantify function of the horizontal semicircular (SCC) vestibule-ocular reflex (VOR)
• Exposure to vestibulotoxic drugs (e.g., gentamicin)
• Concern for Meniere’s or vestibular hypofunction (preferentially evaluates the low frequency response of the VOR)
• To quantify function of the horizontal, posterior or anterior SCC VOR
• Exposure to vestibulotoxic drugs (e.g., gentamicin)
• Concern for vestibular hypofunction
• Easy to Administer • Results can be difficult to interpret • Often falsely absent response in second
tested ear • Semi-Invasive • Migraine patients may be particularly
sensitive to calorics
• Easy to Administer • Non-invasive • Portable • Can evaluate function of all SCC
including vertical • Measures gain as well as corrective
(covert and overt) saccades to evaluate the VOR
• Using high peak head velocities, contributions from the ‘healthy’ ear are minimized
• To evaluate patients with suspected • Good test for bilateral vestibular loss Rotary Chair bilateral horizontal SCC loss
• The clinician must be aware of artifacts (suboptimal calibration, goggle slippage artifacts, etc)
• Testing is technician dependent as head impulses are performed manually
• Not a good test for unilateral vestibular loss since the healthy side can drive the vestibular response (a low peak head velocity condition)
• Not widely available • More difficult to administer – many
patients find testing uncomfortable or intolerable (usually migraine patients)

OTOLITHS
• Bedside evaluation • Ocular alignment • Subjective visual vertical (SVV)
• Laboratory evaluation • Vestibular-Evoked Myogenic
Potentials (VEMPs) • Cervical • Ocular
Gold DR, et al. Repositioning maneuvers for BPPV. Curr Treat Options Neurol 2014

Otolith Function
(utricle – linear translation and head tilt)

Redrawn & modified from: Leigh and Zee. The Neurology of Eye Movements. 5th Edition.
Physiologic Ocular Tilt Reaction (OTR)
1) Head tilts rightexcites right utricle
2) Right eye elevates &Left eye depresses
3) Ocular counter-roll, top poles toward left ear

OTOLITHS • Bedside evaluation of the Otolith (utricle)
• Ocular alignment - https://collections.lib.utah.edu/details?id=187677 • SVV
Bucket Test

Otolith Dyfunction

• LEFT-sided utricle pathway destruction
Static Utricle Imbalance
Brain perceives right head tilt and tries to get back to earth vertical
aVOR app

RL
SVV
Head tilt left
Skew deviation (left hypotropia)
SVV to the left https://collections.lib.utah.edu/ details?id=187730

OTOLITHS • Laboratory testing
• VEMPs - https://collections.lib.utah.edu/details?id=1306743 • Ocular VEMPs – utricle pathways • Cervical VEMPs – saccule pathways
Test When to Order Strengths Weakness
VEMPs • •
Concern for SCDS With vestibular neuritis, VEMPs can help localize to the superior or inferior
• • •
Easy to Administer Non-invasive Since oVEMPs are a test of the utricle-
• VEMPs are commonly non-localizing or absent – e.g., due to suboptimal sternocleidomastoid contraction in
divisions of the vestibular nerve – e.g., horizontal and anterior SCC
ocular motor pathways, ‘central’ patterns have been described which •
cVEMP testing Not widely available
hypofunction with abnormal ipsilateral may have some localizing value in ocular VEMP (oVEMP) suggests superior certain conditions (medial longitudinal division while posterior SCC fasciculus syndromes) hypofunction with abnormal ipsilateral cervical VEMP (cVEMP) suggests inferior division
• When Meniere’s is suspected, there is no conclusive evidence that VEMPs help to establish this diagnosis

COCHLEA
• Laboratory evaluation • Audiometry
• Bedside evaluation • Hearing to finger rub/tuning
fork • Rinne & Weber
Gold DR, et al. Repositioning maneuvers for BPPV. Curr Treat Options Neurol 2014

Symptoms of Auditory Disease
• Hearing loss
• Fullness • Popping • Pressure • Pain • Tinnitus
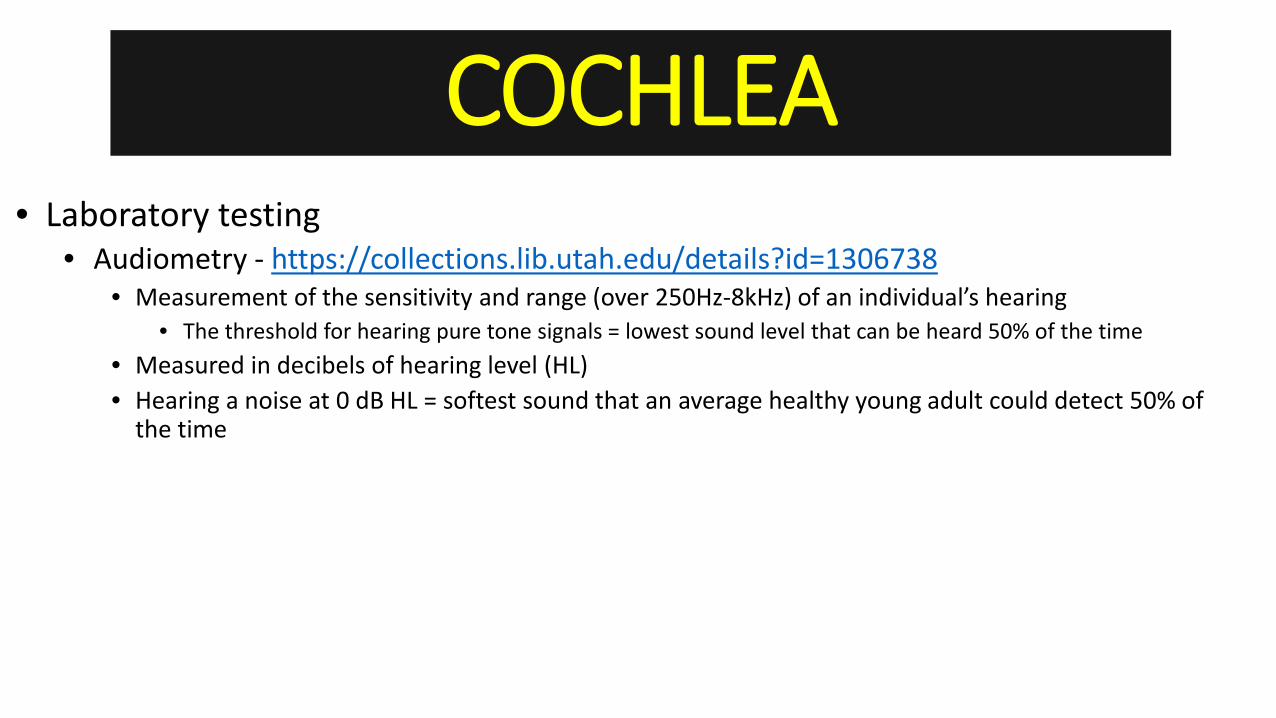
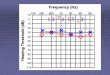
COCHLEA • Laboratory testing
• Audiometry - https://collections.lib.utah.edu/details?id=1306738 • Measurement of the sensitivity and range (over 250Hz-8kHz) of an individual’s hearing
• The threshold for hearing pure tone signals = lowest sound level that can be heard 50% of the time • Measured in decibels of hearing level (HL) • Hearing a noise at 0 dB HL = softest sound that an average healthy young adult could detect 50% of
the time

COCHLEA – Air Conduction • AUDIOMETRY
• Air conduction threshold tests conductive and neural components (noise through air with headphones/ear buds)
Noise enters external auditory
canal
Sound pressure funneled to
tympanic membrane (TM)
TM vibrates Moves ossicles
Moves fluid inside cochlea
forming a frequency-
specific fluid wave
Frequency-dependent
cochlear nerve excitation
• Lesion anywhere will cause increased air conduction thresholds…need bone conduction thresholds to interpret

ox t
d res f
e
COCHLEA – Bone Conduction • AUDIOMETRY
• Bone conduction thresholds tested by applying sound directly to the cochlea (oscillator on mastoid - noise transmitted through bone)
N ise enters e ternal audi ory
canal
Soun p sure unneled to tympanic
membrane (TM)
TM vibrates Moves ossicl s
Moves fluid inside cochlea
forming a frequency-
specific fluid wave
Frequency-dependent
cochlear nerve excitation
• Conductive component of hearing is bypassed…test of how well cochlea and centralauditory system are working
COCHLEA • Laboratory testing
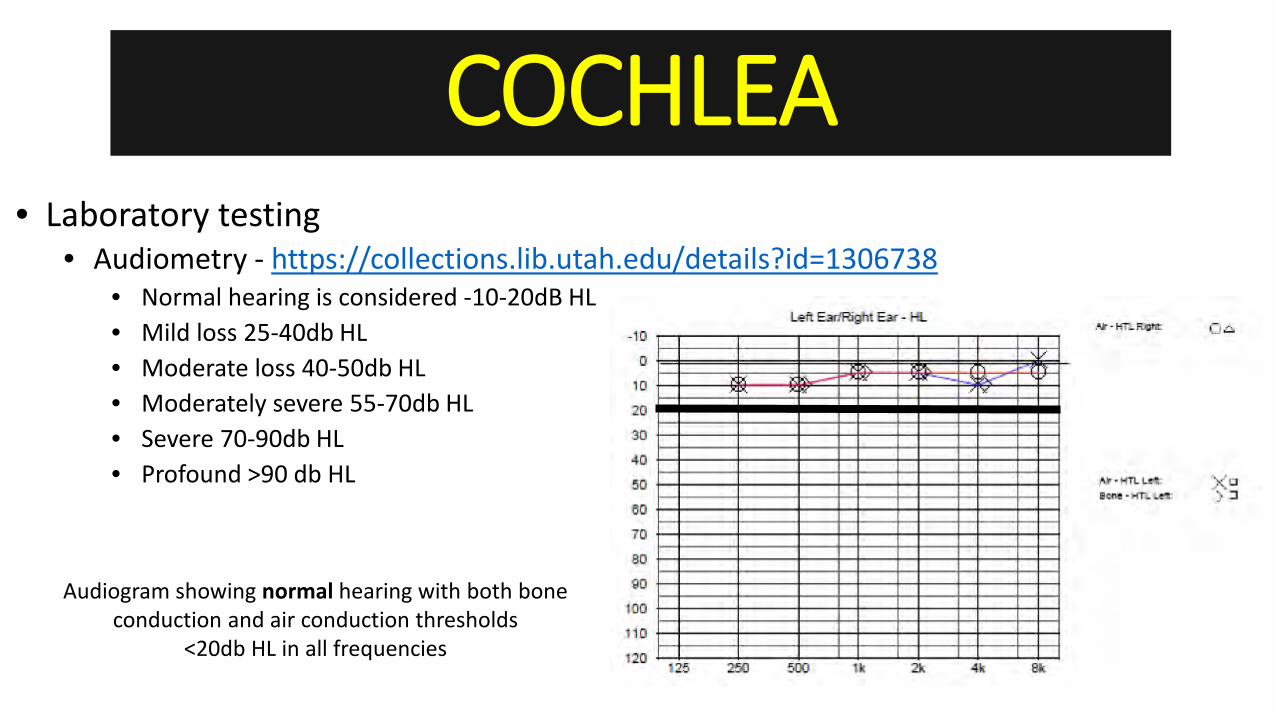
• Audiometry - https://collections.lib.utah.edu/details?id=1306738 • Normal hearing is considered -10-20dB HL • Mild loss 25-40db HL • Moderate loss 40-50db HL • Moderately severe 55-70db HL • Severe 70-90db HL • Profound >90 db HL
Audiogram showing normal hearing with both bone conduction and air conduction thresholds
<20db HL in all frequencies

COCHLEA • Laboratory testing
• Audiometry • Is it conductive hearing loss?
• Decrease in hearing for air conducted sounds, normal bone conducted thresholds • Is it sensorineural hearing loss?
• Decrease in both air and bone conducted sounds

COCHLEA • Bedside testing
• Rinne/Weber - https://collections.lib.utah.edu/details?id=1307288
• Sensorineural HL • Rinne: AC>BC • Weber: lateralizes to good
ear • Conductive HL
• Rinne: BC>AC • Weber: lateralizes to bad ear

COCHLEA Test When to Order Strengths Weakness
• Aural fullness • Easy to Administer • Often only an initial test, majority of • Autophony • Non-invasive otologic etiologies of vertigo will require Audiometry • Fluctuating hearing further confirmatory testing (i.e. CT, • Pulsatile tinnitus vestibular evoked myogenic potentials • Concern for Meniere’s, superior canal (VEMPs), calorics)
dehiscence syndrome (SCDS), vestibular neuritis/labyrinthitis
TAKE HOME POINTS
• The labyrinth is made up of • Semicircular canals – angular acceleration detectors • Otoliths (utricle & saccule) – linear acceleration detectors • Cochlea – hearing
• The bedside evaluation & history in patients with vestibular or auditory symptoms is used to localize the problem, narrow the differential diagnosis, and guide further work-up
• Audiometry is almost always needed to better define auditory function • Vestibular testing can be chosen based on the localization and etiology

NOVEL
• North American Neuro-Ophthalmology Society (NANOS) – Neuro-Ophthalmology Virtual Education Library (NOVEL)
• http://novel.utah.edu/Gold/ • Instructional vestibular and ocular motor exam videos • Lots of pathology
• Smartphone App – aVOR