Embed Size (px)
Citation preview
1/29/08
1
Vesico-vaginal Fistulas: Current Assessment and
Management Dr. Andrew J Marks
UBC Urology Grand Rounds January 23, 2008
Outline
• History • Epidemiology • Etiology and Pathophysiology • Presentation and Diagnosis • Management and Outcomes • New Technologies and Techniques • VVF’s and “fistula tourism”

1/29/08
2
Definition
• A vesicovaginal fistula is an abnormal communication between the urinary bladder and the vagina that results in the continuous and often involuntary loss of urine into the vaginal vault (Riley 2006)

1/29/08
3
History
• Von Roonhuyse: surgical principles of VVF repair (1663)
• Fatio: first successful repair in 1675 • Mettauer: first American to perform a
successful closure 1838 • Sims: refined and described technique 1852 • Trendelenberg 1882 • Martius 1928
1/29/08
4
Etiology
• Industrialized nations: > 75% of VVF’s are caused by injury to the bladder at the time of gynecologic, urologic or other pelvic surgery (Symmonds 1984, Lee 1988, Tancer 1992)
Etiology: developed world
• Traumatic • Postsurgical • External trauma
• Radiation therapy • Advanced malignancy • Infection/inflammatory disorder • Foreign body • Obstetric • congenital
1/29/08
5
Etiology: developed world
• Iatrogenic bladder injury during abdominal hysterectomy 0.5-1.0% (Keetel et al 1978)
• Bladder injury during vaginal hysterectomy variable, approximately 0.13-1.7% (Mathevet et al 2001)
• Overall the incidence of post hysterectomy VVF 0.1-0.2% (Harris 1995)
congenital
1/29/08
6
Radiation induced VVF
• months to years after treatment (mean presentation 8.7 months)
• Secondary to local endarteritis • Alert et al 1980: 1.6% incidence urinary fistula all
types XRT for cervical CA • Perez et al (1999) incidence of 0.6-2% with XRT and
brachy for stage I-III cervical CA • Langkilde 1998: 6 of 7 post radiation VVF repairs
failed, recommend routine urinary diversion in these cases
• Many suggest abdominal approach and interposition routinely
Risk factors for radiation induced VVF
• Intra-operative injury • prior uterine surgery • endometriosis • infection • Diabetes mellitus • arteriosclerosis • PID • Prior radiation before surgery
1/29/08
7
Etiology: The developing world
• Majority due to obstructed labour (Arrowsmith 1996)
• Wall et al 2004: 96.5% of 932 VVF’s seen at a Nigerian hospital over 7 years associated with labor and delivery
• incidence in developing countries: 0.3-0.4% (Margolis et al 1994)
• Unrepaired fistulas in Nigeria 800,000 to 1,000,000 (Ismail 2001)
Obstructing labor complex (Arrowsmith 1996)
• Urethral loss • SUI • Hydroureteronephrosis • Renal failure • Rectovaginal fistula • Rectal atresia • Anal sphincter
incompetence
• Amenorrhea • Pelvic inflammatory
disease • Secondary infertility • Osteitis pubis • Vaginal stenosis • Footdrop
1/29/08
8
Pathophysiology
• Post hysterectomy • Unrecongnized
iatrogenic cystotomy near vaginal cuff
• Tissue necrosis from cautery/suture placement
• Unknown factors (Meeks et al 1997)
• Obstetric • Pressure necrosis from
prolonged labor to pelvic organs
• Risk factors include young conception age, poor nutrition, absence of qualified personnel and obstetric care.
Clinical presentation
• Constant or intermittent drainage of urine per vagina
• Recurrent cystitis • Perineal skin irritation • Vaginal fungal infections • Pelvic pain (rare)
1/29/08
9
Diagnosis
• Physical exam • Vital dye testing • Vaginoscopy • Cystoscopy • Biopsy (with history of radiation or
malignancy) • Urine analysis, C & S +/- cytology
Vital dye testing
• Methylene blue/indigo carmine • May use speculum exam/tampon • Double dye test
• Methylene blue/indigo carmine instilled into bladder
• Pyridium ingested orally • Tampon in vagina • Blue dye: VVF, orange dye: UVF
1/29/08
10
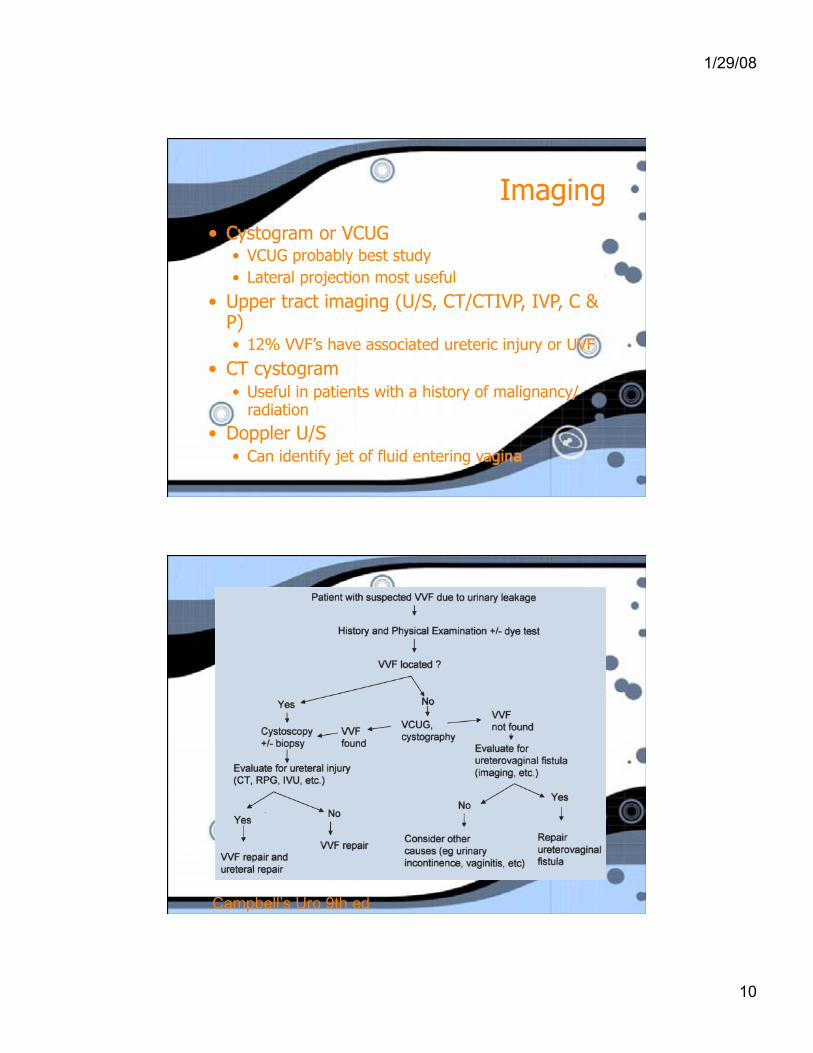
Imaging • Cystogram or VCUG
• VCUG probably best study • Lateral projection most useful
• Upper tract imaging (U/S, CT/CTIVP, IVP, C & P) • 12% VVF’s have associated ureteric injury or UVF
• CT cystogram • Useful in patients with a history of malignancy/
radiation
• Doppler U/S • Can identify jet of fluid entering vagina
Campbell’s Uro 9th ed
1/29/08
11
Hutch’s criteria to prevent VVF during gynecological surgery
(Hutch & Noll 1969) • immediate detection of injury • watertight closure • satisfactory drain placement • avoid vaginal incisions after recognition
of bladder injury • prolonged uninterrupted post op bladder
drainage
Non-operative treatment
• Prolonged bladder drainage • De-epithelialization • Fibrin sealant/collagen injection

1/29/08
12
• Mostly retrospecitve data, poorly defined data points regarding size, location, duration of VVF
• No consensus regarding the possibility of closure of VVF with drainage or the optimal duration of drainage
• Size < 1cm reasonable cutoff • Long interval from causative insult associated
with steeply decreasing chances of spontaneous closure
Fibrin sealant • Pettersen 1979
• 9 patients with chronic urinary fistulas, the only VVF in the group failed to close
• Venkatesh & Ramanujam 1998 • 30 patients with anorectal,
urethrovesicorectal fistulas, all with at least 1 prior repair
• Overall success 60% but both VVF’s failed
1/29/08
13
Fibrin Sealant (continued)
• Tsurusaki • Chronic ureteral fistula from transplant kidney,
sealed with third administration of fibrin sealant
• Evans et al Jurol 2003 • Studied several groups of fistula patients including
a group of traumatic urinary fistulas • 100% success rate with urinary fistulas • Only 1 VVF in the group. Size, location, duration
not disclosed
Surgical options
• Abdominal repair • Vaginal repair • Urinary diversion
1/29/08
14
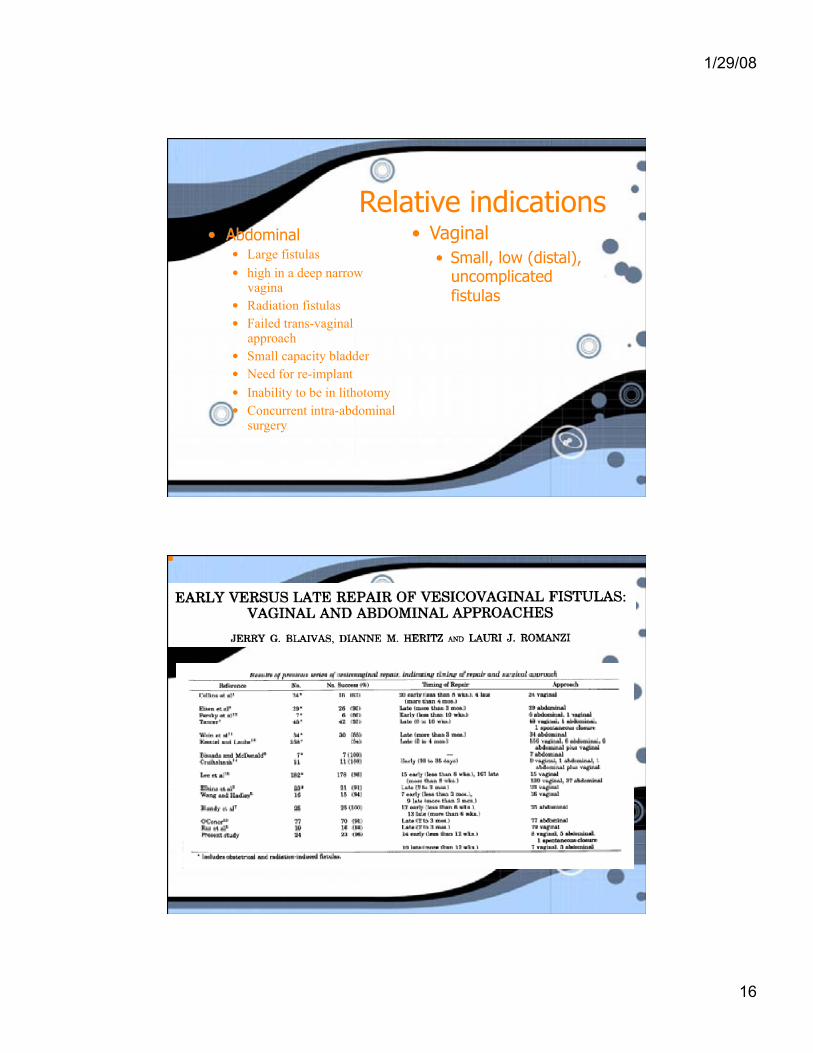
Early vs Late Surgery • All retrospective data, mostly showing no
difference in outcomes • Classic teaching: delay 2-3 months for
surgical VVF, 3-6 for obstetric VVF, and 6-12 months for radiation induced VVF
• In developing countries the advantages of early repair include early continence rehab, decreased waiting times, marital benefit, reduced stigma (Melah et al IJGO 2006)
Early vs Late Surgery
• most authors suggest waiting until inflammation/infection resolved
• Lee et al found VVF’s repaired very early (10-15 days) were more likely to fail
1/29/08
15
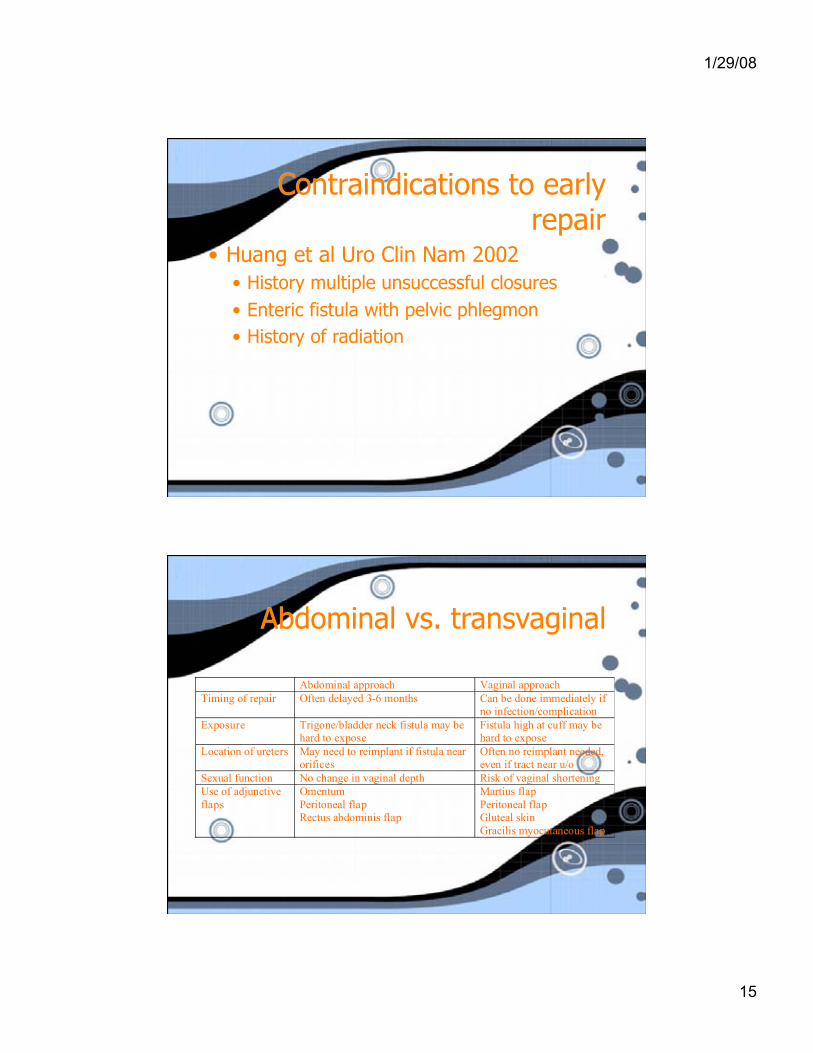
Contraindications to early repair
• Huang et al Uro Clin Nam 2002 • History multiple unsuccessful closures • Enteric fistula with pelvic phlegmon • History of radiation
Abdominal vs. transvaginal
Abdominal approach Vaginal approach Timing of repair Often delayed 3-6 months Can be done immediately if
no infection/complication Exposure Trigone/bladder neck fistula may be
hard to expose Fistula high at cuff may be hard to expose
Location of ureters May need to reimplant if fistula near orifices
Often no reimplant needed, even if tract near u/o
Sexual function No change in vaginal depth Risk of vaginal shortening Use of adjunctive flaps
Omentum Peritoneal flap Rectus abdominis flap
Martius flap Peritoneal flap Gluteal skin Gracilis myocutaneous flap
1/29/08
16
Relative indications • Abdominal
• Large fistulas • high in a deep narrow
vagina • Radiation fistulas • Failed trans-vaginal
approach • Small capacity bladder • Need for re-implant • Inability to be in lithotomy • Concurrent intra-abdominal
surgery
• Vaginal • Small, low (distal),
uncomplicated fistulas
1/29/08
17
To excise or not to excise…
• Raz, Vasavada, Margolis, Mercer: not necessary and possibly detrimental • May increase size of fistula, making it more
unlikely to close • Fibrous ring of the fistula may provide support • Bleeding from resection may compromise healing/
block catheter • Cruikshank et al S Med J 1988: 100% success in
11 patients with no excision
To excise or not to excise…
• Iselin et al J Urol 1998: Yes • Crucial to have healthy tissue apposed • In their series of 20 patients, all healed
with fistula excision
1/29/08
18
To excise or not to excise…
• Remains controversial, no RCT’s to assess the question
• Likely that small fistulas with minimal scarring/inflammation will heal with or without excision
• Larger, inflammed/infected, densely scarred fistulas may require some revision before closure
Antibiotic prophylaxis
• Tomlinson et al BJOG 1998 • Single blind RCT of single dose 500mg of
Ampicillin IV vs placebo prior to obstetric VVF repair in 79 women
• Primary outcomes: VVF repair failure and objective incontinence
• Secondary outcomes: febrile morbidity, antibiotic use, urinary tract infections
1/29/08
19
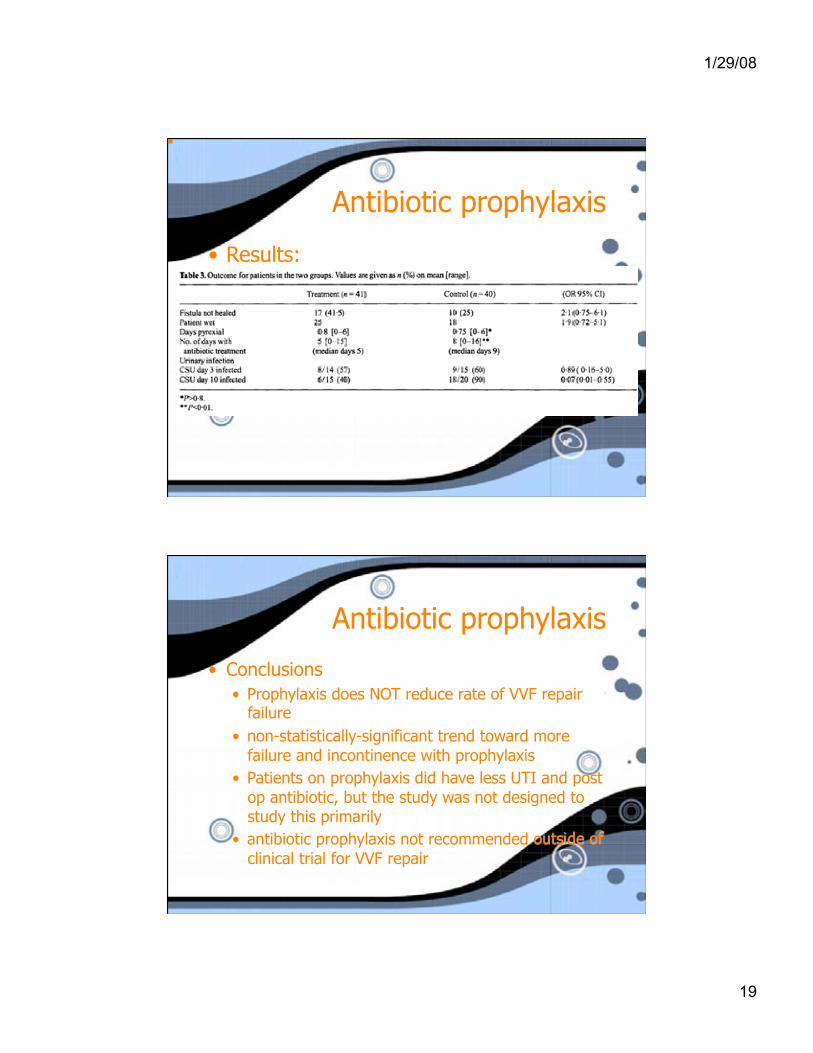
Antibiotic prophylaxis
• Results:
Antibiotic prophylaxis
• Conclusions • Prophylaxis does NOT reduce rate of VVF repair
failure • non-statistically-significant trend toward more
failure and incontinence with prophylaxis • Patients on prophylaxis did have less UTI and post
op antibiotic, but the study was not designed to study this primarily
• antibiotic prophylaxis not recommended outside of clinical trial for VVF repair
1/29/08
20
urinary diversion
• Complex, recurrent, severe VVF’s or those related to radiation
• Conduit diversion or orthotopic • Chronic NT and ureteric occlusion for non-surgical candidates
• Last resort: ureterosigmoidostomy
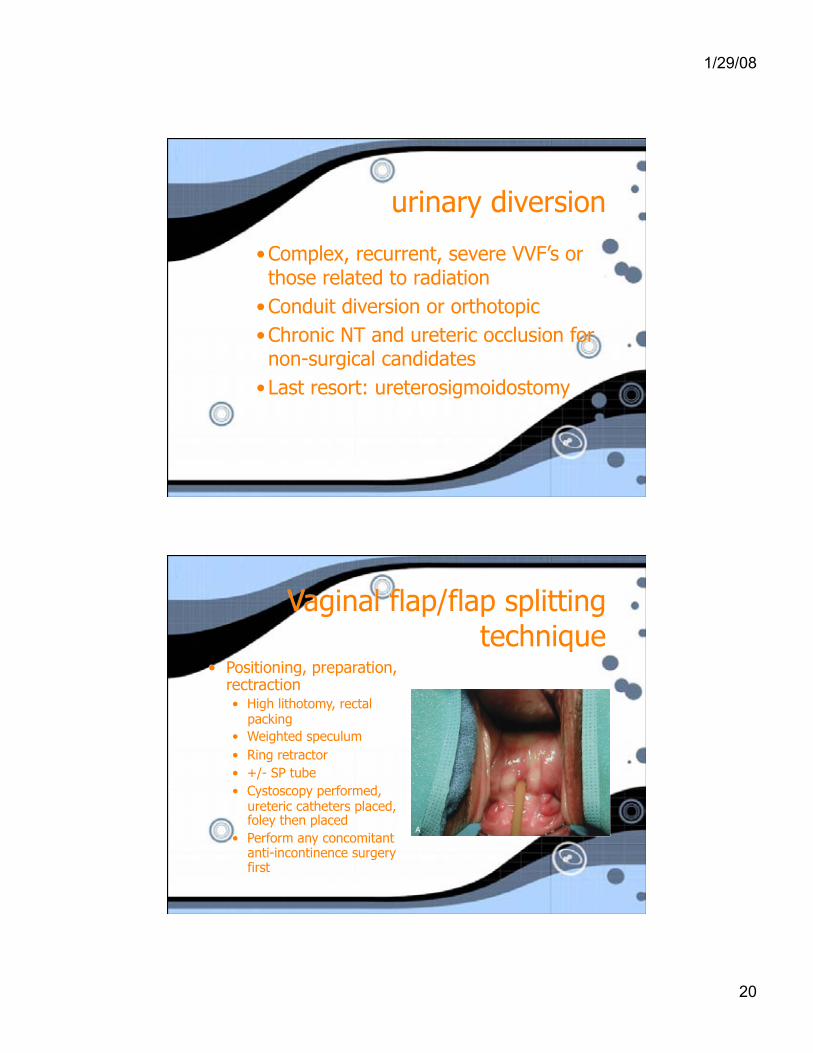
Vaginal flap/flap splitting technique
• Positioning, preparation, rectraction • High lithotomy, rectal
packing • Weighted speculum • Ring retractor • +/- SP tube • Cystoscopy performed,
ureteric catheters placed, foley then placed
• Perform any concomitant anti-incontinence surgery first
1/29/08
21
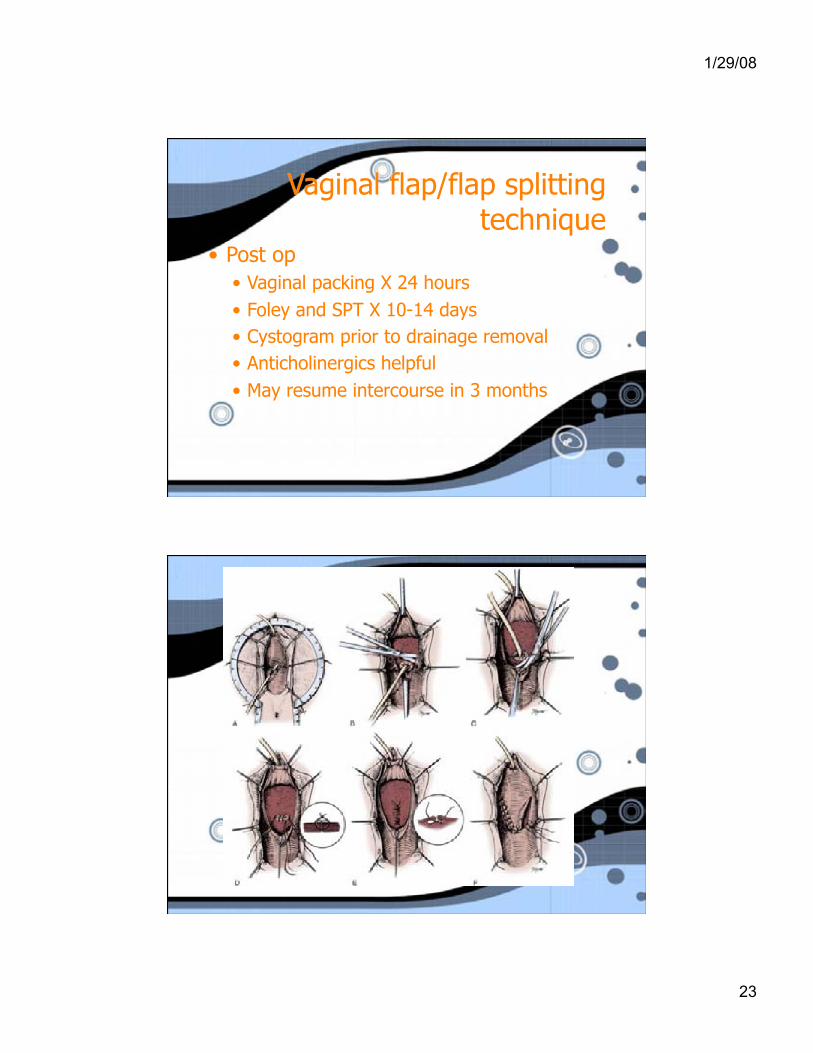
Vaginal flap/flap splitting technique
• Incision • Cannulate tract with
small foley for traction
• Mark out flaps • Inject under mucosa
with N/S or local • Inverted U or J
incorporating fistula
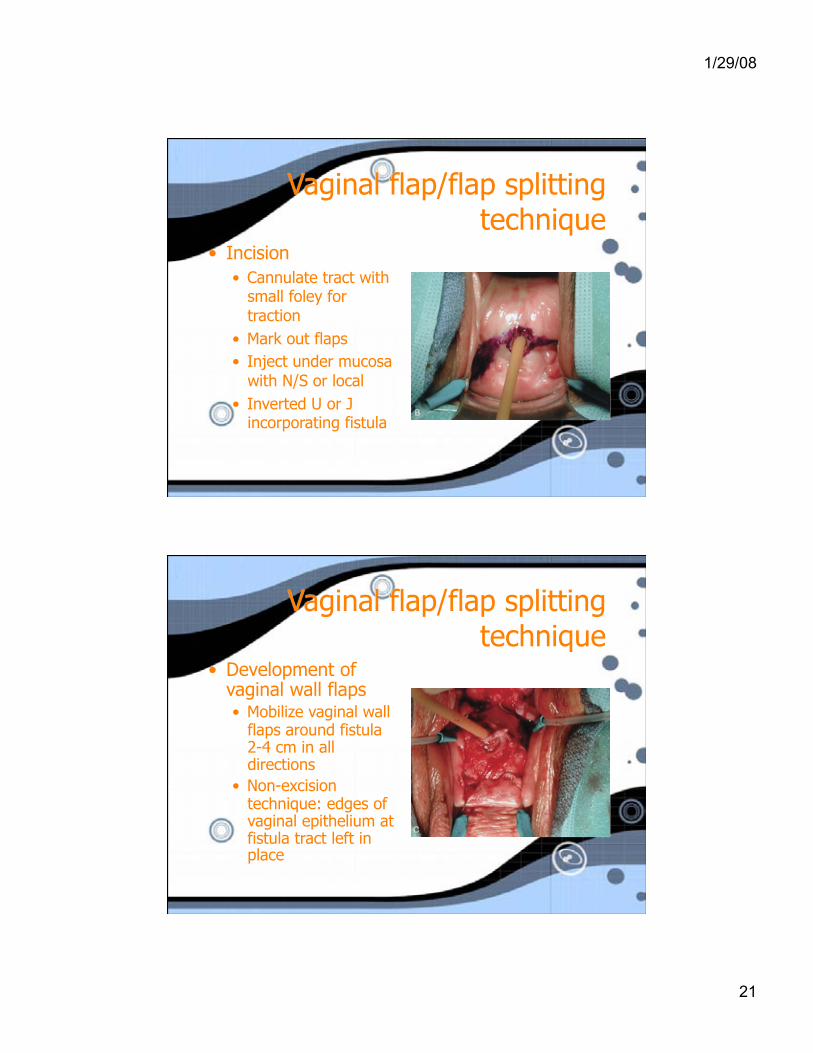
Vaginal flap/flap splitting technique
• Development of vaginal wall flaps • Mobilize vaginal wall
flaps around fistula 2-4 cm in all directions
• Non-excision technique: edges of vaginal epithelium at fistula tract left in place
1/29/08
22
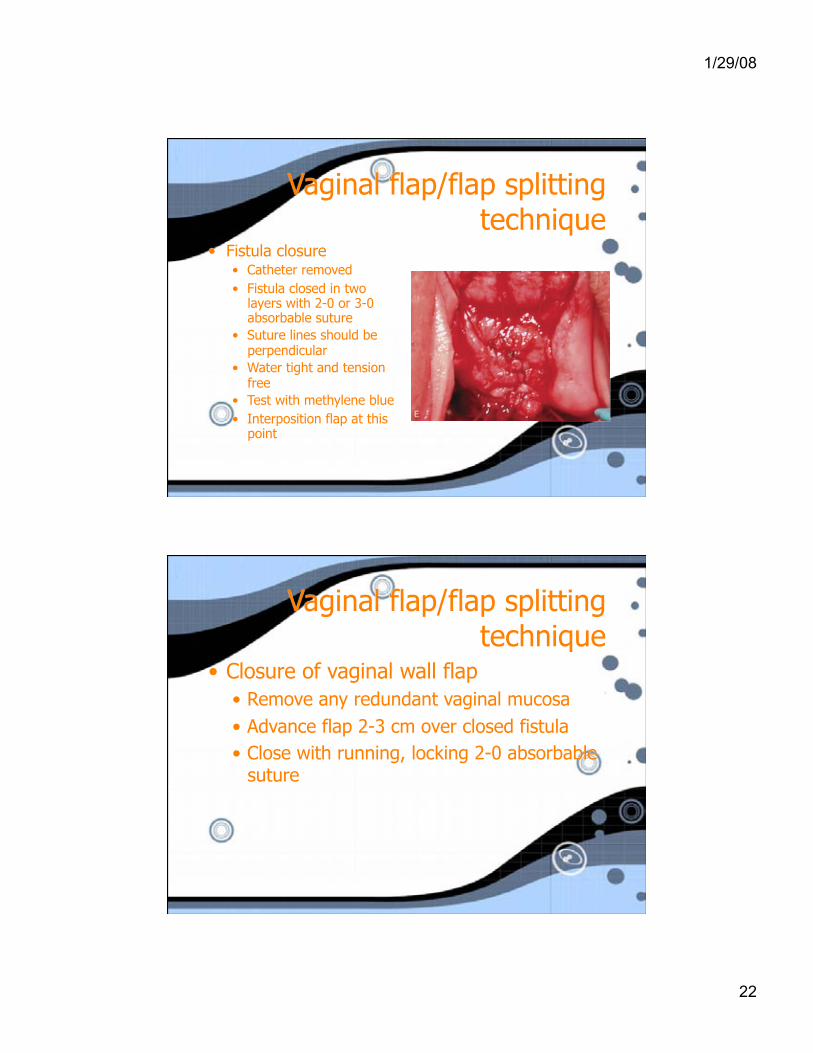
Vaginal flap/flap splitting technique
• Fistula closure • Catheter removed • Fistula closed in two
layers with 2-0 or 3-0 absorbable suture
• Suture lines should be perpendicular
• Water tight and tension free
• Test with methylene blue • Interposition flap at this
point
Vaginal flap/flap splitting technique
• Closure of vaginal wall flap • Remove any redundant vaginal mucosa • Advance flap 2-3 cm over closed fistula • Close with running, locking 2-0 absorbable
suture
1/29/08
23
Vaginal flap/flap splitting technique
• Post op • Vaginal packing X 24 hours • Foley and SPT X 10-14 days • Cystogram prior to drainage removal • Anticholinergics helpful • May resume intercourse in 3 months
1/29/08
24
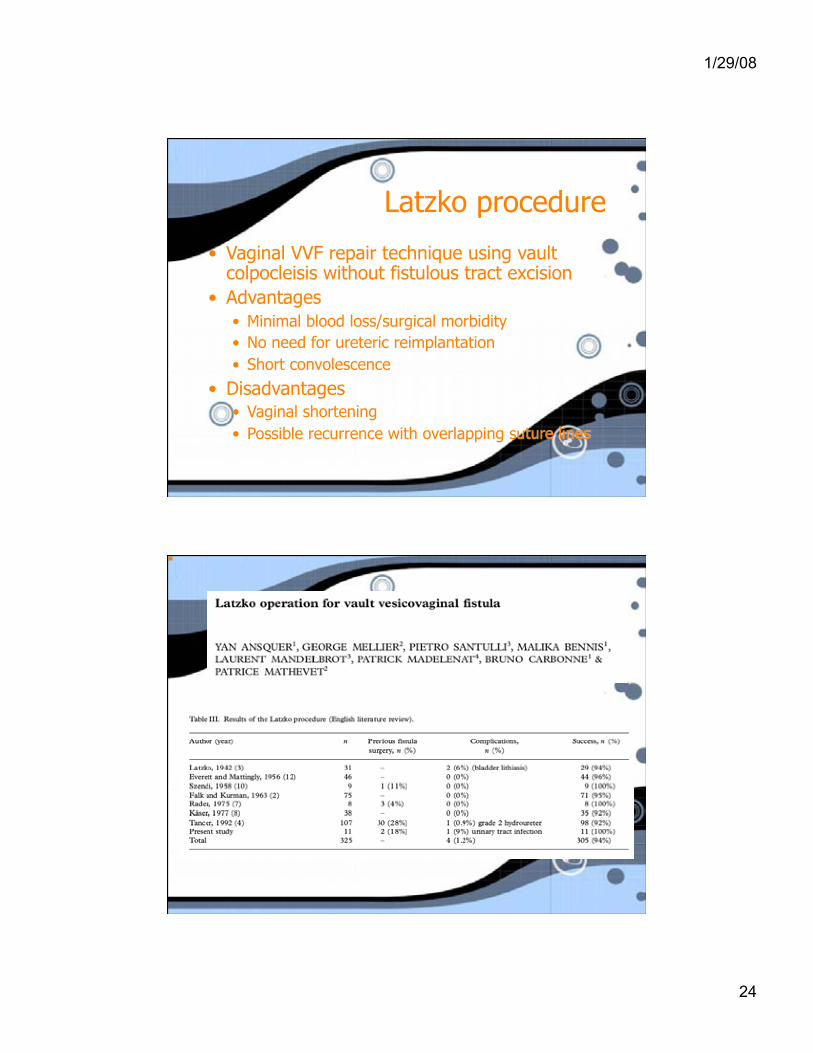
Latzko procedure
• Vaginal VVF repair technique using vault colpocleisis without fistulous tract excision
• Advantages • Minimal blood loss/surgical morbidity • No need for ureteric reimplantation • Short convolescence
• Disadvantages • Vaginal shortening • Possible recurrence with overlapping suture lines
1/29/08
25
Vaginal cuff excision • First described by Iselin in 1998 • Further series (Amundsen 2001, Flynn 2004)
have shown 100% success rates • excision of entire fistulous tract in a wide
inverted cone shaped wedge, multiple layer closure
• No vaginal flaps needed and theoretically no vaginal shortening
• Small studies show limited post op voiding symptoms/sexual dysfunction
Abdominal surgical approaches
• Better for cases where augmentation or reimplantation necessary
• Longer recovery, longer LOS • More blood loss • Greater cosmetic deformity • Intraperitoneal, extraperitoneal,
transvesical approaches
1/29/08
26
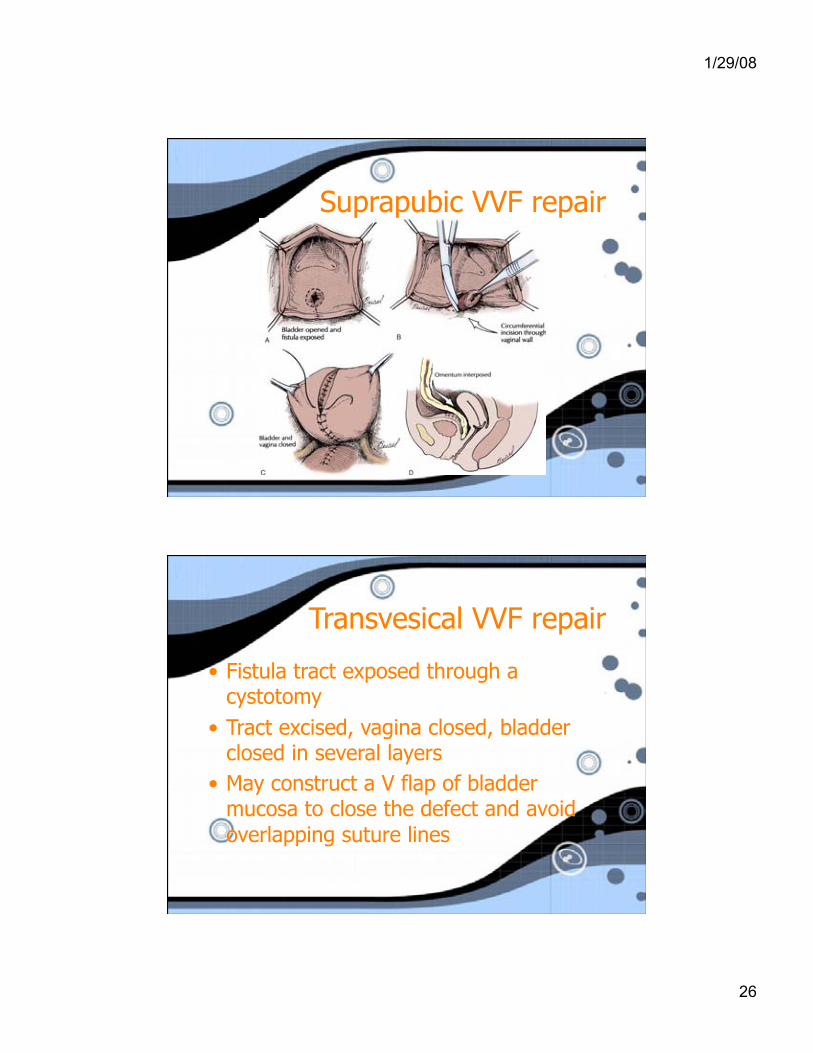
Suprapubic VVF repair
Transvesical VVF repair
• Fistula tract exposed through a cystotomy
• Tract excised, vagina closed, bladder closed in several layers
• May construct a V flap of bladder mucosa to close the defect and avoid overlapping suture lines
1/29/08
27
Tissue Interposition
• Especially useful in large, complex, radiation induced or recurrent fistulas, or when tissue quality is poor
• Most popular/useful are Martius flap, Omental patch, peritoneal flap
• interposition used depends on surgical approach, size and location of fistula, available tissues, and surgeon comfort
1/29/08
28
Martius flap
• First described by Heinrich Martius in 1928 • Most useful for VVF in areas of trigone,
bladder neck and urethra • Blood supply
• Inferior: posterior labial vessels (interna pudendal) • Lateral: obturator artery • Superiorly: external pudendal artery • Flap may be based on either superior or inferior
supply, but usually inferior supply preserved
Martius flap
• Studies show excellent effectiveness with success rates exceeding 90%
• Rangnekar et al 2000: • small series of UVF and VVF, mostly obstetric in
nature • VVF repairs using Martius flap more successful
than anatomic repairs (0/13 failures vs 4/21 failures)
• Recommend routine use of Martius flap, especially with multiple/recurrent fistulas

1/29/08
29
Peritoneal flap
• Most useful in high lying post hysterectomy VVF
• Peritoneum is dissected away from the bladder and vagina until well mobilized then tacked over the VVF repair site

1/29/08
30
Greater Omentum
• Advantages • Able to be mobilized into the pelvis without
tension • Inherent lymphatic properties • Able to promote healing even in the presence of
infection • Ease of epithelialization on its surface
• Blood supply • Main supplies are R and L gastroepiploic arteries • R is usually more robust and further caudad (more
useful for pelvic surgery)
• Retrospective review of 37 abdominal VVF’s between
• 29 VVF of benign etiology, 8 of malignant etiology
• 100% success rate when interposition flap used (omentum or peritoneum)
• Size, location of tissue quality did not affect outcome
• They recommend routine use of interpositions with abdominal approaches to VVF repair
1/29/08
31
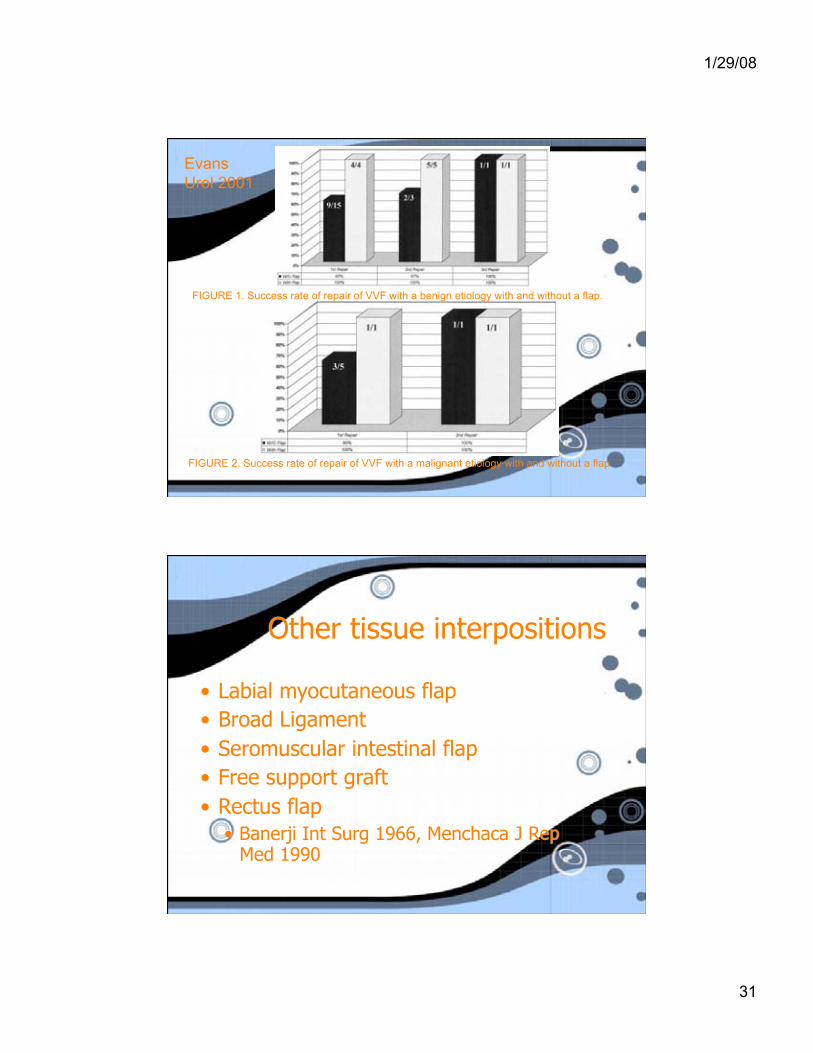
FIGURE 1. Success rate of repair of VVF with a benign etiology with and without a flap.
FIGURE 2. Success rate of repair of VVF with a malignant etiology with and without a flap.
Evans Urol 2001
Other tissue interpositions
• Labial myocutaneous flap • Broad Ligament • Seromuscular intestinal flap • Free support graft • Rectus flap
• Banerji Int Surg 1966, Menchaca J Rep Med 1990
1/29/08
32
Other tissue interpositions
• Anterior or posterior bladder flaps • Gil-Vernet J Urol 1989
• Gracilis flap • Free bladder mucosal flap
• Brandt J Am Coll Surg 1998, Vyas BJOG 2005
• Dura Mater • Alagol Int Ur Neph 2004
Complications of VVF repair
• Bleeding • Ureteric injury • Vaginal shortening/stenosis (vaginal
approaches) • Recurrence of fistula • Incontinence • Detrusor overactivity
1/29/08
33
Post VVF repair incontinence
• Incidence between 8 and 33% (Kelly IJU 1993, Browning IJUG 2004)
• Mostly SUI, some detrusor overactivity • More severe with greater urethra/bladder
neck involvement • Browning 2004: described bulbocavernosus
sling at time of VVF repair • 18/20 “simple” and 4/7 “complex” VVF patients
continent post op
Urodynamic abnormalities in VVF patients
• Hilton et al BJU 1998 • CMG of 30 patients prior to and after VVF repair
• 47% showed SUI • 40% showed DO • 50% had voiding dysfunction • Only 17% had normal urodynamics • Abnormalities most pronounced with urethral/bladder
neck involvement
• 10 patients had post op voiding sx • 1 sx of SUI, 9 urge/UUI • UDS showed 1 SUI, 4 DO • No normal women had abnormal UDS post op
1/29/08
34
Emerging VVF repair techniques
• Laprascopic repair • Robot-assisted repair • Transurethral endoscopic repair
Laprascopic VVF repair
• Theoretical advantages • Magnification • Better hemostasis • Decreased pain • Decreased length of stay • Quicker convalescence and return to work
1/29/08
35
Laprascopic VVF repair
• First reported lap VVF repair Nezhat 1994 • Patient had VVF secondary to laprascopic
treatment of ovarian remnant syndrome • 85 min, 100 cc blood loss, LOS 1 day
• Seven reports in the literature, mostly case reports, small series
• Review of 15 VVF’s repaired laprascopically between 1998-2004
• 93% were post hysterectomy • All had a trial of at least 2 months
conservative treatment • All patients worked up with physical
exam, cystoscopy, retrograde pyelogram and IVP
1/29/08
36
technique
• Low lithotomy position • Cystoscopy, both ureters catheterized • Fistula catheterized with ureteric
catheter or foley • Sponge in vagina as a retractor
Technique (continued) • Bladder opened with harmonic scalped down
to fistula • Tract excised • Bladder dissected from vagina sharply • Bladder closed in two layers, vagina closed
perpendicular to bladder layer (1 layer) • Omental flap used in all patients • Foley catheter and JP drain • Foley out POD #10 with cystogram
1/29/08
37
results
• Mean age 38.8 • Mean F/U 26.2 months • 14 due to hysterectomy, 1 due to obstructed
labor (twins) • 4 had previously failed surgery for VVF • Average OR time: 170 minutes • Average LOS: 3 days • Success rate 93.7%
Sotelo Jurol 2005
complications
• 1 enterocutaneous fistula (closed with conservative treatment)
• 1 inferior epigastric artery injury requiring repeat OR
• 1 failure of laprascopic VVF repair (large, fibrotic fistula)
Sotelo Jurol 2005
1/29/08
38
• Case series of laprascopic intraperitoneal “high up” VVF repair in 12 patients (2007)
• Selection criteria • > 3 months of leakage • Single fistula • At least 6 cm from urethral meatus • No previous failed repair • No ureteric involvement
Mahapatra et al Int Urogyn 2007
• Technique: • Similar exposure and tract excision to that
described by Sotelo et al • Fistula only closed in one layer (bladder
side) with omental interposition • Vaginal wall NOT closed (open to allow
drainage)
1/29/08
39
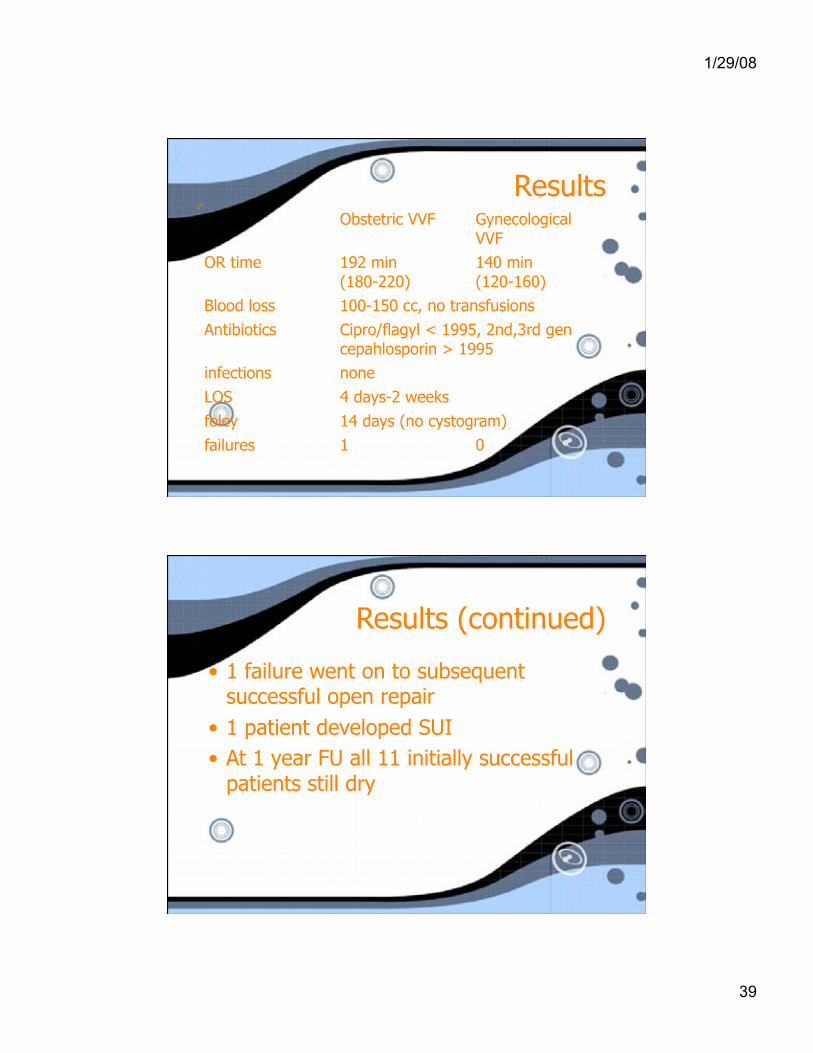
Results Obstetric VVF Gynecological
VVF OR time 192 min
(180-220) 140 min (120-160)
Blood loss 100-150 cc, no transfusions Antibiotics Cipro/flagyl < 1995, 2nd,3rd gen
cepahlosporin > 1995 infections none LOS 4 days-2 weeks foley 14 days (no cystogram) failures 1 0
Results (continued)
• 1 failure went on to subsequent successful open repair
• 1 patient developed SUI • At 1 year FU all 11 initially successful
patients still dry
1/29/08
40
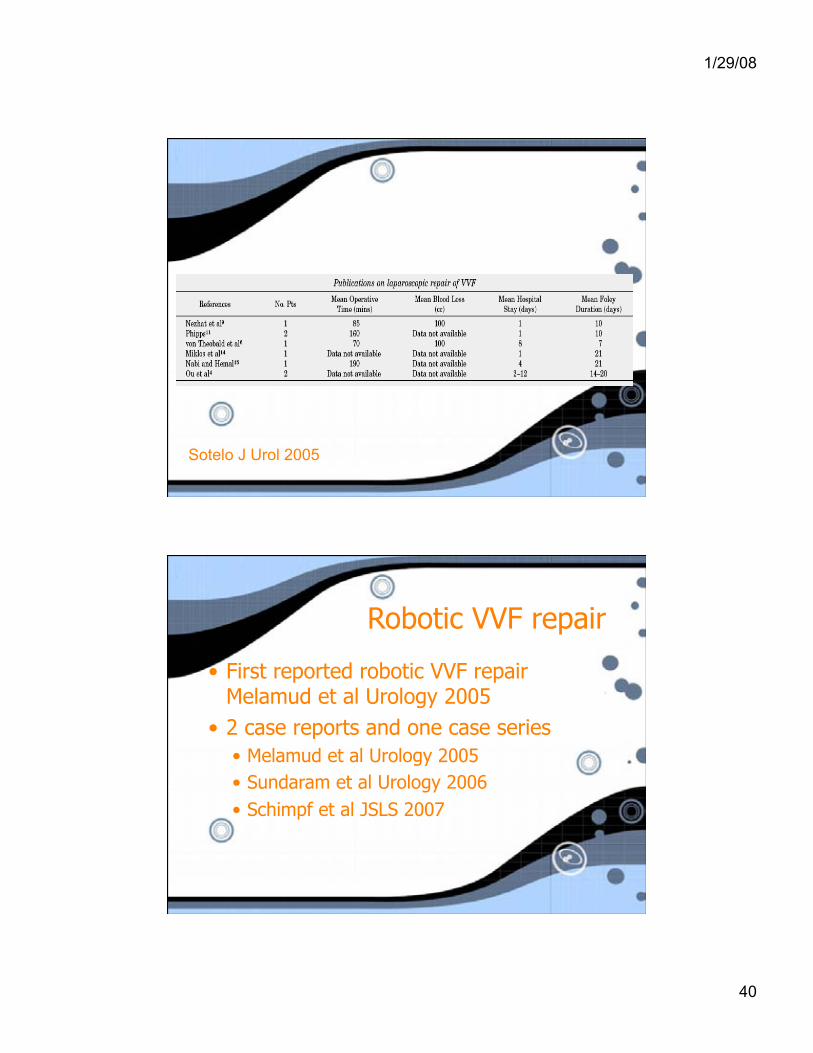
Sotelo J Urol 2005
Robotic VVF repair
• First reported robotic VVF repair Melamud et al Urology 2005
• 2 case reports and one case series • Melamud et al Urology 2005 • Sundaram et al Urology 2006 • Schimpf et al JSLS 2007

1/29/08
41
• series of 5 patients
• ages 26-68
• 4 hysterectomy related VVF, 1 myomectomy related VVF
• all cases had trial of conservative management
• all had supratrigonal fistulas and were deemed unsuitable for vaginal procedures
technique
• Similar to laprascopic technique previously described
• 5 port access similar to DaVinci Prostatectomy • Wet sponge in vagina used to maintain
pneumoperitoneum • Bladder closed in two layers, vagina in one
layer, omental flap used • Foley removed POD # 10 with cystogram
1/29/08
42
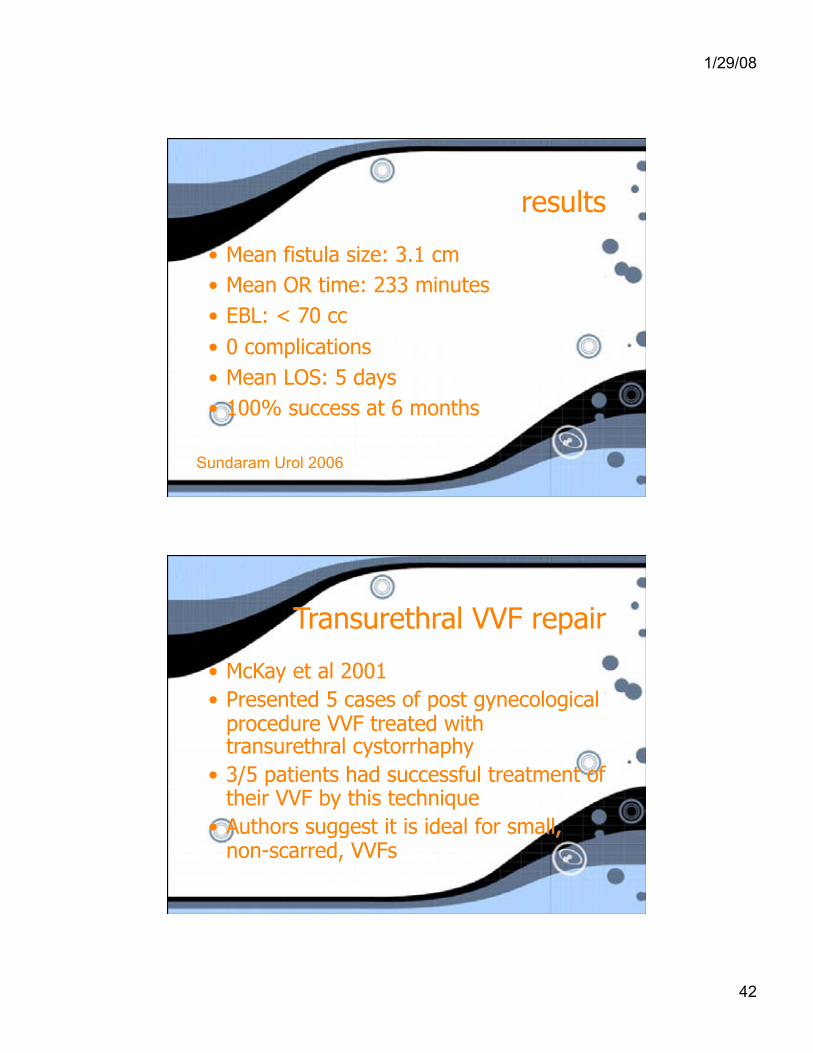
results
• Mean fistula size: 3.1 cm • Mean OR time: 233 minutes • EBL: < 70 cc • 0 complications • Mean LOS: 5 days • 100% success at 6 months
Sundaram Urol 2006
Transurethral VVF repair
• McKay et al 2001 • Presented 5 cases of post gynecological
procedure VVF treated with transurethral cystorrhaphy
• 3/5 patients had successful treatment of their VVF by this technique
• Authors suggest it is ideal for small, non-scarred, VVFs
1/29/08
43
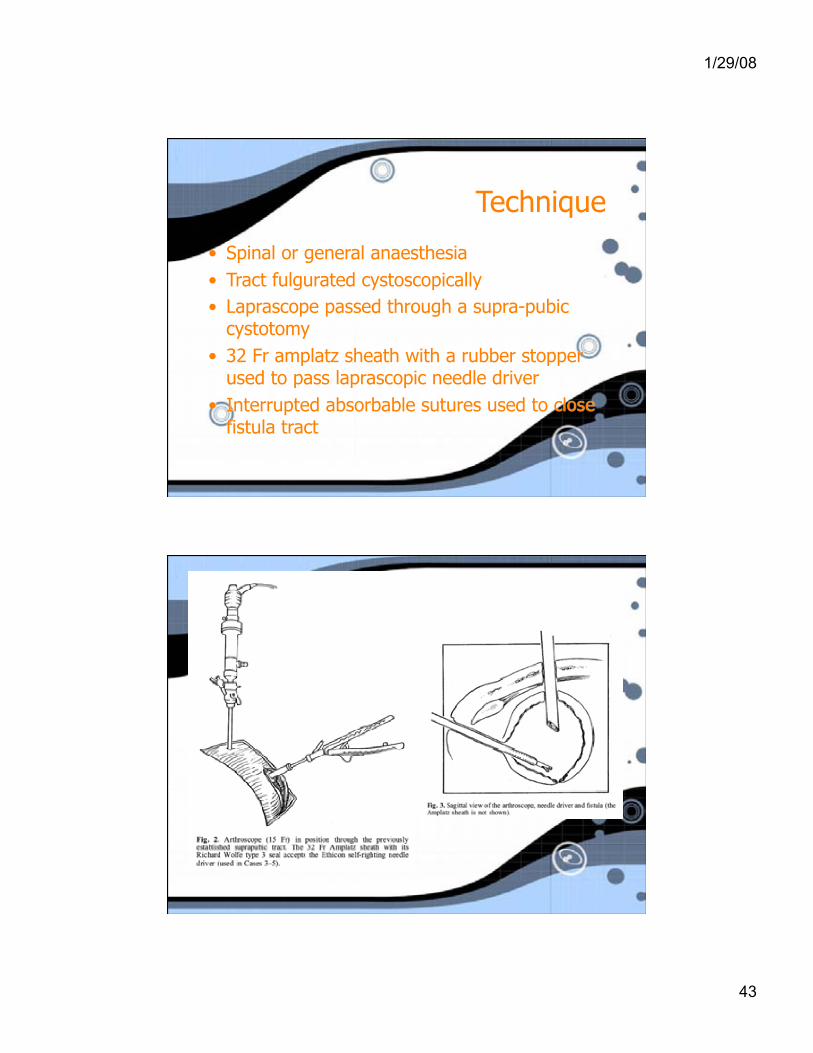
Technique
• Spinal or general anaesthesia • Tract fulgurated cystoscopically • Laprascope passed through a supra-pubic
cystotomy • 32 Fr amplatz sheath with a rubber stopper
used to pass laprascopic needle driver • Interrupted absorbable sutures used to close
fistula tract
1/29/08
44
Minimally invasive VVF repair • Initial results are encouraging for laprascopic
and robot-assisted VVF repair, especially for more proximal fistulas not amenable to vaginal repair
• No RTC to compare with open/vaginal techniques
• Perception that laprascopic VVF repair is technically difficult
• Robot-assisted repair may present a realistic alternative to surgeons without advanced laprascopic skills
Obstetric Fistulas in the Developing World
• WHO estimates 2 million untreated obstetric fistulas worldwide, incidence of 100,000
• Mostly in sub-saharan Africa • 60% or less of births have professional
present, 10% have no trained attendant • Additional morbidity includes fetal demise,
social ostracism and early death
1/29/08
45
Addis Ababa Hospital • Founded in 1974 by Drs.
Reginald and Catherine Hamlin
• Have treated 30,000 women over 33 years
• Now operate out of Addis Ababa and 3 satellite fistula centres
• Provide surgery, rehabilitation, counselling, education
• Many former patients become nurses’ aides
Addis Abab Hospital
• In 2003, their supporting foundation received 1.3 million US$ in donation
• Why?
1/29/08
46
“Fistula tourism”
• Many fistula centres staffed by visiting North American/European surgeons
• Growing concern that although well intentioned, their short tenures and use of limited resources are not as helpful as promoting local solutions
1/29/08
47
Wall et al 2006
• Many visiting surgeons visit for “an experience” and are not specifically trained to deal with this pathology
• Social aspects often forgotten • Long term care and follow up must be
assured • Use of innovative procedures must be within
confines of EBM and ethical practice
Suggestions for improvement
• $$$ • Long term commitments • “Fistula champions” • Academic partnerships • Development of infrastructure • Holistic care approach
1/29/08
48
Morgan IUGJ 2007
• “Fistula tourism” derogatory • Many surgeons with diverse backgrounds will
bring skills to desperately needed areas • Innovation necessary, especially given
constraints • One “champion” not needed, comprehensive
program needed • Academic partnership not needed,
development needed
Conclusions
• Etiology of VVF differs in developed/devloping world
• Work up includes P/E, imaging, direct visualisation, dye testing
• Debate continues regarding early/late repair, tract excision and approach
1/29/08
49
Conclusions
• Overall vaginal and abdominal techniques have high success rates, especially with interposition
• Lap/robotic/transurethral repairs investigational but show promise
• 3rd world fistulas remain a complex medical/social problem requiring ongoing effort locally and internationally
Thank you!!!












![Aetiology of Vesico Vaginal Fistula …P. Majinge et al. 650 der, ureter and/or the uterus, cervix and/or vagina [2]. The physical result of urinary incontinence has profound social](https://img.pdfslide.us/doc/110x75/5e52cfd79cb8e03fca620d87/aetiology-of-vesico-vaginal-fistula-p-majinge-et-al-650-der-ureter-andor-the.jpg)
















