Embed Size (px)
DESCRIPTION
Ventilator Modes & RN Role of Ventilator Patients in ICU. Microteaching Project ICU Clinical Pre-Conference. Objectives. Comprehend the purpose of different ventilator modes and settings and apply to patient case study. - PowerPoint PPT Presentation
Citation preview
Ventilator Modes & RN Role of Ventilator
Patients in ICU Microteaching Project
ICU Clinical Pre-Conference
Objectives
Comprehend the purpose of different ventilator modes and settings and apply to patient case study.
Apply ABG interpretation knowledge to case study and adjust vent settings accordingly.
Identify important nursing implications when taking care of a patient on a ventilator.
Demonstrate understanding of ventilator settings, modes, and the nursing role during this ICU clinical experience.
ICU PATIENT CASE A 68 year old female patient with history of COPD is admitted
for pneumonia and respiratory distress. She is intubated in the Emergency room and following are the initial ventilator settings:
Pt weighs 175 pounds
CMV
Vt: 700 ml
FiO2: 100%
Rate: 12 bpm
Peep: +5 cm H2O
Pressure Support (PS): N/A
What does all this mean???
VENTILATOR MODES
CONTROLLED MECHANICAL VENTILATION (CMV)
SYNCRONIZED MECHANICAL INTERMITTENT VENTILATION (SIMV)
PRESSURE CONTROL VENTILATION (PC)
CPAP
EXTUBATED THEN WHAT??
VENTILATOR SETTINGS
MODE: a preprogramed settings that tells the ventilator how to oxygenate the patient
Vt (Tidal Volume): How big a breath the lungs need to fully inflate. This is weight based and calculated, ~8-10 ml/kg. In our example, pt weigh 80 kgs, so her needed Vt is ~650-700 ml.
FiO2: Oxygen requirement in percentage (ex. 40%, 80%, 100%)
Rate: how many breaths per minute the patient needs a breath PEEP: positive end expiratory pressure
Pressure Support (PS): a small “boost” or “step stool” of breath to help the patient get to their full tidal volume for best alveoli inflation and gas exchange potential.
CONTROLLED MECHANICAL VENTILATION(CMV)
It gives the patient a set tidal volume at a set time with almost no variation. The vent is “essentially blind” to the what the patient is doing. The patient’s with this type of ventilation are fully sedated, sometime paralyzed for medical is a good se therapy, and not taking any breaths on their own. It is a setting to allow the patient’s lungs to “rest”.
Our patient example:
Vent Orders:
Pt weighs 175 pounds
CMV
Vt: 700 ml
FiO2: 100%
Rate: 14 bpm
Peep: +5 cm H2O
Pressure Support (PS): N/A
About 30 minutes after Initially intubation….
Blood gases are collected and analyzed….
Here are her initial blood gases:
pH: 7.25
PaCO2: 82
HCO3: 24
PO2: 180
Base Excess: -1.8
Critical Thinking Discussion:
What’s your interpretation of her blood gases?
What needs changing?
What else do you want to know?
SYNCHRONIZED INTERMITTENT MECHANICAL VENTILATION (SIMV)
Three days later, our female patient is improving and is beginning to start the weaning process. The physician changes the ventilator orders to this:
SIMV
Vt: 700 ml
FiO2 40%
Rate: 10
PEEP: +5 mmHg
PS: 10
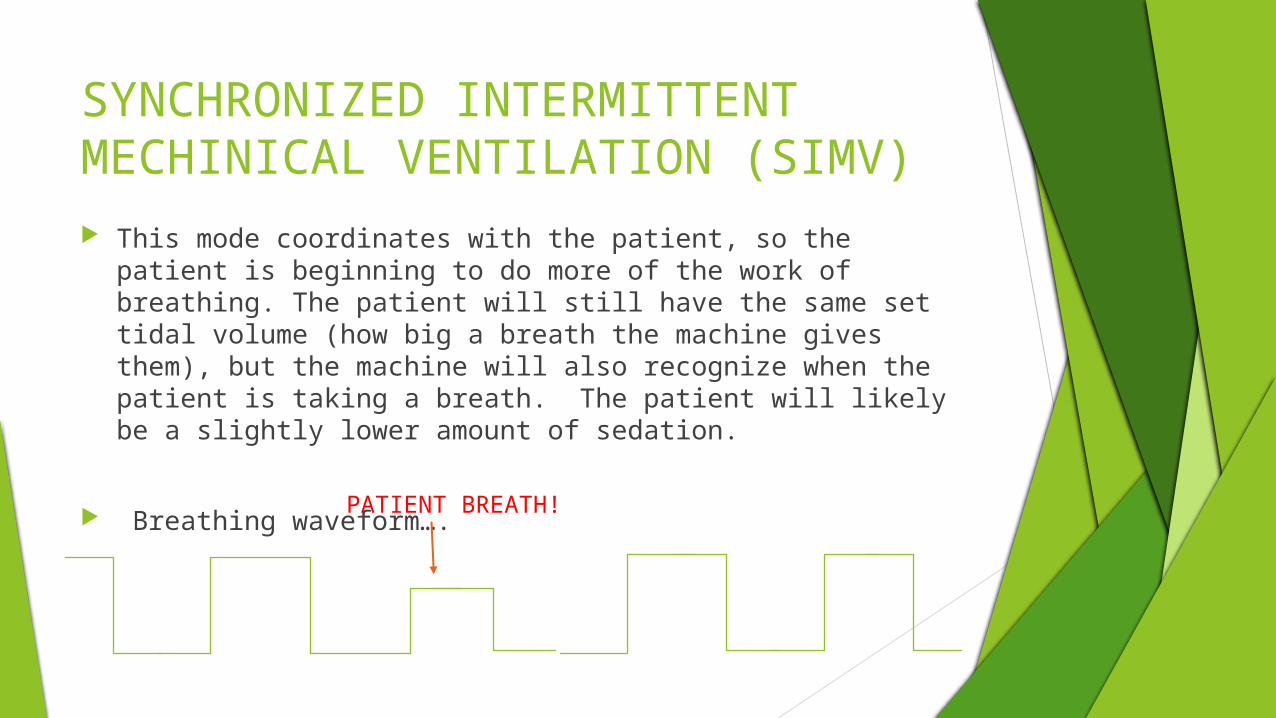
SYNCHRONIZED INTERMITTENT MECHINICAL VENTILATION (SIMV) This mode coordinates with the patient, so the patient is
beginning to do more of the work of breathing. The patient will still have the same set tidal volume (how big a breath the machine gives them), but the machine will also recognize when the patient is taking a breath. The patient will likely be a slightly lower amount of sedation.
Breathing waveform….PATIENT BREATH!
What’s PS?? SIMV
Vt: 700 ml
FiO2 40%
Rate: 10
PEEP: +5 mmHg
PS: 10
Pressure Support (PS): a small “boost” or “step stool” of breath to help the patient get to their full tidal volume for best alveoli inflation and gas exchange potential.
Critical Thinking DiscussionHOW DOES PS BENEFIT THE PATIENT?
WHAT WOULD HAPPEN IF THERE WAS NO PRESSURE SUPPORT?
AGAIN ABOUT 30-45 MINUTES AFTER ANY CHANGES, NEW BLOOD GASES ARE (USUALLY)
COLLECTED…..
New Blood Gas Results: pH: 7.34 PaCo2: 55 HCO3: 24 O2: 98
Critical Thinking Discussion:
What’s your interpretation of her blood gases?
What needs changing?
What else do you want to know?
Continued Weaning….
Pt is doing well on last change. RR 12-20 depending on rest. Two days later, the patient is cooperative, tolerating the vent, and CXR is improved after the last 5 days of antibiotics. Now what??
Physician rounds and makes more vent changes.
New Orders: CPAP FiO2 40% PEEP: +5 cm H2O
Continuous Positive Airway Pressure (CPAP)
OSA: CPAP at home is External and bleeds in room air or in some cases oxygen if the patient needs it.
CPAP mode: Similar except it is Invasive via the OETT. This is essentially like a “test” mode to see if the patient is ready for extubation. Intubation is very traumatic to larynx, vocal cords, and trachea.
Critical Thinking : How else do you know CPAP?
Ready for Extubation?? Our female patient is responsive, follows commands, is calm with
minimal sedation. She is breathing 12-18 bpm on the vent, and maintain a SaO2 of 95-97%. Her lung sounds are clear.
Let’s extubate…..to what?
Which of the following modalities would be best? Why??
A. 100% Non-rebreather
B. 80% Partial rebreather
C. 50% Venti Mask
D. 6 L Nasal Cannula
E. 4L Nasal Cannula
F. 2L Nasal Cannual
G. Room Air
Pressure Control Ventilation Let’s change our patient’s lung condition from COPD to
pulmonary fibrosis or Adult Respiratory Distress Syndrome (ARDS). This conditions make the lung very FRIABLE, FRAGILE, STIFF, AND DIFFCULT TO VENTILATE. Control mode ventilation we have discussed will likely not benefit this situation.
Pressure Control Ventilation sets the Inspiratory Pressure and Expiratory Pressure. It does not use Tidal Volume.
PC Inspiratory Pressure (I:15)
PC Expiratory Pressure (E:5), just like PEEP as you already know.
FiO2: 60%, or whatever is necessary to keep SaO2 > 92%.
Rate: 14-18.
No Tidal Volume, No Pressure Support!
Similar to Invasive Bi-PAP
Nursing Role: Patients on Ventilators
Stay in collaboration with your Respiratory Therapist….Learn to read CXR.
Monitor SaO2, Respiratory Rate q1h. Observe how patient is breathing.
Follow vent changes. Respiratory Therapist will round on these patient q2hours and give treatments q4h and PRN.
Learn how to read where an OETT is taped, and how to listen for an “air leak”.
Get to know breathing medications and their side effects even if you aren’t administering them. Some can cause tachycardia & tremors!
Listen to BS at least q2h.
Nursing Role: Patient on Ventilators
Mouth Care q2-4 hours. Learn how to suction and perform q2h and PRN. Do
not irrigate OETT with saline prior to suctioning. Assess secretions (Color, Consistency, Amount) and
document. Monitor and document for changes in these secretions.
Turn patient q2h and learn if the patient’s bed has kinetic therapy.
Educate family on coughing..…It’s going to happen!
Nursing Role: Patient on Ventilators
Feeding
Analgesic
Sedation
Thrombolembolic
Head of Bed <30 degrees
Ulcer Prophylaxis
Glucose Control
FAST HUG
References
Kherallah, Mazen (2011). Basic ventilator modes. PDF power point retrieved September 28, 2014 from http://www.mecriticalcare.net/downloads/lectures
Muthiah, Muthiah P. (2012). “Basics of mechanical ventilation”. PDF power point retrieved September 28, 2014 from
http://www.uthsc.edu/Internal/docs/