Embed Size (px)
Citation preview
Epidemiology of Ventilator Associated Pneumonia in an
Adult ICUImperial College Healthcare NHS Trust, St Mary's
Campus, London
Kingston H, Sange M, Rey V, Jepson A, Stotz M
IntroductionVentilator Associated Pneumonia (VAP)
Pneumonia following 48h invasive ventilationIncidence 8‐28%*Mortality 24‐50%*Interventions reduce riskCostlyBSAC HAP (including VAP) guidelines, 2008†
*Chastre J et al. AJRCCM; 2002:165, 867-903†Masterton RG et al. JAC; 2008:62, 5-34
BackgroundAims of our project (audit)
Review incidence of VAP on St. Mary’s ICUOrganisms and susceptibilitiesCalculate cost of antibioticsAudit the diagnosis of VAP
St Mary’s adult ICUA 13 bed closed general ICUElectronic records
Suspicion of VAP
Patients with suspected VAP started on antibiotics
Vancomycin + piperacillin/tazobactam standard first lineVancomycin discontinued 48h if no MRSAPiperacillin/tazobactam 5 days initially
Bronchoalveolar lavage (BAL) taken firstNon‐directed unless formal bronchoscopy indicated
Definition of VAPBacteriological criteria
BAL with ≥ 104 potentially pathogenic organisms
Clinical criteriaImaging:
New or progressive infiltratesAnd 2 of:
WCC > 12 x 109/L or < 4 x 109/LTemperature > 38˚CPurulent sputum
AJRCCM; 2005:171, 388-416
ResultsNumber of
patients%
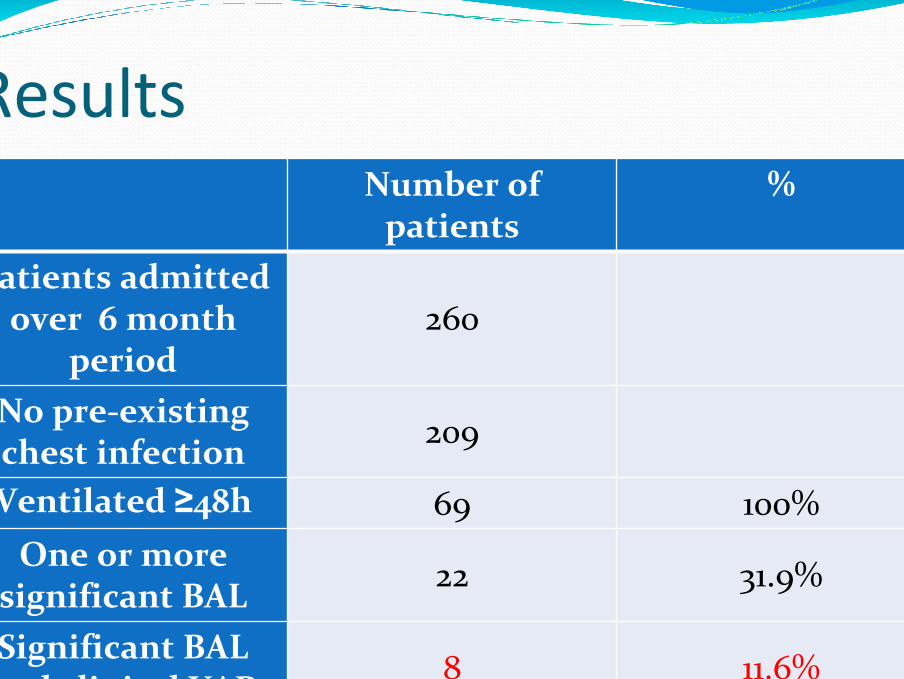
Patients admitted over 6 month
period260
No pre‐existing chest infection 209
Ventilated ≥48h 69 100%One or more
significant BAL 22 31.9%
Significant BAL and clinical VAP 8 11.6%
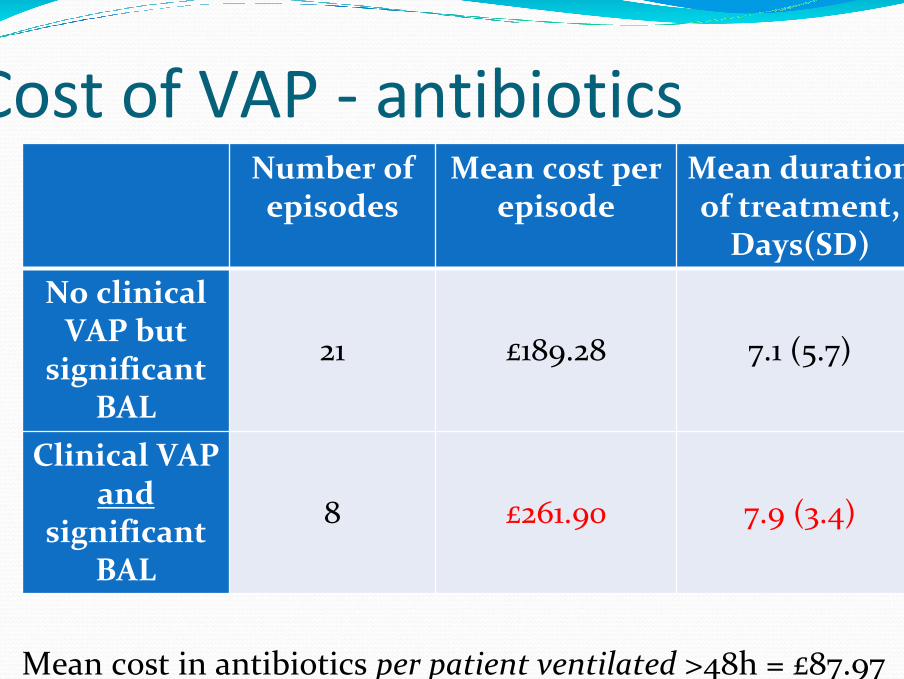
Cost of VAP ‐ antibiotics
Mean cost in antibiotics per patient ventilated >48h = £87.97
Number of episodes
Mean cost per episode
Mean duration of treatment,
Days(SD)No clinical
VAP but significant
BAL
21 £189.28 7.1 (5.7)
Clinical VAP and
significant BAL
8 £261.90 7.9 (3.4)
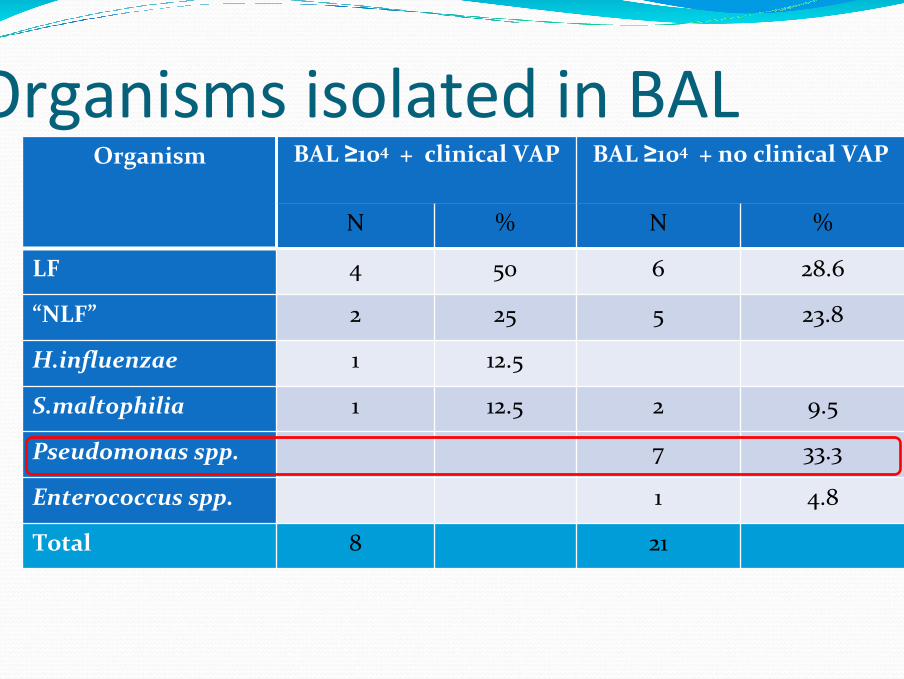
Organisms isolated from BAL
Organism BAL ≥104 + clinical VAP BAL ≥104 + no clinical VAP
N % N %
LF 4 50 6 28.6
“NLF” 2 25 5 23.8
H.influenzae 1 12.5
S.maltophilia 1 12.5 2 9.5
Pseudomonas spp. 7 33.3
Enterococcus spp. 1 4.8
Total 8 21
Organisms isolated in BAL
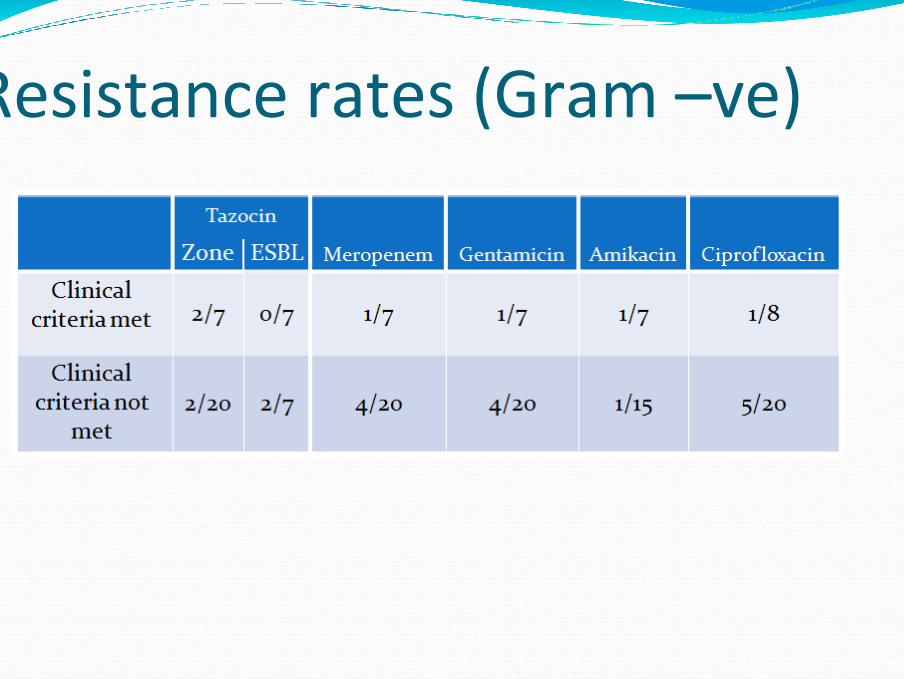
Resistance rates (Gram –ve)
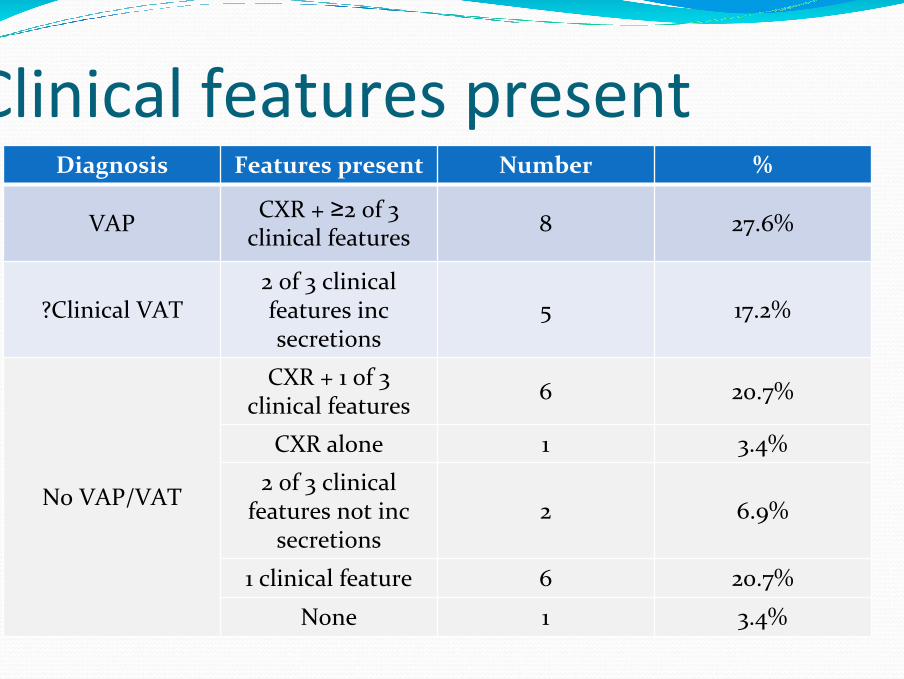
Clinical features presentDiagnosis Features present Number %
VAP CXR + ≥2 of 3 clinical features 8 27.6%
?Clinical VAT2 of 3 clinical features inc secretions
5 17.2%
No VAP/VAT
CXR + 1 of 3 clinical features 6 20.7%
CXR alone 1 3.4%
2 of 3 clinical features not inc
secretions2 6.9%
1 clinical feature 6 20.7%
None 1 3.4%
Recording of DiagnosisIn none of the 8 cases was a diagnosis of VAP found anywhere within the electronic notesIn 3 of the 8 cases a lower respiratory tract infection of some kind was coded for.Implies lack of consideration of pneumonia as a noteworthy entity
perhaps due to continuum ‘no pneumonia – VAT –VAP’Uncertainty when to diagnose itDiagnosis made days after treatment started
ConclusionIncidence of VAP low
Only microbiologically confirmed VAPInsensitive clinical criteriaNot all patients may get BAL doneFalse negative BAL
ExpensiveLocal variation in pathogensVariation in pathogens isolated from BAL depending on if clinical criteria metSignificant BAL in absence of clinical VAP
PerspectivesRaise VAP awarenessInterventions to implement?
?Anaesthetic hygieneVentilator Care BundleKinetic bedsSpecial ET tubes
Subglottic suctioningSilver coated
All patients with clinical criteria need BALRe‐Audit