Embed Size (px)
Citation preview
Venous Thromboembolism
and You!
Global Distributor Summit
Las Vegas, 3rd June 2013
• Aetiology of VTE and where DJO fits
• DJO Product Offering
– VenaFlow Elite
– VenaPure
• Key Clinical Aspects for Combined Prophylaxis
• Implications for Pharmacological Prophylaxis
• VTE: A Hospital Acquired Condition
– Is it just Orthopaedics?
• VenaFlow S Mode
– What is it and Why
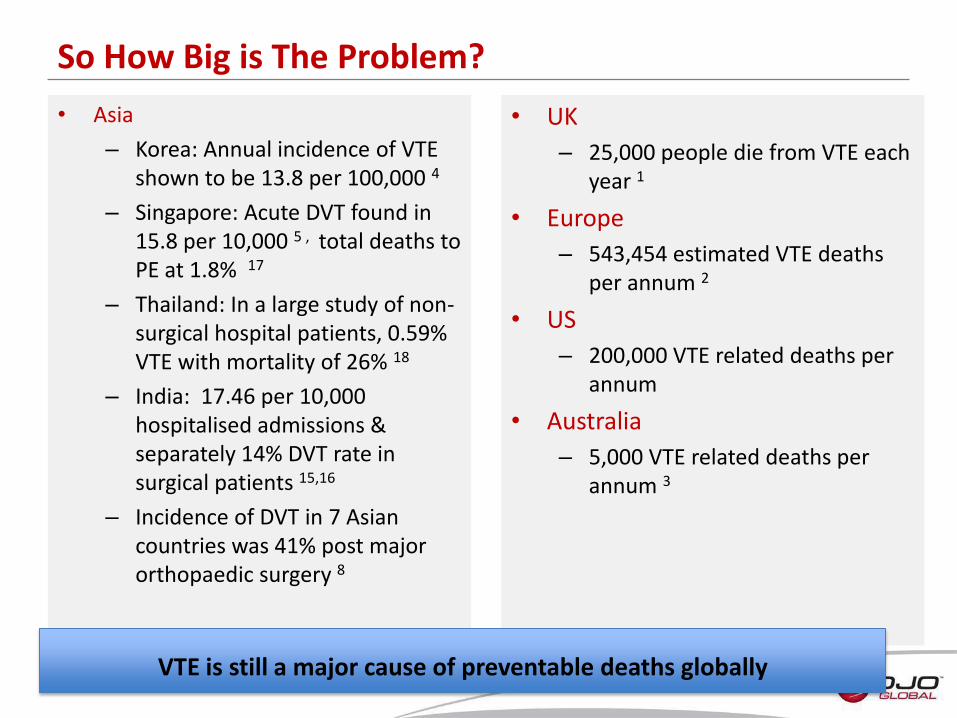
So How Big is The Problem?
• UK
– 25,000 people die from VTE each year 1
• Europe
– 543,454 estimated VTE deaths per annum 2
• US
– 200,000 VTE related deaths per annum
• Australia
– 5,000 VTE related deaths per annum 3
• Asia
– Korea: Annual incidence of VTE shown to be 13.8 per 100,000 4
– Singapore: Acute DVT found in 15.8 per 10,000 5 , total deaths to PE at 1.8% 17
– Thailand: In a large study of non-surgical hospital patients, 0.59% VTE with mortality of 26% 18
– India: 17.46 per 10,000 hospitalised admissions & separately 14% DVT rate in surgical patients 15,16
– Incidence of DVT in 7 Asian countries was 41% post major orthopaedic surgery 8
VTE is still a major cause of preventable deaths globally
• PROVE registry compared VTE events in Europe/Australia with those in Asia 9: – Asian patients younger – More proximal DVTs – Fewer patients received prophylaxis
• Piovella and his review work from 2005 showed 7: – Using Venography, incidence of DVT following orthopaedic surgery was
higher than in Western populations – Lack of awareness in Asian countries – slow to adopt new techniques
• Multinational study involving 32 countries proved that high percentage of hospitalised patients were at risk of VTE but too few received appropriate prophylaxis22: – Surgical patients: 64.4% at risk – only 58.5% received correct
prophylaxis – Medical patients: 41.5% at risk – only 39.5% received correct
prophylaxis
Under-diagnosed - Under-prophylaxed!
Low rate of thromboprophylaxis in Asian population despite their high risk of VTE.
• Hospital versus Community acquired – 10% of patients will develop VTE in hospital, with 0.5% developing immediately
post-discharge! – 74% of VTE present in outpatients 10
• 42% of VTE outpatients have had hospital admissions • Only 40% received prophylaxis in hospital
– 2/3 of VTE deaths occur post-discharge • Lack of clinical studies in certain areas
– Highest risk groups: Obs & Gyn, Medical, Oncology • National differences not recognised
– Health systems – Income growth & distribution
• Varying levels of VTE awareness • Underestimate risk
– No risk assessment at admission or prior to surgery – 72.9% patients demonstrate 1 or more risk factors for DVT 17
– Patients readmitted into other departments – lost in system • Lack of acceptance of guidelines
Why is there still VTE?
Risk assessment is critical for all patients not just to assess risk of VTE but to identify other possible co-morbidities.
• Personal Health Cost
– 30% greater cumulative risk of recurrent VTE after 1st case
– Sequelae of post-thrombotic syndrome, PE, PAH
– Loss of work, social mobility, lack of confidence
• Financial Burden
– Cost of treating VTE • Hospitalisation
• Drugs
• Care givers
• Long term sequelae
• National pressures for effective VTE management
– Public reporting
– Accountability
– #1 potentially preventable death in hospitalised patients
– VTE management rated #1 most effective safety policy in US hospitals
– Health systems may stop paying for hospital induced VTE
Why VTE Prophylaxis?
Prophylaxis works: Reduced risk of VTE from
1.8 to 1.1! 19
General Risk Factors for DVT
• Age > 60 years
• Obesity (BMI >30kg/m2)
• Oestrogen-containing contraceptive therapy
• Pregnancy
• Use of HRT (Hormone Replacement Therapy)
• Critical care admission
• Travel for extended periods of time (plane, train, truck, car)
• Personal history or first degree relative with history of VTE
• Active cancer or cancer treatment
• Severe asthma
• One or more significant medical comorbidities (eg. Heart disease, metabolic, endocrine or respiratory pathologies, acute infectious diseases, inflammatory conditions)
• Varicose veins with phlebitis
• Known thrombophilias
• DVT is often asymptomatic, however if symptoms do exist: – Calf pain or tenderness, or both – Swelling with pitting oedema – Swelling below knee in distal DVT and up to groin in proximal DVT – Increased skin temperature – Superficial venous dilatation – Cyanosis can occur with severe obstruction – Coughing and/or chest pain
• The Silent Killer
– The clinical signs can be unreliable especially in early thrombosis. In up to 50% of cases, there are few or no significant signs and symptoms. (Turner & Turner 1982)
– Only 25% of patients with DVT display clinical signs (O’Meara 1990)
Clinical signs and symptoms of VTE
• What caused it?
– 2 recent surgeries on her foot in March 2011
– Later complained of pain in her leg
– DVT & PE!
• Why was it missed?
– Slower heart rate – increased risk of stasis
– Misdiagnosis
So who is at risk?
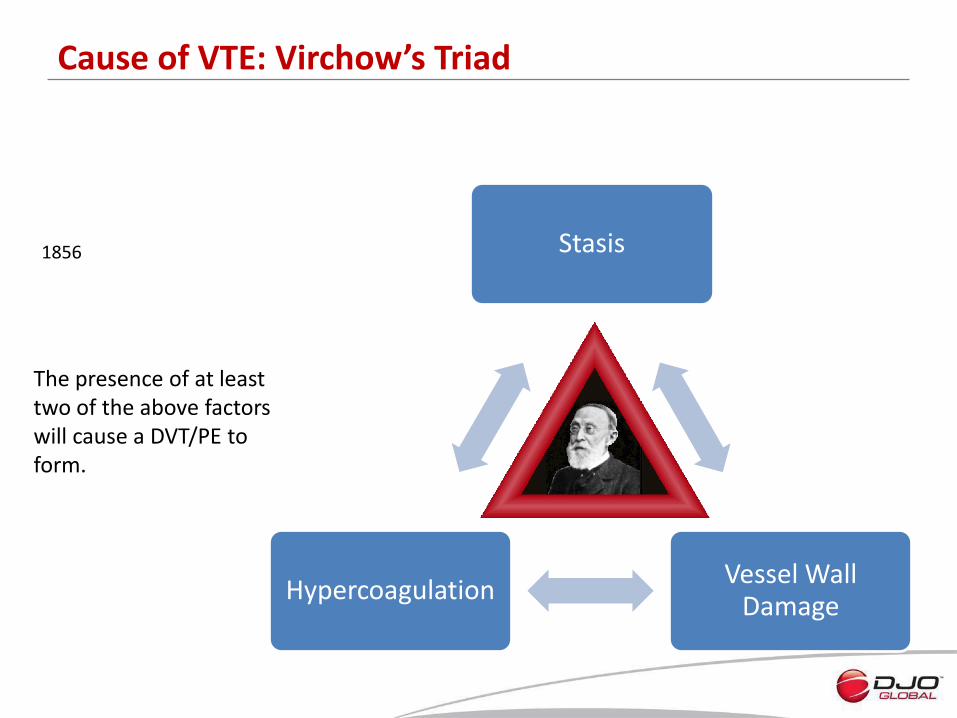
Stasis
Vessel Wall Damage
Hypercoagulation
Cause of VTE: Virchow’s Triad
1856
The presence of at least two of the above factors will cause a DVT/PE to form.
Methods of Preventing DVT
A. Prevention of Stasis and Endothelial Damage (Mechanical)
Leg elevation and early ambulation
Graduated elastic compression
Intermittent pneumatic compression
Plantar foot compression B. Prevention of Hypercoaguable State (Pharmaceutical) Oral anticoagulants Low dose Subcutaneous Heparin Low Molecular Weight Heparin (LMWH) Pentasaccharides- Fondaparinux Oral LMWH C. Combination of Methods from A and B
Pharmaceutical Prophylaxis
• Use of drugs to prevent VTE by affecting the ability of the blood to clot
– Vitamin K antagonists (warfarin/coumadin) long term, now mostly used for treatment (oral use) • Block synthesis of vitamin K-dependent coagulation factors
– Heparins
• Unfractionated heparin (UFH) injections short term
– Low molecular weight heparins (LMWH), such as Clexane/Lovenox (enoxaparin & dalteparin) indicated for VTE prophylaxis in medical & surgical patients. Injection only.
– Fondaparinux – synthetic sugar (pentassacharide) that binds to Factor Xa.
– New synthetic oral anticoagulants:
• Pradaxa (dabigatran) launched March 2009 – direct thrombin inhibitor, IIa
• Xarelto (rivaroxaban) and Eliquis (apixaban) – Factor Xa
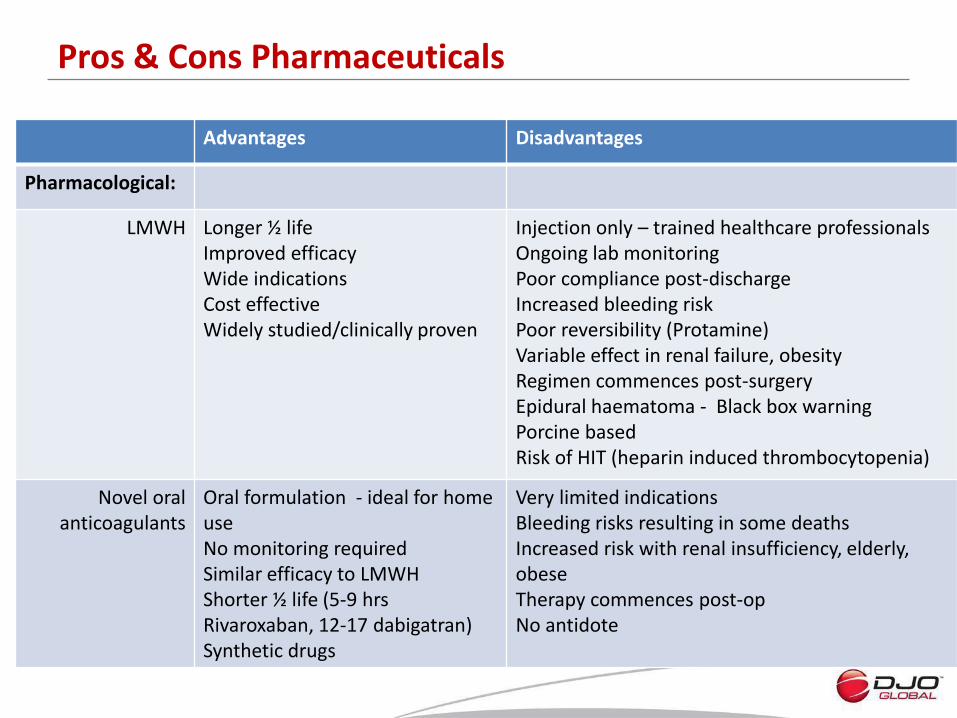
Advantages Disadvantages
Pharmacological:
LMWH Longer ½ life Improved efficacy Wide indications Cost effective Widely studied/clinically proven
Injection only – trained healthcare professionals Ongoing lab monitoring Poor compliance post-discharge Increased bleeding risk Poor reversibility (Protamine) Variable effect in renal failure, obesity Regimen commences post-surgery Epidural haematoma - Black box warning Porcine based Risk of HIT (heparin induced thrombocytopenia)
Novel oral anticoagulants
Oral formulation - ideal for home use No monitoring required Similar efficacy to LMWH Shorter ½ life (5-9 hrs Rivaroxaban, 12-17 dabigatran) Synthetic drugs
Very limited indications Bleeding risks resulting in some deaths Increased risk with renal insufficiency, elderly, obese Therapy commences post-op No antidote
Pros & Cons Pharmaceuticals
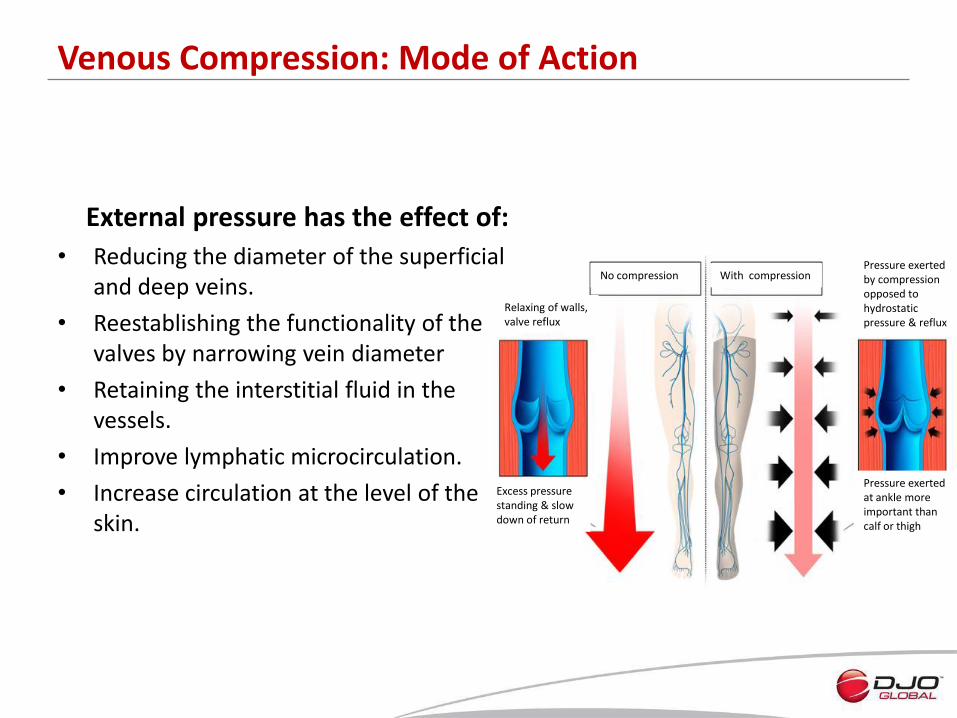
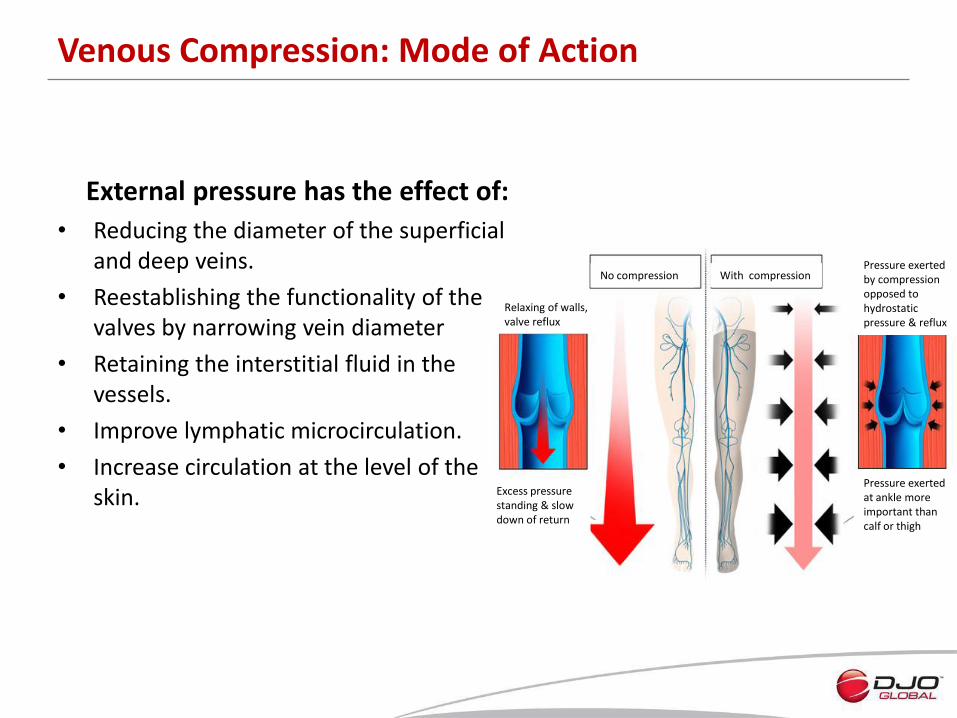
External pressure has the effect of:
• Reducing the diameter of the superficial and deep veins.
• Reestablishing the functionality of the valves by narrowing vein diameter
• Retaining the interstitial fluid in the vessels.
• Improve lymphatic microcirculation.
• Increase circulation at the level of the skin.
Venous Compression: Mode of Action
No compression With compression
Relaxing of walls, valve reflux
Excess pressure standing & slow down of return
Pressure exerted by compression opposed to hydrostatic pressure & reflux
Pressure exerted at ankle more important than calf or thigh
• Recumbent/immobile
– Patients laying in bed require low levels of pressure (>10mmHg) to control venous stasis
– This is sufficient to prevent thrombus formation
– Pressures in excess of 30 mmHg do not have beneficial effect if patient is laying down
• Ambulatory/standing
– Far higher levels of pressure required to influence blood flow
– Pressure during walking fluctuates between 20-100mmHg
– Working pressures of 40-50mmHg are required to influence this
Why different levels of compression?
• Recumbent/immobile
– Patients laying in bed require low levels of pressure (>10mmHg) to control venous stasis
– This is sufficient to prevent thrombus formation
– Pressures in excess of 30 mmHg do not have beneficial effect if patient is laying down
• Ambulatory/standing
– Far higher levels of pressure required to influence blood flow
– Pressure during walking fluctuates between 20-100mmHg
– Working pressures of 40-50mmHg are required to influence this
Why different levels of compression?
Where Do We Fit In?
Stasis
Vessel Wall Damage
Coagulation Changes
Intermittent Pneumatic Compression
Graduated Compression Stockings
Intermittent Pneumatic Compression
Pharmacological modalities
Graduated Compression Stockings
VenaFlow VenaPure
VenaFlow VenaPure
Mechanism of Action: VenaPure & VenaFlow
• VenaPure
- Reduce venous dilation preventing endothelial damage
- Graduated compression profile increases blood flow velocity (138.4%) Sigel 1975
• VenaFlow
- Increases venous velocity by 112% above baseline, empties veins bringing vein walls into opposition
• Tissue Factor Pathway Inhibitors & Tissue Plasminogen Activators – released by body in response to vessel damage
• Only device to truly replicate normal ambulation and the mechanism of action of the calf muscle pump
– Demonstrated by the Doppler comparisons
• Very easy to set up device
• Compliance meter is standard
– Essential to ensure that the correct therapy is being administered
• Integrated Sequential Flow System ensures that the minimal amount of tubing is used to administer maximum benefit
– Reduces the risk of pressure points on leg
• Clinically proven with recent studies to reduce DVTs
– Eisele 2007, Westrich 2006, Silbersack 2004
• Clinically proven to be more effective than competitors in reducing DVT
– Lachiewicz 2004
• One device for all situations
– Delivers the same clinically proven compression profile
VenaFlow Elite
• Design and manufacture has been based on the market leader (TED)
• Uses the same clinically proven compression profile that has demonstrated a reduction in the rate of DVTs
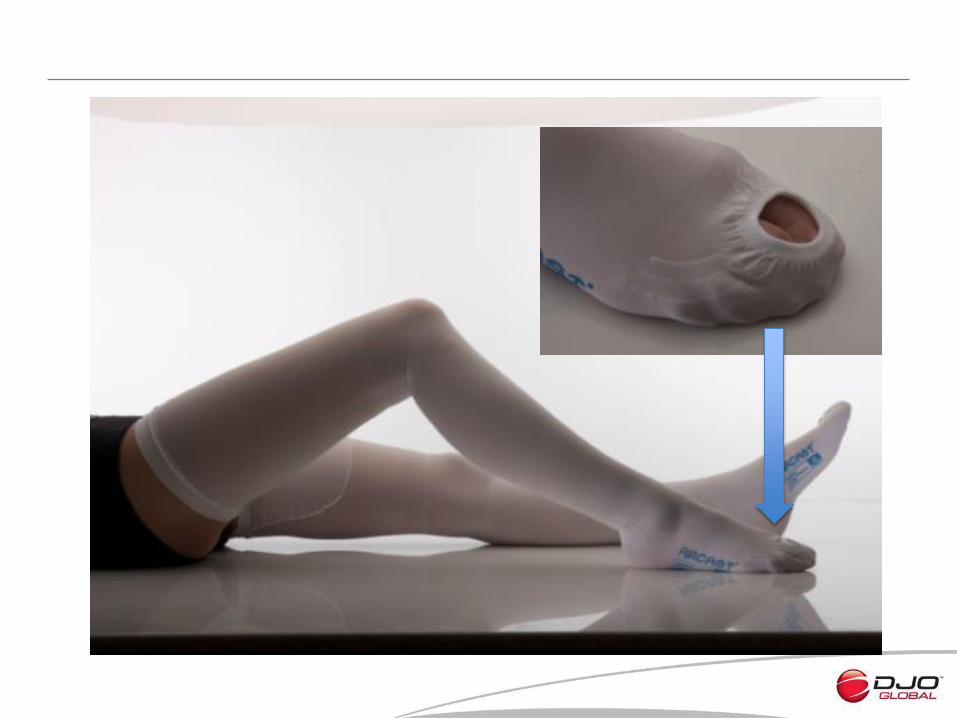
• Inspection toe on top of the stocking facilitates nurse observations
– Less risk of the patient picking up dirt etc from the ward floor
• Range of sizes available ensure the majority of the population are covered
• All the dispenser boxes contain tape measures – enough for every patient
– No need to reuse tape measure and risk cross infection
VenaPure

VenaFlow Elite
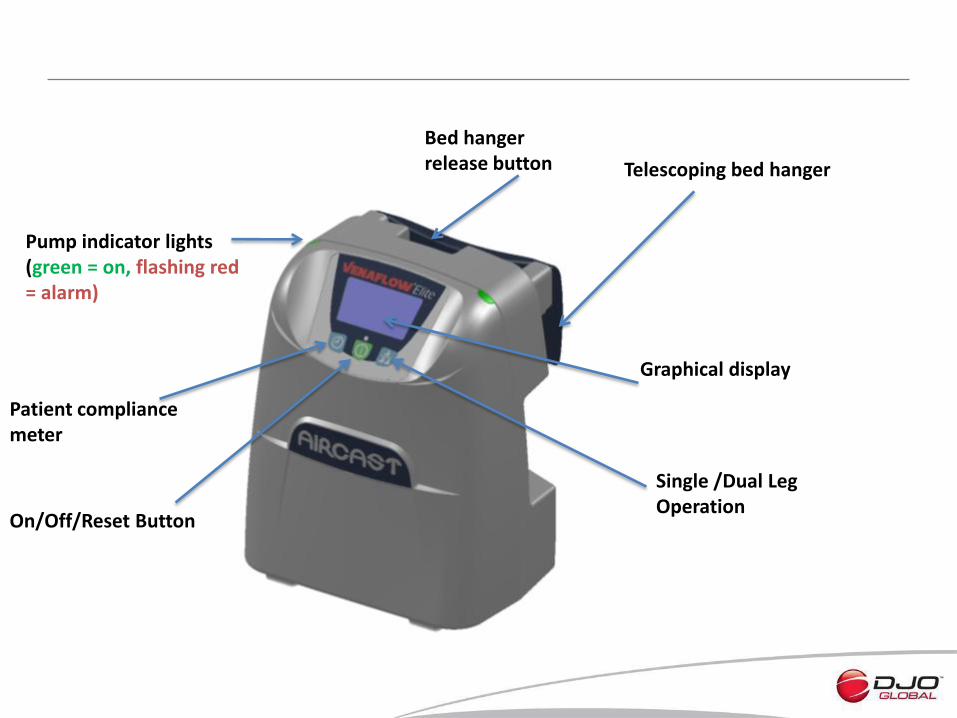
Bed hanger release button
Pump indicator lights (green = on, flashing red = alarm)
Telescoping bed hanger
Graphical display
Single /Dual Leg Operation
On/Off/Reset Button
Patient compliance meter
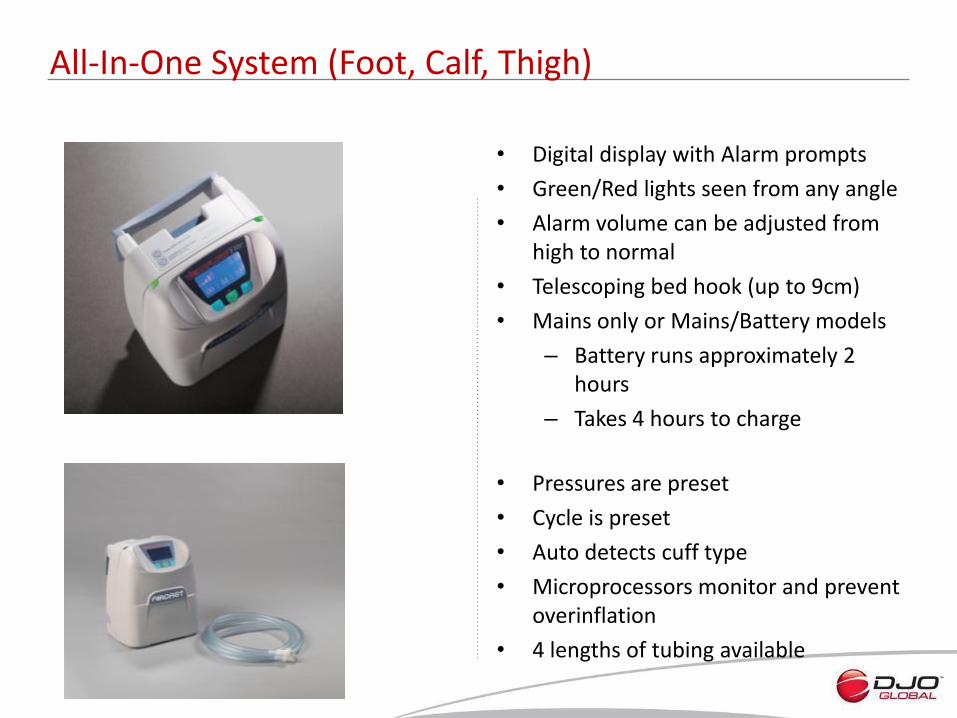
• Digital display with Alarm prompts
• Green/Red lights seen from any angle
• Alarm volume can be adjusted from high to normal
• Telescoping bed hook (up to 9cm)
• Mains only or Mains/Battery models
– Battery runs approximately 2 hours
– Takes 4 hours to charge
• Pressures are preset
• Cycle is preset
• Auto detects cuff type
• Microprocessors monitor and prevent overinflation
• 4 lengths of tubing available
All-In-One System (Foot, Calf, Thigh)
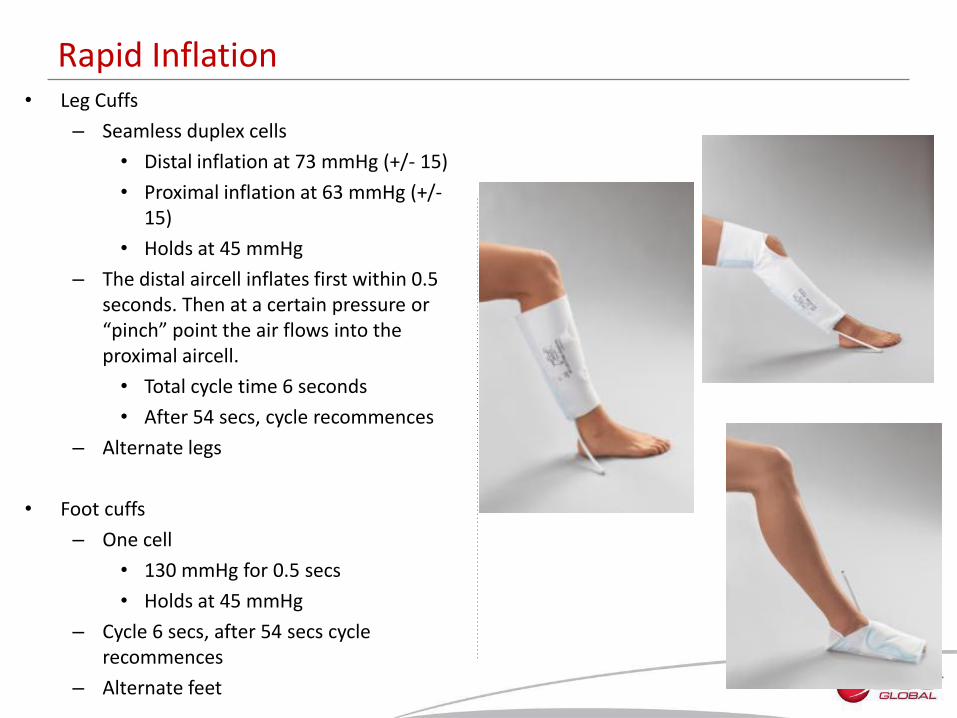
• Leg Cuffs
– Seamless duplex cells
• Distal inflation at 73 mmHg (+/- 15)
• Proximal inflation at 63 mmHg (+/- 15)
• Holds at 45 mmHg
– The distal aircell inflates first within 0.5 seconds. Then at a certain pressure or “pinch” point the air flows into the proximal aircell.
• Total cycle time 6 seconds
• After 54 secs, cycle recommences
– Alternate legs
• Foot cuffs
– One cell
• 130 mmHg for 0.5 secs
• Holds at 45 mmHg
– Cycle 6 secs, after 54 secs cycle recommences
– Alternate feet
Rapid Inflation
• Cool, lightweight, breathable sleeves
– Durable fabric
– Brushed nylon & polyester
• 3 sizes of calf cuff and 1 size for thigh
– Minimal inventory required
– Can be trimmed to size
• Bariatric calf cuff available (up to 76cm)
– Bariatric doppler results unchanged
• Cuffs are Single Patient Use
• Aircells can be placed anterior, posterior, medial, lateral on leg
– Does not affect performance
• Safe connectors, durable tubing, anti-kinking
• Can be applied with or without anti-embolism stockings
– Medical decision
Cuffs and Tubing
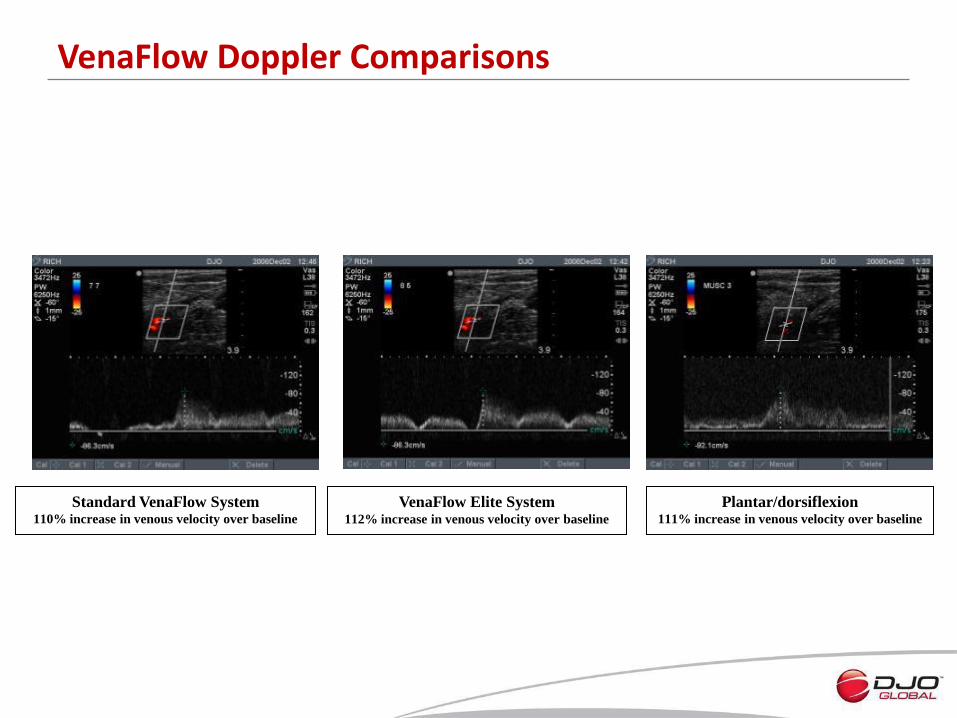
VenaFlow Doppler Comparisons
Standard VenaFlow System 110% increase in venous velocity over baseline
VenaFlow Elite System 112% increase in venous velocity over baseline
Plantar/dorsiflexion 111% increase in venous velocity over baseline
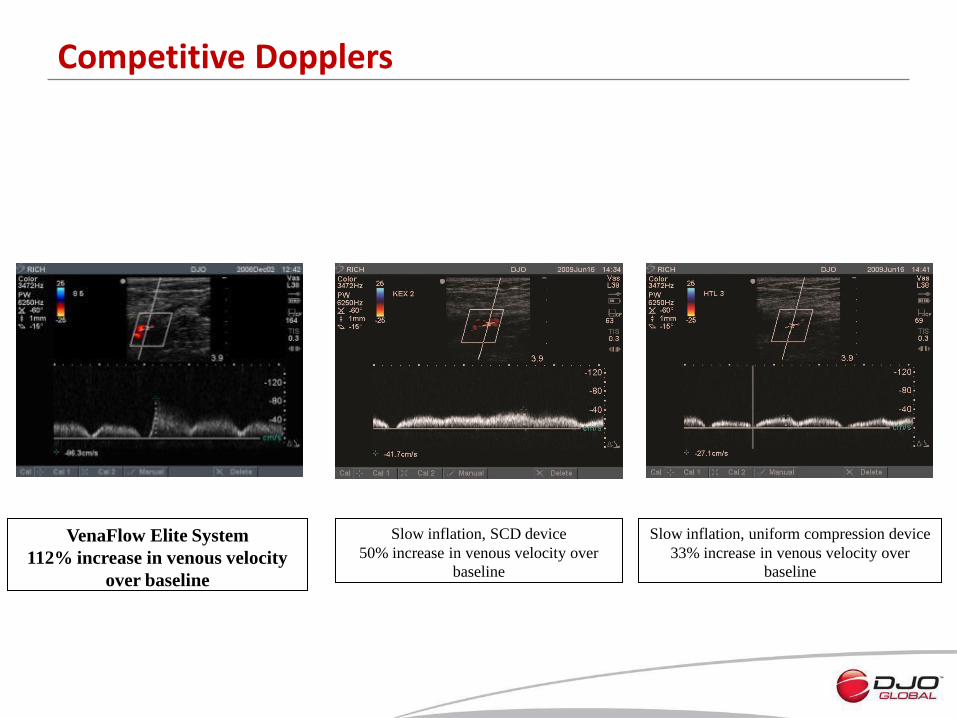
Competitive Dopplers
Slow inflation, SCD device
50% increase in venous velocity over
baseline
Slow inflation, uniform compression device
33% increase in venous velocity over
baseline
VenaFlow Elite System
112% increase in venous velocity
over baseline
• Sleeves or Foot cuffs should be worn throughout the immobilsation period, pre-op, intra-op and post-op
• Cuffs should be kept on for 24 hours and for as many days as prescribed until the patient is fully mobile
• At sleep – device should not be disconnected – risk of DVT forming if no prophylaxis used
• Remove daily and inspect skin for signs of pressure damage
• Become familiar with the fault alarms both visual and audible with corresponding coding.
In Service Recommendations
VenaPure Anti-Embolism Stockings
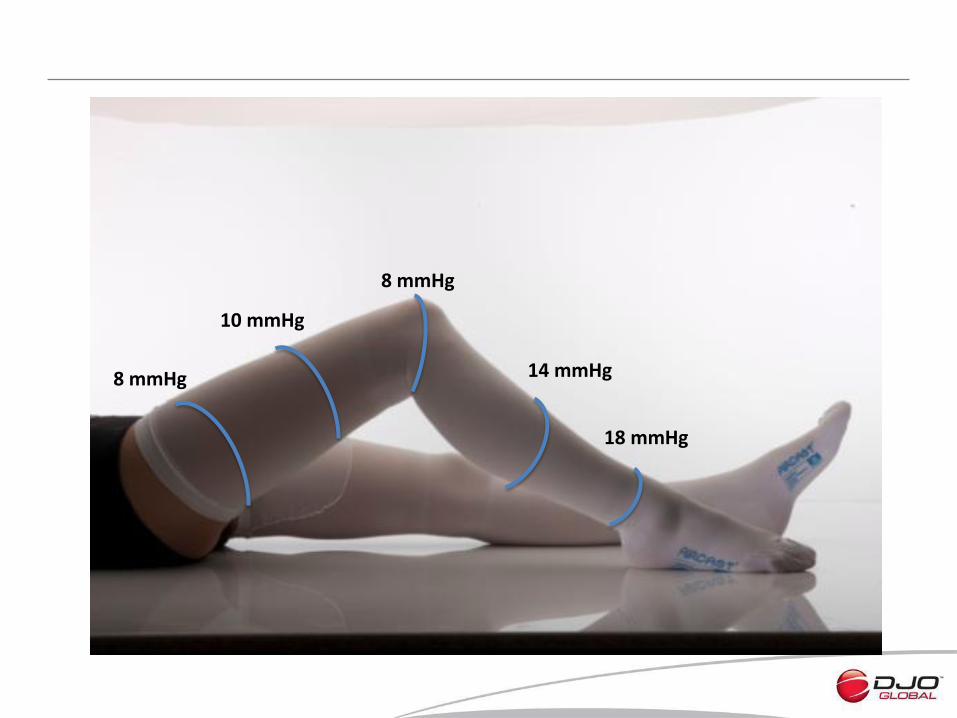
8 mmHg
10 mmHg
8 mmHg
14 mmHg
18 mmHg


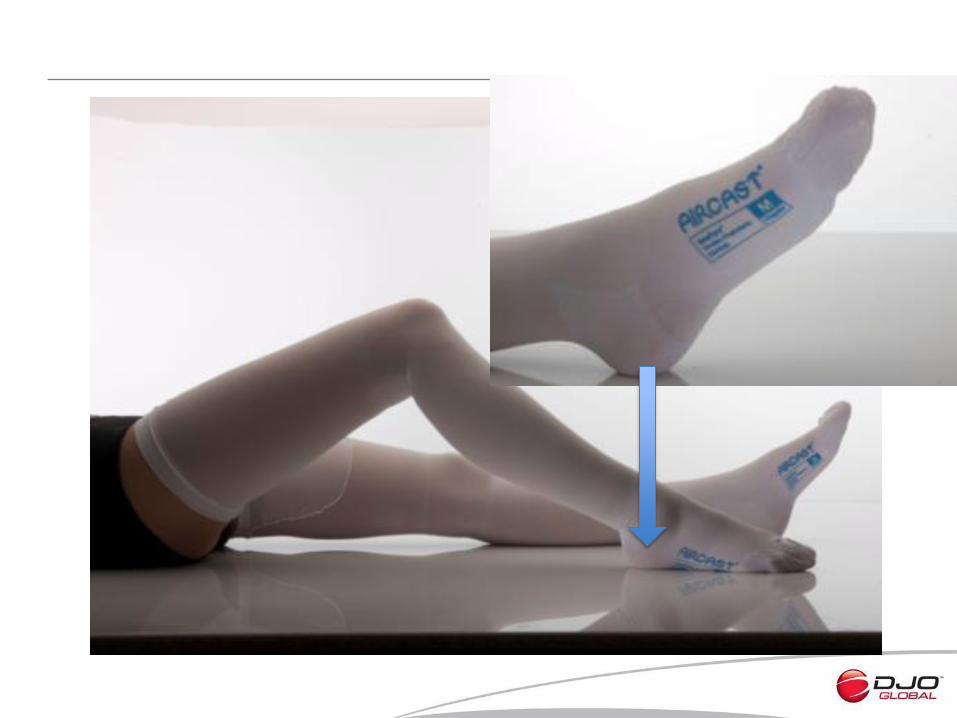
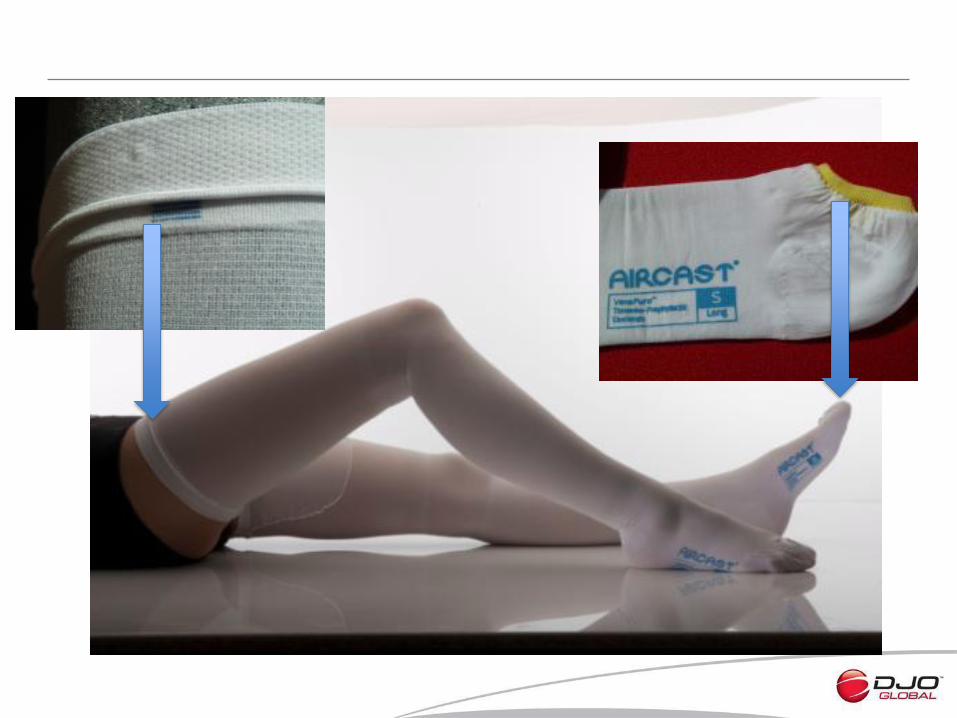
In-Service Recommendations
• Stockings should be worn throughout immobilisation period, pre-operatively, intra-operatively, and post-operatively.
• Stockings should be kept on for 24 hours and should not be left off for more than 30 minutes when bathing etc.
• Ensure the proper fit. Re-measure if decrease/increase in œdema and reapply correct size
• It is recommended that stockings continue to be worn for at least 6 weeks post surgery
Review
• DVT is real and lethal!!
• Hospital based disease.
• Preventable cause of death.
• Massively under diagnosed.
• Under treated.
• Multimodal treatments efficient.
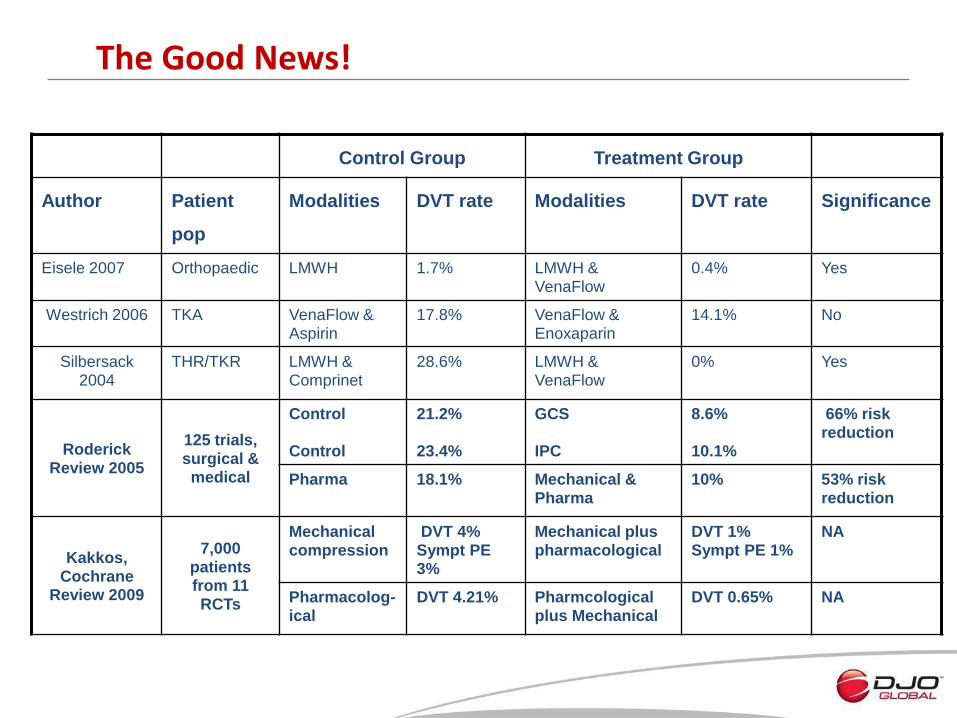
The Good News!
Control Group Treatment Group
Author Patient
pop
Modalities DVT rate Modalities DVT rate Significance
Eisele 2007 Orthopaedic LMWH 1.7% LMWH & VenaFlow
0.4% Yes
Westrich 2006 TKA VenaFlow & Aspirin
17.8% VenaFlow & Enoxaparin
14.1% No
Silbersack 2004
THR/TKR LMWH & Comprinet
28.6% LMWH & VenaFlow
0% Yes
Roderick Review 2005
125 trials, surgical & medical
Control Control
21.2% 23.4%
GCS IPC
8.6% 10.1%
66% risk reduction
Pharma 18.1% Mechanical & Pharma
10% 53% risk reduction
Kakkos, Cochrane
Review 2009
7,000 patients from 11 RCTs
Mechanical compression
DVT 4% Sympt PE 3%
Mechanical plus pharmacological
DVT 1% Sympt PE 1%
NA
Pharmacolog-ical
DVT 4.21%
Pharmcological plus Mechanical
DVT 0.65% NA
• High risk patients: – Bleeding – Wound hematoma – Renal insufficiency – HIT
• Type of surgery – High risk orthopaedic procedures – CABG – Spinal – Neurosurgery
• Type of anaesthesia – Neuraxial, spinal or epidural risk of haematoma
• Virchow Triad – All 3 factors covered
When Mechanical is Enough!
• In a Japanese study looking at hip surgery 11
– Mechanical prophylaxis only – Incidence of VTE:
• Fatal PE 0% • Symptomatic PE 0.03% • Symptomatic DVT 0.1%
• Review of the use of pharmaprophylaxis in the OR and ICU 12
– Effective no more than 2/3 of the time – Only protects against hypercoagulation – Importance of IPC placement pre-anaesthesia, peri-op and post-op
location – Disconnection of IPC is not recommended until patient fully
ambulatory • Review of gynaecological procedures in benign surgery 13
– Use of IPC alone demonstrated VTE event of <1%
Where’s The Clinical Proof?
• In cervical spine patients, where there is an increased risk of wound haematoma when using pharmacologicals 20
– IPC was used alone
– Single level trial showed 1-2% VTE, multi-level trial 7% DVT & 2% PE
– Data is comparable to that achieved with drug regimen, but without the associated high bleeding risk
• Review of the use of mechanical prophylaxis generally 21
– Clinically proven to reduce incidence of VTE, also stimulates fibrinolysis and physiologic inhibitors of coagulation
– Important to initiate mechanical before, during and after surgery to limit venous stasis and endothelial damage from venous distention
• Meta-analysis in variety of clinical settings14
– IPC alone reduced DVT incidence 60%
1. NICE Clinical Guidance 92 January 2010
2. Cohen, Thromb & Haemost. 2007
3. National Health & Medical Research Council, Australia 2011
4. Jang Thromb Haemost. 2010
5. Lee Ann Acad Med Singapore 2002
6. Prasannan, AJS 2005
7. Piovella, J.Thromb Haemost. 2005
8. Angchaisuksiri, Thromb Haemost 2011
9. Tupie, J.Thromb Haemost 2005
10. Spencer, Arch Intern Med 2007
11. Sugano, J. Arthroplasty, 2009
12. Burns, AORN 2012
13. Rahn. Obs & Gyn 2011
14. Urbankova, J Throm Haemost 2004
15. Lee , Eur J Vas Endovas Surg 2009
16. Tauro , J Clin Diag Research 2010
17. Sule , Int J Angiol 2011
18. Aniwan , Blood Coag & Fibrinolysis 2010
19. Cheng, Thrombosis 2011
20. Epstein , Spine 2005
21. Caprini, Clin Appl Thromb Hemost 2010
22. Cohen AT, Lancet 2008
Clinical References
It’s Not Just About Orthopaedics!
44
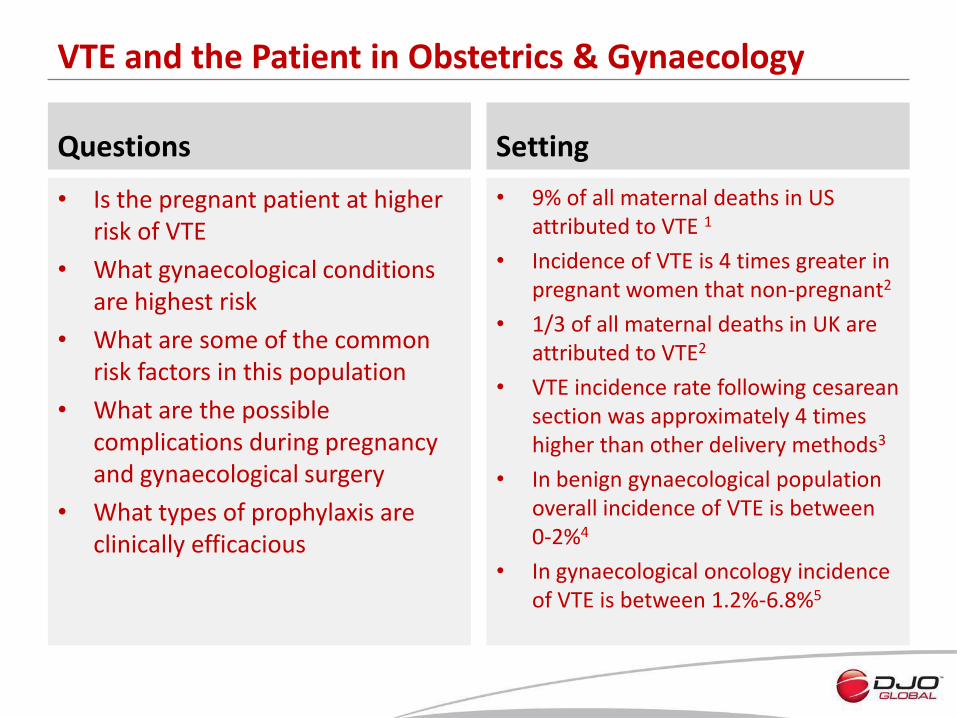
VTE and the Patient in Obstetrics & Gynaecology
Questions
• Is the pregnant patient at higher risk of VTE
• What gynaecological conditions are highest risk
• What are some of the common risk factors in this population
• What are the possible complications during pregnancy and gynaecological surgery
• What types of prophylaxis are clinically efficacious
Setting
• 9% of all maternal deaths in US attributed to VTE 1
• Incidence of VTE is 4 times greater in pregnant women that non-pregnant2
• 1/3 of all maternal deaths in UK are attributed to VTE2
• VTE incidence rate following cesarean section was approximately 4 times higher than other delivery methods3
• In benign gynaecological population overall incidence of VTE is between 0-2%4
• In gynaecological oncology incidence of VTE is between 1.2%-6.8%5
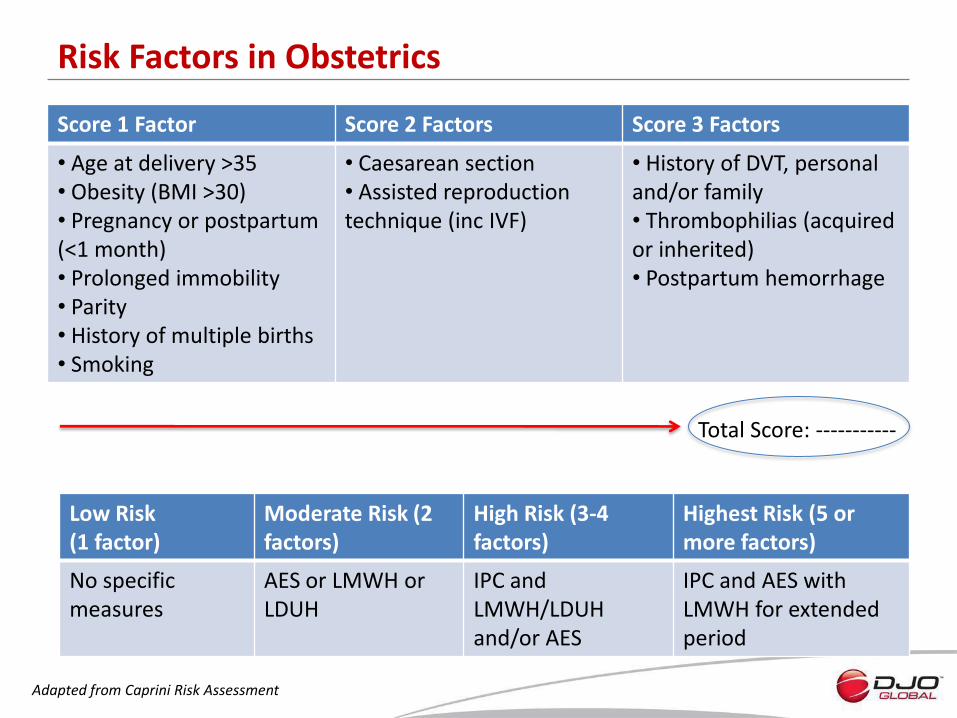
Risk Factors in Obstetrics
Score 1 Factor Score 2 Factors Score 3 Factors
• Age at delivery >35 • Obesity (BMI >30) • Pregnancy or postpartum (<1 month) • Prolonged immobility • Parity • History of multiple births • Smoking
• Caesarean section • Assisted reproduction technique (inc IVF)
• History of DVT, personal and/or family • Thrombophilias (acquired or inherited) • Postpartum hemorrhage
Total Score: -----------
Low Risk (1 factor)
Moderate Risk (2 factors)
High Risk (3-4 factors)
Highest Risk (5 or more factors)
No specific measures
AES or LMWH or LDUH
IPC and LMWH/LDUH and/or AES
IPC and AES with LMWH for extended period
Adapted from Caprini Risk Assessment
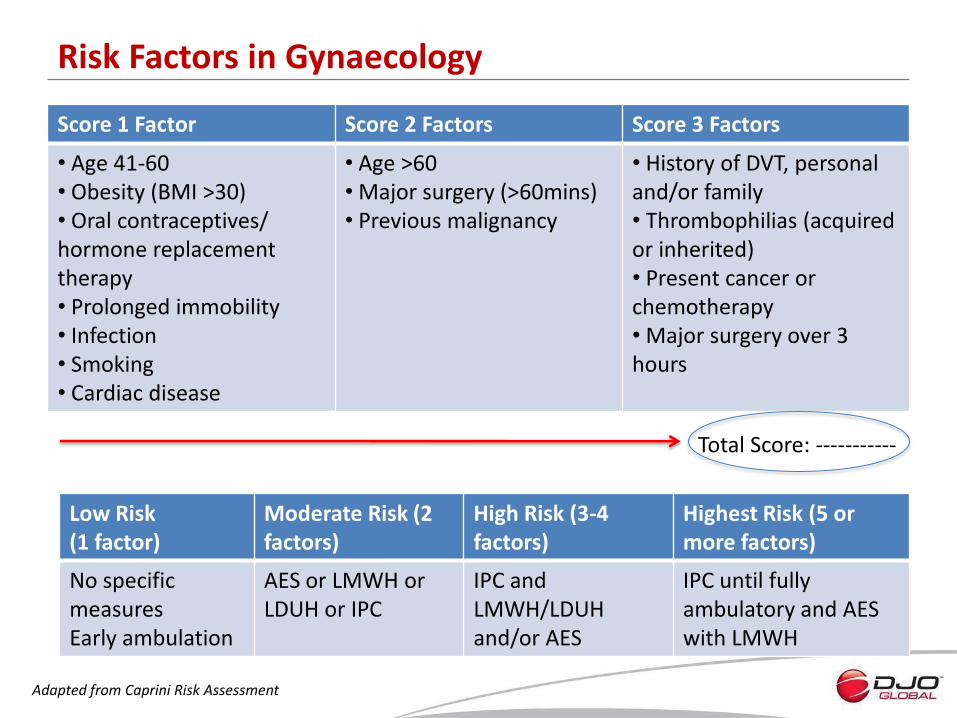
Risk Factors in Gynaecology
Score 1 Factor Score 2 Factors Score 3 Factors
• Age 41-60 • Obesity (BMI >30) • Oral contraceptives/ hormone replacement therapy • Prolonged immobility • Infection • Smoking • Cardiac disease
• Age >60 • Major surgery (>60mins) • Previous malignancy
• History of DVT, personal and/or family • Thrombophilias (acquired or inherited) • Present cancer or chemotherapy • Major surgery over 3 hours
Total Score: -----------
Low Risk (1 factor)
Moderate Risk (2 factors)
High Risk (3-4 factors)
Highest Risk (5 or more factors)
No specific measures Early ambulation
AES or LMWH or LDUH or IPC
IPC and LMWH/LDUH and/or AES
IPC until fully ambulatory and AES with LMWH
Adapted from Caprini Risk Assessment
Complications/Concerns
• Use of heparin preferred during pregnancy BUT1:
– 40-50% increase in maternal blood volume
– ↑ in renal excretion of heparin
– ↑ in protein binding of heparin
– Shorter ½ life and lower peak plasma concentrations mean higher dose and more frequent administration
• According to Asian guidelines, use of new oral anticoagulants is not recommended during pregnancy, puerperium & during breast feeding
• Risk of epidural or spinal haematoma with regional anaesthesia1
• Bleeding risk
• Higher incidence of illiac vein DVT in pregnancy, but harder to diagnose2
• Approximately 70% of patients with fatal PE are only diagnosed at autopsy6
The Solution
Obstetrics
• Risk assessment in early pregnancy essential and then repeat if admitted to hospital
• ACOG guidelines recommend the use of IPC pre-Caesarean delivery, especially due to the bleeding risk with thromboprophylaxis1
• AES recommended ante- and post-partum for all women who have had prior VTE2
Gynaecology
• IPC & AES post gynaecologic pelvic surgery vs AES alone reduced DVT rates to 4.8% versus 12.5%7
• Use of IPC for benign procedures reduced incidence of VTE and decreased the potential morbidities associated with heparin prophylaxis4
• In gynaecological cancer surgery, VTE decreased from 6.5% with IPC alone to 1.9% in combination with unfractionated heparin5
• Moderate risk patients should recieve anticoagulant or IPC8
• High risk patients should receive combined prophylaxis with pharma and mechanical 8
References
1. ACOG, Thromboembolism in Pregnancy, Sept 2011
2. Marik, New England J of Medicine, 2008:359
3. Simpson, Brit J of Obstetrics & Gynaecology Jan 2001 Vol 108
4. Rahn, Obstetrics & Gynecology Nov 2011 Vol 118 No 5
5. Einstein, Obstetrics & Gynecology Nov 2008 Vol 112 No 5
6. Maxwell, Obstetrics & Gynecology Dec 2001 Vol 98 No 6
7. Gao, Chin Med J(Eng) 2012 Dec 125(23)
8. Asian venous thromboembolism guidelines, Int Angio 2012 (31)
VTE and the Patient in Neurosurgery
Questions
• With the shortage of epidemiological data on VTE incidence in this patient population, what are the risks
• What risks do pharmacological agents pose in neurosurgery
• What are some of the common risk factors in this population
• What are the possible complications
• What types of prophylaxis are clinically efficacious
Setting
• 40% DVT rates within first 3 weeks post stroke, identified by MRI1
• 15.5% of patients have DVT following spinal surgery, if no prophylaxis administered2
• Calf DVT may be as high as 40-80% in patients following major trauma and spinal cord injury2
• Increased use of pharmacologial prophylaxis increases risk of haematoma and cauda equina syndrome2
• Use of low dose heparin in cranial & spinal procedures risks minor & major postop haemorrhage3
• Incidence of VTE in patients undergoing neurosurgery could be as high as 25%4
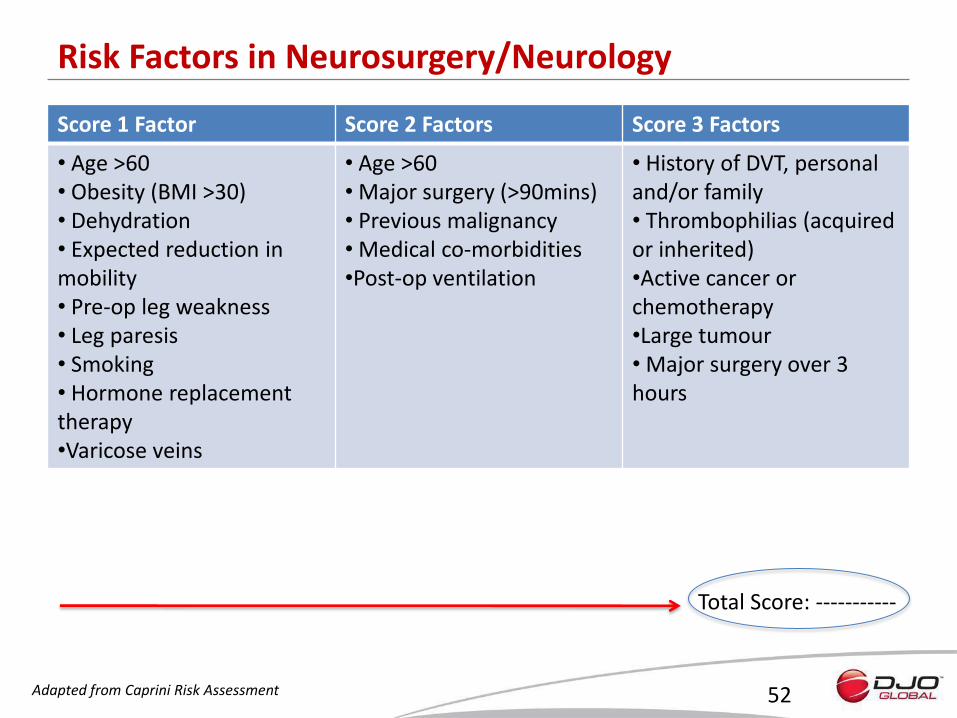
Risk Factors in Neurosurgery/Neurology
Score 1 Factor Score 2 Factors Score 3 Factors
• Age >60 • Obesity (BMI >30) • Dehydration • Expected reduction in mobility • Pre-op leg weakness • Leg paresis • Smoking • Hormone replacement therapy •Varicose veins
• Age >60 • Major surgery (>90mins) • Previous malignancy • Medical co-morbidities •Post-op ventilation
• History of DVT, personal and/or family • Thrombophilias (acquired or inherited) •Active cancer or chemotherapy •Large tumour • Major surgery over 3 hours
52
Total Score: -----------
Adapted from Caprini Risk Assessment
53
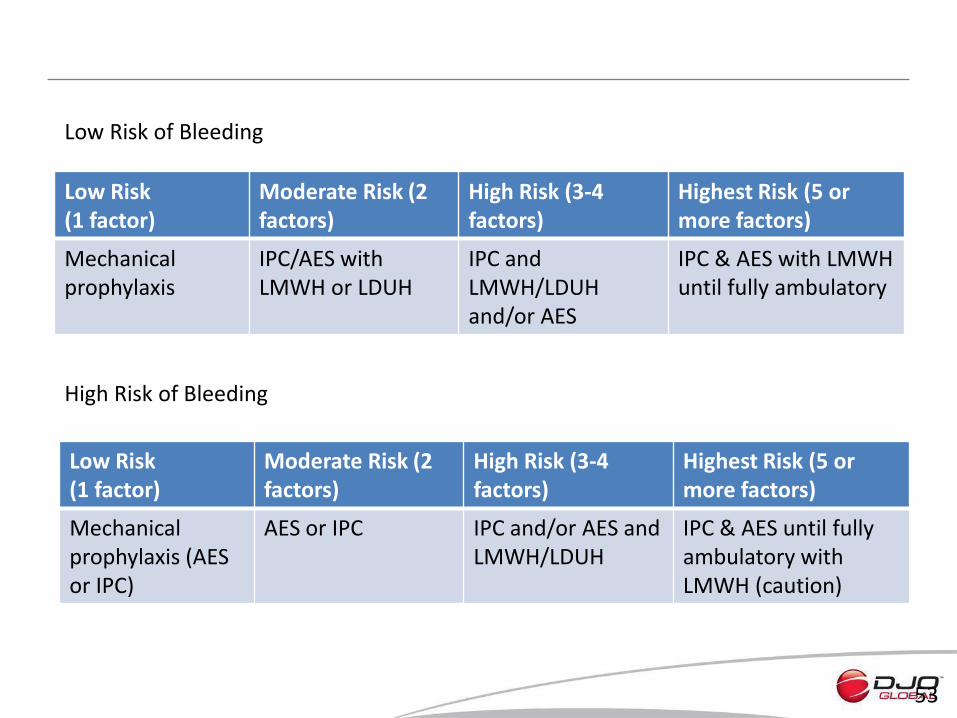
Low Risk (1 factor)
Moderate Risk (2 factors)
High Risk (3-4 factors)
Highest Risk (5 or more factors)
Mechanical prophylaxis
IPC/AES with LMWH or LDUH
IPC and LMWH/LDUH and/or AES
IPC & AES with LMWH until fully ambulatory
Low Risk (1 factor)
Moderate Risk (2 factors)
High Risk (3-4 factors)
Highest Risk (5 or more factors)
Mechanical prophylaxis (AES or IPC)
AES or IPC IPC and/or AES and LMWH/LDUH
IPC & AES until fully ambulatory with LMWH (caution)
Low Risk of Bleeding
High Risk of Bleeding
Complications/Concerns
• Use of anticoagulants in the peri-operative period limited due to fear of intracranial bleeding
• Patients are at risk of VTE throughout the surgery, therefore the initiation of prophylaxis is critical
• In CLOTS 1 trial on post-stroke patients, the use of AES alone showed no clinical benefit in reducing the risk of VTE5
• Stroke patients present with a variety of co-morbidities, a number of factors can be associated with VTE
• Benefits of using pharmacological prophylaxis needs to be considered relative to the risks of bleeding
The Solution
• In patients with intracerebral haemorrhage, the use of AES plus IPC to reduce VTE was significantly reduced versus AES alone: 4.7% vs 15.9%6
• Haemorrhagic stroke patients admitted to hospital were monitored for DVT7:
– 9.2% DVT and 2.4% PE on heparin alone
– 0.23% DVT and 0 PE on combination IPC & heparin
• Mechanical prophylaxis provided effective prophylaxis against VTE, the added efficacy of pharmacologicals needs to be weighed against risk of bleeding3
• Mechanical prophylaxis is integral part of neurological practice, used pre-, peri- and post-operatively8
• Recent CLOTS 3 study in post stroke patients showed reduction from 12.1% in no prophylaxis group to 8.5% with IPC9
Estimated that about 3,000 patients could avoid a DVT and 1,500 lives saved, just with the use of IPC in post stroke patients! 9
References
1. Naccarato, Cochrane Review 2010
2. Bryson, Journal of Ortho Surg & Research 2012, 7:14
3. Epstein, Surg Neurol 2005 Oct 64(4) 295-301
4. Browd, Neurosurg Focus 2004, 17(4) E1
5. CLOTS 1, Lancet 2009
6. Lacut, Neurology 2005 65:865-869
7. Kamran Neurology June 1998 Vol 50 No 6
8. Auguste, Neurosurg Focus 2004, 17(4) E3
9. CLOTS 3, Press Report from BBC News , 31st May 2013 (trial not yet published)
VenaFlow S Mode
• Internationally, concerns have been raised in some centres by:
– The noise of the pump, especially at night
– The startle effect of leg movement, especially during surgery
– Perceived pain of “rapid” inflation
• The objective is to add a function “S Mode” to the Elite to allow the user to select a slower compression mode, which will significantly reduce the “Startle Effect”
Project Rationale
• To build a new, separate pump with standard rapid inflation plus the additional S mode function
• S mode equates to slow compression of a lower pressure profile during a slightly longer cycle
• The design change is reflected primarily by:
– Software change
– Replacement of a current icon for S mode icon
Project Design
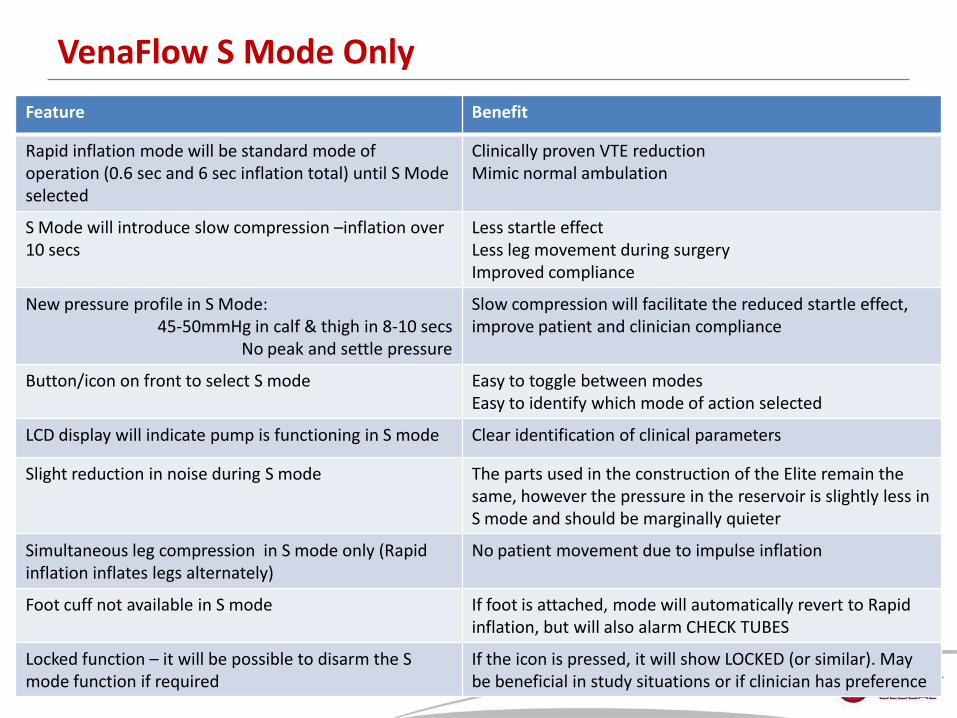
Feature Benefit
Rapid inflation mode will be standard mode of operation (0.6 sec and 6 sec inflation total) until S Mode selected
Clinically proven VTE reduction Mimic normal ambulation
S Mode will introduce slow compression –inflation over 10 secs
Less startle effect Less leg movement during surgery Improved compliance
New pressure profile in S Mode: 45-50mmHg in calf & thigh in 8-10 secs
No peak and settle pressure
Slow compression will facilitate the reduced startle effect, improve patient and clinician compliance
Button/icon on front to select S mode Easy to toggle between modes Easy to identify which mode of action selected
LCD display will indicate pump is functioning in S mode Clear identification of clinical parameters
Slight reduction in noise during S mode The parts used in the construction of the Elite remain the same, however the pressure in the reservoir is slightly less in S mode and should be marginally quieter
Simultaneous leg compression in S mode only (Rapid inflation inflates legs alternately)
No patient movement due to impulse inflation
Foot cuff not available in S mode If foot is attached, mode will automatically revert to Rapid inflation, but will also alarm CHECK TUBES
Locked function – it will be possible to disarm the S mode function if required
If the icon is pressed, it will show LOCKED (or similar). May be beneficial in study situations or if clinician has preference
VenaFlow S Mode Only
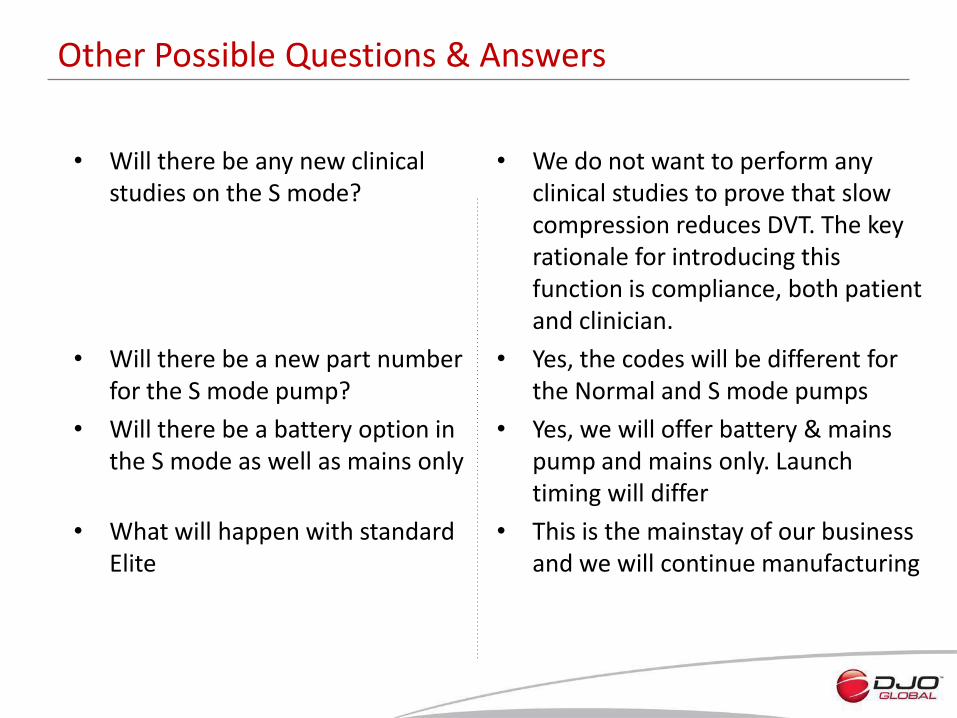
• Will there be any new clinical studies on the S mode?
• Will there be a new part number for the S mode pump?
• Will there be a battery option in the S mode as well as mains only
• What will happen with standard Elite
• We do not want to perform any clinical studies to prove that slow compression reduces DVT. The key rationale for introducing this function is compliance, both patient and clinician.
• Yes, the codes will be different for the Normal and S mode pumps
• Yes, we will offer battery & mains pump and mains only. Launch timing will differ
• This is the mainstay of our business and we will continue manufacturing
Other Possible Questions & Answers
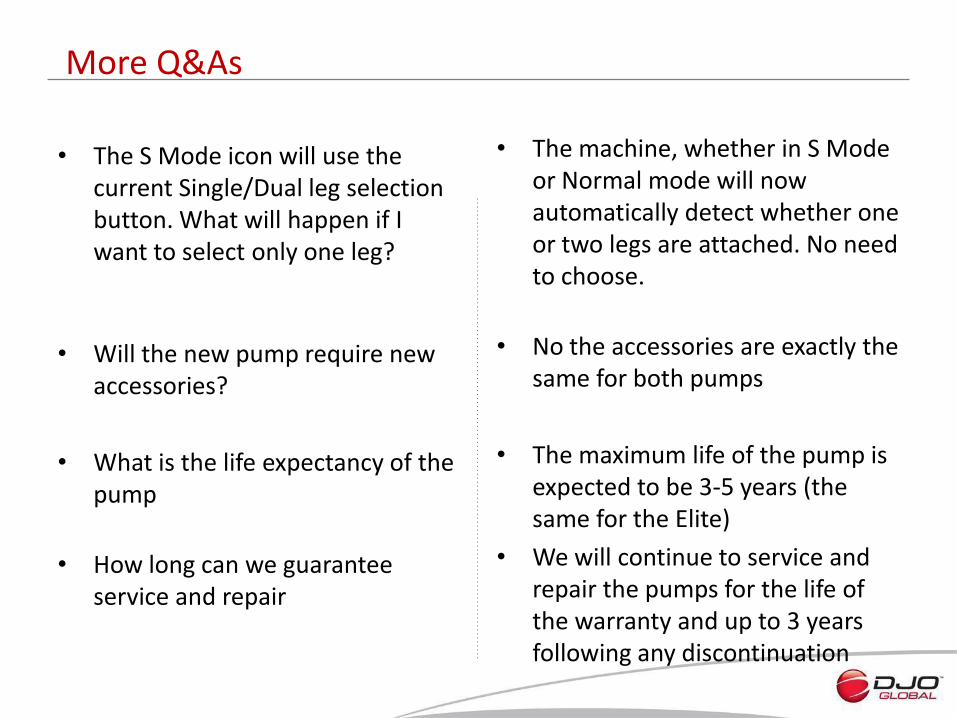
• The S Mode icon will use the current Single/Dual leg selection button. What will happen if I want to select only one leg?
• Will the new pump require new accessories?
• What is the life expectancy of the pump
• How long can we guarantee service and repair
• The machine, whether in S Mode or Normal mode will now automatically detect whether one or two legs are attached. No need to choose.
• No the accessories are exactly the same for both pumps
• The maximum life of the pump is expected to be 3-5 years (the same for the Elite)
• We will continue to service and repair the pumps for the life of the warranty and up to 3 years following any discontinuation
More Q&As
Let’s Keep the Blood Flowing!
Compression Therapy
Global Distributor Summit
Las Vegas, 3rd June 2013

• What is Compression Therapy
– How does it differ from VTE prevention
• A tour through our DJO factory
• Veinax Programme
– Rationale
– Product Specification
– Marketing Support
• Our Expertise
• Case Study
External pressure has the effect of:
• Reducing the diameter of the superficial and deep veins.
• Reestablishing the functionality of the valves by narrowing vein diameter
• Retaining the interstitial fluid in the vessels.
• Improve lymphatic microcirculation.
• Increase circulation at the level of the skin.
Venous Compression: Mode of Action
No compression With compression
Relaxing of walls, valve reflux
Excess pressure standing & slow down of return
Pressure exerted by compression opposed to hydrostatic pressure & reflux
Pressure exerted at ankle more important than calf or thigh
• Recumbent/immobile
– Patients laying in bed require low levels of pressure (>10mmHg) to control venous stasis
– This is sufficient to prevent thrombus formation
– Pressures in excess of 30 mmHg do not have beneficial effect if patient is laying down
• Ambulatory/standing
– Far higher levels of pressure required to influence blood flow
– Pressure during walking fluctuates between 20-100mmHg
– Working pressures of 40-50mmHg are required to influence this
Why different levels of compression?
• Recumbent/immobile
– Patients laying in bed require low levels of pressure (>10mmHg) to control venous stasis
– This is sufficient to prevent thrombus formation
– Pressures in excess of 30 mmHg do not have beneficial effect if patient is laying down
• Ambulatory/standing
– Far higher levels of pressure required to influence blood flow
– Pressure during walking fluctuates between 20-100mmHg
– Working pressures of 40-50mmHg are required to influence this
Why different levels of compression?
• Affects blood vessels of circulatory system • Various terms used
– Post-thrombotic syndrome – Chronic venous insufficiency – Chronic venous disease
• Can be as a result of: – DVT / PE – Phlebitis (inflammation of the vein) – Higher than normal blood pressure in the veins leading to damage to
the valves (incompetent valves) – Family history of varicose veins – Environmental/behavioural factors
• Prolonged standing or sitting
– Personal factors • Overweight • Pregnancy • Smoking • Lack of exercise
Venous Diseases – What are they?
• Swelling at the ankles
• Calves feel tight
• Legs may feel heavy, tight, restless or achy
• May be painful to walk
• Discolouration of the skin
• Varicose veins
• Itchiness of skin
Symptoms
• In venous disease, large veins become incompetent
• Blood refluxes back towards feet instead of passing smoothly towards heart
• Blood oscillates between damaged segments of valves
• Leads to gradual rise in pressure in venous circulation
– Walking no longer effective at reducing pressure
– Changes occur in microcirculation • Oedema formation
• Tissue changes (lipodermatosclerosis)
• Possibly ulceration
Venous Circulation
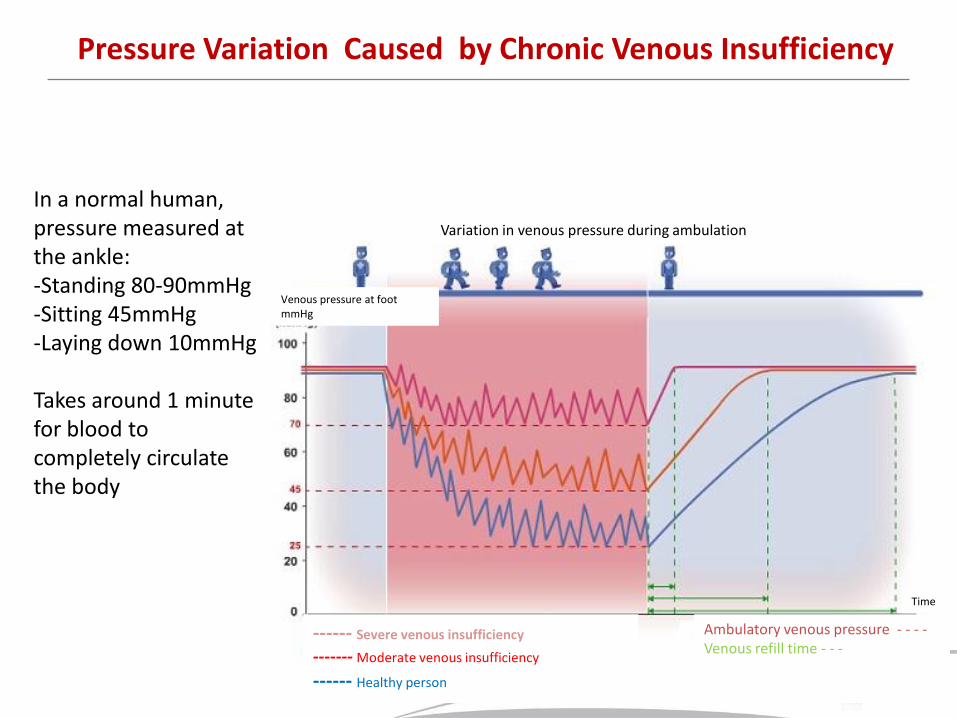
Pressure Variation Caused by Chronic Venous Insufficiency
In a normal human, pressure measured at the ankle: -Standing 80-90mmHg -Sitting 45mmHg -Laying down 10mmHg
Takes around 1 minute for blood to completely circulate the body
Variation in venous pressure during ambulation
Venous pressure at foot mmHg
------ Severe venous insufficiency
------- Moderate venous insufficiency
------ Healthy person
Ambulatory venous pressure - - - - Venous refill time - - -
Time
• 1st Stage
– Venous dilation without oedema
– Legs feel heavy, pain in calf, night cramps, skin feels hot and burning
• 2nd Stage
– Venous dilation with oedema in feet and ankles, especially at night, during warm weather and then eventually permanently
• 3rd Stage
– Complications of chronic venous insufficiency (CVI)
– Varicose eczema, skin pigmentation, hyperdermatitis, leg ulcers
Stages of Venous Insufficiency
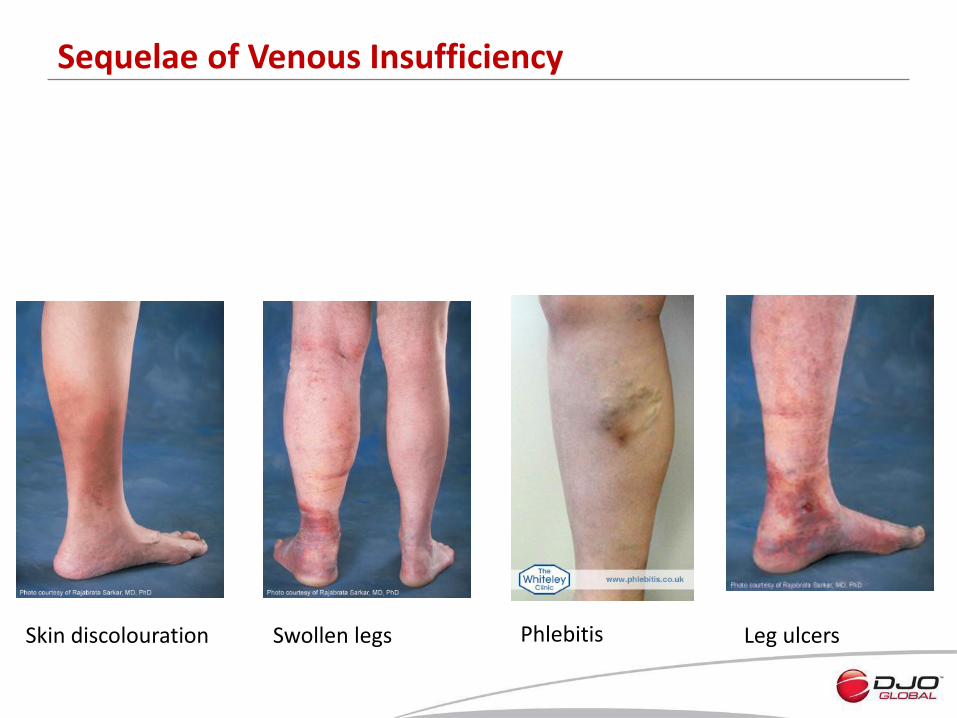
Skin discolouration Swollen legs Leg ulcers
Sequelae of Venous Insufficiency
Phlebitis
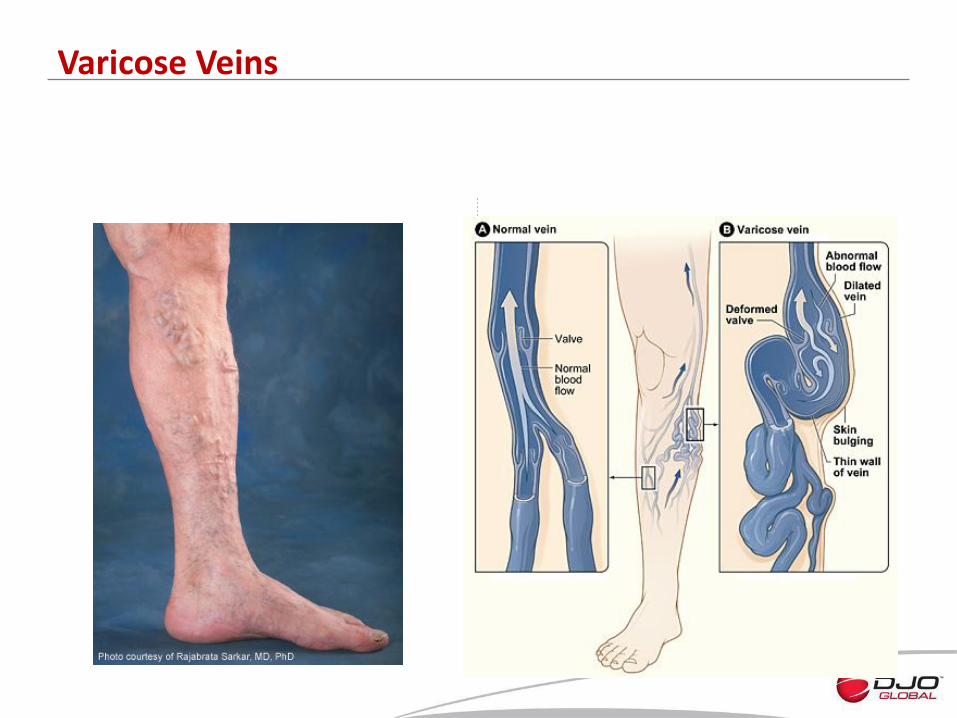
Varicose Veins
• Conservative:
– Exercise
– Compression therapy • Stockings
• Layered bandages
• Garments
– Wound and skin care
– Pharmacological therapy
• Interventional: – Sclerotherapy
– Ablative therapy with endovenous radiofrequency and laser
– Endovascular therapy
• Surgical: – Ligation and stripping
– Subfascial endoscopic perforator surgery
– Valve reconstruction
Treatment Options
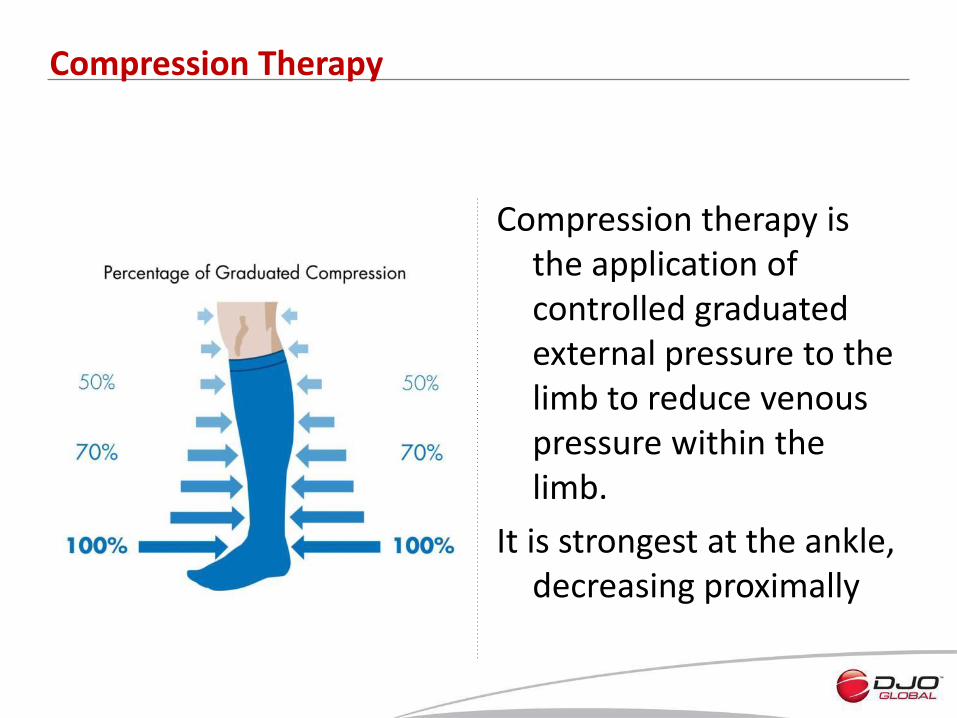
Compression therapy is the application of controlled graduated external pressure to the limb to reduce venous pressure within the limb.
It is strongest at the ankle, decreasing proximally
Compression Therapy
So What is the Fuss?
• Prevalence of varicose veins estimated at between 5 – 30% of adults:
– Female : Male 3:1
• CVI been estimated in:
– 21.2% of men >50yrs
– 12.0% of women >50yrs
• Estimated prevalence of venous ulcers of ≈ 0.3%
• US estimates that ≈ 2.5m have CVI
– Of which 20% will develop venous ulcers
• > 50% of venous ulcers require prolonged therapy lasting >1yr
The effects of varicose veins and CVI are devastating both for the patient, but also the family and the healthcare system
Welcome to Asheboro
Headquarters in Asheboro, North Carolina Established 1989 Started with 25 employees and 30 knitting machines. Jan 2011 DJO acquired ETI Now employs 235 personnel
We are the world’s largest manufacturer of medical graduated compression hosiery for the private label industry.
ETI (Elastic Therapy Inc.) Now DJO
233 Knitting Machines 140,00 pairs knitted per week > 7 million pairs per year
Knitting

•
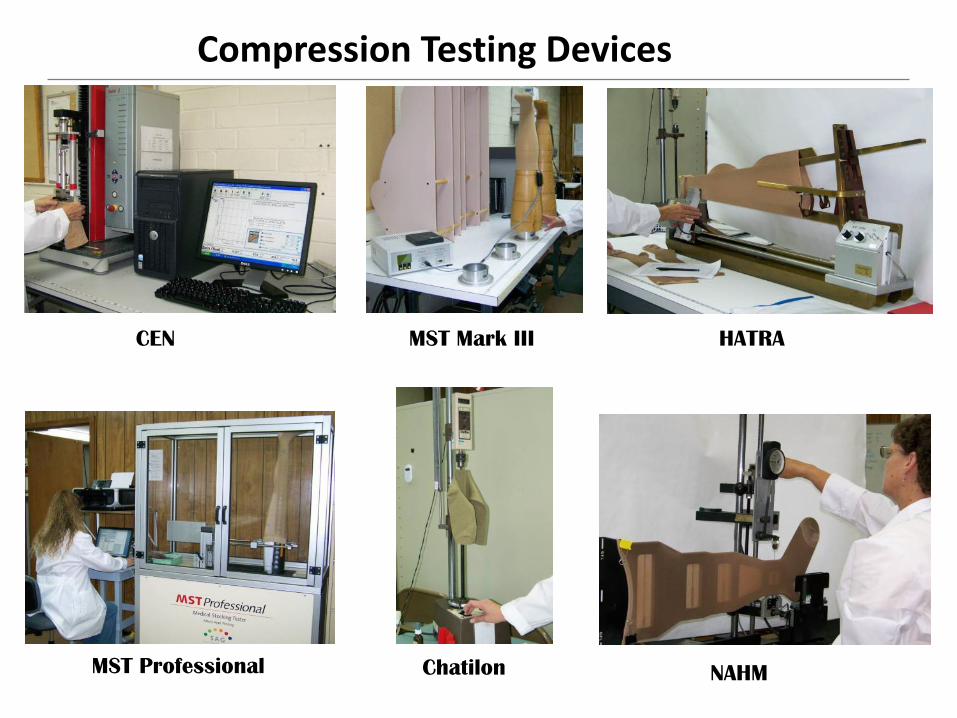
Compression Testing Devices
HATRA
NAHM MST Professional
CEN MST Mark III
Chatilon
Dyeing
Boarding
Sewing
75 sewing machines

> 6,000 SKUs
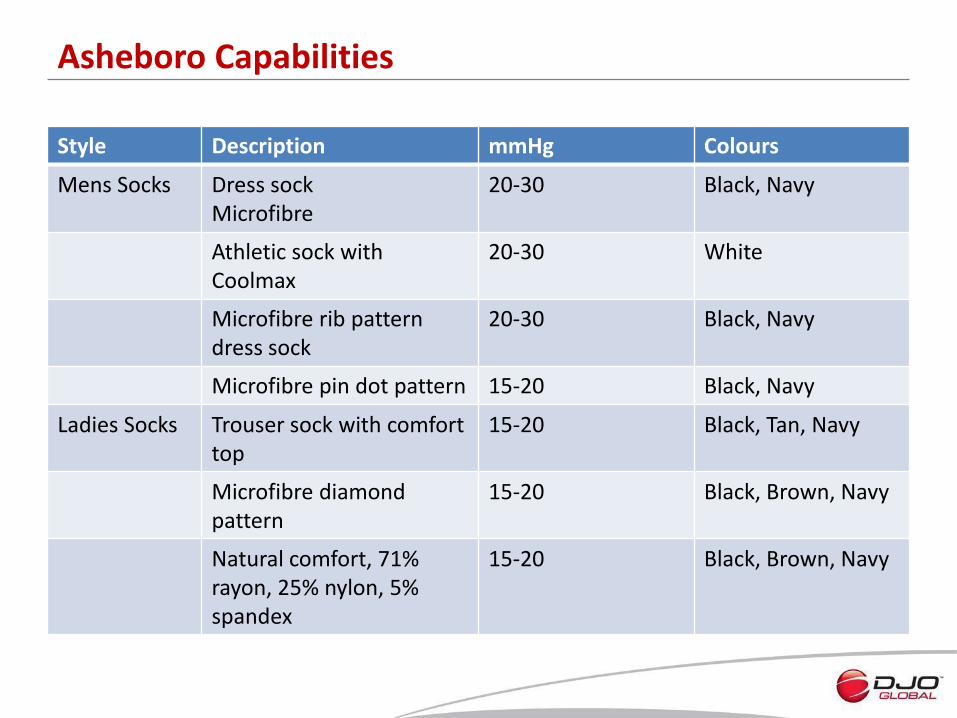
Asheboro Capabilities
Style Description mmHg Colours
Mens Socks Dress sock Microfibre
20-30
Black, Navy
Athletic sock with Coolmax
20-30 White
Microfibre rib pattern dress sock
20-30 Black, Navy
Microfibre pin dot pattern 15-20 Black, Navy
Ladies Socks Trouser sock with comfort top
15-20 Black, Tan, Navy
Microfibre diamond pattern
15-20 Black, Brown, Navy
Natural comfort, 71% rayon, 25% nylon, 5% spandex
15-20 Black, Brown, Navy
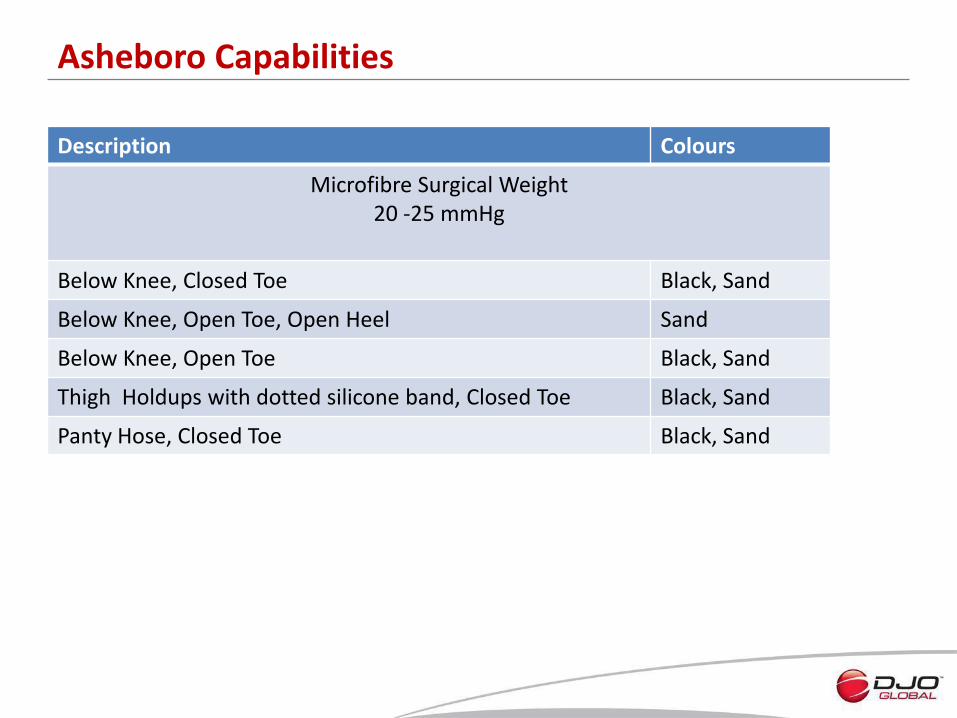
Asheboro Capabilities
Description Colours
Microfibre Surgical Weight 20 -25 mmHg
Below Knee, Closed Toe Black, Sand
Below Knee, Open Toe, Open Heel Sand
Below Knee, Open Toe Black, Sand
Thigh Holdups with dotted silicone band, Closed Toe Black, Sand
Panty Hose, Closed Toe Black, Sand
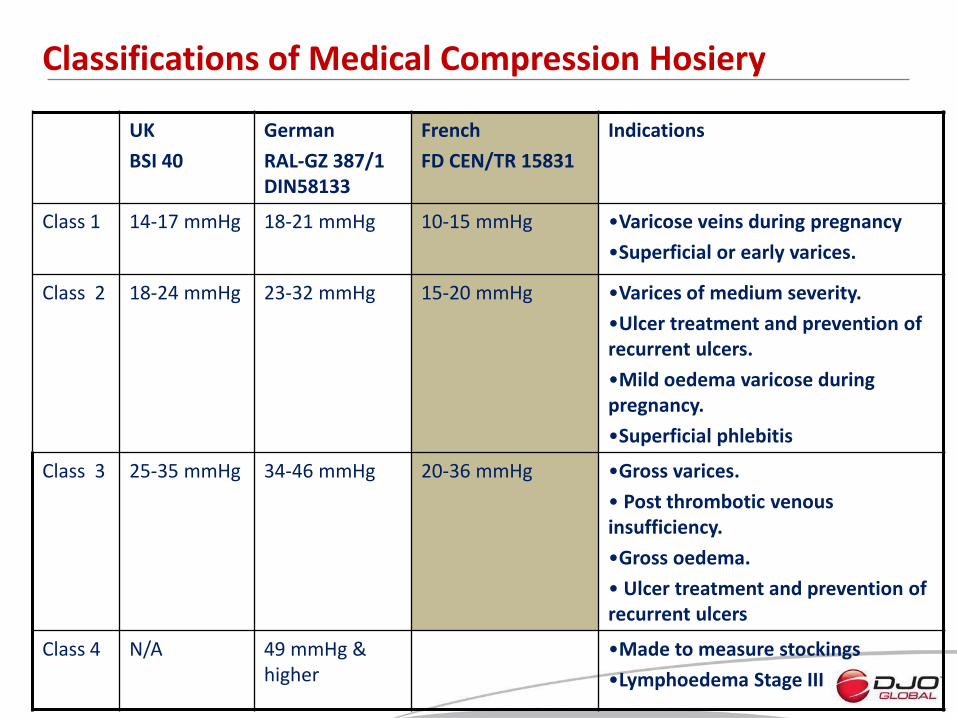
Classifications of Medical Compression Hosiery
UK
BSI 40
German
RAL-GZ 387/1 DIN58133
French
FD CEN/TR 15831
Indications
Class 1 14-17 mmHg
18-21 mmHg 10-15 mmHg •Varicose veins during pregnancy
•Superficial or early varices.
Class 2 18-24 mmHg
23-32 mmHg 15-20 mmHg •Varices of medium severity.
•Ulcer treatment and prevention of recurrent ulcers.
•Mild oedema varicose during pregnancy.
•Superficial phlebitis
Class 3 25-35 mmHg
34-46 mmHg 20-36 mmHg •Gross varices.
• Post thrombotic venous insufficiency.
•Gross oedema.
• Ulcer treatment and prevention of recurrent ulcers
Class 4 N/A 49 mmHg & higher
•Made to measure stockings
•Lymphoedema Stage III
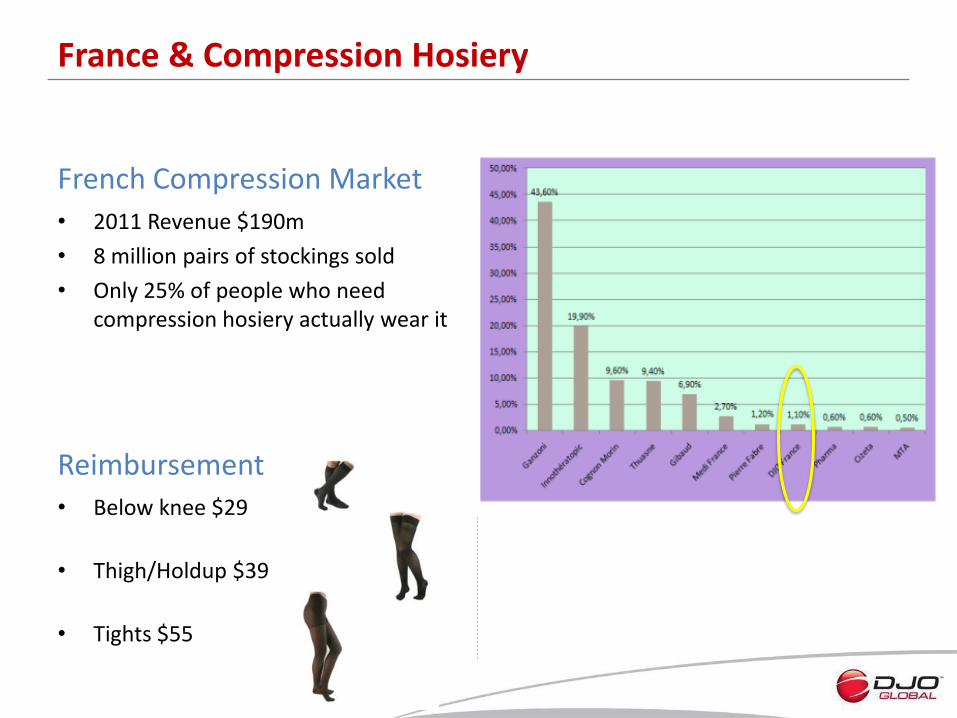
• 2011 Revenue $190m
• 8 million pairs of stockings sold
• Only 25% of people who need compression hosiery actually wear it
French Compression Market
French Competition
• Below knee $29
• Thigh/Holdup $39
• Tights $55
Reimbursement
France & Compression Hosiery

Veinax France
• Old
– 228 SKUs
– One length
– Mediocre quality
– Healthy sales
• New
– 360 SKU
– 2 lengths
– Exceptional quality
– Modern design
– Major push on sales
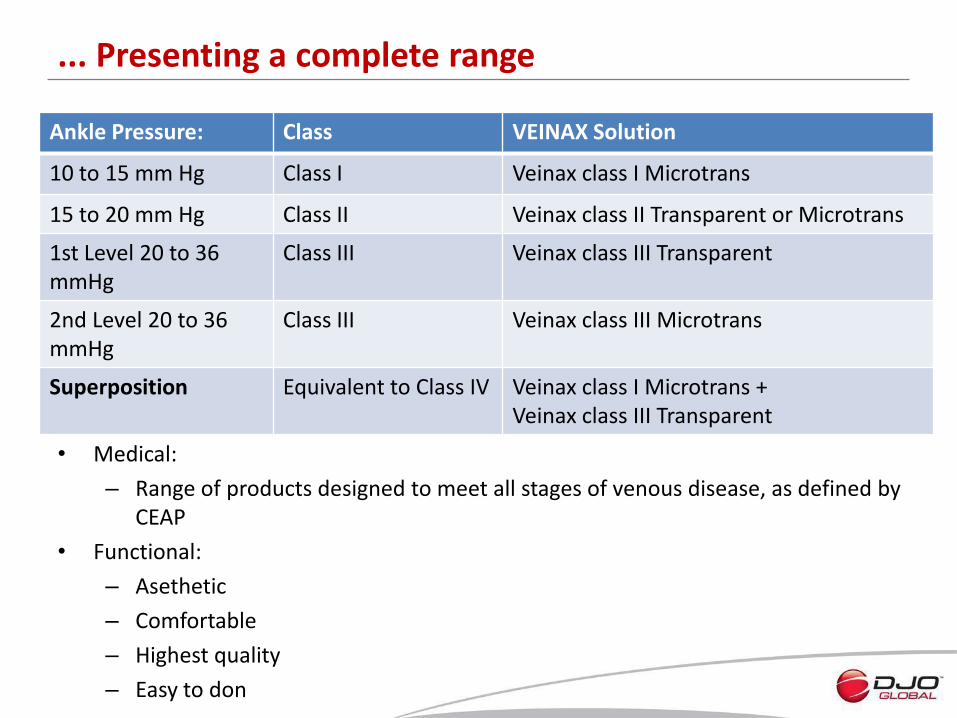
... Presenting a complete range
Ankle Pressure: Class VEINAX Solution
10 to 15 mm Hg Class I Veinax class I Microtrans
15 to 20 mm Hg Class II Veinax class II Transparent or Microtrans
1st Level 20 to 36 mmHg
Class III Veinax class III Transparent
2nd Level 20 to 36 mmHg
Class III Veinax class III Microtrans
Superposition Equivalent to Class IV Veinax class I Microtrans + Veinax class III Transparent
• Medical:
– Range of products designed to meet all stages of venous disease, as defined by CEAP
• Functional:
– Asethetic
– Comfortable
– Highest quality
– Easy to don
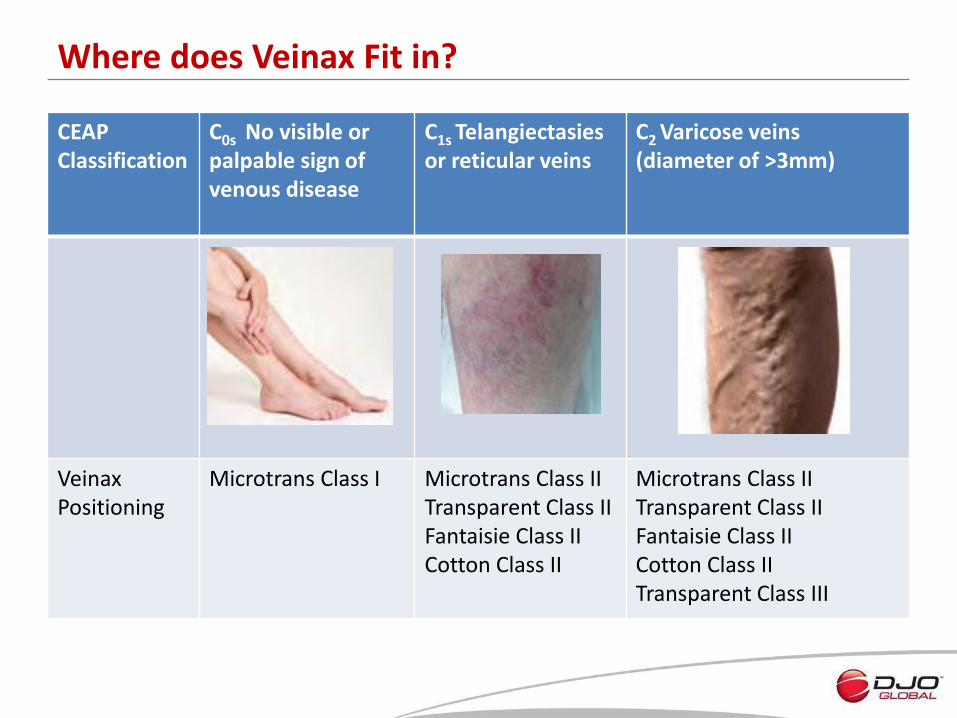
CEAP Classification
C0s No visible or palpable sign of venous disease
C1s Telangiectasies or reticular veins
C2 Varicose veins (diameter of >3mm)
Veinax Positioning
Microtrans Class I Microtrans Class II Transparent Class II Fantaisie Class II Cotton Class II
Microtrans Class II Transparent Class II Fantaisie Class II Cotton Class II Transparent Class III
Where does Veinax Fit in?
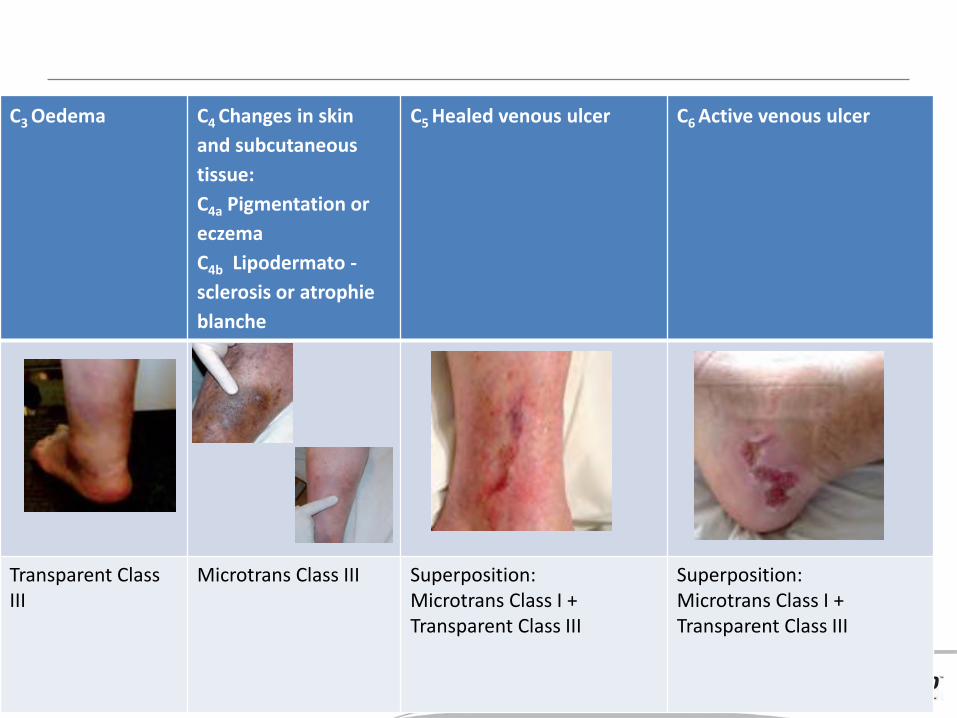
C3 Oedema
C4 Changes in skin
and subcutaneous
tissue:
C4a Pigmentation or
eczema
C4b Lipodermato -
sclerosis or atrophie
blanche
C5 Healed venous ulcer C6 Active venous ulcer
Transparent Class III
Microtrans Class III Superposition: Microtrans Class I + Transparent Class III
Superposition: Microtrans Class I + Transparent Class III
• Quality of manufacture
• Softness of yarn
• Softness on skin
• Easy to don
• Robust yarn but softness maintained
• Modern, attractive packaging
Subjective Aspects
• Extra flat seams:
– Toe box
– Self fixating band
• Extendable toe box which adapts to all morphologies.
• Reinforced section at level of toe.
• Reinforced sole.
• Reinforced heel.
• Wide hem for knee high.
• Panty area of the tights provides additonal support without extra compression.
• Unequalled transparency.
• Edge to edge stitching on the top band.
Objective Aspects



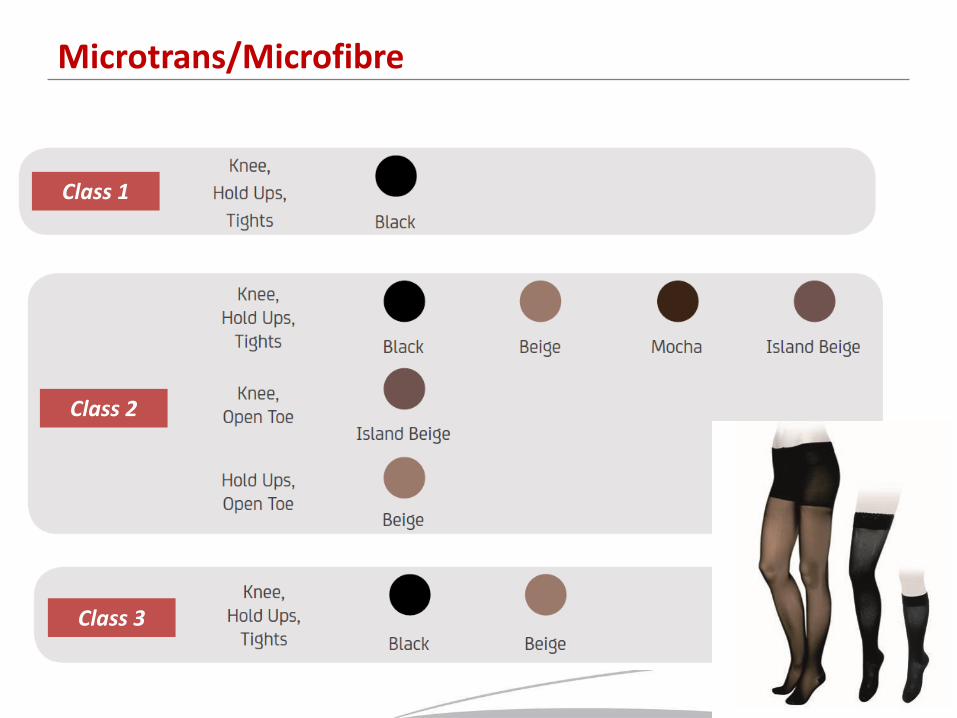
Microtrans/Microfibre
Class 1
Class 2
Class 3

Fantaisie / Diamond Pattern (Microfibre)
Class 2
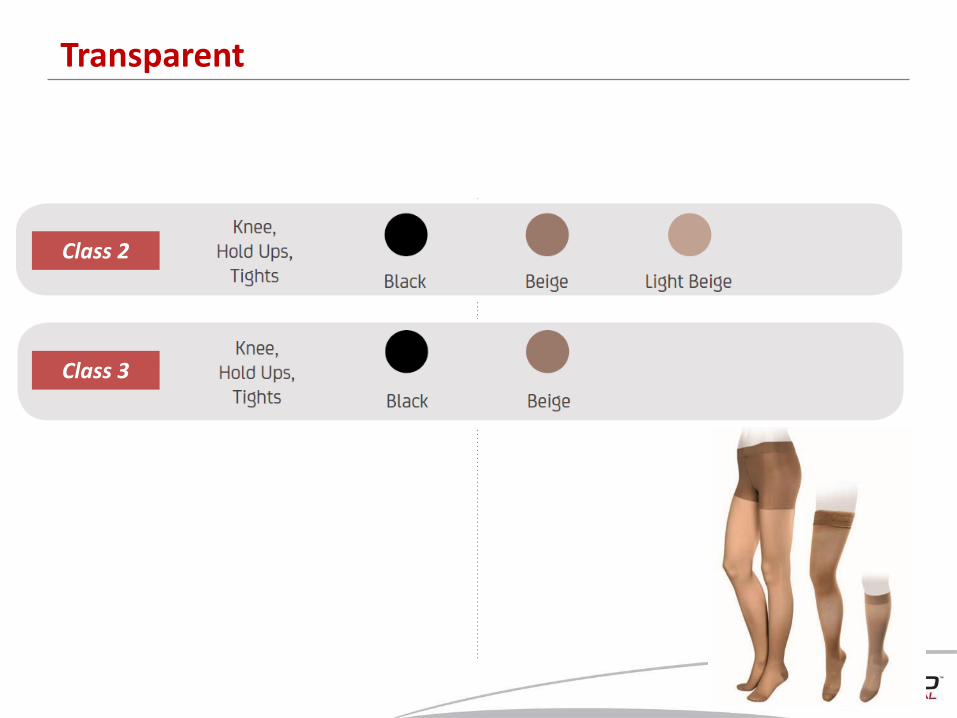
Transparent
Class 2
Class 3
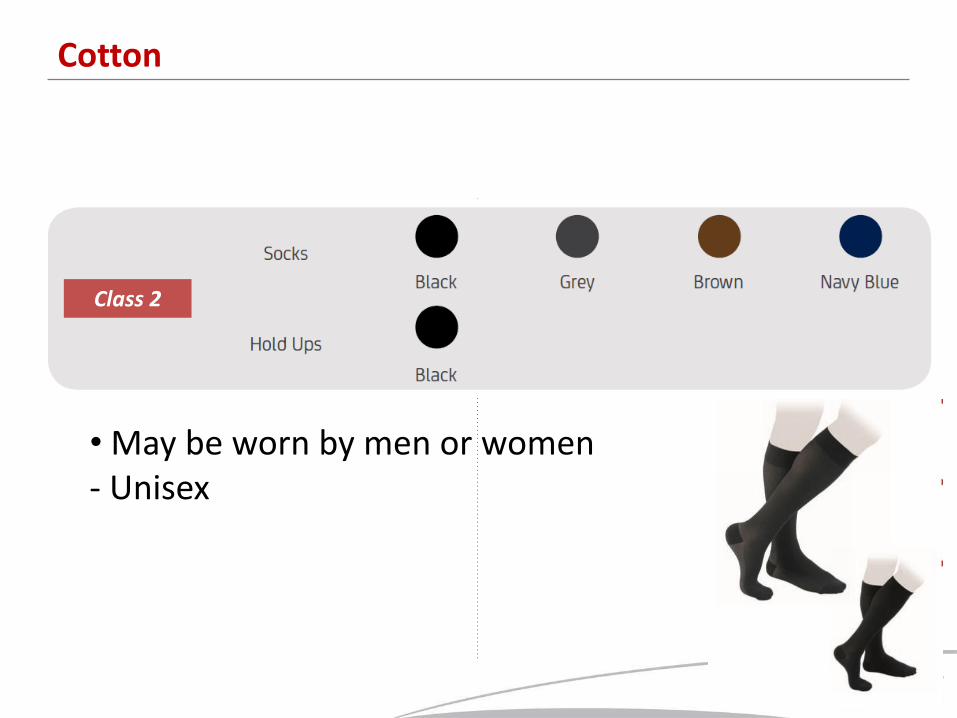
Cotton
• May be worn by men or women - Unisex
Class 2
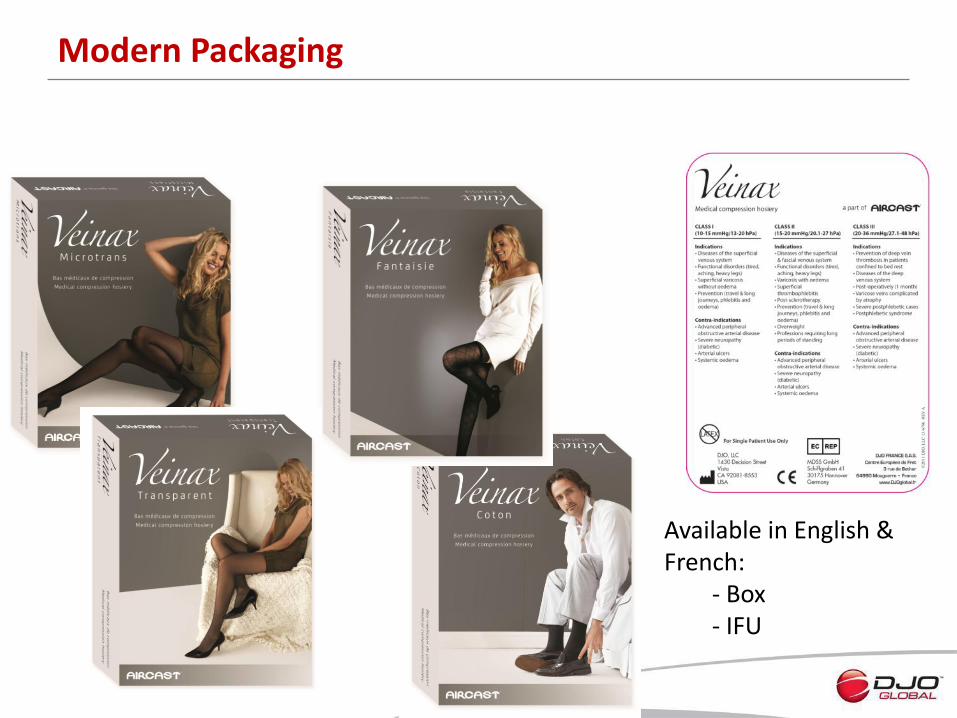
Modern Packaging
Available in English & French: - Box - IFU
Your Team in Asheboro

Welcome
• ETI Compression Stocking
• In Hospital & Retail Channels
• Limfix Japan
Japan
Population 130M GDP per capita >$30K USD Healthcare expend. 8% of GDP Per person 2600 $
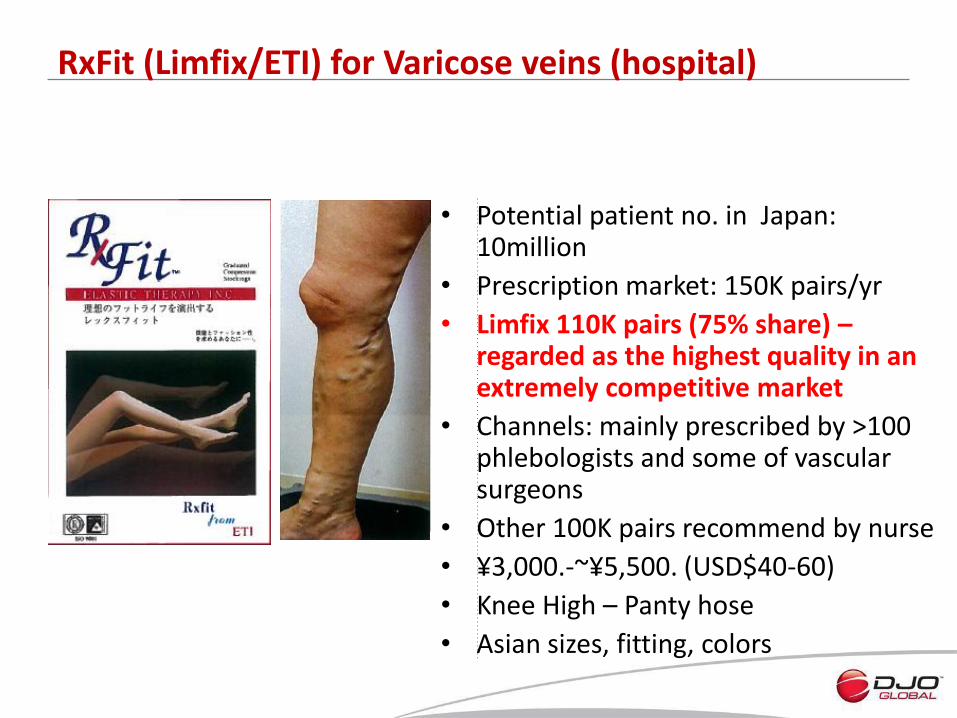
RxFit (Limfix/ETI) for Varicose veins (hospital)
• Potential patient no. in Japan: 10million
• Prescription market: 150K pairs/yr
• Limfix 110K pairs (75% share) – regarded as the highest quality in an extremely competitive market
• Channels: mainly prescribed by >100 phlebologists and some of vascular surgeons
• Other 100K pairs recommend by nurse
• ¥3,000.-~¥5,500. (USD$40-60)
• Knee High – Panty hose
• Asian sizes, fitting, colors

Current hospital channels: Society of Phlebology College of Angiology Society for Vascular Surgery Society for Lymphology
Developing hospital channels:
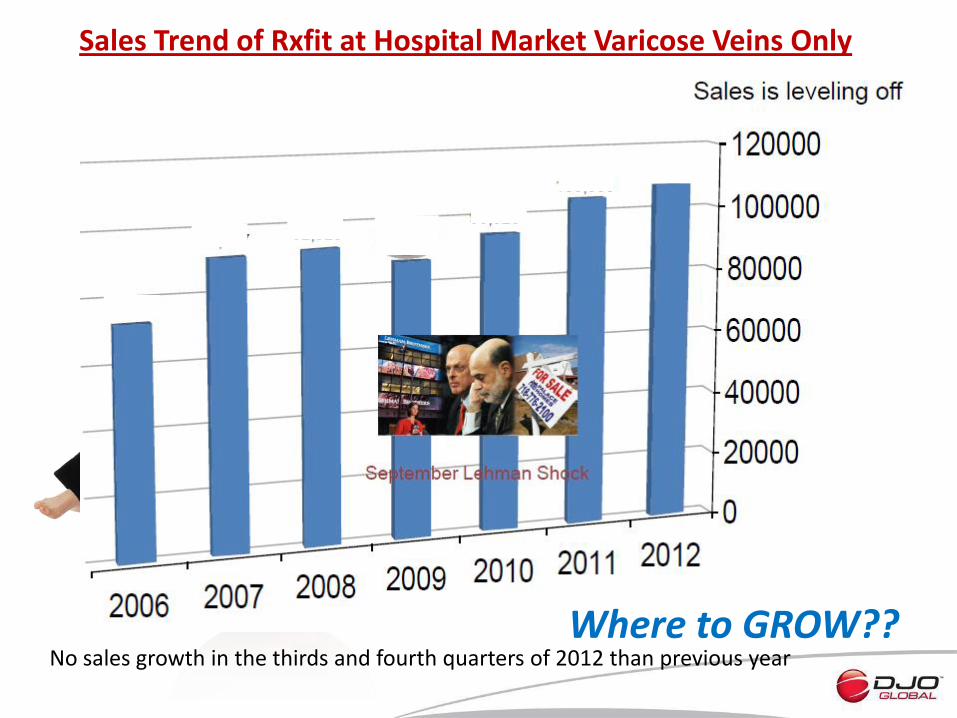
Sales Trend of Rxfit at Hospital Market Varicose Veins Only
No sales growth in the thirds and fourth quarters of 2012 than previous year Where to GROW??
Characteristics of Consumer Markets
(Varicose Veins, Fatigue, Edema and Slimness)
• OTC – No sales at over US$ 20.00 / pair
Dr. Scholl
• Mail Order (popular 10 years ago) and TV Shopping
• Internet Sales
- Market size >> x10 of hospital market
- There is no prominent player in the market
- > 20 competitors, nobody >5%
- Amazon, Rakuten portal…
TV Shopping

Strategies by LimFix
• Internet sales - starts advertising as of June 1, 2013
• New Company, New Brand, New Packing, New Pricing… for selling stockings as consumer products
• 15-20mmHg, beige and black, knee length and panty hose
• Target middle price range (>USD30)
- New Brand : Leg polus Fit New Company: Comprize Inc.

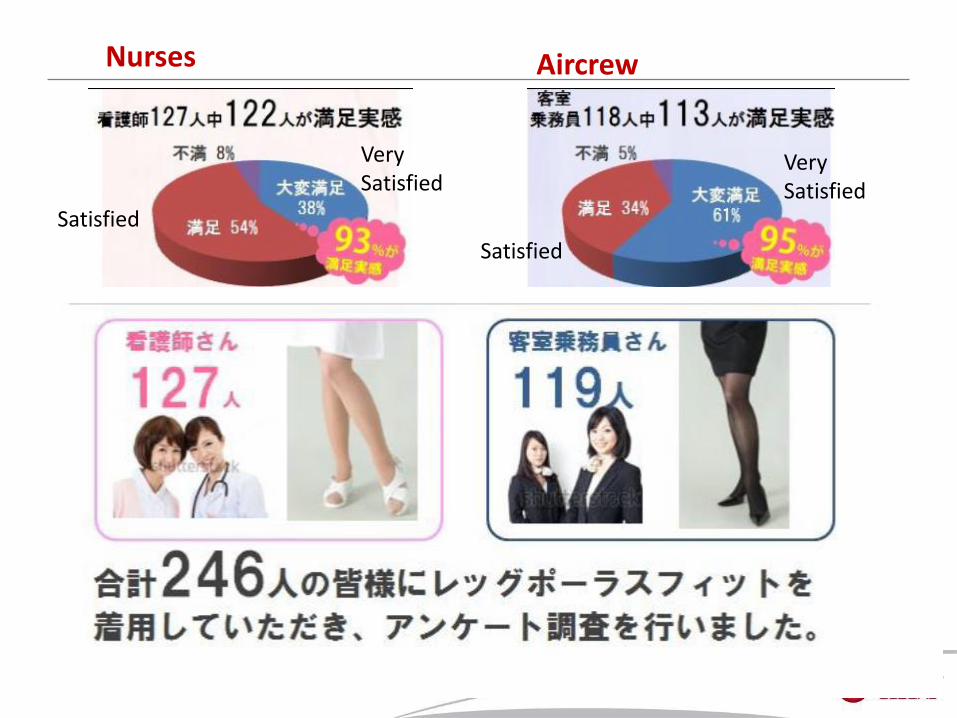
Satisfied
Very Satisfied
Nurses
Satisfied
Very Satisfied
Aircrew
• Increased awareness of varicose vein
• Large potential in E-channels
• ETI stockings has the highest quality, endorsed by healthcare professionals
• Leverage on Limfix local experties & experience
• Asian sizes, fitting, colors
• New venture for future GROWTH
Thank you!
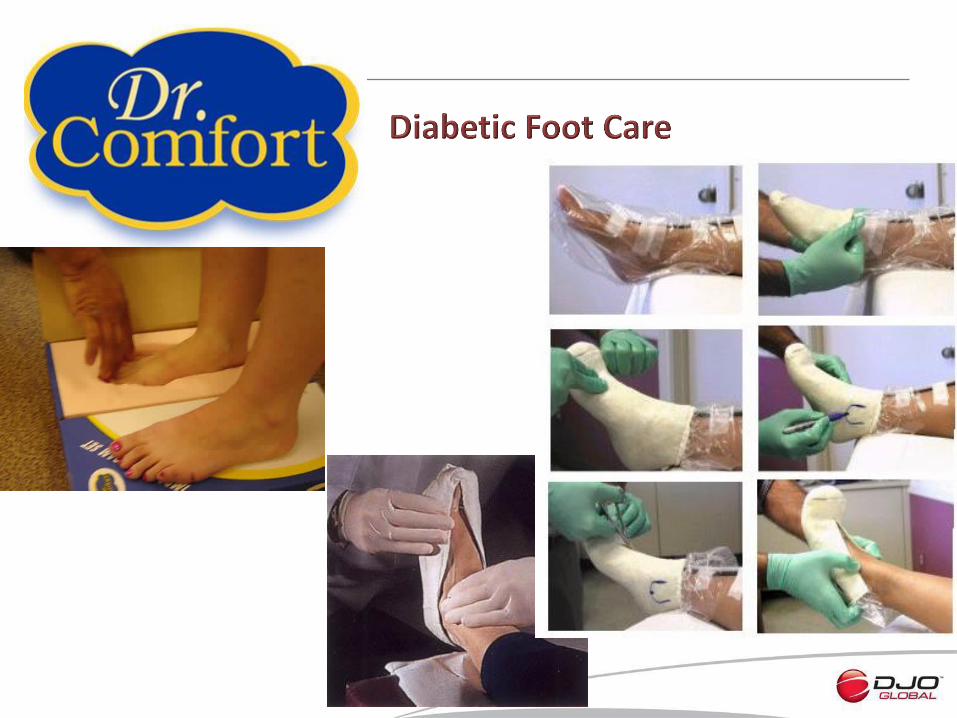
Dr Comfort Diabetic Foot Care
Global Distributor Summit
Las Vegas, 3rd June 2013
Dr Roy Lidtke
• Clinical associate professor of Podiatric Medicine specialising in lower extremity biomechanics
• Currently Assistant Professor, Department of Internal Medicine Section of Rheumatology at Rush University Medical Centre, Chicago
– Ranked among the top 50 hospitals in the US
• Published extensively on lower extremity biomechanics, often associated with osteoarthritis and the effect with therapeutic footwear
• Co-inventor on patent for the new Dr Comfort Flex-OA shoe
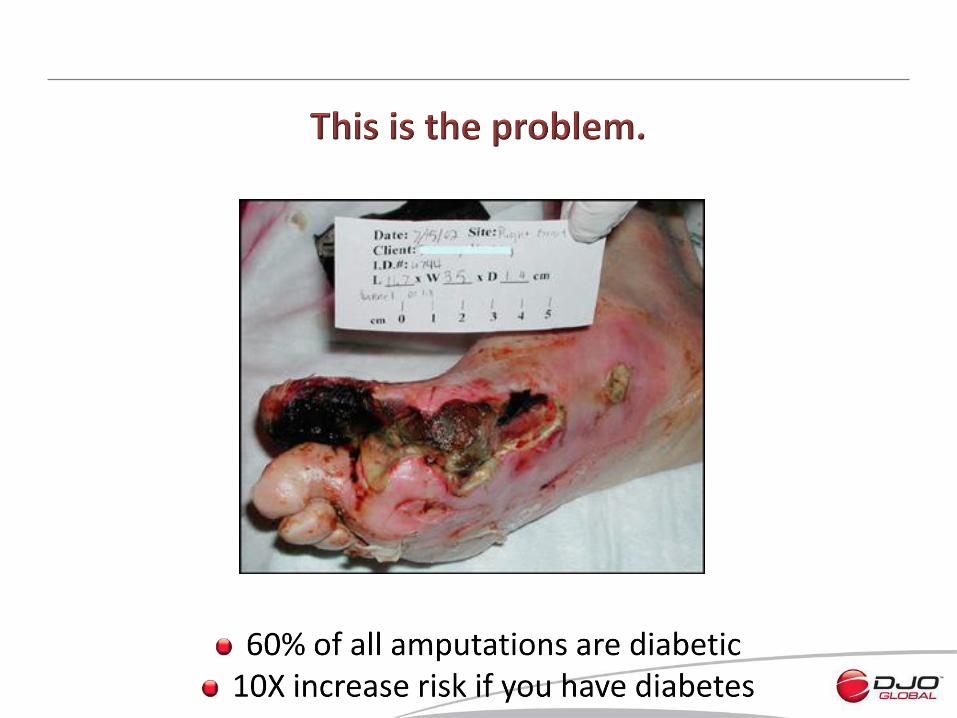
What has driven the US Dr Comfort Business?
• Driven by the cost & level of amputations in the US
• 1993 Therapeutic Shoes for Persons with Diabetes (TSPD) Act came into force
• Since 1996 number of foot and let amputations in the US fell by more than half
– Since Medicare started paying for blood sugar monitoring & protective shoes and other medical devices
– Increase in number of diabetics who had annual foot exam
• 2006 Therapeutic footwear for consumers with diabetes provided framework for specialist companies to receive reimbursement
– 1 pair of extra depth shoes plus 3 pairs of inserts per year
– Patients must present with diabetes and related foot condition
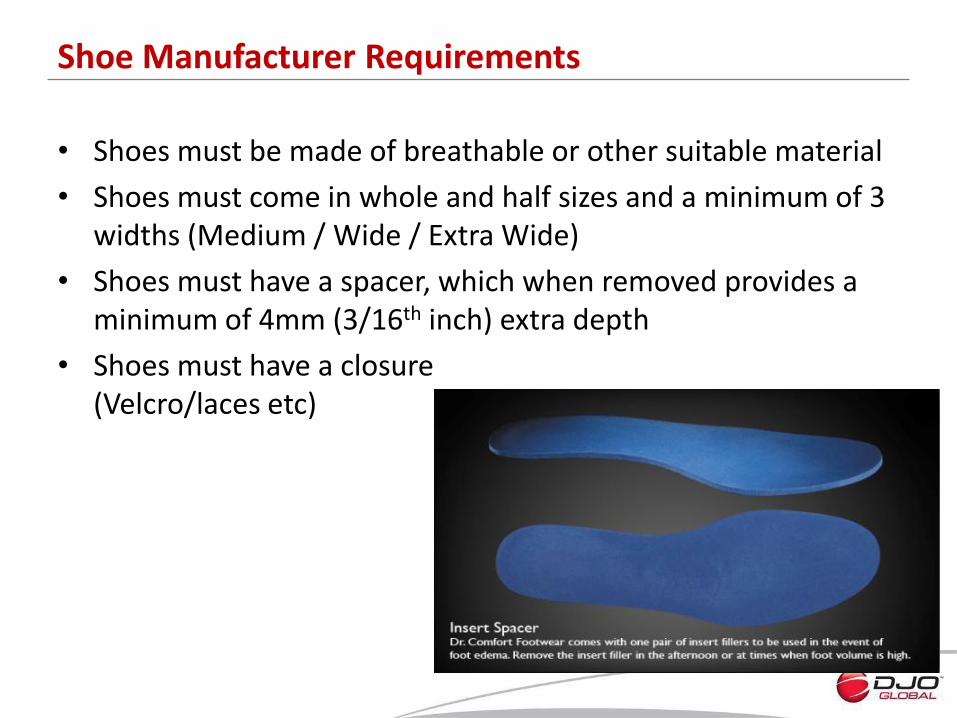
Shoe Manufacturer Requirements
• Shoes must be made of breathable or other suitable material
• Shoes must come in whole and half sizes and a minimum of 3 widths (Medium / Wide / Extra Wide)
• Shoes must have a spacer, which when removed provides a minimum of 4mm (3/16th inch) extra depth
• Shoes must have a closure (Velcro/laces etc)
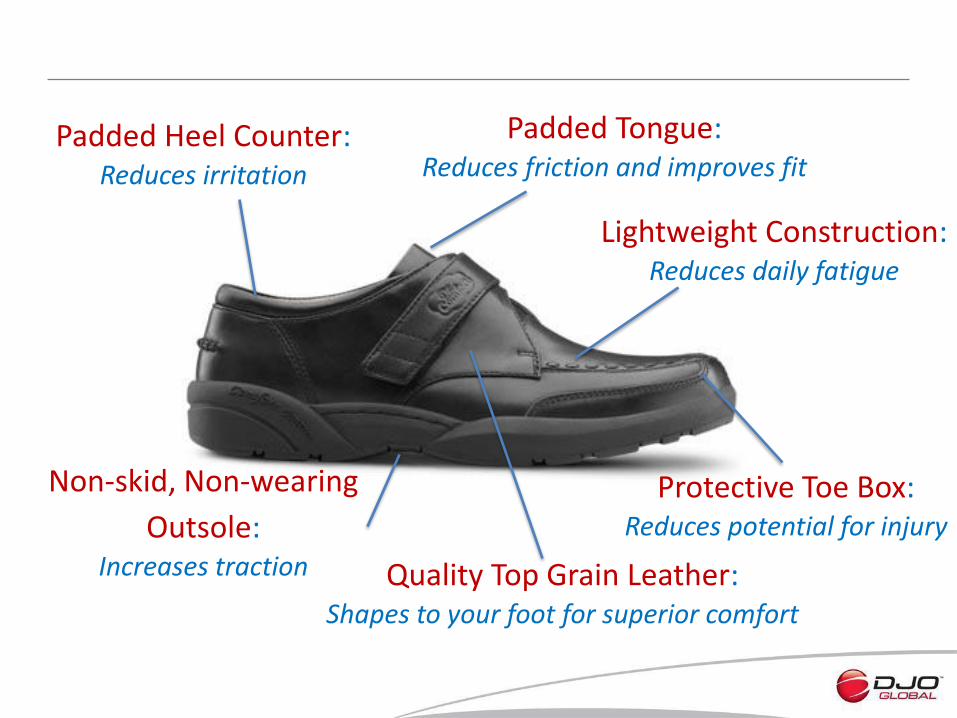
Padded Heel Counter: Reduces irritation
Padded Tongue: Reduces friction and improves fit
Non-skid, Non-wearing
Outsole: Increases traction
Protective Toe Box: Reduces potential for injury
Lightweight Construction: Reduces daily fatigue
Quality Top Grain Leather: Shapes to your foot for superior comfort

Firm Heel Counter: Provides enhanced support
Smooth Leather Lining: Keeps feet cool and dry while reducing chances for irritation
against seams
Extra Width & Depth in the
Toe Box & Forefoot Area: Reduces pressure on problem feet
Extra 11 mm Deep
Lightweight Outsole: Coring keeps soles light
Shankpiece: Give shoe structure and
makes the shoe bend only where your foot bends
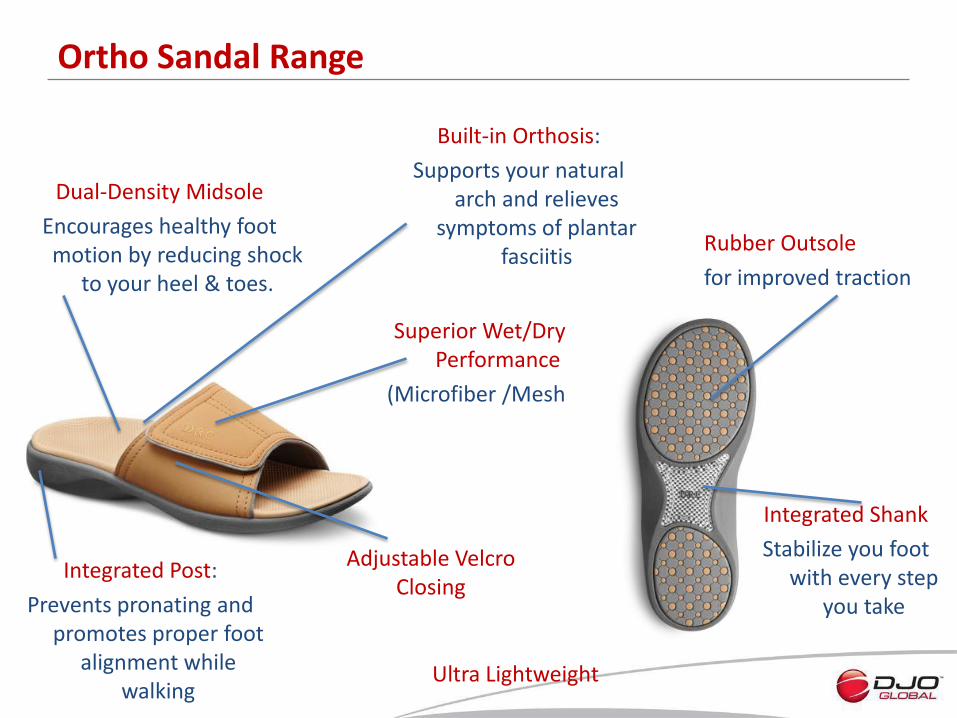
Ortho Sandal Range
Superior Wet/Dry Performance
(Microfiber /Mesh)
Dual-Density Midsole
Encourages healthy foot motion by reducing shock
to your heel & toes.
Ultra Lightweight
Adjustable Velcro Closing
Built-in Orthosis:
Supports your natural arch and relieves
symptoms of plantar fasciitis
Integrated Post:
Prevents pronating and promotes proper foot
alignment while walking
Integrated Shank
Stabilize you foot with every step
you take
Rubber Outsole
for improved traction
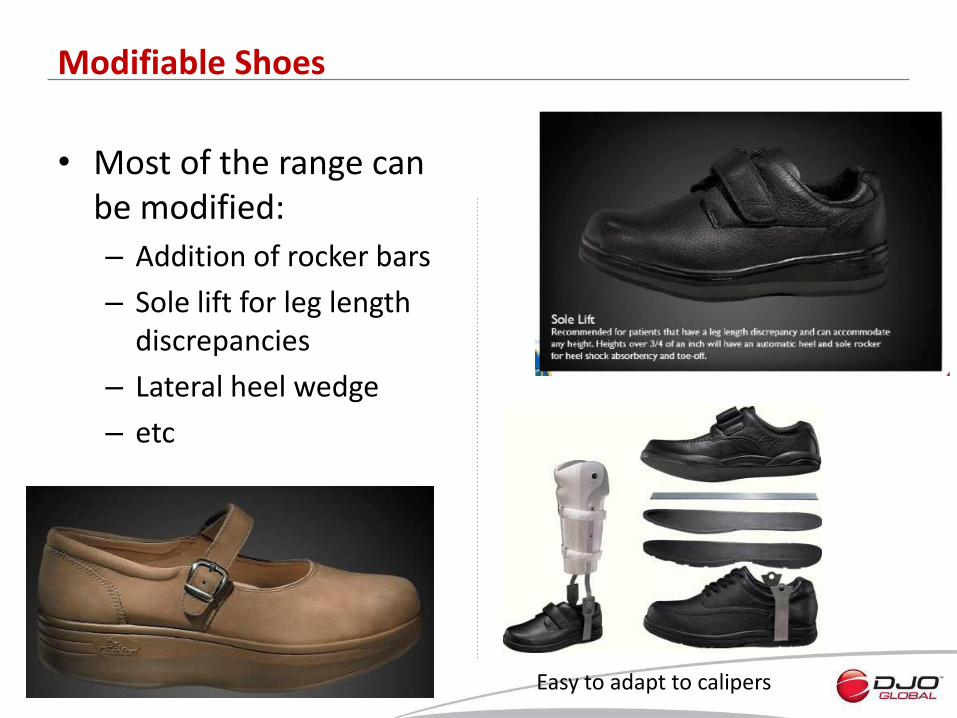
• Most of the range can be modified:
– Addition of rocker bars
– Sole lift for leg length discrepancies
– Lateral heel wedge
– etc
Modifiable Shoes
Easy to adapt to calipers
• Roy H. Lidtke • Assistant Professor of Internal Medicine
• Rush University Medical Center • Chicago, IL
DJO Global’s Vision
How do I get my patients moving without
causing tissue damage?
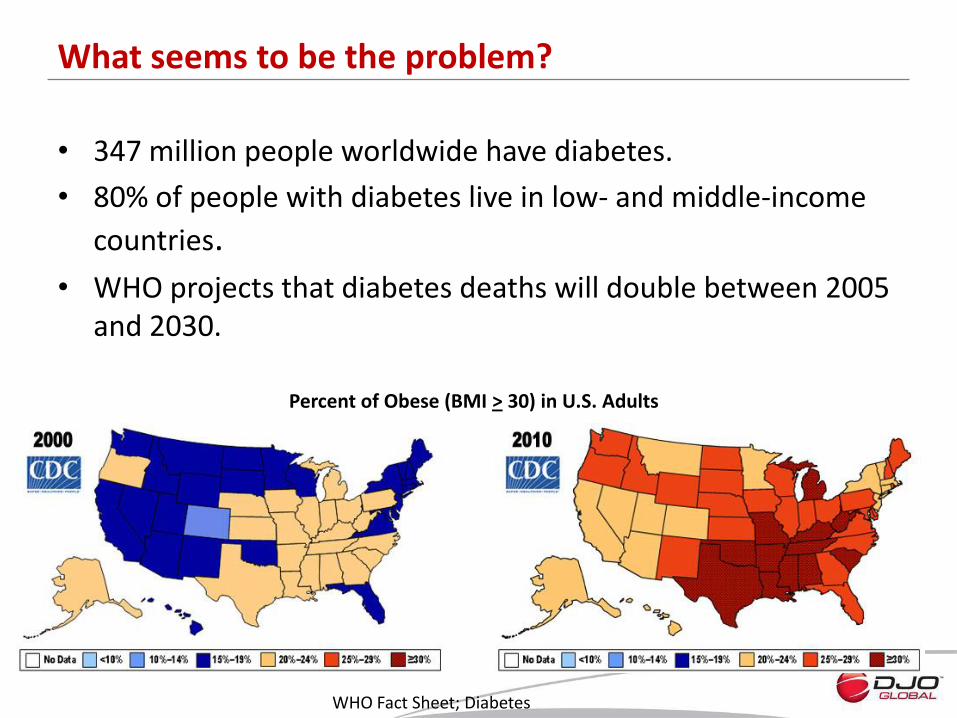
• 347 million people worldwide have diabetes.
• 80% of people with diabetes live in low- and middle-income
countries.
• WHO projects that diabetes deaths will double between 2005 and 2030.
What seems to be the problem?
Percent of Obese (BMI > 30) in U.S. Adults
WHO Fact Sheet; Diabetes
International Working Group on the Diabetic Foot Diabetes Metab Res Rev 2000; 16 (Suppl 1): S84±S92.
National Diabetes Information Clearinghouse NIH Publication No. 09–3185




Firm 20-30 mmHg Moderate 15-20 mmHg Gentle 10-15 mmHg

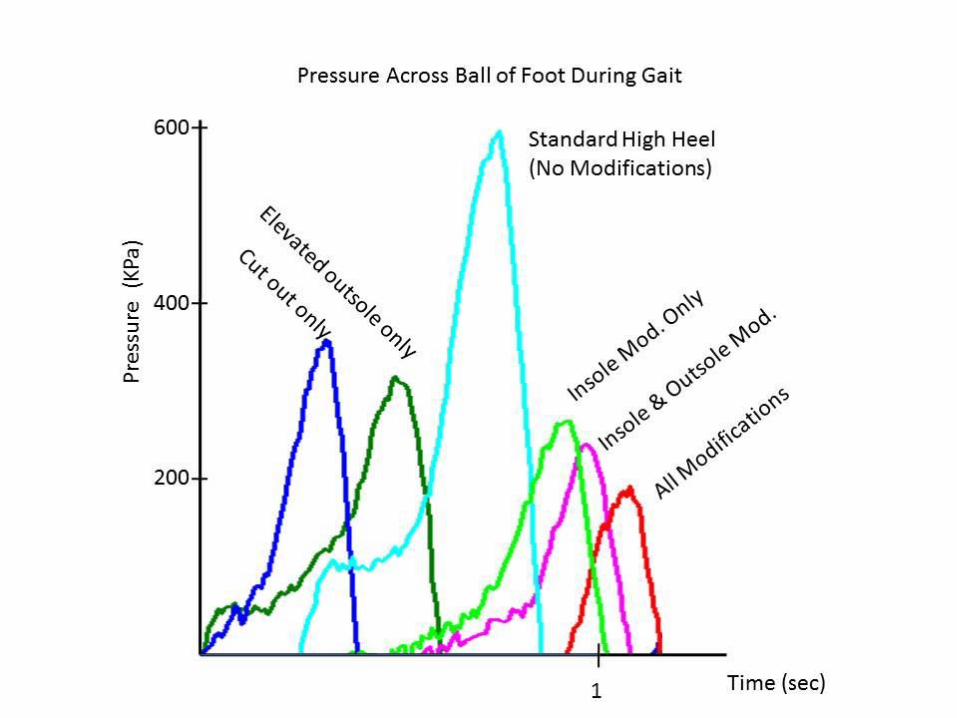
Metatarsal head area cut out lower
than toe
Anterior Rock Outsole Ball Depression
Elevated Proximal Area
Insole area elevated at central metatarsal shafts
Choices!
Men’s and Women’s Range
All Seasons
• USPs: – 3 widths
– Extra depth in toe box
– Lightweight
– Removeable insole
– Easily modifiable
– Modern design
• Advantages over competition: – Individual orders possible
– No minimum quantities
– Full fitting service available
– Short delivery times
– Product range maintained
Therapeutic shoes designed with comfort in mind
European Positioning

European Positioning
Casual Line Active Line Smart Line
Womens Betty Annie Patty
Refresh Spirit Plus Move Kelly
Kristin Delight Paradise
Mens Fisherman Douglas Justin
Performance Endurance Champion Plus Ranger
Captain Wing

Women’s Range
Betty Black
Move Black
Annie Black Annie Acorn
Delight Walnut Kristin Black
Patty Beige
Kelly Camel
Paradise Black
Refresh Pink Spirit Plus White
Delight Black
Betty Beige
Paradise Saddle Tan
Smart
Casual
Active
Douglas Chestnut Douglas Black
Wing Chestnut
Patrick Multi
Wing Black
Captain Chestnut
Ranger Black
Justin Chestnut Nubuck
Captain Black
Performance Black Champion Plus Black
Fisherman Black
Justin Black
Endurance Black
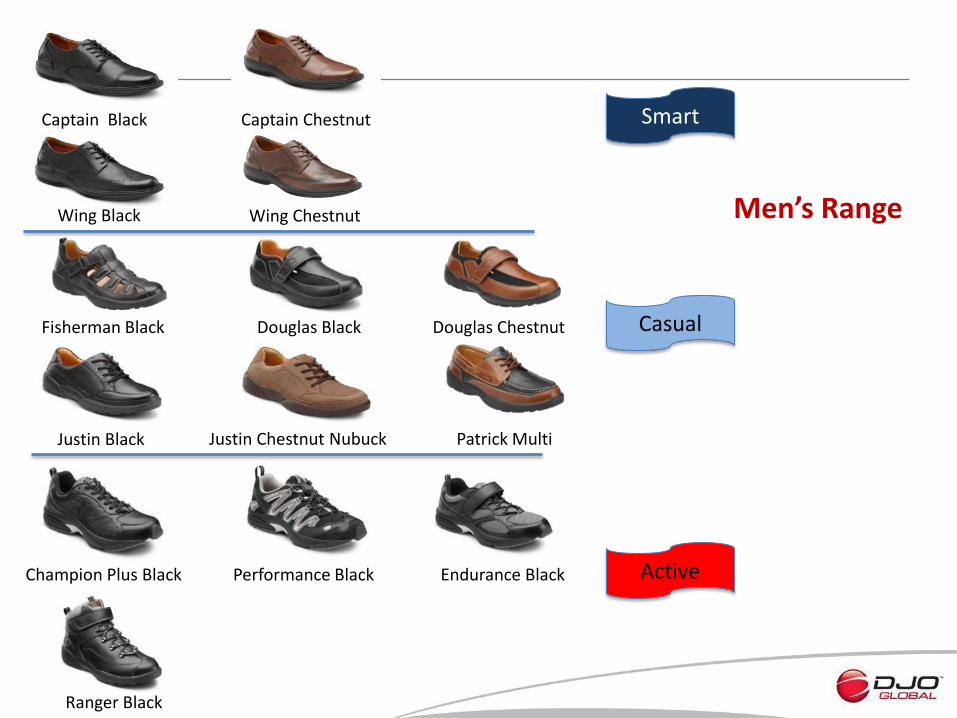
Men’s Range
Smart
Casual
Active
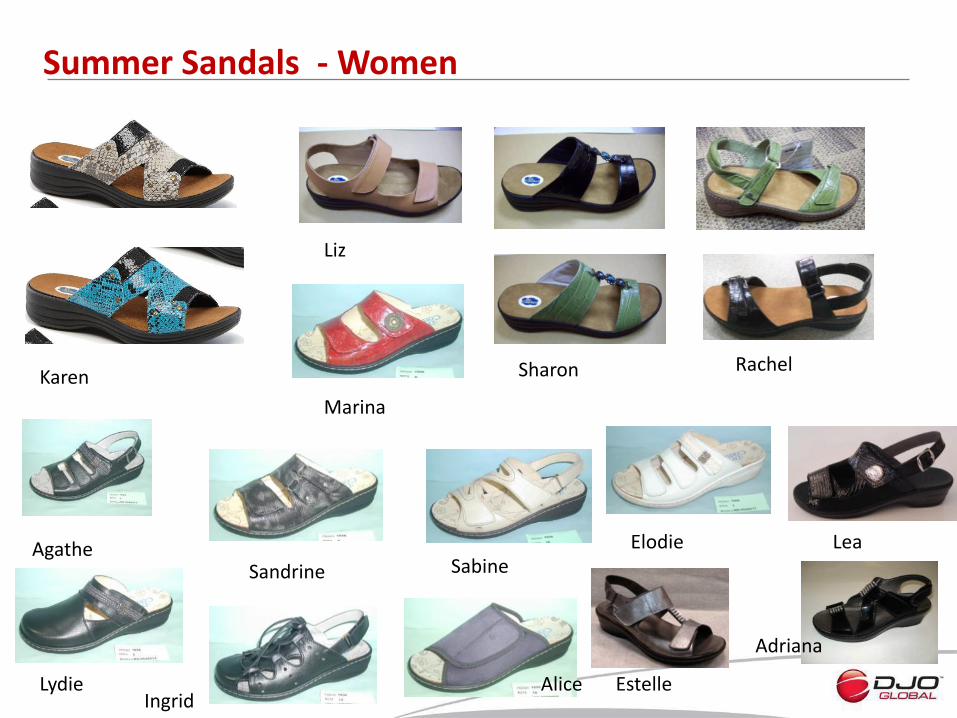
Summer Sandals - Women
Karen
Liz
Sharon Rachel
Agathe
Lydie
Marina
Sandrine Sabine
Ingrid
Elodie
Alice
Lea
Estelle
Adriana

Men’s Sandals
Pascal Benat
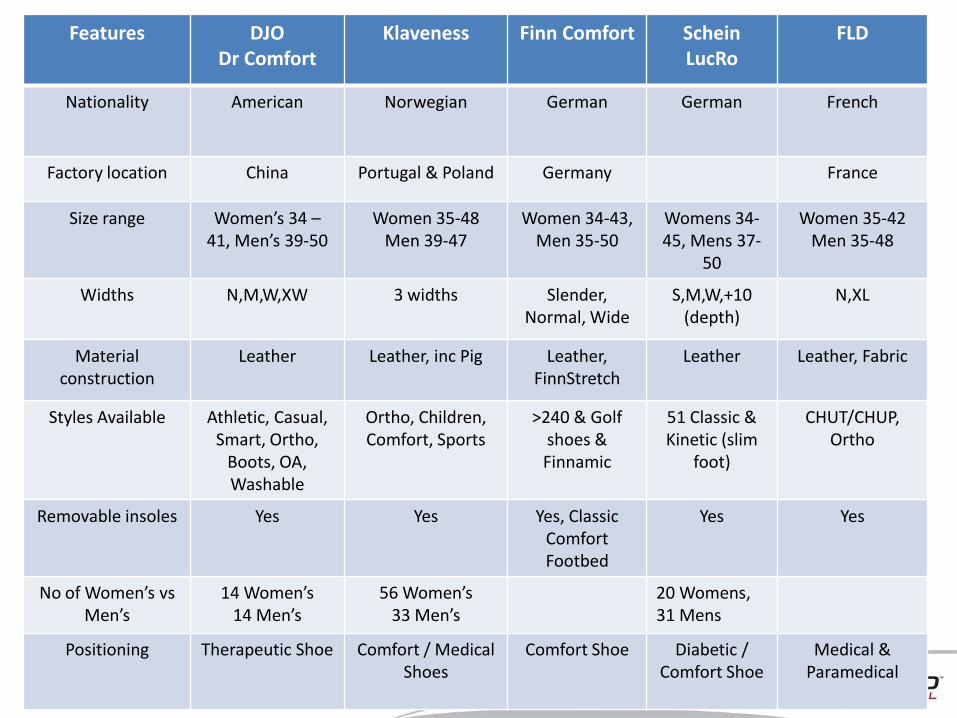
Competitor Overview Features DJO
Dr Comfort Klaveness Finn Comfort Schein
LucRo FLD
Nationality American Norwegian German German French
Factory location China Portugal & Poland Germany France
Size range Women’s 34 – 41, Men’s 39-50
Women 35-48 Men 39-47
Women 34-43, Men 35-50
Womens 34-45, Mens 37-
50
Women 35-42 Men 35-48
Widths N,M,W,XW 3 widths Slender, Normal, Wide
S,M,W,+10 (depth)
N,XL
Material construction
Leather
Leather, inc Pig Leather, FinnStretch
Leather Leather, Fabric
Styles Available Athletic, Casual, Smart, Ortho,
Boots, OA, Washable
Ortho, Children, Comfort, Sports
>240 & Golf shoes & Finnamic
51 Classic & Kinetic (slim
foot)
CHUT/CHUP, Ortho
Removable insoles Yes Yes Yes, Classic Comfort Footbed
Yes Yes
No of Women’s vs Men’s
14 Women’s 14 Men’s
56 Women’s 33 Men’s
20 Womens, 31 Mens
Positioning Therapeutic Shoe Comfort / Medical Shoes
Comfort Shoe Diabetic / Comfort Shoe
Medical & Paramedical
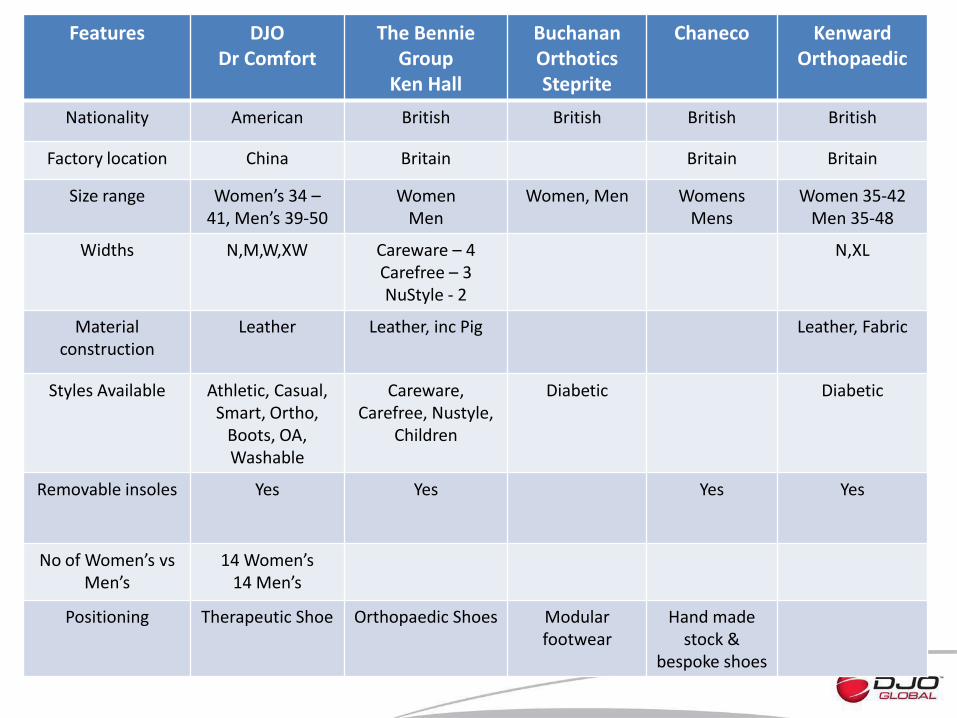
Competitor Overview Features DJO
Dr Comfort The Bennie
Group Ken Hall
Buchanan Orthotics Steprite
Chaneco Kenward Orthopaedic
Nationality American British British British British
Factory location China Britain Britain Britain
Size range Women’s 34 – 41, Men’s 39-50
Women Men
Women, Men Womens Mens
Women 35-42 Men 35-48
Widths N,M,W,XW Careware – 4 Carefree – 3 NuStyle - 2
N,XL
Material construction
Leather
Leather, inc Pig Leather, Fabric
Styles Available Athletic, Casual, Smart, Ortho,
Boots, OA, Washable
Careware, Carefree, Nustyle,
Children
Diabetic Diabetic
Removable insoles Yes Yes Yes Yes
No of Women’s vs Men’s
14 Women’s 14 Men’s
Positioning Therapeutic Shoe Orthopaedic Shoes Modular footwear
Hand made stock &
bespoke shoes