Embed Size (px)
Citation preview

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
799
VEGF Pathway-targeted Therapy for Advanced Renal Cell Carcinoma: A Meta-analysis of Randomized Controlled Trials
Fei LIU (刘 飞)1, Xianguo CHEN (陈先国)2, Ejun PENG (彭鄂军)3, Wei GUAN (管 维)3, Youyuan LI (李有元)3, Zhiquan HU (胡志全)3, Zhangqun YE (叶章群)3, Qianyuan ZHUANG (庄乾元)3 1Department of Urology, the Second Affiliated Hospital of Nanchang University, Nanchang 330006, China 2Department of Urology, the First Affiliated Hospital of Anhui Medical University, Hefei 230022, China 3Department of Urology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030,
China © Huazhong University of Science and Technology and Springer-Verlag Berlin Heidelberg 2011
Summary: Immunotherapy which has been in practice for more than 20 years proves effective for the treatment of metastatic renal cell carcinoma (mRCC). Anti-angiogenesis-targeted therapy has recently been identified as a promising therapeutic strategy for mRCC. This study was aimed to evaluate the ef-fectiveness of vascular endothelial growth factor (VEGF) pathway-targeted therapy for mRCC by com-paring its effectiveness with that of immunotherapy. The electronic databases were searched. Random-ized controlled trials (RCTs) on comparison of VEGF inhibiting drugs (sorafenib, sunitinib and bevaci-zumab) with interferon (IFN) or placebo for mRCC treatment were included. Data were pooled to meta-analyze. A total of 7 RCTs with 3451 patients were involved. The results showed that anti-VEGF agents improved progression-free survival (PFS) and offered substantial clinical benefits to patients with mRCC. Among them, sunitinib had a higher overall response rate (ORR) than IFN (47% versus 12%, P<0.000001). Bevacizumab plus IFN produced a superior PFS [risk ratio (RR): 0.86, 95% confidence interval (CI): 0.76–0.97; P=0.01] and ORR (RR: 2.19; 95% CI: 1.72–2.78; P<0.00001) in patients with mRCC over IFN, but it yielded an increase by 31% in the risk of serious toxic effects (RR: 1.31; 95% CI: 1.20–1.43; P<0.00001) as compared with IFN. The overall survival (OS) was extended by sorafenib (17.8 months) and sunitinib (26.4 months) as compared with IFN (13 months). It was concluded that compared with IFN therapy, VEGF pathway-targeted therapies improved PFS and achieved significant therapeutic benefits in mRCC. However, the risk to benefit ratio of these agents needs to be further evaluated. Key words: renal cell carcinoma; targeted therapy; vascular endothelial growth factor; meta-analysis; immunotherapy
Renal cell carcinomas (RCC) are the most fre-quently occurring cancer within the kidney. They are pathologically classified into different types and 85% of them are clear cell tumors[1–3]. According to the studies by Jemal et al[4, 5], an estimated 57 760 Americans were diagnosed with kidney cancer and 12 980 died of the disease in the United States in 2009, and 3 370 (ap-proximately by 6.2%) new cases were increased in the past one year. At initial presentation, 25%–30% of pa-tients with RCC are found to have overt metastases[6]. After nephrectomy, 20%–30% of patients with initially localized disease will experience relapse and progres-sion[7]. RCC patients developing metastases and relapse have a poor prognosis and the 5-year survival rate is less than 10%[8].
Metastatic RCC is an intractable disease due to in-herent tumor resistance to chemotherapy and radiother-
Fei LIU, E-mail: [email protected]
apy[9, 10]. The development of RCC is thought to be in-fluenced by the immune system, and thus in recent years, immunotherapeutic cytokines such as interferon (IFN) and interleukin 2 have been extensively investigated and applied in clinical practice. IFN has become a standard systemic therapy in mRCC. Some studies reported 10% to 15% overall response rate (ORR) in IFN therapies along with substantial toxicities and approximately 12 months of the median overall survival (OS)[11, 12]. Al-though a limited subset of patients (5%–10%) experi-enced durable complete remission, most gained no clini-cal benefits or couldn’t tolerate the adverse effects of immunotherapy[13]. For this reason, new therapies for mRCC have been clinically desired.
With the pathogenesis of RCC being further eluci-dated, more and more relevant therapeutic agents are identified and used in clinical practice. Von Hip-pel-Lindau (VHL) syndrome is an autosomal dominant disorder resulting from the mutation of the VHL tumor suppressor gene and this condition was found to be asso-ciated with increased susceptibility to clear-cell RCC[14].
J Huazhong Univ Sci Technol[Med Sci]
DOI 10.1007/s11596-011-0680-0 31(6):799-806,2011

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
800
Approximately 60% of the patients with clear-cell RCC were found to have inactivation (gene silencing, muta-tion) of VHL tumor suppressor gene, which would acti-vate the hypoxia-response pathway and result in the over-expression of hypoxia-inducible factor (HIF), lead-ing to the increased transcription of vascular endothelial growth factor (VEGF)[15, 16]. VEGF is a potent pro-angiogenic protein that can promote endothelial cell migration, increase vascular permeability and stimulate tumor angiogenesis[17]. These discoveries have provided theoretical basis for anti-angiogenesis-targeted therapy for malignant tumors.
In recent years, anti-angiogenesis-targeted therapies have been identified as a promising therapeutic strategy. Some newly-developed agents that target the VEGF sig-naling pathway, such as the small-molecular VEGF re-ceptor inhibitors, sorafenib and sunitinib, and the anti-VEGF monoclonal antibody bevacizumab, have shown encouraging treatment benefits in advanced RCC patients in some randomized controlled trials[18–20]. IFN, which is often used as the standard comparator for the assessment of new treatments in mRCC, however, has not offered advantages in clinical benefits to the patients with mRCC[19, 21]. Thus, in this study, we performed the randomized controlled trials (RCTs)-based review and used meta-analysis to evaluate the effectiveness and safety of the VEGF-targeted drugs (sorafenib, sunitinib and bevacizumab) in the treatment of mRCC. 1 MATERIALS AND METHODS 1.1 Inclusion Criteria
RCTs that evaluated the clinical efficacy of the anti-angiogenesis agents targeting VEGF pathway were included. Case reports, cohort studies and case series were excluded from this study. There was no limitation to the country of research, but the language of publica-tion was confined to English.
The subjects in all the reviewed studies were pa-tients aged more than 18 years who were diagnosed as having advanced RCC, and had a component of clear cell histology and no previous exposure to VEGF pathway inhibitors.
Therapy regimens involved sorafenib, sunitinib and bevacizumab, with IFN or placebo serving as a com-parator.
Outcome measures consisted of ORR (complete re-sponse plus partial response), clinical benefit rate (ORR plus stable disease rate), progression-free survival (PFS) and adverse events (AEs). 1.2 Search Strategy
RCTs were identified by a comprehensive search of citations from the databases Medline, Embase, Web of Science and the Cochrane Library and Embase, by using the keywords “sorafenib”, “sunitinib”, “bevaci-zumab” and “renal cell carcinoma”. The text terms “vascular endothelial growth factor”, “targeted therapy” were also used to identify relevant information. Ab-stracts and meeting presentations from the American Society of Clinical Oncology (ASCO) conferences were also searched for relevant RCTs. We screened articles initially by titles and abstracts to identify the relevant studies. After exclusion of irrelevant articles and identi-
fications of duplicates from different databases, we evaluated the remaining articles in full text in terms of inclusion criteria and finally identified the eligible pub-lications. 1.3 Data Extraction
In order to prevent bias and improve reliability, data of characteristics and clinical response of each selected study were extracted independently and brought into a standardized form by two reviewers, including informa-tion on study design, participants, interventions and out-come measures. All disagreements were resolved by discussion to reach consensus among the investigators. 1.4 Assessment of Study Quality
Study quality was assessed in duplicate by two re-viewers according to the Jadad scoring method. The validated scale allows assessment of the methodological quality of each trial by quantifying the study’s randomi-zation, blinding methods, and description of patient withdrawals and dropouts, resulting in a total score of 0–5, with a score 0–2 indicating a study with poor qual-ity and a score 3–5 indicating a study with good qual-ity[22]. Additionally, the level of evidence for each study was identified according to the modified GRADE quality assessment criteria developed by the GRADE Working Group. The quality of evidence of the reviewed studies was rated on a 4-degree scale: high, moderate, low and very low levels[23]. 1.5 Statistical Analysis
Clinical variability was determined through evalua-tion of intervention differences among all studies. Meta-analysis was used to perform a quantitative data synthesis in studies that were comparable. Otherwise a narrative synthesis approach was chosen. For the meta-analysis, two different approaches were used: a fixed-effect model and a random-effect model, under the assumption of homogeneity and heterogeneity between studies, respectively. Assessment of the heterogeneity among all studies was performed with the Chi-square based Q test. In the analysis of pooled data, risk ratio (RR) was calculated by using 95% confidence interval (95% CI). Forest plots were used for graphic representa-tion of data. The vertical lines in our plots positioned at 1 (RR=1), represent equivalence in efficacy between the intervention and control treatments. The RRs were sig-nificant when the value 1 was not within the 95% CI.
All data analyses were performed by using Review Manager Software (version 5.0, the Cochrane Collabora-tion, UK). A two-tail P value less than 0.05 was consid-ered statistically significant in all tests. 2 RESULTS 2.1 Study Characteristics
A total of seven RCTs on VEGF pathway-targeted therapy for mRCC met the inclusion criteria, with a total of 3 451 patients included. Of the seven RCTs, three in-volved sorafenib[18, 24, 25], one sunitinib[19] and three bevacizumab[20, 26, 27]. IFN or placebo served as a com-parator for the 7 studies. There were phase Ⅱ trials in 3 RCTs[20, 24, 25], and phase Ⅲ trials in 4 RCTs[18, 19, 26, 27]. Although all included studies were RCTs, only two stud-ies had randomization procedure in detail. One study used centrally allocation via a telephone randomization

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
801
system[24], and the other utilized the interactive voice recognition system[27]. Six studies employed a stratified random block design and an intention-to-treat analysis approach[18–20, 25–27]. The information on blinding in pro-tocols was available in five RCTs[18–20, 25, 27]. Baseline characteristics were comparable between treatment and control groups in every RCT. Investigators in the most studies assessed tumor response rates [complete response (CR), partial response (PR), stable disease (SD), pro-
gressive disease (PD)] according to the Response Evaluation Criteria in Solid Tumors (RECIST)[28]. All the 7 studies had PFS data after targeted therapy, and only two reported the results of OS[18, 29]. The data of the other studies for OS were immature. All the 7 RCTs had good methodological quality which was evaluated according to the Jadad scoring method (table 1). According to the modified GRADE quality assessment criteria, the quality of evidence for all included studies was high (table 1).
Table 1 Study characteristics and quality of the included trials
†RDT: Randomized discontinuation trial is also a controlled trial with randomization. SOR: Sorafenib; SUN: Sunitinib; BEV: Bevacizumab; IFN: Interferon; RCT: Randomized controlled trial; PFS: Progression-free survival; OS: Overall survival; RR: Re-sponse rate; ORR: Overall response rate; PD: Progressive disease; LOE: Level of evidence
2.2 Overall Analysis
The outcomes of the RCTs were shown in detail in table 2. Results of meta-analysis showed patients in dif-ferent treatment arms of studies experienced lower risk of PD and improved PFS as compared with control arms (fig. 1), suggesting that VEGF pathway-targeted therapy
for mRCC is more effective in inhibiting tumor progress. Analyses of tumor response rate in different arms of tri-als also showed anti-VEGF agents produced superior ORR and offered substantial clinical benefits to patients with mRCC, although no pooled data were available due to heterogeneity of interventions (fig. 2 and 3).
Table 2 Outcomes of the included RCTs
Regimens Median PFS (months) Median ORR (%) Clinical benefit rate (%) Median OS (months) SOR vs. Placebo Escudier B, 2007 5.5 vs. 2.8† 9.8 vs. 1.8 83.6 vs. 54.6 17.8 vs. 14.3† Ratain MJ, 2006 5.6 vs. 1.4† NR NR NR
SOR vs. IFN Escudier B, 2009 5.7 vs. 5.6 5.2 vs. 8.7 79.4 vs. 64.1† NR
SUN vs. IFN Motzer RJ, 2007 11 vs. 5† 31 vs. 6† 79.0 vs. 55.0 26.4 vs. 21.8
BEV+IFN vs. IFN Rini BI, 2008 8.5 vs. 5.2† 25.5 vs. 13.1† NR NR Escudier B, 2007 10.2 vs. 5.4† 31 vs. 13† 77.5 vs. 62.6 NR
BEV vs. Placebo Yang JC, 2003 4.8 vs. 2.5† 10 vs. 0 NR ND‡
†P<0.05 for all comparisons between the treatment and control groups in the included RCTs; ‡P>0.2 for all comparisons of OS be-tween groups in Yang study. NR: Not reported; ND: Not detailed 2.3 Sorafenib Studies
Three studies evaluated the effectiveness of soraf-enib treatment for mRCC. Two of them were pla-cebo-controlled trials, and one study was conducted to evaluate the effectiveness of sorafenib versus that of IFNα-2a. 2.3.1 PFS and OS The Escudier study[18] reported that the median PFS was 5.5 months in the sorafenib group and 2.8 months in the placebo group (P<0.001), and sorafenib was associated with a 56% reduction in the risk of progression [hazard ratio (HR)=0.44; 95% CI: 0.35 to 0.55)]. Ratain et al[24] reported the median PFS was sig-nificantly longer with sorafenib than with placebo (24 vs.
6 weeks, respectively; P=0.0087). The data of the PD rates from the above two studies (heterogeneity P=0.008) showed a RR of 0.45 (95% CI: 0.24–0.83) and were highly statistically significant (P=0.01) in favor of the sorafenib treatment group (fig. 1). Escudier et al[25] re-ported the median PFS was similar between soraf-enib-treated and IFN-treated groups (5.7 months and 5.6 months, P=0.50). Only the Escudier study[18, 30] reported the final OS data which showed that treatment with sorafenib was associated with an improved survival com-pared with placebo (17.8 vs. 14.3 months, respectively; HR=0.78; 95% CI: 0.62 to 0.97; P=0.0287).
Drugs No. of patients Median age Author Year Phase
Treatment Control
Study
design Treatment Control Treatment control
Outcome
measure
Jadad
score LOE
Escudier B 2007 Ⅲ SOR Placebo RCT 451 452 58 59 PFS, RR, OS 5 High
Ratain MJ 2006 Ⅱ SOR Placebo RDT† 32 33 58 60 PFS, RR 4 High
Escudier B 2009 Ⅱ SOR IFN RCT 97 92 62 62.5 PFS, RR 5 High
Motzer RJ 2007 Ⅲ SUN IFN RCT 375 375 62 59 PFS, RR , OS 5 High
Rini BI 2008 Ⅲ BEV+IFN IFN RCT 369 363 61 62 PFS, ORR, PD 3 High
Escudier B 2007 Ⅲ BEV+IFN IFN RCT 327 322 61 60 PFS, RR , OS 5 High
Yang JC 2003 Ⅱ BEV Placebo RCT 76 40 53&54 53 PFS, RR 5 High

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
802
Fig. 1 Meta-analysis of progressive disease in different arms of studies
A random effect model is used. Trials to the left of the vertical line in the plot showed a reduction in risk of tumor progress with the intervention treatment.
Fig. 2 Clinical benefit rate analysis in different treatment arms of trials No meta-analysis was performed due to heterogeneity of interventions. All risk ratios >1.0 indicated a clinical benefit of the intervention treatment.
Fig. 3 ORR analyses in different treatment arms of trials
No meta-analysis was performed due to heterogeneity of interventions. Most risk ratios >1.0 favored VEGF-targeted therapy, although there was no significant difference between sorafenib and IFN.
2.3.2 Response Rates (ORR and Clinical Benefit Rate) Escudier et al[18] reported that overall responses and clinical benefits occurred in more patients in the soraf-
enib group than in the placebo group (overall response: 9.8% vs. 1.8%, P<0.001) (clinical benefit: 83.6% vs. 54.6%, P<0.001). Another study[25] showed soraf-

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
803
enib-treated patients had a significantly higher clinical benefit rate than those who received IFN (79.4% vs. 64.1%, P=0.006), but sorafenib group had a lower ORR than IFN group (5.2% vs. 8.7%). The data of ORR and clinical benefit rate weren’t pooled because of the clini-cal heterogeneity of the above studies. The individual group data of responses for therapy were not available in the Ratain study[24]. 2.4 Sunitinib Studies
One RCT[19] was conducted to assess the efficacy of sunitinib in mRCC, and it reported the results of PFS, OS and tumor response rates. 2.4.1 PFS and OS The median PFS was significantly longer in the sunitinib group than in the IFN group (11 vs. 5 months, respectively), corresponding to a HR of 0.42 (95% CI: 0.32 to 0.54; P<0.001). Updated results of this study presented at the 2008 ASCO annual meeting showed the median OS of patients treated with sunitinib and IFN were 26.4 months versus 21.8 months (P=0.051), respectively[29]. 2.4.2 Response Rates (ORR and Clinical Benefit Rate) Sunitinib treatment was associated with a higher ORR assessed by independent review than IFN (31% vs. 6%, respectively; P<0.001), and the updated ORR was 47% for sunitinib versus 12% for IFN (P<0.000001)[29]. As-sessed by blinded central review of imaging study, treatment with sunitinib was associated with higher clinical benefit rate than that with IFN (79% vs. 55%, respectively), due to the bulk proportion of patients with SD in sunitinib and IFN groups (48% vs. 49%, respec-tively). 2.5 Studies Relevant to Bevacizumab
Three studies evaluated the efficacy of bevacizumab treatment for mRCC. One RCT was placebo-controlled trial, and two RCTs were conducted to assess the effec-tiveness of bevacizumab plus IFN combination therapy. 2.5.1 PFS and OS The Rini study[26] reported that the median PFS was longer in the bevacizumab plus IFN group than in the IFN monotherapy group (8.5 months vs. 5.2 months, respectively; P<0.0001), and bevacizumab plus IFN treatment was associated with a 29% reduction in the risk of progression (HR=0.71; 95% CI: 0.61 to 0.83; P<0.0001). Escudier et al[27] reported the median duration of PFS was significantly longer in the bevaci-zumab plus IFN group than that in the IFN monotherapy group (10.2 vs. 5.4 months; HR=0.63, 95% CI: 0.52–0.75; P=0.0001). By using a random effect model to combine these PD rate data of the above two studies (heterogeneity P=0.09), the test for overall effectiveness was significantly in favor of the bevacizumab plus IFN combination regimen (RR=0.86, 95% CI: 0.76–0.97; P=0.01; fig. 1). By using a fixed effect model, bevaci-zumab plus IFN therapy was still favored. Yang et al[20] reported that the time to PD was significantly prolonged in the high-dose bevacizumab group as compared with that in the placebo group (4.8 vs. 2.5 months; HR=2.55, P<0.001), and borderline significant difference was found in the time to PD between the low-dose bevacizu-mab group and the placebo group (3.0 vs. 2.5 months; HR=1.26, P=0.053).
At the last analysis in the Yang study, there were no significant differences in OS between groups (high-dose/low-dose bevacizumab and placebo groups,
P>0.20 for all comparisons)[20]. 2.5.2 Response rates (ORR and Clinical Benefit Rate) As reported in the Escudier study[27], ORR was signifi-cantly higher in the bevacizumab plus IFN arm than in the IFN arm (31% vs. 13%, respectively; P=0.0001). Due to the bulk population of patients with SD in bevacizu-mab plus IFN and IFN groups (46% vs. 50%), clinical benefit rates were high in both groups (77% vs. 63%, respectively). Similarly, the Rini study[26] also showed that bevacizumab plus IFN group had a higher ORR than IFN group (25.5% vs. 13.1%, respectively; P<0.0001), and the detailed data of the clinical benefit rate and SD were not reported. Pooling the ORR data in a meta-analysis showed bevacizumab plus INF combina-tion regimen was statistically favored in terms of overall effect (RR=2.19, 95% CI: 1.72–2.78; P<0.00001; fig. 4). Yang et al[20] just reported four patients with mRCC in high-dose bevacizumab group had objective responses and the tumor response rate was 10%. 2.6 AEs
All studies reported the drug-related AEs in detail. AEs were defined and graded according to the National Cancer Institute Common Terminology Criteria for Ad-verse Events (CTCAE version 3.0), which included grade 1–5 (table 3)[31].
The treatment-emergent AEs attributed to sorafenib were predominantly of grade 1 or 2, and the most com-mon events were diarrhea, rash, fatigue, and nausea. Se-rious AEs (grade 3/4) occurring in sorafenib treatment arms were reported similarly common in the Escudier[18] and Ratain[24] studies (34% vs. 31%, respectively). Pro-portions of drug-related AEs overall (and grade 3/4) were fairly similar in the sorafenib and IFN treatment groups: 94.8% (41.2%) and 88.9% (35.6%), respectively[25]. The most frequent sorafenib-related serious AEs were hand-foot syndrome and hypertension. The above-men-tioned toxic effects were managed successfully using some medical interventions (antihypertensive and der-matologic), as thus sorafenib was generally well toler-ated.
Motzer et al[19] reported most AEs occurring during treatment in sunitinib and IFN groups were also in grade 1 or 2, and the patients with AEs in grade 3/4 were rela-tively less in both groups, but most general AEs of all grades occurred more frequently in the sunitinib group than in the IFN group. The most common AEs with sunitinib were fatigue, diarrhea, vomiting, hypertension, and hand-foot syndrome. Most treatment-emergent AEs in sunitinib and IFN groups were ameliorated by discon-tinuity of the agents (38% vs. 32%, respectively) or re-duction (32% vs. 21%, respectively) of the dose.
Primary studies[20, 32] reported that the bevacizu-mab-related AEs were minimal, with the most common and substantial events being hypertension and asympto-matic proteinuria, which would be decreased after the cessation of therapy. Bevacizumab was also generally well-tolerated with no life-threatening toxic effects. However, an increase in bevacizumab-related toxicities was observed in the bevacizumab plus IFN combination treatment group. Grade 3 and 4 AEs in patients receiving bevacizumab plus IFN and IFN monotherapy were re-ported in the Rini (79% vs. 61%, respectively; P<0.0001)[26] and Escudier (60.2% vs. 45.1%, respec-

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
804
tively)[27] studies, and combining these data of the two studies showed bevacizumab plus IFN combination regimen was highly associated with an increase of 31%
in the risk of serious toxic effects (RR=1.31, 95% CI: 1.20–1.43, P<0.00001; fig. 5).
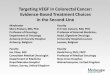
Fig. 4 Meta-analysis of ORR in bevacizumab+IFN treatment trials
A fixed effect model is used. The pooled RR significantly favored bevacizumab plus INF treatment.
Table 3 The grades of AEs according to the NCI CTCAE Descriptions for AEs
Grade 1 Mild: asymptomatic or minimal symptoms and intervention not indicated Grade 2 Moderate: symptoms not interfering with ADL or causing difficulty performing some ADL, intervention
not indicated or indicated for <24 h
Grade 3 Severe: symptoms interfering with ADL and intervention indicated for ≥24 h or even hospitalization
Grade 4 Life-threatening or disabling Grade 5 Death AE: Adverse event; ADL: Activities of daily living; NCI CTCAE: National Cancer Institute Common Terminology Criteria for Adverse Events Version 3.0
Fig. 5 Meta-analysis of grade 3/4 AEs in bevacizumab+IFN treatment trials A fixed effect model is used. Bevacizumab+IFN treatment showed an increase of 31% in the risk of serious toxic effects. 3 DISCUSSION
The current results of this systematic review showed that anti-VEGF agents could significantly prolong PFS and offer important clinical benefits to patients with mRCC, and among them, sunitinib was a relatively ef-fective agent with an updated ORR of 47%. Moreover, it was encouraging that bevacizumab plus IFN combina-tion therapy in patients with mRCC produced more clinical therapeutic benefits than IFN monotherapy. However, the combination regimen was also associated with increased toxic effects. As the gold standard on judging new agents, OS is an important assessment indi-cator as the primary endpoint of RCTs[33]. In this study, OS in most included RCTs is immature or not reported, and thus results on OS in mRCC are inconclusive.
Sorafenib is a small molecular inhibitor of VEGF and its receptors, and was approved by the Food and Drug Administration as monotherapy for advanced RCC in December 2005[34, 35]. Sorafenib-treated patients ex-perienced an ORR of less than 10%. Moreover, the me-dian PFS in sorafenib-treated arm was similar to that of
IFN-treated arm and ranged from 5.5 to 5.7 months. The reason for the unsatisfactory clinical effectiveness of sorafenib versus IFN in the included trials is not entirely clear at present. We speculated that it might result from the weaker inhibition of VEGF receptor in sorafenib than in sunitinib[34]. However, sorafenib therapy demonstrated an improved OS according to the result of secondary OS analysis censoring placebo patients. These contradictory results would make clinicians more hesitant in selecting sorafenib as the first-line treatment for advanced RCC.
Sunitinib is a small-molecule inhibitor of the tyro-sine-kinase portion of the VEGF family and its receptors, and was approved by the Food and Drug Administration as monotherapy for advanced RCC in January 2006[36]. In two sequential phase Ⅱ trials [37, 38], sunitinib resulted in an ORR of 45% in cytokine-refractory patients with mRCC, which was similar to the updated ORR of 47% reported in the Motzer study[19]. Among the VEGF-tar-geted agents, sunitinib produced the best ORR in mono-therapy for mRCC. The longer median OS in sunit-inib-treated group (26.4 months) than that in the previous trials (13 months)[39] indicated sunitinib treatment had extended the lives of patients with mRCC. All data of

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
805
superior PFS, ORR and OS in patients undoubtedly made sunitinib selected as first-line treatment for mRCC[40].
Bevacizumab is a monoclonal antibody that binds and neutralizes circulating VEGF protein but does not affect the VEGF receptor[41]. The effectiveness of this drug in mRCC was initially identified in a phase Ⅱ trial in 2003. Subsequently, another phase Ⅱ trial showed a trend toward improved median PFS (8.5 months) and ORR (13%) with bevacizumab monotherapy[42]. Fur-thermore, the results of our study showed that bevacizu-mab plus IFN produced a superior PFS and ORR in pa-tients with mRCC over IFN monotherapy, but the risk of toxic effects was increased by 31%. However, the con-tribution of IFN to the anti-tumor effect of this combina-tion regimen is unclear at present. More importantly, the risk to benefit ratio for each patient with bevacizumab plus IFN combination therapy should be assessed, al-though this regimen was recommended as first-line ther-apy for patients with advanced RCC by the NCCN kid-ney cancer panel members[40].
It is interesting to note in table 2 that indirectly compared with bevacizumab monotherapy, bevacizumab plus IFN produced a similar encouraging ORR of 31% as sunitinib in patients with untreated RCC, which was as-sociated with more clinical benefits. However, another study showed there was no improved clinical outcome with the addition of erlotinib to bevacizumab[42]. Ac-cording to the results of the current review, we seemed to be bewildered by selecting monotherapy or combination therapy for patients with mRCC. Additional clinical trials should be conducted to define the efficacy and safety of monotherapy and combination therapy for mRCC.
We excluded some clinical trials without control group as establishing control group is crucial for evalua-tion of clinical outcomes. There were some limitations in our study. The number of included studies was less, al-though all of them were high-quality clinical trials. Moreover, a language bias in selecting RCTs published only in English may exist. Unfortunately, this meta-analysis was unable to demonstrate an improved OS in patients with VEGF-targeted therapy as mature OS data, thus far are awaited from the most included studies.
In conclusion, our study demonstrated that anti-VEGF agents offered improved PFS and substantial clinical benefits to patients with mRCC. The goal of mRCC treatment is to maximize overall clinical thera-peutic benefit, which means extending OS for every pa-tient while maximizing their quality of life[43]. For this goal, additional clinical trials concerning the efficacy versus toxicity profile of each VEGF-targeted agent for mRCC should be further explored for the choice of the treatment with the best optimal risk to benefit ratio for each patient with this challenging disease.
REFERENCES 1 Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA
Cancer J Clin, 2010,60(5):277-300 2 Kovacs G, Akhtar M, Beckwith BJ, et al. The Heidelberg
classification of renal cell tumours. J Pathol, 1997,183(2): 131-133
3 Karumanchi SA, Merchan J, Sukhatme VP. Renal cancer: molecular mechanisms and newer therapeutic options.
Curr Opin Nephrol Hypertens, 2002,11(1):37- 42 4 Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008.
CA Cancer J Clin, 2008,58(2):71-96 5 Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009.
CA Cancer J Clin, 2009,59(4):225-249 6 Ljungberg B, Cowan NC, Hanbury DC, et al. EAU
guidelines on renal cell carcinoma: the 2010 update. Eur Urol, 2010,58(3):398-406
7 Rouviere O, Bouvier R, Negrier S, et al. Nonmetastatic renal-cell carcinoma: is it really possible to define ra-tional guidelines for post-treatment follow-up. Nat Clin Pract Oncol, 2006,3(4):200-213
8 Motzer RJ, Bander NH, Nanus DM. Renal-cell carcinoma. N Engl J Med, 1996,335(12):865-875
9 Amato RJ. Renal cell carcinoma: review of novel sin-gle-agent therapeutics and combination regimens. Ann Oncol, 2005,16(1):7-15
10 Linehan WM, Zbar B. Focus on kidney cancer. Cancer Cell, 2004,6(3):223-228
11 Medical Research Council Renal Cancer Collaborators. Interferon-alpha and survival in metastatic renal carci-noma: early results of a randomised controlled trial. Lan-cet, 1999,353(9146):14-17
12 Motzer RJ, Bacik J, Murphy BA, et al. Interferon-alfa as a comparative treatment for clinical trials of new thera-pies against advanced renal cell carcinoma. J Clin Oncol, 2002,20(1):289-296
13 Motzer RJ, Murphy BA, Bacik J, et al. Phase Ⅲ trial of interferon alfa-2a with or without 13-cis-retinoic acid for patients with advanced renal cell carcinoma. J Clin Oncol, 2000,18(16):2972-2980
14 Gnarra JR, Tory K, Weng Y, et al. Mutations of the VHL tumor suppressor gene in renal carcinoma. Nat Genet, 1994,7(1):85-90
15 Wiesener MS, Munchenhagen PM, Berger I, et al. Con-stitutive activation of hypoxia-inducible genes related to overexpression of hypoxia-inducible factor-1alpha in clear cell renal carcinomas. Cancer Res, 2001,61(13): 5215-5222
16 Rini BI, Small EJ. Biology and clinical development of vascular endothelial growth factor-targeted therapy in re-nal cell carcinoma. J Clin Oncol, 2005,23(5):1028-1043
17 Dvorak HF. Vascular permeability factor/vascular endo-thelial growth factor: a critical cytokine in tumor angio-genesis and a potential target for diagnosis and therapy. J Clin Oncol, 2002,20(21):4368-4380
18 Escudier B, Eisen T, Stadler WM, et al. Sorafenib in ad-vanced clear-cell renal-cell carcinoma. N Engl J Med, 2007,356(2):125-134
19 Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med, 2007,356(2):115-124
20 Yang JC, Haworth L, Sherry RM, et al. A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N Engl J Med, 2003,349(5):427-434
21 Szczylik CD, Demkow T, Staehler M, et al. Randomized phase Ⅱ trial of first-line treatment with sorafenib versus interferon in patients with advanced renal cell carcinoma: Final results. J Clin Oncol (Meeting Abstracts), 2007,25:5025
22 Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding

J Huazhong Univ Sci Technol[Med Sci] 31(6):2011
806
necessary. Control Clin Trials, 1996,17(1):1-12 23 Atkins D, Briss PA, Eccles M, et al. Systems for grading
the quality of evidence and the strength of recommenda-tions Ⅱ: pilot study of a new system. BMC Health Serv Res, 2005,5(1):25
24 Ratain MJ, Eisen T, Stadler WM, et al. PhaseⅡ pla-cebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma. J Clin Oncol, 2006,24(16):2505-2512
25 Escudier B, Szczylik C, Hutson TE, et al. Randomized phase Ⅱ trial of first-line treatment with sorafenib versus interferon Alfa-2a in patients with metastatic renal cell carcinoma. J Clin Oncol, 2009,27(8):1280-1289
26 Rini BI, Halabi S, Rosenberg JE, et al. Bevacizumab plus interferon alfa compared with interferon alfa monother-apy in patients with metastatic renal cell carcinoma: CALGB 90206. J Clin Oncol, 2008,26(33):5422-5428
27 Escudier B, Pluzanska A, Koralewski P, et al. Bevacizu-mab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase Ⅲ trial. Lancet, 2007,370(9605):2103-2111
28 Therasse P, Arbuck SG, Eisenhauer EA, et al. New guide-lines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst, 2000,92(3):205-216
29 Figlin RA, Hutson TE, Tomczak P, et al. Overall survival with sunitinib versus interferon (IFN)-alpha as first-line treatment of metastatic renal cell carcinoma (mRCC). J Clin Oncol (Meeting Abstracts), 2008,26:5024
30 Escudier B, Eisen T, Stadler WM, et al. Sorafenib for treatment of renal cell carcinoma: Final efficacy and safety results of the phase Ⅲ treatment approaches in re-nal cancer global evaluation trial. J Clin Oncol, 2009, 27(20):3312-3318
31 National Cancer Institute. Common terminology criteria for adverse events (version 3). 2003. http://ctep.cancer. gov/protocolDevelopment/electronic_applications/docs/ ctcaev3.pdf.(accessed Mar 16, 2009).
32 Yang JC. Bevacizumab for patients with metastatic renal cancer: an update. Clin Cancer Res, 2004,10(18): 6367S-6370S
33 Rini BI. Vascular endothelial growth factor-targeted therapy in renal cell carcinoma: current status and future directions. Clin Cancer Res, 2007,13(4):1098-1106
34 Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 ex-hibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res, 2004, 64(19):7099-7109
35 Kane RC, Farrell AT, Saber H, et al. Sorafenib for the treatment of advanced renal cell carcinoma. Clin Cancer Res, 2006,12(24):7271-7278
36 Mendel DB, Laird AD, Xin X, et al. In vivo anti-tumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and plate-let-derived growth factor receptors: determination of a pharmacokinetic/pharmacodynamic relationship. Clin Cancer Res, 2003,9(1):327-337
37 Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA, 2006,295(21):2516-2524
38 Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endo-thelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell car-cinoma. J Clin Oncol, 2006,24(1):16-24
39 Coppin C, Porzsolt F, Awa A, et al. Immunotherapy for advanced renal cell cancer. Cochrane Database Syst Rev, 2005,25(1):CD001425
40 NCCN. NCCN Clinical Practice Guidelines in Oncol-ogyTM. Kidney Cancer Version 2. 2009. http://www. nccn.org/professionals/physician_gls/PDF/kidn ey.pdf (ac-cessed Mar 16, 2009).
41 Presta LG, Chen H, O'Connor SJ, et al. Humanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disor-ders. Cancer Res, 1997,57(20):4593-4599
42 Bukowski RM, Kabbinavar FF, Figlin RA, et al. Ran-domized phase Ⅱ study of erlotinib combined with bevacizumab compared with bevacizumab alone in me-tastatic renal cell cancer. J Clin Oncol, 2007,25(29): 4536-4541
43 Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet, 2009,373(9669):1119-1132
(Received Feb. 21, 2011)