Embed Size (px)
Citation preview

1
Immunotherapy in GU Cancers
Dr Ravindran Kanesvaran
Medical Oncologist
National Cancer Centre Singapore

2
Disclosures
• Speaker Bureau: Pfizer, J&J, Sanofi, Novartis,
MSD
• Advisory Board/ Consultant: GSK, Novartis,
Bayer, J&J, Mundipharma, Astellas, MSD, BMS
• Research support: Sanofi, J&J, Astellas

3
Outline
• Introduction
• Immunotherapy in mBC
• Immunotherapy in mRCC
• Summary

4
Bladder and Kidney Cancers Singapore
Singapore Cancer Registry Interim Annual Report Trends in Cancer Incidence in Singapore 2010-2014

5
Metastatic Bladder Cancer
• Approximately 25% of patients will have muscle-invasive disease
and either present with or later develop metastases

6
Current Treatment : Chemotherapy

7
Current first line treatment

8
Carboplatin in patients “unfit” for
cisplatin
• Data suggests that CDDP > carbo in terms of efficacy
– MA Galsky Annals 2011 : CDDP > Carbo wrt CR, ORR
– Multiple phase II studies reveal CDDP > Carbo in terms of ORR
• EORTC 30896 (ASCO 2010)
– G/Carbo vs M-CAVI (M, V and Carbo) in pts CCT 30-60, PS 2
– OS same (about 8.5 mths); G/Carbo better tolerated
• Definition of pts unfit for CDDP (Galsky, JCO June 2011)
– ECOG 2
– CCT < 60
– ≥ G2 hearing loss or ≥ G2 neuropathy
– NYHA III CCF

9
Current Treatment: Immunotherapy

10
Role of immune system in advanced bladder
cancer
Martincorena I, Campbell PJ. Science. 2015;349:1483-9
High mutational load may correlate with immunogenicity, and provides valuable prognostic information

11
IMvigor 210: Study Design
• Single-arm phase II study with 2 cohorts
Pts with inoperable
advanced or metastatic
UC, predominantly TCC
histology, evaluable
tumor tissue for
PD-L1 testing
Cohort 1
Previously untreated,
cisplatin ineligible
Cohort 2
Prior platinum
treatment
Atezolizumab
1200 mg IV Q3W
until PD
Atezolizumab
1200 mg IV Q3W
until loss of benefit
Rosenberg JE, et al. Lancet. 2016;387:1909-1920
Primary endpoints: confirmed ORR by RECIST v1.1 (per central review), ORR per immune-modified RECIST (per investigator)Secondary endpoints: DoR, PFS, OS, safety

12
Post platinum – Responses
• Responses seen in all PD-L1 IC subgroups; higher response seen with higher PD-L1 status
• After a median follow-up of 11·7 months, the median duration of response was not yet reached in
any of the PD-L1 subgroups (range 2·0–13·7 months)
• At the time of the updated data cutoff, ongoing responses were reported in 38 (84%) of the 45
responding patients
• The median time to response was 2·1 months (95% CI 2·0–2·2)

13
Post platinum – Conclusion
• Targeting PD-L1 with atezolizumab is effective in heavily pretreated
patients with locally advanced or metastatic urothelial carcinoma
• Responses were seen in all PD-L1 expression subgroups
• Higher response rates in patients with higher levels of PD-L1
expression on immune cells
• Data led to FDA accelerated approval of atezolizumab for advanced
or metastatic UC after PD during or following platinum-based
therapy

14
Cohort 1 (Previously untreated and
cisplatin ineligible)
• Many patients are cisplatin ineligible due to poor
performance status, impaired renal function, or
comorbidities
• Non-cisplatin–based regimens associated with short
response duration, lack of survival benefit, high
discontinuation rate
• Many patients do not end up receiving systemic
treatment

15
Cisplatin ineligible – Survival
• No clear difference in OS between PD-L1 subgroups
• Median OS was not reached in patients with no risk factors
• 13·4 months in patients with one risk factor (either visceral metastases or ECOG 2)
• 6·2 months in patients with two risk factors
• 19·1 months median OS reported in the stable disease subgroup

16
Cisplatin ineligible – Conclusion
• Durable responses to atezolizumab in previously untreated cisplatin-
ineligible patients metastatic urothelial carcinoma
– Responses seen in all PD-L1 subgroup
• Survival to date appears favourable
• Low incidence of AE despite numerous co-morbidities

17
Was the accelerated approval too early?

18
IMvigor211: A Phase III Randomized Study
Examining Atezolizumab
vs. Chemotherapy for Platinum-Treated
Advanced Urothelial Carcinoma
Thomas Powles,1 Yohann Loriot,2 Ignacio Durán,3 Alain Ravaud,4 Margitta M. Retz,5
Nicholas J. Vogelzang,6 Sanjeev Mariathasan,7 Na Cui,7 Christina L. Derleth,7
Michiel S. van der Heijden8
1Barts Cancer Institute ECMC, Barts Health and the Royal Free NHS Trust, Queen Mary University of London,
London, UK; 2Département de Médecine Oncologique, Université Paris-Saclay
and Gustave Roussy, Villejuif, France; 3Department of Medical Oncology, Hospital Universitario Virgen del Rocío
and Institute of Biomedicine of Seville, Seville, Spain; 4Hôpital Saint-André CHU and Department of Medical
Oncology, Bordeaux University Hospital, Bordeaux, France; 5Department of Urology, Klinikum Rechts der Isar,
Technical University Munich, Munich, Germany; 6US Oncology Research, Comprehensive Cancer Centers of
Nevada, Las Vegas, Nevada, USA; 7Genentech, Inc., South San Francisco, CA, USA; 8Department of Medical
Oncology, Netherlands Cancer Institute, Amsterdam, Netherlands
Powles T, et al. EAS 2017, IMvigor211.

19
Key Eligibility Criteria• mUC with progression during or following
platinum-based chemotherapy– ≤ 2 prior lines of therapy
• Measurable disease per RECIST v1.1• ECOG PS 0-1• Evaluable sample for PD-L1 testing• TCC histology as primary component
(N = 931)
IMvigor211 Study Design
▪ Primary endpoint
▪ OS, tested hierarchically
in pre-specified populations
19
Atezolizumab 1200 mg q3w
R1:1
No crossover permitted per protocol
Survival follow-up
Loss of clinical benefit
RECIST v1.1
progression
Stratification Factors• No. of risk factorsa (0 vs. 1/2/3)• Liver metastases (yes vs. no)• PD-L1 status (0/1 vs. 2/3)• Chemotherapy (vinflunine vs. taxanes)
▪ Additional endpoints
▪ Efficacy: RECIST v1.1 ORR, PFS and DOR
▪ Safety
▪ PROs: EORTC QLQ-C30
Chemotherapy (investigator’s choice)
• Vinflunine q3w• Docetaxel q3w• Paclitaxel q3w
aDefined by time from prior chemotherapy < 3 mo, ECOG performance status > 0 and hemoglobin < 10 g/dL.

20
OS Analysis: IC2/3 Population
20
HR = 0.87 (95% CI: 0.63, 1.21)
P = 0.41
Events/Patients
Median OS(95% CI)
12-mo OS Rate(95% CI)
Atezolizumab 72/116 11.1 mo (8.6, 15.5) 46% (37, 56)
Chemotherapy 88/118 10.6 mo (8.4, 12.2) 41% (32, 50)
No. at Risk
Atezolizumab 116 100 85 77 71 58 51 39 27 19 11 6 0
Chemotherapy 118 100 91 82 71 61 47 32 24 15 9 5 1
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Ove
rall
Surv
ival
100
Months

21
OS Analysis: ITT Population
Events/Patients
Median OS(95% CI)
12-mo OS Rate(95% CI)
Atezolizumab 324/467 8.6 mo (7.8, 9.6) 39% (35, 44)
Chemotherapy 350/464 8.0 mo (7.2, 8.6) 32% (28, 37)
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Ove
rall
Surv
ival
100
Months
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Ove
rall
Surv
ival
100
Months
HR = 0.85 (95% CI: 0.73, 0.99)
P = 0.038
No. at Risk
Atezolizumab 467 405 327 280 245 201 177 138 90 59 34 13 1
Chemotherapy 464 397 330 268 219 175 140 99 60 42 17 7 1

22
OS in Clinical and Treatment Subgroups
NE, not estimable. Unstratified hazard ratios are plotted. Dashed line refers to HR for ITT population.
1.0
Atezolizumab better Chemotherapy better
SubgroupPD-L1 status IC2/3
IC1/2/3
ITT
Tobacco use history Current
Previous
Never
ECOG PS 0
1
Primary tumor site Bladder
Urethra
Renal pelvis
Ureter
Liver metastases Yes
No
Lymph node–only metastases Yes
No
Chemotherapy stratification Taxane
Vinflunine
Atezolizumab mOS Chemotherapy mOS11.1 mo 10.6 mo
8.9 mo 8.2 mo
8.6 mo 8.0 mo
9.2 mo 6.7 mo
8.4 mo 8.2 mo
10.4 mo 8.1 mo
12.0 mo 10.1 mo
6.1 mo 6.4 mo
8.9 mo 7.7 mo
NE 12.5 mo
5.9 mo 8.5 mo
8.9 mo 8.1 mo
4.0 mo 5.2 mo
10.1 mo 9.7 mo
17.4 mo 12.2 mo
8.1 mo 7.2 mo
8.3 mo 7.5 mo
9.2 mo 8.3 mo

23
IMvigor211 – Conclusion
• The primary endpoint of OS was not met in the IC2/3 population
• Due to delayed separation of the Kaplan-Meier curves, the
differences in mOS and HR do not fully reflect the clinical activity
achieved with atezolizumab
• The safety data showed no new safety signals and demonstrated a
more favorable safety profile for atezolizumab than for
chemotherapy

24
Nivolumab in mBC

25
Overall Survival
• At a median follow-up of 7·00
months (IQR 2·96–8·77),
median OS was 8·74 months
(95% CI 6·05 to not reached)
in the overall population,
• Median OS 11·30 months
(8·74 to not reached) in the
subgroup of patients with PD-
L1 expression of > 1%
• Median OS 5·95 months
(4·30–8·08) in the subgroup
with PD-L1 expression of < 1%

26
Pembrolizumab K-045

27
Stratification Factors
• ECOG PS (0/2 vs 2)
• Hemoglobin level (<10 vs ≥10 g/dL)
• Liver metastases (yes vs no)
• Time from last chemotherapy dose (<3 vs ≥3
mo)
KEYNOTE-045: Study Design
Pembrolizumab
200 mg IV Q3W
For 2 years
Paclitaxel 175 g/m2 Q3W (n=84)
OR
Docetaxel 75 mg/m2 Q3W (n=84)
OR
Vinflunine 320 mg/m2 Q3W (n=87)
R (1:1)
N=542
Key End Points
Primary: OS and PFS in total and PD-L1 CPS ≥10% populations
Secondary: OR and DOR in total and PD-L1 CPS ≥10%
populations; safety in total population
n=270
n=272
Key Eligibility Criteria
• Urothelial carcinoma of the renal pelvis, ureter,
bladder, or urethra
• Transitional cell predominant
• PD after platinum-based chemo for advanced
disease or recurrence within 12 mo of
perioperative platinum-based therapy for
localized muscle-invasive disease
• ECOG PS 0-2
• Provision of tumor sample for biomarker
assessment
CPS = combined positive score; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; IV = intravenous; OS = overall survival; PD =
progressive disease; PD-L1 = programmed death ligand 1; PFS = progression-free survival; PS = performance status; Q3W – every 3 weeks; R = randomization.

28
† ECOG PS scores range from 0 to 5, with 0 indicating no symptoms and higher scores indicating greater disability.‡ PD-L1 CPS: the percentage of tumor and infiltrating immune cells with PD-L1 expression out of the total number of tumor cells.§Risk factors include the Bellmunt risk factors: ECOG PS score >0; hemoglobin concentration <10 g/dL; presence of liver metastases,2 plus time since the completion/discontinuation of previous therapy <3 mo.3
CPS = combined positive score; ECOG = Eastern Cooperative Oncology Group; PD-L1 = programmed death ligand 1; PS = performance status.
1. Bellmunt J, et al. N Engl J Med. 2017; February 17 [Epub ahead of print]; 2. Bellmunt J, et al. J Clin Oncol. 2010;28:1850-1855; 3. Sonpavde G, et al. Eur Urol. 2013;63:717-723.
KEYNOTE-045: Baseline Characteristics

29
CI = confidence interval; CPS = combined positive score
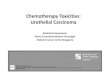
KEYNOTE-045: Overall Survival
• The median OS was 10.3 months (95% CI, 8.0 to 11.8) in the pembrolizumab group vs 7.4 months
(95% CI, 6.1 to 8.3) in the chemotherapy group
• In patients who had a tumor PD-L1 CPS of 10% or more, the median OS was 8.0 months (95%
CI, 5.0 to 12.3) in the pembrolizumab group vs 5.2 months (95% CI, 4.0 to 7.4) in the
chemotherapy group
Total Population CPS ≥10% Population

30
KEYNOTE-045: Overall Survival in Key
Subgroups

31
KEYNOTE-045: Conclusion
• Pembrolizumab significantly improved OS over chemotherapy in patients
with advanced urothelial carcinoma following first-line platinum-based
therapy: OS benefit observed in all PD-L1 populations
• No significant difference in PFS between pembrolizumab and chemotherapy
• ORR significantly higher and responses more durable with pembrolizumab
• Lower incidence of treatment-related AEs of any grade (60.9% vs 90.2%)
and grade 3-5 severity (15.0% vs 49.4%) with pembrolizumab
• Updated results after 22.5 mths follow-up remained consistenta
• Responses ongoing at data cutoff:– All patients: 57.9% in the pembrolizumab arm; 20.0% in the chemotherapy arm
– CPS ≥10: 73.3% in the pembrolizumab arm; 33.3% in the chemotherapy arm
aR de Wit, et al. ESMO Poster Presentation 2017

32
Pembrolizumab K-052

33
KEYNOTE-052: Study Design

34
KEYNOTE-052: Baseline Characteristics

35
KEYNOTE-052: Objective Responses
• Median time to response was 2 months

36
KEYNOTE-052: PFS
• Median PFS was 2 months (95% CI 2–3); 6 month PFS of 30% (25–35)
• 6 month OS was 67% (95% CI 62–73)

37
KEYNOTE-052: Conclusion
• First-line pembrolizumab demonstrated clinically meaningful
antitumor activity in cisplatin-ineligible patients with advanced
urothelial cancer
• No new safety signals were identified

38
Avelumab

39
Durvalumab

40
Summary of IO (2nd line) trials
Chism D. J Natl Compr Canc Netw 2017;15(10):1277–1284

41
Summary of cisplatin-ineligible first line trials
Chism D. J Natl Compr Canc Netw 2017;15(10):1277–1284

42
Comparing Toxicities between PD-1 and PD-L1
inhibitors
Pillai RN. Cancer 2017 Sep 28. doi: 10.1002/cncr.31043

43
Summary
• Chemotherapy still has an important role in the management of mBC
• We have 5 IO drugs with some data for use in mUC but only one with phase III trial data to support its use (Pembrolizumab)
• Biomarker studies seem to show a relationship but not clear
• Accelerated approval does not guarantee phase 3 trial success
• More IO drugs and combination trials are ongoing
• Cost will play a big role in its usage and access in non reimbursable markets

44
Outline
• Current standards
• Immunotherapy in mBC
• Immunotherapy in mRCC
• Summary

Rationale for Immunotherapy in RCC
• Spontaneous remissions attributed to the immune system of advanced RCC have been observed1
• RCC exhibits immune cell infiltrates, and several immune escape mechanisms have been reported in RCC2,3
• Historically, the mainstay of treatment for patients with mRCC was immunotherapy with interleukin-2 or interferon-α1
• Immuno-Oncology (I-O) is an evolving treatment modality encompassing agents designed to directly harness the patient’s own immune system to fight cancer7,8
Tregs CD45+ Memory T Cells CD8+ T Cells CD4+ T Cells
Studies have documented alterations in various immune cell types in RCC, including3-6:
levels: Poor
prognosis
levels: Fair/Poor prognosis
levels: Fair/Poor
prognosis/no association
levels: Fair/Poor prognosis
RCC=renal cell carcinoma; mRCC=metastatic renal cell carcinoma; Treg=regulatory T cell.1. Escudier B. Ann Oncol. 2012;23(Suppl 8):viii35-viii40 2. Noessner E et al. OncoImmunology. 2012;1(8):1451-1453. 3. Bockorny B et al. Expert Opin Biol Ther. 2013;13(6):911-925. 4. Hotta K, et al. Br J Cancer. 2011;105(8):1191-1196. 5. Nakano O et al. Cancer Res. 2001;61(13):5132-5136. 6. Igarashi T et al. Urol Int. 2002;69(1):51-56. 7. Ascierto PA et al. J Trans Med. 2014;12:141. doi: 10.1186/1479-5876-12-141. 8. Eggermont A et al. OncoImmunol. 2014;3(1):e27560.

46
NCCN 2017

47
Phase III, randomized, open-label trial of nivolumab vs everolimus in subjects with advanced or metastatic clear cell RCC who have received prior anti-angiogenic therapy
* Patients may continue treatment beyond progression (RECIST 1.1) if investigator-assessed clinical benefit is achieved and treatment is well tolerated.
Nivolumab3 mg/kg IV q2w Until progression*,
unacceptable toxicity, withdrawal of
consent, or end of trial
Key Inclusion Criteria▪ Advanced/metastatic clear cell RCC▪ No more than 3 total prior regimens in
advanced/metastatic setting▪ 1 or 2 prior anti-angiogenic therapy
regimens in advanced/metastatic setting▪ Karnofsky PS ≥70%; No CNS metastases▪ No prior therapy with mTOR inhibitor▪ No glucocorticoid use (equivalent to >10 mg
of prednisone daily)
R
1:1Everolimus10 mg PO qd
• Primary Outcome Measure: OS• Secondary Outcome Measures: PFS, ORR, DOR etc
N=821
Safety and Efficacy of Nivolumab for Metastatic Renal Cell Carcinoma: Real-World Data From an Italian Expanded Access Program
Key Inclusion Criteria
▪ ≥18 years with advanced or metastatic RCC
▪ ≥1 prior systemic treatment in the advanced or metastatic setting
▪ Patients with untreated CNS metastases or active autoimmune disease were excluded
N=389
Nivolumab3 mg/kg IV q2w
Until progression*, unacceptable toxicity, withdrawal of consent
• This analysis included all patients who received ≥1 dose of nivolumab
• AEs monitored and graded using the National Cancer Institute CTCAETerminology Criteria for Adverse Events v4.0
• ORR, PFS), and OS were evaluated
1. Motzer RJ et al. N Engl J Med. 2015. doi:10.1056/NEJMoa1510665.

Characteristic Nivolumab (N = 389)
Male, n (%) 291 (75)
Median age, years (range)≥75, n (%)
65 (34–85)70 (18)
ECOG PS, n (%)012NA
176 (45)174 (45)
24 (6)15 (4)
Histology, n (%)Clear cellNon-clear cellNA
356 (92)26 (7)7 (2)
Metastasis site, n (%)BoneLiverCNS
193 (50)128 (33)
32 (8)
Number of prior systemic therapies, n (%)
12≥3
80 (21)137 (35)170 (44)
NA = not available, percentages may not add to 100% due to rounding
Characteristic Nivolumab (N=410)
Everolimus(N=411)
Total ( N=821)
Male, n (%) 315 (77) 304 (74) 619 (75)
Median age, years (range) 62 (23–88) 62 (38–86) 62 (34–85)
Karnofsky performance status – no (%)
<70708090100
2(<1)22 (5)
110 (27)150 (17)126 (31)
1 (<1)30 (7)
116 (28)130 (32)134(33)
3 (<1)52 (6)24 (6)15 (4)
260 (12)
Disease sites that could be evaluated - no (%)1≥2
68 (17)341 (83)
71 (17)338 (82)
139 (17)679 (83)
Metastasis site, n (%)LungLiverBone
278 (68)100 (24)76 (19)
273 (66)87 (21)70 (17)
551 (67)187 (23)146 (18)
Number of prior systemic therapies, n (%)
SunitinibPazopanibAxitinib
246 (60)119 (29)51 (12)
242 (59)131 (32)50 (12)
488 (59)250 (30)101 (12)
Previous nephrectomy -no. (%)Yes No
364 (89)46 (11)
359 (87)52 (13)
723 (88)98 (12)
NA = not available, percentages may not add to 100% due to rounding
CheckMate 025
Baseline Patient Characteristics
Real-World Data

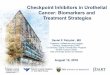
Overall Survival
Median OS at 2 years follow-up,
months (95% CI)
Nivolumab 26.0 (22.2–29.6)
Everolimus 19.7 (17.6–22.3)
HR (95% CI): 0.73 (0.61–0.88);
P=0.0006
• Median follow-up was 33.6 months
• Median OS was not reached
• With a (range: 1–17). 6-month and 9-month OS rates were 80% and 73%, respectively.
CheckMate 025 Real-World Data
Median follow-up of 9.2 months
1. Motzer RJ et al. N Engl J Med. 2015. doi:10.1056/NEJMoa1510665.

50
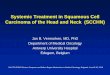
Progression-Free Survival
Median PFS, months (95% CI)
Nivolumab 4.6 (3.7–5.4)
Everolimus 4.4 (3.7–5.5)
HR=0.88 (95% CI, 0.75–1.03) P=0.11
No. of patients at riskNivolumab 410 230 145 116 81 66 48 29 11 4 0Everolimus 411 227 129 97 61 47 25 16 3 0 0
0 3 6 129 15
Months
18 21 24 27 30
0.0
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
gre
ssio
n-F
ree
Su
rviv
al (
Pro
bab
ility
)
Nivolumab
Everolimus
1. Motzer RJ et al. N Engl J Med. 2015.doi:10.1056/NEJMoa1510665.
• In an ad hoc sensitivity analysis of patients who had not progressed or died at 6 months, median PFS was 15.6 months for Nivolumab versus 11.7 months for Everolimus (HR=0.64; 95% CI, 0.47–0.88)1
• Median PFS was 4.6 months (95% CI: 3.6, 5.7;)
• 6-month and 9-month PFS rates were 44% and 35%, respectively
CheckMate 025 Real-World Data

51
Objective Response Rate
• Nivolumab was associated with a greater number of objective responses1
Nivolumab n=410
Everolimusn=411
Objective response rate, %1 26 5
Odds ratio (95% CI)6.13(3.77–9.95)
P<0.0001
Best overall response, %
Complete response
Partial response
Stable disease
Progressive disease
Not evaluated
1
25
34
35
6
<1
5
56
27
11
Median time to response, months (range)
3.5 (1.4–24.8) 3.7 (1.5–11.2)
Median duration of response, months (range)*
12.0 (0–36.8) 12.0 (0–33.0)
Ongoing response, n/N (%) 30/105 (29) 3/22 (14)
1. Motzer RJ et al. N Engl J Med. 2015. doi:10.1056/NEJMoa1510665.
Best response N = 389
ORR, n (%)
95% CI (%)
86/389 (22)
18, 26
Best objective response, n (%)
CR
PR
SD
PD
Not determined
2 (<1)
84 (22)
120 (31)
144 (37)
39 (10)
CR = complete response; PD = progressive disease
CheckMate 025 Real-World Data

52
Checkmate 025: Overall Survival by Number and Sites of Metastasis
SubgroupNivolumab
Events/patients, nEverolimus
Events/patients, n
No. of sites of metastasis
1 14/68 21/71
≥2 168/341 194/338
Bone metastases
Yes 42/76 45/70
No 141/334 170/341
Liver metastases
Yes 54/100 52/87
No 129/310 163/324
0 21
Nivolumab Everolimus
Favors
Motzer RJ et al. Oral presentation at ASCO GU 2016. 498.

53
Checkmate 025: Treatment-Related AEs in ≥15% of Patients
Nivolumabn=406
Everolimusn=397
Any grade Grade 3 Grade 4* Any grade Grade 3 Grade 4†
Treatment-related AEs1, % 79 19 1 88 33 4Fatigue 34 2 0 34 3 0Nausea 15 <1 0 17 1 0Pruritus 14 0 0 10 0 0Diarrhea 14 1 0 21 1 0Decreased appetite 12 <1 0 20 1 0Rash 10 <1 0 20 1 0Cough 9 0 0 19 0 0Anemia 8 2 0 24 8 1Dyspnea 7 1 0 13 <1 0Peripheral edema 4 0 0 14 <1 0Pneumonitis 4 1 <1 15 3 0Mucosal inflammation 3 0 0 19 3 0Dysgeusia 3 0 0 13 0 0Hyperglycemia 2 1 <1 12 3 <1Stomatitis 2 0 0 29 4 0Hypertriglyceridemia 1 0 0 16 4 1Epistaxis 1 0 0 10 0 0
* Grade 4 AEs not listed in table: increased blood creatinine (1), acute kidney injury (1), anaphylactic reaction (1).† Grade 4 AEs not listed in table: increased blood triglycerides (2), acute kidney injury (1), sepsis (1), chronic obstructive pulmonary disorder (1), increased blood cholesterol (1), neutropenia (1), pneumonia (1).1. Motzer RJ et al. N Engl J Med. 2015.doi:10.1056/NEJMoa1510665.

Treatment-related AE Any grade (N = 389) Grade 3–4 (N = 389)
Total, n (%) 124 (32) 27 (7)
General, n (%)Fatigue/astheniaPyrexiaLack of appetite/anorexia
60 (15)49 (13)12 (3)5 (1)
9 (2)9 (2)
01 (<1)
Skin and mucosal, n (%)Rash
38 (10)34 (9)
2 (<1)2 (<1)
Gastrointestinal, n (%)DiarrheaNausea/vomiting
33 (8)18 (5)8 (2)
5 (1)3 (1)
2 (<1)
Pain, n (%) 7 (2) 0
Endocrine, n (%)HypothyroidismHyperthyroidismAutoimmune hypophysitis
12 (3)6 (2)6 (2)
1 (<1)
1 (<1)00
1 (<1)
Respiratory/pulmonary, n (%)Pneumonitis
7 (2)3 (1)
3 (1)1 (<1)
Hematologic, n (%)Anemia
11 (3)9 (2)
3 (1)3 (1)
Hepatic/pancreatic, n (%)Increased transaminase
9 (2)5 (1)
00
Real world data: Treatment-related AEs in ≥1% of patients
• Treatment-related grade 3–4 AEs occurred in 27 (7%) patients• AEs were generally manageable with treatment according to protocol-specified guidelines• No treatment-related deaths were reported

Checkmate 025 - Conclusions
➢ Nivolumab significantly improved efficacy compared to everolimus in previously treated pts with advanced metastatic RCC.
▪ Median OS: 26 months (Nivolumab) vs 19.7 months (Everolimus) (hazard ratio, 0.73; P = 0.002).
▪ ORR 25% (nivolumab) vs 5% (Everolimus) (OR: 1.72; P = .0246)
➢ All-grade and grade 3/4 toxicity were lower with nivolumab compared to everolimus.
➢ The survival improvement and favorable safety profile demonstrated provides evidence for nivolumab as a potential new treatment option for previously treated patients with mRCC.

56
Real world data - Conclusions
• The EAP population included some subgroups that were poorly represented or
not represented at all in the pivotal CheckMate 025 study3
• Despite these differences, comparison of the survival curves suggests that the 9-
month OS rate (73%) in the EAP approached that observed in the nivolumab
arm of the CheckMate 025 trial3
• As in CheckMate 025,4 some patients treated beyond progression derived
further benefit with improved tumor response
• The safety profile of nivolumab appeared consistent with that reported in the
CheckMate 025 trial3
• Noting the limitations of this study type, preliminary data from this EAP appear to
confirm data from the pivotal trial and suggest that nivolumab is effective for the
treatment of metastatic RCC in routine clinical practice
56
3. Motzer RJ et al. N Engl J Med. 2015;373:1803-1813.4. Escudier B et al. Eur Urol. 2017. doi: 10.1016/j.eururo.2017.03.037.5. Escudier B et al. Eur Urol. 2017. doi: 10.1016/j.eururo.2017.02.010.

5757
Phase III, randomized, open-label trial of nivolumab combined with ipilimumab vs sunitinib monotherapy in treatment-naïve patients with advanced or metastatic clear cell RCC1
• Primary Outcome Measures: PFS and OS• Key Secondary Outcome Measures: ORR, safety• Select Exploratory Outcome Measure: HRQoL, HRU, predictive
biomarkers
N=1070
Start Date: October 2014Estimated Trial Completion Date: September 2019Estimated Primary Completion Date: June 2019Status: Ongoing, not recruitingStudy Director: Bristol-Myers Squibb
R
1:1
Sunitinib
50 mg PO qd for 4 weeks
( 6 week cycles)
Nivolumab
3 mg/kg IV q3w for 4 doses, then q2w
Key Inclusion Criteria
• Advanced/metastatic clear cell RCC
• No prior systemic therapy for RCC
• Prior adjuvant/neoadjuvant therapy allowed if the agent did not target the VEGF pathway, and recurrence occurred ≥6 months after last dose
• Karnofsky PS ≥70%
• Available FFPE archival or recent tumor tissue sample
• No prior treatment with VEGF pathway agents or agents targeting T-cell costimulation or checkpoint pathways
• No current or history of CNS metastases
Ipilimumab
1 mg/kg IV q3w for 4 doses
Until progression*, unacceptable
toxicity, withdrawal of
consent, or end of trial (up to 5 years)
* Patients may continue treatment beyond progression (RECIST 1.1) if investigator-assessed clinical benefit is achieved and treatment is well-tolerated.2
1. Clinicaltrials.gov. NCT02231749. Accessed November 9, 2016. 2. Hammers H et al. Poster presentation at ASCO 2015. TPS4578.See speaker notes for abbreviations.
Checkmate 214: 1L Nivolumab + Ipilimumab

58
Results of Checkmate-214

59
1st line Phase III trials of combination IO based
therapies in mRCC
Therapeutic target Control
arm
Experimental arm(s)
PD-1 and CTLA-4 Sunitinib Nivolumab + Ipilimumab x 4
Nivolumab
PD1 and IDO-1 Sunitinib
or
Pazopanib
Pembrolizumab + Epacadostat
PD-1 and VEGF Sunitinib Bevacizumab + Atezolizumab
PD-L1 and VEGF Sunitinib Axitinib + Avelumab
PD-L1 and VEGF Sunitinib Axitinib + Pembrolizumab
VEGF/FGF and (PD1 or
mTOR)
Sunitinib Lenvatinib + Pembrolizumab
OR
Lenvatinib + Everolimus
Vaccine (DC+autologous
tumor)
Sunitinib Sunitinib + AGS-003
(rocapuldencel-T)Modified from G. Sonpavde

60
Outline
• Current standards
• Immunotherapy in mBC
• Immunotherapy in mRCC
• Summary

61
Summary
• IO has an established role in the treatment of mRCC( Nivolumab)
• New standard established with recent IO data in first line mRCC ( int/ poor risk)
• A number of ongoing studies in the first line setting with IO combination studies show promise
• Cost and access present a major challenge which needs to be overcome