Embed Size (px)
Citation preview

A Dialysis Case Presentation and Discussion
Edited by William F. Owen, Jr.
Vascular Occlusion and Cardiac Conduction Disturbances in a Patient Undergoing Peritoneal Dialysis
Discussant: Jonathan Kay From: Section of Rheumatology, Lahey Clinic Medical Center, Burlington, and the Department of Medicine, Harvard Medical School, Boston, Massachusetts
Case Presentation
A 46-year-old woman, who had previously been well, developed nausea, vomiting, and anorexia in May 199 1. Her medical history was remarkable only for arthritis involving the knees and the proximal interphalangeal joints of the hands, which was treated for 2 years with ibuprofen and hydroxychloroquine sulfate while she was in her twenties. Her family history was remarkable for a sister who died at age 5 of “nephritis.” Twin brothers both had chronic renal failure caused by primary oxalosis. One had died at age 29 of myocardial infarction and the other at age 34 of complications of gangrene. Neither parent had been diagnosed with renal disease, and both died in their sixties of myocardial infarction. The patient had no chil- dren. Laboratory studies revealed a hematocrit of 26.6%, a BUN of 124 mg/dl, a serum creatinine of 11.2 mg/dl, a serum calcium of 9.2 mg/dl, and a serum phosphate of 7.9 mg/dl. Liver function studies were normal. Urinalysis revealed proteinuria and pyuria without crystals or casts. A 24-hour urine collection revealed normal urinary oxalate excretion. Both kidneys were small and hyperechoic on ultrasonographic examination. Extensive evaluation re- vealed no clear cause for renal failure. A Tenckhoff cath- eter was placed, and maintenance peritoneal dialysis was initiated in July 199 1 for uremic symptoms. A regimen of calcium carbonate, erythropoietin, and Nephrocaps was begun.
Shortly after beginning peritoneal dialysis, the patient noticed transient episodes in which her fingertips became cyanotic, painful, and cool to the touch for periods of about 10 minutes. Subsequently, transient mottling of the skin on her legs developed. She also noted the onset of calf
Address correspondence and reprint requests to: Jonathan Kay, MD, Section of Rheumatology, Lahey Clinic Medical Center, 41 Mall Road, Burlington, MA 01805. Seminars in Dialysis-Vol 6, No 2 (Mar-Apr) 1993 pp 135- 139
pain when walking. The frequency of these episodes in- creased over the course of 1 month, and she was referred for rheumatological evaluation.
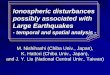
On examination, livedo reticularis was present on both lower legs. The fingers were cool to the touch, and the toes were cyanotic. Joint deformities and signs of inflammation were absent. The arterial pulses were normal in both upper extremities and in both femoral arteries: however, the popliteal, posterior tibial, and dorsalis pedis arterial pulses were very weak bilaterally. No bruits were audible. Labo- ratory studies revealed an erythrocyte sedimentation rate of 75 mm/hr, cholesterol of 240 mg/dl, and triglycerides of 176 mg/dl. Antinuclear antibodies, rheumatoid factor, and cryoglobulins were absent. The CH50 was slightly elevated to 276, and levels of Clq, C3, and C4 were normal. Serum oxalate was 99 mmol/L (normal, <6 mmol/L). Biopsies of the skin on both lower legs demonstrated deposition of calcium oxalate crystals within the lumina and muscular walls of the subcutaneous arteries (Fig. 1). No evidence of vasculitis or cholesterol emboli was found. Aortography demonstrated narrowing of the left anterior tibial and right distal popliteal arteries and occlusion of both posterior tibial arteries at or near their origins. There was collateral blood flow to both ankles.
Treatment with 10 mg oral nifedipine three times daily was started, with transient improvement of acrocyanosis and livedo reticularis. The dosage was increased to 30 mg, three times daily, with symptomatic improvement. How- ever, complete heart block developed subsequently, and treatment with nifedipine was discontinued. Treatment with isosorbide dinitrate resulted in persistent improve- ment of acrocyanosis and livedo reticularis. Unfortunately, while awaiting evaluation for combined liver-kidney trans- plantation, the patient awakened early one morning, com- plained of abdominal pain, and collapsed. Resuscitative efforts failed.
Postmortem examination of the heart and kidneys re- vealed that the coronary vessels were pliable, with a 40% to 50% focal narrowing of the luminal diameter of the
135

136 Kav
FG. I . Punch biopsy of skin from the patient’s lower leg, examined under polarizing light, showing refractile crystalline material of varying sizes. Hematoxylin and eosin stain; ~ 4 0 0 .
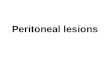
proximal left anterior descending and circumflex arteries. Areas of intimal proliferation contained both spherical deposits of needlelike crystals in a stellate array, consistent with calcium oxalate crystals, and deposits of calcium phosphate, associated with atherosclerotic disease. Exten- sive deposition of calcium oxalate crystals was present within the atrioventricular node, the bundle of His, and the left bundle branch (Fig. 2) . Moderate patchy oxalate crystal deposition was noted in the interstitium, within the cells, and within the media of the small arteries in tissue taken from the left ventricle.
The kidneys were small, weighing 58 and 60 g, and had a coarse capsular nodularity consistent with severe neph- rosclerosis. Several minute nephroliths (diameter, 0.4 cm) were imbedded within the cortical parenchyma, which, on crystallographic analysis, were found to be composed of calcium oxalate monohydrate. The surface crystals were composed of calcium oxalate dihydrate. Specimen radiog- raphy revealed the diffuse deposition of radio-opaque crys- tals throughout both kidneys. Microscopic examination of the kidney demonstrated severe glomerulosclerosis and extensive interstitial, intratubular, and glomerular crystal deposition consistent with oxalosis. Although no apple- green birefringence was noted on polarization microscopy with Congo red staining, immunoperoxidase staining dem- onstrated /32-microgIobulin deposition within the syno- vium of the left shoulder.
These histological findings suggested that the cause of sudden death was complete atrioventricular block caused by the interruption of the cardiac conduction system by deposits of calcium oxalate crystals.
Discussion
Jonathan Kay: Several clinical manifestations of primary oxalosis appeared in this unfortunate woman: chronic renal failure, vascular occlusion, and cardiac conduction disturbances. Histological examination of tissues demonstrated that each of these clinical presentations was caused by deposits of calcium oxalate crystals. The strong family history of renal failure related to primary oxalosis under- scores the hereditary basis for this metabolic defect. Although this woman had no history of nephrolithi- asis, and liver biopsy was not performed to identify a
FIG. 2. Autopsy specimen of the patient’s cardiac conduction system showing crystal deposition (arrows) within the bundle of His. Trichrome stain: x 100.
specific enzyme deficiency, her clinical presentation was most consistent with that of primary hyperox- aluria type I. The cardiac and vascular disease may have been accelerated by the administration of as- corbic acid. a ubiquitous constituent of the multivi- tamin preparations that are routinely administered to individuals with end-stage renal disease (ESRD).
Over the past decade, much has been learned about primary hyperoxaluria type I. The deficient enzyme has been identified and cloned, and the advances made in liver transplantation have allowed for correction of the metabolic defect in some pa- tients. However, this case emphasizes the fulminant course of this disease when renal failure has devel- oped and the inadequacy of available therapies to reverse this devastating condition.
Metabolism of Oxalate and Oxalosis
Although oxalic acid is found in plants and vege- tables, it is poorly absorbed from the gastrointestinal tract. Most of the oxalate within the body is derived from the endogenous metabolism of ascorbic acid, or vitamin C, and glyoxylate (1). Ascorbic acid is oxidized to oxalate (2). Much of the glyoxylate in the body is transaminated to glycine, a reaction that is dependent on the cofactor pyridoxine ( 3 ) . Pyri- doxine deficiency will thus lead to decreased conver- sion of glyoxylate to glycine and increased conver- sion of glyoxylate to oxalate. Glyoxylate is oxidized to oxalate in the cytosol by lactate dehydrogenase and nicotinamide adenine dinucleotide (4). The ingestion of precursors of glyoxylate, such as ethylene glycol, will also result in increased oxalate biosyn- thesis ( 5 ) . Oxalate itself is an end product of metab- olism in mammals and is normally excreted in the urine.
Primary hyperoxaluria may occur because of in- sufficient activity of an enzyme involved in the me- tabolism of glyoxylate. Primary hyperoxaluria type I (glycolic aciduria) is caused by a deficiency of the hepatic peroxisomal enzyme a1anine:glyoxylate ami- notransferase (AGT) (6). Pyridoxine is a cofactor for this enzyme (7). Primary hyperoxaluria type I is inherited as an autosomal recessive disorder. Ap-

VASCULAR OCCLUSION AND CARDIAC CONDUCTION DISTURBANCES 137
proximately 65% of affected individuals present with symptoms of calcium oxalate nephrolithiasis, such as renal colic or gross hematuria. before the age of 5 . More than 80% of patients with this condition die in renal failure before the age of 20 (3). This patient was highly unusual in that the initial manifestation of the disease was uremia and that this occurred after the age of 40.
Primary hyperoxaluria type I1 (L-glyceric aciduria) is caused by a deficiency of the cytosolic enzyme D- glycerate dehydrogenase, or glyoxylate reductase. In- dividuals with this condition excrete excessive amounts of both oxalate and L-glyceric acid in their urine. The limited number of cases reported makes determination of the inheritance pattern difficult. but primary hyperoxaluria type I1 also appears to be inherited as an autosomal recessive disorder (8, 9).
Patients with chronic renal failure with normal oxalate metabolism and who ingest normal exoge- nous loads of glyoxylate precursors have elevated plasma levels of oxalate because of reduced oxalate clearance by the kidney (10). The contributory role of oxalosis in the progression of chronic renal failure is unknown. The serum of uremic individuals is supersaturated with calcium oxalate before hemodi- alysis ( 1 1). In patients with primary hyperoxaluria type I ( 12) or ESRD unrelated to oxalosis ( 1 3) who undergo hemodialysis or continuous ambulatory peritoneal dialysis (CAPD), the rate of oxalate for- mation exceeds that of oxalate removal. Despite greater clearance of oxalate by hemodialysis than by CAPD (12, 13), the steady-state levels of plasma oxalate in patients with chronic renal failure who are receiving CAPD are similar to levels in patients receiving hemodialysis ( 13, 14).
Because of dialysate losses, water-soluble vitamins, such as vitamin C, are routinely administered to patients with ESRD (15). Because ascorbic acid is metabolized to oxalate, formulations of vitamins containing ascorbic acid (vitamin C) increase the concentration of plasma oxalate in patients with chronic renal failure who are undergoing hemodi- alysis ( 1 6- IS) or peritoneal dialysis (19). Thus, the administration of vitamin supplements containing ascorbic acid to patients with chronic renal failure may exacerbate manifestations of oxalosis. Daily oral supplements of ascorbic acid (100 mg, 0.57 mmol) may result in a 19% increase in levels of plasma oxalate in patients without primary hyperoxaluria who are undergoing peritoneal dialysis (19). The patient began taking a multivitamin with 100 mg of ascorbic acid per tablet shortly before she noted the onset of acrocyanosis, livedo reticularis, and calf claudication. Perhaps the additional ingestion of this precursor of oxalate accelerated the deposition of calcium oxalate crystals in the vessels.
Vascular Complications of Oxalosis
Soon after the initiation of peritoneal dialysis in this patient, intermittent episodes of acrocyanosis developed. She had no previous history of Raynaud's phenomenon, which might have accompanied a sys-
temic rheumatic disease, such as systemic lupus er- ythematosus. After the onset of episodic acrocy- anosis, transient mottling of the skin on her legs developed in a purplish reticular pattern. Livedo reticularis appears when stasis of blood exists in the superficial venules draining the skin. These venules, supplied by arterioles that branch like a candelabra into capillaries perpendicular to the surface of the skin, are arranged in a meshlike network parallel to and just beneath the epidermis. Thus, the pattern of discoloration follows the anatomic distribution of the superficial cutaneous venules and resembles chicken wire or a fishnet (20).
Livedo reticularis may occur in healthy individ- uals who are exposed to the cold, or it can be secondary to increased blood viscosity. Disease states that cause increased blood viscosity or that obstruct blood flow to or from superficial cutaneous venules may present with livedo reticularis. Polycythemias, paraproteinemias, cold precipitable proteinemias, and hypercoagulable states may each increase blood viscosity and result in livedo reticulark. Atheroscle- rosis, emboli, and vasculitis involving the small ar- terioles supplying the skin may each lead to livedo reticularis. Immune complex deposition, endothelial cell damage mediated by infectious agents or endo- toxin or both, and cutaneous venulitis may each manifest as livedo reticulark (20). Among patients with chronic renal disease, calcification of deep der- mal muscular vessels caused by secondary hyperpar- athyroidism (2 1 ) and deposition of calcium oxalate crystals in cutaneous blood vessels (22) may also cause livedo reticularis. To differentiate these proc- esses in this patient, a punch biopsy of the skin was performed.
Livedo reticularis (22-28) claudicatory symp- toms, acrocyanosis, and gangrene (22, 27-30) may develop in patients with primary hyperoxaluria be- cause of the deposition of oxalate in blood vessels. Oxalate crystals most often are deposited in the media of arterioles, leading to vascular smooth mus- cle spasm and clinical manifestations of ischemia. These crystals may also be deposited within the lumina of vessels, thereby appearing similar to the atherosclerotic plaques on vascular imaging studies. Calcium oxalate crystals activate complement in vi- tro. Serum incubated with calcium oxalate crystals stimulates generation of neutrophil superoxide, chemiluminescence, hexose monophosphate shunt activity, and chemotaxis. Calcium oxalate crystal- activated serum also augments the adhesion of neu- trophils to endothelial cells of human umbilical vein and neutrophil-mediated 5'Cr release from endothe- lial cells (31). In vivo, these crystals may induce a vasculitis of small arteries and arterioles.
As in the case of this patient, the vascular mani- festations of primary oxalosis often appear shortly after initiation of renal replacement therapy. Renal clearance of oxalate decreases as renal function wors- ens. As soon as dialysis has been initiated, urinary clearance of oxalate is greatly reduced, and levels of plasma oxalate rise (22). The observation that is- chemic symptoms can worsen with nephrectomy has

led to the hypothesis that the failing kidney serves as a sponge that absorbs oxalate crystals and delays their deposition elsewhere. Thus, bilateral nephrec- tomy is relatively contraindicated in primary hyper- oxaluria (32).
Various modalities have been tried without success in the treatment of peripheral vascular insufficiency associated with primary hyperoxaluria, including peritoneal dialysis, heparin anticoagulation, cortico- steroids, epidural block, vasodilators, hyperbaric oxygen, lumbar sympathectomy (30), and phenoxy- benzamine (32). Sublingual nitroglycerin and oral isosorbide dinitrate have improved symptoms of pe- ripheral vascular insufficiency in one patient with primary hyperoxaluria (29). In the patient described previously, symptoms of acrocyanosis and livedo reticularis improved with use of the vasodilatory calcium channel blocker nifedipine. After discontin- uation of nifedipine. the patient’s vascular symptoms improved on oral nitrate therapy.
Cardiac Complications of Oxalosis
Subsequent to the onset of peripheral vascular symptoms and while this patient was on nifedipine therapy, transient complete heart block developed. Arrhythmia resolved when nifedipine was stopped. Crystals that were consistent with calcium oxalate were deposited within coronary arteries and in the interstitium, within the cells, and within the media of the small arteries in tissue taken from the left ventricle. Although vasospasm of the coronary arter- ies could induce ischemia of the His bundle and abnormalities of the conduction system, no evidence of recent or remote myocardial infarction was found on postmortem examination. Nifedipine has no ap- preciable effect on atrioventricular nodal conduction (33). The development of complete heart block in this patient suggests the presence of underlying dis- ease in the conduction system.
As also seen in the vasculopathy associated with primary hyperoxaluria, deposition of calcium oxa- late crystals in tissue may cause the observed clinical manifestations. In this patient, calcium oxalate crys- tals most likely contributed to disturbances in the conduction system. Complete heart block has been reported (26, 34-40) in several patients with primary oxalosis. In three patients, deposits of oxalate crystals were demonstrated in the cardiac conduction system at postmortem examination (34, 38, 40). A study (41) in nephrectomized rats that were given auxiliary heart allografts suggests that myocardial deposition of oxalate crystals is dependent on time and damage to local tissues. Similar to the patient presented previously, a 45-year-old woman with primary ox- alosis has been reported who developed livedo retic- ularis followed by several episodes of complete heart block shortly after the onset of acute renal failure (26). However, the histological appearance of the cardiac conduction system was not described.
Treatment of Primary Oxalosis
The initial treatment of individuals with primary hyperoxaluria is directed toward decreasing forma-
tion of oxalate calculi and preserving renal function. Because pyridoxine (vitamin B6) is a cofactor for AGT, pyridoxine should be administered to decrease urinary excretion of oxalate (42). However, some individuals have a form of primary hyperoxaluria that is resistant to pyridoxine. Therapy for all pa- tients with primary hyperoxaluria should include an increase in fluid intake and administration of citrate or thiazide diuretics to decrease the excretion of calcium in the urine (43). Although little oxalate is absorbed from the gastrointestinal tract, foods con- taining high levels of oxalate should be avoided (44). These include spinach, rhubarb, peanuts, chocolates, parsley, and tea (45). The administration of precur- sors of oxalate, such as ascorbic acid, should be limited. Orthophosphate or magnesium gluconate can be prescribed to inhibit the formation of calcium oxalate crystals (43).
When a patient with primary hyperoxaluria has developed renal insufficiency, biopsy of the liver should be performed to confirm the diagnosis by measurement of AGT activity (46). The treatment of primary oxalosis has been directed, until recently, toward the correction of end-organ damage resulting from deposition of oxalate crystals. When end-stage renal failure has occurred, aggressive dialysis should be instituted to maximize clearance of oxalate. When the patient has a pyridoxine-sensitive form of pri- mary hyperoxaluria type I, pyridoxine therapy should be continued. Renal transplantation has been attempted, but many of the transplanted kidneys have failed because of deposition of oxalate in the graft. A medical regimen aimed at optimizing re- moval of oxalate has resulted in improved graft survival (47).
Because the enzyme that is deficient in primary hyperoxaluria type I (AGT) is predominantly ex- pressed in the liver (48), the current surgical ap- proach to therapy corrects the underlying metabolic defect and restores renal function by combined he- patic and renal transplantation. In 1985, Watts and colleagues (49) in Cambridge, England, reported the first combined liver-kidney transplant in a patient with primary hyperoxaluria type I. Although the patient died from disseminated cytomegalovirus in- fection 8 weeks after operation. the underlying met- abolic defect had been corrected. The following year, Watts and his group (50) performed a successful combined liver-kidney transplant in another patient with primary hyperoxaluria type I. That patient has remained asymptomatic over a 50-month follow-up period and has returned to full-time employment (37).
Of nine patients with primary hyperoxaluria type I who underwent combined liver-kidney transplan- tation by the group in Cambridge, England, at the Mayo Clinic, or at the University of Michigan, four have survived, with follow-up of 36 to 50 months after operation. They have remained without symp- toms of systemic oxalosis or of renal disease. The major complications associated with this procedure have been infections, biliary leaks, and poor function of the transplanted kidney. The outcome was better in patients with a shorter duration of renal failure

VASCULAR OCCLUSION AND CARDIAC CONDUCTION DISTURBANCES 139
before transplantation and with less systemic depo- sition of calcium oxalate crystals. The patient in their series with congestive cardiomyopathy caused by myocardial oxalosis and complete heart block had resolution of his symptoms after transplantation (37). However, implantation of a pacemaker may be prudent in a patient with primary hyperoxaluria type I and evidence of cardiac conduction disturbances because these individuals may experience complete heart block and sudden death. Another patient with a dilated cardiomyopathy, presumed to be caused by primary hyperoxaluria type I, demonstrated im- provement in cardiac function after a combined liver-kidney transplantation that was performed at another institution (28). Thus, early diagnosis of primary hyperoxaluria type I, aggressive therapy to lower levels of plasma oxalate and reduce deposits of oxalate in tissues, and early consideration for liver or combined liver-kidney transplantation may offer patients with this inborn error of metabolism the greatest hope for asymptomatic survival.
References 1. Williams HE: Oxalic acid and the hyperoxaluric syndromes. Kidnn,
Int 13:410-417, 1978 2. Baker EM, Saari JC, Tolbert BM: Ascorbic acid metabolism in man.
Am JClm Nirfr 19:371-378. 1966 3. Williams HE, Smith LH Jr: Primary hyperoxaluria. in The 124etabolrc
Basis of Inherited Disease (Fifth Ed). edited by Stanbury JB, Wyngaar- den JB, Frederickson DS, Goldstein JL, Brown MS. New Yorh. McGraw-Hill. 1983, pp. 204-228
4. Sawaki S, Hattori N, Yamada K: Reduction of nicotinamide-adenine dinucleotide by glyoxylate in animal organs. J Vitamin 12303-306, I966
5. Parry MF. Wallach R: Ethylene glycol poisoning. .4m JMed 57: 143- 150, 1974
6. Danpure CJ, Jennings PR: Peroxisomal a1anine:glyoxylate aminotrans- ferase deficiency in primary hyperoxaluria type I. FEBS Lett 201:20- 24, 1986
7. Watts RWE, Veall N, Purkiss P, Mansell MA. Haywood EF: The effect of pyridoxine on oxalate dynamics in three cases of primary hyperox- aluria (with glycollic aciduria). Clin Sci 69:87-90. 1985
8. Williams HE. Smith LH Jr: L-Glyceric aciduria: A new genetic variant of primary hyperoxaluria. N EnglJMed 278:233-239, 1968
9. Chalmers RA, Tracey BM, Mistry J, Griffiths KD, Green A. Winter- born MH: L-Glyceric aciduria (primary hyperoxaluria type 2) in siblings in two unrelated families. J Inherited Metab Dis 7(Suppl 2): 133-1 34. 1984
10. Zarembski PM. Hodgkinson A, Parsons FM: Elevation of the concen- tration of plasma oxalic acid in renal failure. Nature 21251 1-512. 1966
1 1 . Worcester EM. Nakagawa Y, Bushinsky DA, Coe FL: Evidence that serum calcium oxalate supersaturation is a consequence of oxalate retention in patients with chronic renal failure. J Clin Invest 77: 1888- 1896. 1986
12. Watts RWE. Veall N. Purkiss P: Oxalate dynamics and removal rates during haemodialysis and peritoneal dialysis in patients with primary hyperoxaluria and severe renal failure. Clin Sci 66:59 1-597, 1984
13. Costello JF, Sadovnic MJ, Cottington EM: Plasma oxalate levels rise in hemodialysis patients despite increased oxalate removal. J A m soc Nephrol 1:1289-1298. 1991
14. McConnell KN, Rolton HA, Modi KS, Macdougall AI: Plasma oxalate in patients with chronic renal failure receiving continuous ambulatory peritoneal dialysis or hemodialysis. Am JKidney Dis 18:44 1-445, 199 1
15. Wolfson M: Use of water-soluble vitamins in patients with chronic renal failure. Semin Dia/ 1:28-32. 1988
16. Balcke P. Schmidt P. Zazgornik J , Kopsa H, Haubenstock A: Ascorbic acid aggravates secondary hyperoxalemia in patients on chronic he- modialysis. Ann Intern Med 101:344-345, 1984
17. Pru C. Eaton J, Kjellstrand C: Vitamin C intoxication and hyperoxal- emia in chronic hemodialysis patients. Nephron 39:l 12-1 16, 1985
18. Ono K Secondary hyperoxalemia caused by vitamin C supplementa- tion in regular hemodialysis patients. Clin Nephrol26:239-243, I986
19. Shah GM, Ross EA, Sabo A, Pichon M, Reynolds RD, Bhagavan H: Effects of ascorbic acid and pyridoxine supplementation on oxalate
metabolism in peritoneal dialysis patients. Am J Kidney Dis 20:42-49. 1992
20. Copeman PWM: Livedo reticularis: Signs in the skin of disturbance of blood viscosity and of blood flow. Br J Dermatol93:5 19-529, 1975
2 I . Winkelmann RK, Keating FR Jr: Cutaneous vascular calcification, gangrene and hyperparathyroidism. Br J Dermatol83:263-268, 1970
22. Jansen LH. Groeneveld JL, van der Meer J B Deposition of calcium oxalate in the skin in two patients suffering from oxalosis caused by primary hyperoxaluria. Arch Dermatol Res 250323-350, 1974
23. Greer KE, Cooper PH. Campbell F, Westervelt FB Jr: Primary oxalosis with livedo reticularis. Arch Dermatol 116213-214. 1980
24. Winship IM, Saxe NP, Hugel H: Primary oxalosis: An unusual cause of livedo reticularis. Clin Exp Dermatol 16:367-370, 1991
25. Bodemer C, Flament F, Grunfeld JP. De Prost Y. Oxalose primitive et livedo reticulaire: A propos d u n cas. Ann Dermatol Venereol 116:721- 724. 1989
26. Spiers EM. Sanders DY, Omura E F Clinical and histologic features of primary oxalosis. J Am Acad Dermatol22:952-956, 1990
27. Baethge BA, Sanusi ID, Landreneau MD, Rohr MS, Mcdonald J C Livedo reticularis and peripheral gangrene associated with primary hyperoxaluria. Arthritis Rheum 31:1199-1203, 1988
28. Rodby RA. Tyszka TS, Williams J W Reversal of cardiac dysfunction secondary to type I primary hyperoxaluria after combined liver-kidney transplantation. .4m J M e d 90498-504, 1991
29. Dennis AJ Jr. Hudson JB. Humphries AL. Dasgupta G. Wray CH: Nitroglycerin as a remedy for peripheral vascular insufficiency associ- ated with oxalosis. Ann Intern Med 92:799-800, 1980
30. Arbus GS, Sniderman S: Oxalosis with peripheral gangrene. Arch Patho/97:107-I 10, 1974
3 1. Boogaerts MA, Hammerschmidt DE, Roelant C, Venvilghen RL, Jacob HS: Mechanisms of vascular damage in gout and oxalosis: Crystal induced, granulocyte mediated. endothelial injury. Thromb Haemost 50:576-580. 1983
32. Blackburn WE, McRoberts JW, Bhathena D, Vazquez M, Luke RG: Severe vascular complications in oxalosis after bilateral nephrectomy. Ann Intern Med 82:44-46. 1975
33. Rowland E. Evans T. Krikler D: Effect of nifedipine on atrioventricular conduction as compared with verapamil. Intracardiac electrophysiolog- ical study. Br Heart J42:124-127, 1979
34. Coltart DJ, Hudson REB: Primary oxalosis of the heart: A cause of heart block. BrHeartJ33:315-319, 1971
35. Gupta AK. Billings JK, Headington JT: Multisystem crystalline depos- its: Primary hyperoxaluria. Arch Dermatol 125:552-556, 1989
36. Absy MM: Atypical features of primary hyperoxaluria in end-stage renal disease. Am J Nephrol I 1 :30 1-304. 199 I
37. Watts RWE, Morgan SH, Danpure CJ, Purkiss P. Calne RY, Rolles K. Baker LRI, Mansell MA, Smith LH. Merion RM, Lucey M R Combined hepatic and renal transplantation in primary hyperoxaluria type I: Clinical report of nine cases. .4m J Med 90: 179-188, 199 I
38. West RR. Salyer WR, Hutchins GM: Adult-onset primary oxalosis with complete heart block. Johns Hopkins Med J 133: 195-200. 1973
39. Stauffer M: Oxalosis: Report of a case, with a review of the literature and discussion of the pathogenesis. N Engl JMed 263:386-390. 1960
40. Massie BM, Bharati S, Scheinman MM. Lev M. Desai J, Rubeson E, Schmidt W Primary oxalosis with pan-conduction cardiac disease: Electrophysiologic and anatomic correlation. Circulation 64:845-852, 1981
4 1. Ono K: Oxalate crystal deposits in the heart in chronic renal failure: An experimental study. Nephrol Dial Transplant 5:493-496, 1990
42. Yendt ER, Cohanim M: Response to a physiologic dose of pyridoxine in type I primary hyperoxaluria. N EnglJ Med 312:953-957, 1985
43. Scheinman JI: Primary hyperoxaluria: Therapeutic strategies for the 90's. Kidnev Int 40:389-399, 1991
44. Yendt ER, Cohanim M. Peters L: Reduction of urinary oxalate excre- tion in primary hyperoxaluria by diet, in Urolithiasis: Clinical and Basrc Research, edited by Smith LH, Robertson WG, Finlayson B. New York, Plenum Press, 1981, pp. 373-377
45. Kasidas GP, Rose GA: Oxalate content of some common foods: Determination by an enzymatic method. J Hum Nutr 34:255-266, 1980
46. Danpure CJ, Jennings PR, Watts RWE: Enzymological diagnosis of primary hyperoxaluria type I by measurement of hepatic ala- nine:glyoxylate aminotransferase activity. Lancet 1 :289-29 I , 1987
47. Scheinman JI. Najarian JS. Mauer SM: Successful strategies for renal transplantation in primary oxalosis. Kidney Int 25:804-811, 1984
48. Kamoda N, Minatogawa Y, Nakamura M, Nakanishi J, Okuno E. Kid0 R: The organ distribution of human alanine-2-oxoglutarate ami- notransferase and alanine-glyoxylate aminotransferase. Biochem Med 23:25-34, 1980
49. Watts RWE, Calne RY. Williams R, Mansell MA, Veall N, Purkiss P, Rolles K: Primary hyperoxaluria (type I): Attempted treatment by combined hepatic and renal transplantation. Q J Med 57:697-703. 1985
50. Watts RWE. Calne RY. Rolles K, Danpure CJ, Morgan SH. Mansell MA. Williams R, Purkiss P Successful treatment of primary hyperox- aluria type I by combined hepatic and renal transplantation. Lancet 21474-475, 1987