Embed Size (px)
Citation preview

J. Cranio-Max.-Fac. Surg. 16 (1988) 2 4 7
J. Cranio-Max.-Fac. Surg. 16 (1988) 247-265 © Georg Thieme Verlag Stuttgart • New York
Variations of a Standard Approach for Correction of the Bird-Face Deformity Hugo L. Obwegeser
Director emeritus of the Clinic for Maxillo-Facial Surgery, University Hospital Ziirich, and Professor emeritus and Head of Department of Oral Diagnosis and Oral Surgery, Dental School, University of Ziirich, Switzerland.
Submitted 7.4.87; accepted 23.8.87
Introduction
The so-called bird-face deformity has various aetiologies. The skeletal and clinical pictures of bird-face deformity are, however, more or less always the same. The age of the patient at onset and the specific aetiology of the develop- mental disturbances influence the degree of malformation. Accordingly, the correction of bird-face deformity in- volves a general procedure which is almost the same for all cases, varying only according to the degree of malforma- tion. The only major difference in treating the malforma- tion depends on whether the case presents a symmetrical or an asymmetrical bird-face deformity. Whenever a general problem arises, we should look for a general solution. This solution, if need be, should also be adaptable to solve particular problems. It is not difficult to find a solution to a given problem, the real difficulty is to identify the problem. Based on our philosophy and our principles of treatment planning for the correction of fa- cial deformities, we believe that we have found such a so- lution to correct the bird-face deformity so that we are able to speak of a standard procedure for correction of bird-face deformity. In our clinic, this procedure has proved reliable for treating the symmetrical as well as the asymmetrical forms. This is discussed below. Maxillary protrusion, inferior position of the maxilla or an open bite do not change the principles involved in the correction of the bird-face. It only necessitates additional osteotomies.
The Anatomical Basis of the Symmetrical Form
Anatomically, this is primarily a bilateral hemimandibular micromandibulism associated with retrogenia. Both sides of the mandible exhibit the same abnormalities of the body including the chin and ascending ramus, angle and TMJ region. In the sagittal plane, the dental arch is longer than the body of the mandible. Accordingly, all teeth can be present with or without crowding, even though this is always associated with protrusion of the lower anterior teeth. Thus, an apparently normal occlusion might exist but with a much greater proclination of the lower teeth, particularly in the anterior region. On the other hand, the small mandible might give rise to a negative incisor overjet associated with a distocclusion. The presence of anterior
Summary
Variations of a standard operation technique for the correction of the bird-face deformity on the basis of fundamental planning principles are described. The main principle is the lengthening of the mandibular base in the retromolar and mental regions. The pre- conditions for the feasibility of this procedure are: ap- propriate tooth extraction and retropositioning of the lower anterior segment in spite of a seemingly good preoperative occlusion. The correction planning must, in addition to the mandible, also consider the maxilla. The asymmetrical bird-face deformity is also corrected in one operation but it is first made symmetrical to fa- cilitate its correction. Case illustrations with corre- sponding operation drawings demonstrate the varia- tion possibilities of the surgical technique as adapted to particular cases.
Key words
Bird-face deformity - Micromandibulism - Mandibu- lar deficiency.
maxillary protrusion might either accentuate the retropo- sitioned mandible or simulate it. The mandibular arch is characteristically very narrow. This is manifest not only in the area of the occlusal plane but also and especially in the anterior half of the body, and at the lower border of the mandible. The ascending ramus too is very short, and the angle of the mandible is markedly small in size. The lower border of the mandible is notched anterior to the angle. The extent of the diminu- tion of the affected mandible varies depending on the aeti- ology and the age of the patient at the onset of the under- development as stated above. Thus, early childhood anky- losis and congenital aplasia of the condyle lead to the most marked form of this mandibular malformation.
The Anatomical Basis of the Asymmetrical Form
In the case of the symmetrical form, the developmental de- ficit, be it anlage-induced or secondarily acquired due to early childhood trauma or disease of the TMJ, affects both sides of the mandible equally and to the same extent. In the case of the asymmetrical form, however, only one side is affected, or both sides are affected unequally. The characteristic example of unilateral bird-face deformity is the deformity resulting from unilateral ankylosis occur- ring during early childhood. In this case, the affected side exhibits the skeletal anomalies described for the symmetri- cal form while the unaffected side exhibits normal devel- opment. There is an analogous condition of the alveolar process and dental alignment. The unaffected side appears to grow beyond the facial midline while the affected side remains diminished in all its parts and lies retropositioned. This produces the asymmetrical bird-face deformity. In the case with a complete dentition, crowding occurs in the premolar region of the diminished side and, as in the case of the symmetrical form, there is lower anterior protru- sion, often associated with crowding.

248 J. Cranio-Max.-F ac. Surg. 16 (1988) H. L. Obwegeser
Secondary Effects on the Maxilla
Retardation in the vertical development of the maxilla on the affected side develops unilaterally or bilaterally in the following cases: early childhood ankylosis, hemifacial mic- rosomia, other congenital or anlage-induced or acquired anomalies which affect the TMJ in early childhood. The unilateral cases result in a tilted occlusal plane, while in the bilateral cases the posterior part of the maxilla is retarded in its vertical development.
Presurgicat Treatment Measures
Presurgical treatment measures become urgent either be- cause of aetiological reasons or due to the clinical picture of the anatomical substrate in question.
Ankylosis In the case where ankylosis is the cause of the bird-face, there is no doubt that it must be treated first, no matter whether it is unilateral or bilateral. We have had very good results from reconstruction of the TMJ by interposition- ing laminated lyocartilage (Obwegeser and Farmand, 1982). We are of the opinion that long-term maintenance and stability of mouth opening is necessary prior to the overall corrective surgery in order to prevent relapse of the ankylosis which adversely affects the whole corrective procedure. A follow-up period of at least one year is ne- cessary following treatment of the ankylosis.
Impacted Teeth There is impaction of the wisdom teeth and occasionally the second molars and often crowding of the premolars due to shortening of the mandible in the molar and retro- molar regions. Due to the reduced height of the body of the mandible in this region the roots of the teeth are situ- ated close to the lower border of the mandible. Here lies the point of greatest weakness. The danger of fracturing the mandible in this region, be it during the mobilization of the ankylosis or mandibular advancement by means of sagittal osteotomy, is equally high. Hence, teeth to be ex- tracted should be removed 4 to 6 months prior to treat- ment of the ankylosis or correction of the bird-face defor- mity respectively, so that there is enough time for osseous repair of the extraction wounds.
Orthodontic Presurgical Treatment The aims of orthodontic presurgical treatment must be to create a normal dental arch and curve of Spee containing only as many teeth as can be maintained in proper angula- tion to their respective mandibular base. The dental arches must relate correctly to each other subsequent to mandib- ular advancement and eventual repositioning of the maxil- la. Protrusion of the lower anterior teeth always occurs. The upper anteriors may also occasionally be protruded. The protrusion of the lower anteriors prevents advancement of the mandible. Hence, this must be corrected after the ex- traction of at least one premolar on each side. The result- ing gap should be closed orthodontically in an antero-pos- terior direction and not vice versa. It is best to leave the removal of the bicuspids for the surgical repositioning of the anterior alveolar segment. Surgery can utilize the whole width of the bicuspids.
In extreme cases of micromandibulism, a severe crowding exists in the bicuspid and molar regions in addition to the protrusion of the lower anteriors. This includes a lingually displaced premolar tooth and, occasionally, lingual inclina- tion of the molars. Thus, under such circumstances, several teeth might have to be sacrificed on either side in order to maintain the rest of the teeth in their proper angulation to the mandibular base. This would mean the extraction of one incisor and one premolar tooth on each of the affect- ed sides in addition to the removal of the wisdom tooth and possibly the second molar. This increases the incisor overjet; the greater the overjet the better. Unfortunately, adequate orthodontic presurgical treat- ment is very often unachievable. In these cases, the neces- sary extraction of the teeth in the incisor and premolar re- gions and the retraction of the mandibular anteriors must be accomplished surgically. If there is no crowding to start with, an excellent result from both the occlusal and aes- thetic points of view may be obtained in spite of no or- thodontic presurgical treatment.
Aims of Treatment The patient and the surgeon pursue the same treatment goal which includes the following objectives: the restora- tion of a normal appearance, the maintenance or restora- tion of good occlusion or intercuspidation and avoidance of disadvantages, especially those resulting from external incisions. It goes without saying, that patients who have already suffered due to the bird-face deformity would not readily accept further deformities or disabilities such as visible scars caused by external incisions or damage to the mandibular branch of the facial nerve.
Planning and Treatment Philosophy
It is the skeletal structure that gives form to the face. Hence, the skeletal anomaly must be evaluated in detail and the skeletal parts repositioned to restore a normal fa- cial skeleton and proper occlusion. In the course of time, our experience in treatment planning for correction of cranio-maxillofacial skeletal anomalies has crystallized in- to the following essential principles of treatment planning. These principles also indisputably apply to the correction of bird-face deformity:
1. The facial skeleton is the framework that determines the shape of the face.
2. All reconstructive surgery of the facial skeleton ought to be performed without employing external incisions on the face.
3. In planning corrective surgery of the facial skeleton, the sequence must be: first the profile then the occlu- sion.
4. The size and position of the bases of the facial thirds determine the profile type. Therefore, a real alteration of the facial profile can be achieved only by altering the bases of the facial thirds.
5. When planning an orthognathic case, consider the jaws as if they were edentulous. Then one will be able to plan to place the bases, not just the teeth, into their correct relationship.
6. In the treatment of a facial anomaly, the correct angu- lation of the teeth to their respective jaw base is more important than any other cephalometric angles.

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (i988) 2 4 9
7. Only retain as many teeth in the alveolar process as can be maintained in their proper angulation to the re- spective jaw base.
8. In the case of micromandibulism, do not elongate the mandible only without widening the mandibular con- tOUr.
9. In orthognathic surgery the segments must be made so loose that they can be easily overcorrected with a pair of tweezers.
10. Cortical bone shrinks 'like a mushroom in the sun' and cancellous bone melts away like an ice cream, when used as onlay grafts for contour correction.
11. Transform an asymmetrical facial deformity first into a symmetrical one. Then it is either already corrected or it becomes easier to correct.
General Principles of the Operation Technique
Subject to the above-mentioned planning philosophy and treatment principles, the normal length of the mandibular base and its normal position in relation to the other parts of the facial skeleton and at the same time the correct an- gulation of the teeth to their mandibular base must be re- stored. There are two possibilities to achieve the latter: to reduce the number of teeth or to lengthen the mandibular base. We prefer the first alternative. To this effect we re- move one premolar tooth from each side and set back and upright the anterior tooth-bearing alveolar process to its correct angulation. If vertical excess of the anterior alveo- lar process exists, then it will be reduced accordingly (Ho- fer, 1942; K61e, 1959; Obwegeser, 1968 b; 1969). The lengthening of the mandibular base is achieved by surgery in the retromolar and chin regions. Surgery in the retro- molar area involves a variation of the sagittal split osteoto- my where the mental foramina mark the anterior osteoto- my line as described for the correction of edentulous man- dibular prognathism (Obwegeser, 1968 a), and surgery in the chin region involves either a one-, two- or three-step augmentation genioplasty (Obwegeser, 1957, 1958, 1974, Neuner, 1965). Quite often, the mandible exhibits an ante- rior horizontal deficiency. This region must also be cor- rected for aesthetic and occlusion reasons. This deficiency is corrected by a vertical osteotomy either in the symphy- seal region or laterally. Moreover, an onlay of lyophilized cartilage slices to correct the contour might be desirable. It is almost self-evident that presurgical orthodontic treat- ment becomes near-indispensable if there is no other way to obtain a good occlusion. The advantage of presurgical orthodontics is that after the extraction of one premolar tooth on each side, a simultaneous correction of the pro- trusion of the lower anteriors can also be achieved. This obviously means simplification of surgery. There will be one tooth-bearing segment less. Intermaxillary fixation be- comes easier too, because now the teeth of the anterior segment can be used for this purpose. The situation in the maxilla must also be evaluated and in- cluded in the treatment planning. In cases of total or ante- rior maxillary vertical excess or dorsal maxillary vertical deficiency, as in the case of early childhood ankylosis, the lengthening of the mandibular base must be followed by repositioning of the maxillary base. This applies especially to cases of micromandibulism associated with an open bite. On the one hand, the length of the lip and the necessi- ty for a certain exposure of the upper teeth limit the crani-
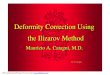
Fig. 1 Diagramatic illustration of a procedure for lengthening the horizontal ramus and increasing the height of the ascending ramus by means of an osteotomy just anterior to the angle, based on the angle-ostectomy procedure described by the author (Obwegeser 1964). The lateral cortex is osteotomized as a decortication proce- dure and kept separately, as a free fragment, in antibiotic solution, or left pedicled on the masseter muscle. The contents of the man- dibular canal are freed. After completion of this procedure on both sides of the mandible the osteotomy is performed somewhere an- terior to the angle. Now the mandible can be moved forward and downward depending on the planned position of the maxilla. The lateral cortical plate is reposit ioned and fixed to bridge the buccal surface defect. Fresh autogenous or frozen allogenic bone is used to bridge the lingual defect.
al repositioning of the maxilla in the anterior region. On the other hand, there are also limitations to the caudal re- positioning of the dorsal maxillary region after bilateral ankylosis surgery. The ascending ramus is short and, after a sagittal split osteotomy, its ligaments limit the caudal repositioning. To lengthen the ramus in such cases one might have to opt for a different osteotomy with an osteo- tomy line anterior to the angle to allow sufficient length- ening of the ramus. We have previously used such a proce- dure (Fig. 1) for the correction of a severe open-bite defor- mity (Obwegeser 1964) and cases of severe antomandibu- lism (prognathism). The sequence of the various steps of the operation is as follows: If repositioning of the maxilla is necessary, then it is performed first. The maxilla is brought to the desired position by means of a splint which has been constructed prior to surgery, on the operation models mounted ac- cording to the facebow-registered position of the TMJ. It is then fixed by means of osteosynthesis. Two suspension wires, one on each side of the piriform aperture, are insert- ed. The vestibular incisions are sutured. Surgery on the mandible begins with the extraction of the first premolar on each side followed by the horizontal osteotomy, 5 mm below the apices and mobilization of the anterior segment. It is, of course, possible to perform an additional vertical osteotomy of the anterior segment to fit it to the upper dental arch, by dividing it medially with or without tooth extraction and appropriate ostectomy in the extraction area, as required. Now, one has an idea of the amount of bone left to per- form a one- or much more preferable, a two- and rarely a three-step sliding osteotomy of the chin. The osteotomized segments must be muscle-pedicled. A 5 mm bone bridge should be maintained between the alveolar and genial seg-

2 5 0 J. Cranio-Max.-Fac. Surg. 16 (1988) H. L Obwegeser
Fig.2a Fig.2b
Fig.2 a and b Schematic presentation of the procedure for correcting bird-face deformity by lengthening the mandible in the retromotar and chin regions by means of an extended sagittal split osteotomy and a two-step augmentation genioplasty respectively, combined with maxillary elevation in the anterior region, The reposit ioned segments are fixed in position by means of wire or screw osteosynthesis, This procedure is performed subsequent to the extraction of a premolar on each side of the mandible and orthodontic retraction of the lower an- terior teeth.
ments (Fig. 6). Next a long-surface sagittal split procedure is performed on either side. Most commonly, a vertical osteotomy through the middle of the bone bridge is per- formed to correct horizontal deficiency of the mandibular base and the dental arches. In cases where, due to a two- step sliding osteotomy, no bone bridge can be maintained, the necessary horizontal correction of the dental arch is achieved by means of a vertical osteotomy in the premolar area where the bicuspids have been extracted. The next step after completion of all osteotomies is the reposition- ing of the segments. All segments must be so loose that they can easily be repositioned with a pair of tweezers to the position where they are to be fixed. First the occlusion is adjusted and fixed, then follows the intersegmental fixa- tion by means of osteosynthesis. It is often desirable to place cancellous bone on the genial steps and between the sagittally split bone fragments if in- dicated. We ourselves use homologous frozen cancellous bone for this purpose. We also use the same material for interpositional grafting of the spaces which result from the necessary maxillary repositiouing, thus diminishing the need for autologous rib or iliac graft material. We have long abandoned the use of freeze-dried bone. Instead, for over 20 years we have used non-lyophilized deep-frozen homologous bone very satisfactorily. This latter bone is prepared by rinsing freshly harvested bone in an antibiotic solution and then immediately deep-freezing it in a suit- ably sealed container. It is again immersed in an antibiotic solution immediately before use. It is self-evident that test- ing the donor for possible viral or bacterial infection has to be carried out, If necessary, horizontal contour deficiencies can be cor- rected by inserting laminated lyophilized cartilage either simultaneously or later.
Variations of the Surgical Approach
Presurgical orthodontics and lengthening of the mandible by surgery in the retromolar and chin regions and simul- taneous maxillary elevation (Fig. 2)
Case 1 (Fig. 3): Post-traumatic bilateral partial ankytosis occurred at the age of 4. The ankylosis was freed at the age of 12. Intensive post-surgical treatment could not pre- vent the development of a slight open bite (Fig. 3 a). Or- thodontic treatment was commenced at the age of 15~ years. After the completion of growth at the age of 17 years, harmonious upper and lower dental arches were re- stored after the extraction of a lower premolar on each side (Fig. 3 b). They could then be placed into proper oc- clusion by surgery (Fig. 3 c). Since it was a partial ankylosis only, which only arose at the age of 4 years, it had not led to an extreme form of micromandibulism and retrogenia (Fig. 3 d and e). However, the chin region was poorly deve- loped, and an anterior maxillary vertical excess was pre> ent (Fig. 3 f, left). The surgical procedure for correction of the lower facial skeleton was a combined osteotomy of maxilla and mandible according to the drawings in Fig. 2. A 6 mm maxillary elevation was achieved by rotating the maxilla cranially. Mandibular advancement surgery by means of the extended sagittal split osteotomy was limited by the occlusion to 10 mm. The two-step advancement ge- nioplasty gave an additional 15 mm, and the rotation of the mandible has, of course, contributed to the profilo- plasty in the chin region. Although the immediate and one year postoperative ce- phalograms (Fig. 3f), and the facial photographs 12 months after surgery (Fig. 3 g and h) and the final occlu- sion (Fig. 3 c) show a rather satisfactory outcome, the ex- tent of the possible advancement of the mandible seemed to be less than one would have wished. Possibly, some loss of space of the extraction gap caused by partial anterior drifting of the posterior teeth might have taken place. This means that presurgical orthodontic treatment ought to produce the greatest possible incisor overjet as a basis for the surgical intervention. The extraction gaps of the pre- molars should be closed in an anterior-posterior direction. In extreme cases, the additional extraction of two incisors is certainly indicated. An additional caudal rotation of the maxilla in its posterior region would bring about further advancement of the chin prominence. However, down-

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 251
Fig. 3 a-h A 17-year-old female patient exhibiting medium-grade micromandibulism and a low-set maxilla after partial bilateral ankylosis at the age of 4. The correction of the deformity has been carried out according to diagrams 2 a and b.
Fig.3a
Fig. 3 a-c ment (c).
Fig.3b Fig. 3 c
Occlusion at the beginning of treatment planning (a) after preliminary orthodontic treatment (b) and one year after surgical treat-
Fig.3d Fig.3e
Fig.3d and e demonstrate patient's pre- operative anterior and lateral views.
Fig.3g and h The anterior and lateral views of the patient taken one year postop- eratively show clearly the enormous im- provement of the chin-throat region and the profile of the lower facial third.
Fig.3g Fig.3h

252 J. Cranio-Max.-Fac. Surg. 16 (1988) H.L. Obwegeser
Fig.3f Lateral cephalograms obtained preoperatively, immediately postoperatively and one year after surgery.
1 i" G
I
Fig.4a Fig.4b
i' ]
Fig.4a and b Schematic illustration of the bird-face correction in lateral and anterior views by surgical retropositioning of the lower anteri- or segment after the extraction of a tooth on each side of the mandible, combined with lengthening of the mandible in the retromolar and chin regions by means of an extended sagittal split osteotomy and two-step augmentation genioplasty respectively, without maintaining a bone bridge between the lateral parts of the mandible. Maxillary elevation surgery is performed simultaneously.
ward rotation of the maxillary molar region may be limi- tared by the restricted possibility of lengthening the ramus in any case, but it is particularly so in juvenile ankylosis c a s e s .
Combined maxillary elevation and mandibular sagittal split advancement with genioplasty, extraction of the first premolars and retropositioning of the lower anterior seg- ment without maintaining an anterior bridge of mandibu-
lar body between the osteotomized lateral segments of the mandible (Fig. 4). Case 2 (Fig. 5): The major differences between our stan- dard method for correction of bird-face deformity and our earlier approach (Obwegeser, 1971, 1973) to this problem is the additional retropositioning of the anterior alveolar segment of the mandible and the widening of the mandibular body in the symphyseal area. This helps over- come the occlusal obstruction encountered in advancing

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 25 3
Fig.5c
Fig.5a Fig.5b Fig.5d
Fig. 5 a-i A 23-year-old female patient exhibiting an anlagednduced bird-face deformity. The correction has been carried out according to the operation technique illustrated in diagram 4a and b. The preoperative pictures (a and b) show a long lower facial third caused by the low-set maxilla and the enormous retrusion of the chin. Although during surgery one premolar has been extracted on each side of the mandible, the anterior pre- and postoperative occlusal views (c and d) exhibit no major differences. The model planning (el shows, on the left, the preoperative Class I interdigitation in the molar and canine regions. According to the model surgery, one premolar is extracted on each side, the lower anterior segment is repositioned, and the mandible is advanced. Additionally, the maxilla is elevated by 7 mm anteriorly and 5 mm posteriorly. The postoperative orthopantomogram (f) shows clearly the osteotomies performed. The lateral head films (g) obtained preoperatively, immediately postoperatively and one year after surgery show the changes of the profile brought about by altering the size, position and the relationship of the bases of the facial thirds. The surgically created profile is in accordance with the skeletal alterations (h and i).
the mandible and thus enabling us to carry out the retro- molar lengthening of the mandible to the extent desired. Whenever possible, one should strive for a two-step ad- vancement genioplasty because by this means a 15 mm ad- vancement of the chin prominence can be achieved and the retrusive chin of the bird-face deformity can be better cor- rected. In cases where the distance between the dental apices and lower border of the chin is short, there would be only a couple of millimetres of bone below the apices after a two-step genioplasty. Therefore, it sometimes happens that no anterior bone bridge can be maintained after com- bined repositioning of the lower anterior segment and two-step genioplasty. In such a case the vertical line of os- tectomy of the extraction gaps meets the horizontal osteo- tomy line of the genioplasty (Fig. 4). Now the mandible has been sectioned into many segments and there follows the laborious process of putting the segments together. The lateral and anterior tooth-bearing segments are brought into proper occlusion by means of intermaxillary fixation. The remaining mandibular segments are fixed to each other, on the one hand by way of dental splinting and on the other hand by means of osteosynthesis. Whenever possible, we prefer wire osteosynthesis for the genioplasty and the anterior tooth-bearing segment areas. If necessary, we use plate osteosynthesis in addition. In the area of the sagittal split osteotomy we use either screws or wire or
plate osteosynthesis. First and foremost, the maxilla must be fixed in the planned position prior to the mandibular osteotomies. The procedure described above is illustrated by case 2 (Fig. 5 a-i). The case was operated on by my co-worker Dr. HadjiangheIou after joint planning. It deals with an an- lage-induced micromandibulism and retrogenia. The lower and midface are long (Fig. 5 a and b), and in combination with the retrusive lower facial third constitute a severe aes- thetic disharmony. Although there is no exact interdigita- tion, the dentition is class I in the molar region (Fig. 5c). The upper dental arch does not permit the advancement of the mandible unless the lower anterior teeth are retracted. The retraction of the lower anteriors following extraction of the first premolars at the same time corrects the protru- sion of the lower anteriors. This procedure is but only a consequence of the previously stated principle Nr. 7 if fol- lowed strictly. This way, the mandible can be advanced at least by the width of a premolar and the retromolar lengthening can be accomplished. This is illustrated clearly by the model surgery (Fig. 5 e). The two-step genioplasty to advance the available chin prominence by 15 mm did not allow the maintenance of a bone bridge between the lateral mandibular segments. The maxilla was elevated by 8 mm. Additional advancement of the chin was achieved by the closing rotation of the mandible. The orthopantomogram (Fig. 5 f) obtained 7 weeks after

254 J. Cranio-Max.-Fac. Surg. 16 (1988) H.L. Obwegeser
Fig.5e
surgery reveals, on the one hand, the very little distance be- tween the apices of the canines and the osteotomy line of the two-step horizontal genioplasty, and on the other hand that the vertical osteotomy lines, which run through the extraction gaps of the premolars, intersect the horizontal osteotomy lines of the genioplasty. Moreover, the all- round interosseous stabilization in the anterior region can also be seen. A comparison of the lateral cephalograms obtained pre-, a few days post-operatively and one year later (Fig. 5 g) and the photographs taken a year after surgery (Fig. 5 h-i) de- monstrate the efficacy of this procedure. Fig. 5 d shows the occlusion of the patient one year after surgery. It is a pity that frequently there is a lack of adequate presurgicaI orthodontic treatment.
Fig.5f
Fig.Sg

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 255
Fig.Sh Fig. 5i
Fig.6a Fig.6b
Fig. 6a and b Lateral and anterior views of the schematic illustration of our standard method for correcting bird-face deformity. Extraction of one premolar on each side and retropositioning of the anterior segment, lengthening of the mandible in the retromolar region and two- step advancement genioplasty, with the maintenance of an anterior bone bridge and expansion of the mandibular arch by means of sym- physotomy with or without simultaneous maxillary elevation.
Lengthening of the mandible in the retromoIar region and two-step advancement genioplasty and retropositioning of the anterior segment with the maintenance of an anterior bone bridge and expansion of the mandibular arch by means of symphysotomy (Fig. 6) Case 3 (Fig. 7): Of course, it would be easy and convenient if, for the correction of all the various typical anomalies, a relevant operation technique could always be applied without the need to adapt it to the particular case. This is possible in some forms of malformations. The method of choice for correcting symmetrical bird-face deformity (Fig. 6) is demonstrated by the following operation tech- nique as used in case 3 (Fig. 7 a-m). It is a case of anlage- induced micromandibulism. At the age of 3 (Fig. 7 a) the child exhibited merely a retroposed mandible with a well-
marked chin prominence but not the real micromandibu- lism with the characteristic profile of bird-face deformity. At maturity, mother (Fig. 7 a) and daughter (Fig. 7 b and c) exhibited nearly the same profile. A characteristic micromandibulism with retrogenia was present. Compared with the upper face, the development of the midface was satisfactory and the lower facial third was not too deep. Thus, no long-face condition existed as is often seen in the bird-face deformity. The occlusion was class II in the molar region, and there was a missing pre- molar on each side of the maxilla (Fig. 7 d and e). The characteristic protrusion of the lower anterior teeth is re- vealed by the side view of the occlusion and the lateral ce- phalogram (Fig. 7 k, left). Since there is a satisfactory rela- tionship between the middle and upper facial thirds, only

256 J. Cranio-Max.-Fac. Surg. 16 (1988) H. L. Obwegeser
Fig.7a Fig.7b
Fig.7d
Fig.7c Fig.7e Fig. 7 a-m A 33-year-old female patient presented with anlage-induced bird-face deformity. Correction was accomplished according to the illustrations in Fig.6. At the age of 3 (a) the mandible of the patient still possessed a good form. The mother, as an adult, exhibited the same anlage-induced micromandibulism as did the patient. The appearance of the patient (b 4-c) reveals a good vertical relationship of the facial thirds and a clear three-dimensional micromandibulism producing the picture of a typical bird-face deformity. The preoperative occlu- sion (d and e) does not allow mandibular advancement despite the distocclusion in the molar region. Obviously, the early extraction of one premolar on each side of the maxilla must have taken place. The model surgery (f) demonstrates the surgical procedure in the occlusal re- gion. g and h show the occlusion two years after surgery. The orthopantomogram (i) obtained two months after surgery hardly shows evi- dence of the vertical osteotomies. The lateral cephalograms (h) obtained preoperatively, immediately postoperatively and two years after surgery show the alteration of the mandibular base. Massive bone apposit ion has taken place in the region of the genioplasty where frozen bone only was used to fill in the space created by the step. The appearance of the patient (I and m) two years after surgery is in accordance with the planned skeletal alteration brought about by this one intervention.
mandibular surgery had to be performed. The planning had also to take into account the rather tall slender-waist- ed body morphology of the patient. Thus, the problem here was to achieve maximal lengthening of the mandible by maintaining a good occlusion and without noticeable change in height of the lower face. The discrepancy be- tween occlusion, position and length of mandible made it clear that one premolar had to be sacrificed on each side
and the anterior segment be retropositioned in order to achieve adequate mandibular advancement. According to the model surgery, a fairly good occlusion could be achieved if there was some expansion of the mandibular arch (Fig. 7 f). The drawing of the operation plan (Fig. 6) shows the retro- positioning of the anterior segment after extraction and ostectomy in the regions of the first bicuspids, two-step

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 257
Fig.7g
Fig. 7 f
Fig. 7h
Fig.7i
Fig.7k

258 J. Cranio-Max.-Fac. Surg. 16 (1988) H.L. Obwegeser
Fig.71 Fig. 7m
advancement genloplasty and bilateral extended sagittal split osteotomy for lengthening the mandible in the retro- molar and chin regions. Further, it indicates the preserva- tion of a subapical anterior bone bridge which had to be sectioned vertically in the symphyseal region to achieve the expansion of the dental and mandibular arches. Deepfroz- en homogenous cancellous bone was used to graft the os- teotomy spaces. Interosseous stabilization was achieved by means of wire osteosynthesis. Additionally, intermaxillary fixation was maintained for six weeks. The postoperative picture of the occlusion (Fig. 7g and h) shows the im- provement of the angulation of the lower anterior teeth with no sign of extraction gaps. The orthopantomogram taken 2 months after surgery reveals the defect between the two finger-like processes of the left anterior bridge of the mandibular body created by expanding the horse-shoe of the mandible after symphysotomy. It also shows the short distance of the apices from the horizontal osteotomy line (Fig. 7 i). It also reveals that the two muscle-pedicled fragments of the chin, used to advance the chin promi- nence, were thin. The lateral cephalograms (Fig. 7 k) show the skeletal findings in the patient before, two weeks and 2 years after surgery respectively. A comparison of these shows that two years after surgery no loss of profile con- tour and bone has occurred, nor in the chin region. Hence, no additional advancement genioplasty was needed. There was rather well defined osteogenesis in the area of the steps where bank bone chips had been placed to compen- sate for the large step. The final photographs of the pa- tient (Fig. 71 and m) show the result of the correction.
Correction of asymmetrical bird-face deformity by shorten- ing the unaffected side of the mandible combined with the normal procedure for correcting a symmetrical type com- bined with the rotation of the lower facial half (Fig. 8) Case 4 (Fig. 9): The correction of asymmetrical bird-face deformity is more difficult by far than the correction of the symmetrical type. In a way it is equivalent to the cor- rection of an unilateral hemifacial microsomia. First we transform the asymmetrical malformation into a symmet-
rical one. The actual correction is facilitated by this means. The same principles of planning the correction of a sym- metrical bird-face condition apply to the correction of the asymmetrical type. We must retract the protrusive anterior segment, no matter whether the unaffected side is retropo- sitioned or not. Otherwise, the dentition poses an obstruc- tion to the advancement of the mandible. The anterior seg- ment is set back only on the unaffected side and that side is additionally shortened by ostectomy. After detatching the chin prominence this creates a sym- metrical but retropositioned mandible. Now the whole mandible can be advanced and lengthened by means of ex- tended bilateral sagittal split osteotomies (Fig. 8). The chin prominence is repositioned anteriorly and laterally by means of either a one-step or two-step genioplasty depend- ing on the amount of bone available between the dental apices and the lower border of chin. A one-sided bird-face deformity is almost always associat- ed with a vertical growth deficiency which affects the as- cending ramus and maxilla on the affected side. Therefore, in addition to restoring the symmetry of the mandibular arch and bilateral lengthening of the mandible, we must also correct this deficiency. To effect this, we rotate the lower half of the facial skeleton downwards and forwards on the affected side, after slightly elevating the other side; it is simultaneously repositioned in the middle of the face in the way that we have described for the correction of hemifacial microsomia (Obwegeser, 1974). First and fore- most, of course, the maxilla must be fixed in the desired position prior to all other osteotomies. The gaps created after lowering the maxilla must be bone-grafted by using either frozen bone or iliac graft from the patient. The mandibular osteotomies then follow. These always include a one-step or two-step advancement genioplasty and bila- teral sagittal split osteotomies. The model planning must take into account the reposition- ing of the maxilla. The extent of maxillary rotation is as- sessed clinically by comparing the discrepancy in height of both sides. The affected and thus shorter side always shows crowding of the teeth. The ones which cannot be

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 259
/
Fig. 8 a Fig. 8 b Fig. 8 c
/ ~ ! / /
Fig. 8 a-c Schematic illustration of the correction of asymmetrical bird-face deformity: (a) demonstrates the osteotomies used to shorten the normal side of the mandible by the width of a premolar, after that, repositioning of the shorter side to the normal half to create a symmet- rical bird-face deformity and then the same correction as in the symmetrical case combined with the rotation of the whole lower facial half; (b) shows the result after the rotation of the lower facial half and reposit ioning and osteosynthesis of the mandibular segments. Second in- tervention (c) for performance of a two-step advancement genioplasty and lyocartilage onlays to augment the chin and to widen the contour of the mandible.
placed in their proper angulation to the jaw base are either removed long before surgery or during the operative procedure. The unaffected and thus longer side of the mandible is shortened by extracting a premolar and re- tracting the anterior alveolar process after ostectomy through the extraction gap, to make it equal to the shorter side. Then and only then, the lower dental arch is brought into occlusion with the upper one. Case 4 illustrates a typical case of asymmetrical bird-face deformity exhibiting a right-sided partial ankylosis which occurred at the age of 2 years. The chin shows a deviation to the short side, and the unaffected side appears to be flattened (Fig. 9 a). The occlusal plane is tilted markedly upwards on the affected side (Fig. 9 b). The retroposition of the chin prominence is not as extreme as in the bilateral type case. The picture of the preoperative occlusion reveals only the presence of asymmetry, but not the shortening and retroposition of the dental arch on the affected side. This is due to the extraction of a premolar on each side of the maxilla, and a lower incisor, years previously. The models show that the dental occlusion does not permit the advancement of the mandible. The model surgery (Fig. 9 f) shows the planned repositioning of the maxilla and mandi- ble after the extraction of the lower left premolar com- bined with a vertical osteotomy in the extraction area. The changes in the shape of the mandible are reproduced by the orthopantomograms (Figs. 9 g and h) obtained preop- eratively and immediately after surgery. The chin frag- ment was sectioned in the middle to achieve symmetry by shortening the longer end. The orthopantomogram ob- tained a year after surgery (Fig. 9 i) shows the nearly sym- metrical form of the surgically-altered mandible. The lateral cephalograms (Fig. 9 k) obtained preoperative- ly, immediately after second surgery and three years after primary surgery, show clearly the changes in the facial skeleton. A year after the first operation, a supplementary two-step augmentation genioplasty was performed. The picture of the postoperative occlusion (Fig. 9 e) shows the difference compared with the preoperative one. Apart
from shortening of the lower left dental arch by the width of a premolar, only the angular correction of the lower anterior segment is noticeable. This is also particularly ob- vious on the postoperative lateral cephalograms.
Postsurgical Treatment and Supplementary Contour Cor- rection
The postsurgical treatment includes the same procedures used in treating all other malocclusions. The intermaxil- lary fixation is maintained for 6 weeks. Then, after one or two more weeks, normal mouth opening should be at- tained. Postoperative orthodontic treatment is due to be com- menced by this time too. Of course, it would be desirable for patients undergoing orthognathic surgery to have fur- ther orthodontic treatment to achieve occlusal perfection. Unfortunately, this is possible only in a few cases. This is because, on the one hand, there are apparently only a few orthodontists capable of preparing high-grade malocclu- sion cases for surgery and, on the other hand, many pa- tients live remote from the place of treatment. Conserva- tion treatment with definitive bridge-work construction should be postponed for at least one year. Osteosynthesis plates must be removed after six months. We do not remove osteosynthesis wires unless they create a problem. Horizontal contour corrections of the mandi- ble are occasionally desirable. This we achieve by means of laminated lyocartilage onlays. Even the chin prominence can be augmented by means of lyocartilage onlays supple- mentary to the two-step advancement genioplasty if neces- sary. Due to bone apposition on the steps, a second pedi- cled advancement genioplasty can also be performed suc- cessfully as seen in the final lateral cephalograms of some of the cases. Generally, these corrections are performed in a second surgical session. Although bird-face patients ex- press a strong wish for a pronounced chin, they often re- ject a second operation even if it would serve this purpose.

260 J. Cranio-Max.-Fac. Surg. 16 (1988) H. L. Obwegeser
Fig.ga Fig. 9b
Fig. 9d
Fig.gc
Fig.9e Fig.9f
Fig. 9 a-n A 24-year-old mate patient exhibiting an asymmetrical bird-face deformity caused by a partial ankylosis of the right TMJ at the age of 2. Correction was achieved according to the operation technique illustrated in Fig. 8. a-c show the typical deformity present in the asymmetrical bird4ace deformity with a reduced facial height on the shorter side. d and e demonstrate a comparable view of the pre- and postoperative occlusion. The model planning (f) shows the operative procedure corresponding to the diagramatic illustration, shortening of only one side, advancement of the whole mandible and rotation of the lower facial half. The orthopantomograms obtained preoperatively (g), immediately postoperatively (h) and two years after surgery (i) disclose clearly the transformation of the asymmetrical mandible into a nearly symmetrical one and the rotation of the lower facial half too. Cephalograms (k) obtained preoperatively, two years postoperatively immedi- ately after supplementary genioplasty and 3 years after the first intervention show the profile of the skeletal alteration. A normal appearance results (I-n) from the surgical intervention.
Supplementary Rhinoplasty
Many cases of so-called bird-face deformity exhibit a no- ticeably prominent, curved nose in addition to microman- dibutism. It is the projecting big nose combined with the retropositioned mandible and the retrusive chin which constitute the simulation of a bird-face. The nose, there- fore, should also be reduced to obtain an aesthetically per- fect profile. Intubation for general anesthesia and possible anterior maxillary repositioning make it impossible to per- form a rhinoplasty simultaneously. Besides, there are no-
ticeably very few patients who like to add rhinoplasty to their orthognathic surgery. Rhinoplasty is performed only after adequate correction of the mandibular anomaly has been attained. The ideal is to combine rhinoplasty with the supplementary genioplasty or contour corrections.
Results
The results of correcting the bird-face deformity accord- ing to the surgical procedures described are extraordinari-

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 261
Fig.9g
Fig.9 i
Fig.gh
ly satisfactory. The approach advocated makes extraoral incisions unnecessary. This surgical approach always pro- duces a major if not a complete correction in one go. We have learned that the patients in question express a real need for a symmetrically positioned, wellrpronounced chin prominence and that they are not satisfied with average re- sults. Thus, in some cases a supplementary surgical inter- vention for further advancement of the chin and lateral augmentation is performed to achieve a perfect result. We never use autologous bone grafts as onlays for that pur-
pose. It undergoes an unforeseeable amount of resorption and only very rarely produces a pleasing chin form. We learned early on that "cortical bone shrinks like a mushroom in the sun and cancellous bone melts away like an ice cream when used as onlays for contour correction". Naturally, postoperative oedema occurs extensively in the whole operation area and particularly the chin region. Thus, the immediate postoperative result is quite different from the late result. Generally, a stable result is only at- tained one year after surgery. This applies to the possible

2 6 2 J. Cranio-Max.-Fac. Surg. 16 (1988) H. L Obwegeser
Fig.9k
Fig.91 Fig.m Fig.9n
loss of contour in the chin region due to resorptive pro- cesses affecting the advanced lower border, as well as to a possible relapse of the mandibular advancement produced by means of sagittal split osteotomies. Eventual changes in the lyocartilage onlays used during the first or second sur- gical session may also be involved.
Discussion
Previously, we had not considered repositioning the lower anterior segment to achieve maximal advancement of the mandible for correction of the bird-face condition. The extent of mandibular advancement was dictated by the ex-

Variations of a Standard Approach for Correction of the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 263
\
Fig. 10 Diagram of our previous method of correcting bird-face deformity without retropositioning of the mandibular anterior seg- ment: Lengthening of the mandible in the retromolar and chin re- gions by means of an extended sagittal split and two-step advance- ment genioplasty respectively (from H. Obwegeser, Deformity of the Jaws. In: d. Mustarde (ed.): "Plastic Surgery in Infancy and Child- hood". Livingstone, Edinburgh (1971) 60).
Fig. 11 Diagram of our previous method of correcting bird-face deformity combined with retropositioning of maxillary protrusion but without retropositioning of the mandibular anterior segment (from H. Obwegeser, Fortschritte und Schwerpunkte der orthopadischen Kiefer-Gesichtschirurgie. In: K. Schuchardt und G. Pfeifer (eds.), Fortschritte der Kiefer- und Gesichtschirurgie, Vol. 21. Thieme, Stuttgart (1976) 55).
isting dentition. Thus, we lengthened the mandible only in the retromolar and chin region as far as the dentition would allow (Fig. 10). Relative to the degree of retrogenia and the extent of advancement genioplasty, surprising pro- file corrections were achieved despite occlusal limitations. The advanced chin fragment was not pedicled. To reduce the amount of resorption in this region, an lilac cortical graft was placed underneath the advancement genioplasty in one case. Surprising results have been achieved by combining this procedure with the correction of maxillary protrusion per- formed either simultaneously (Obwegeser, 1976) or prior to it (Fig. 11). The labiomental fold had always posed a real problem in these cases. Unfortunately, the excellent early results (Obwegeser, 1976) of the case cited had been considerably negated by resorptive processes in the chin region and partial relapse of the mandibular advancement. The procedure did not utilize the present surgical possibilities. At that time, the multistep advancement genioplasty was performed without pedicling the fragments. Thus we had to accept the possibility of contour losses caused by re- sorptive processes. A retrospective study of our patient population (Wegener, 1971) demonstrated a maximum re- sorption of 50 %, the mean being only 14,3 %. Resorption loss was only partially substituted by connective tissue. For years now we have again been performing the pedicled advancement genioplasty. Of course, only parts of the genohyoid muscle and the digastric muscle respectively are left attached, never the platysma. In doing so, the resorp- tion amounted only to about 10 %. The adequate mobilization of the overlying tissues to ac- commodate the lengthening of the mandible and chin did not pose any problem. It is clear that the lateral and cau- dal periosteum of the mandible must be raised to perform the extended sagittal split osteotomy and the advancement genioplasty. By this means adequate soft tissue advance- ment is achieved. In the chin region, the relaxation of the
periostium by additional incisions is almost always neces- sary in extreme cases. We have again long since given up detaching the musculature from the chin area as suggested by Steinha'user (1973). We rarely even weaken it. In our experience possible relapse of the advancement of the mandible or prominence of the chin does not seem to de- pend on these muscles. The planning of our cases is based exclusively on our principle: "First the profile, then the occlusion". This means that the desired profile is determined according to the principles of pictorial art. Of course, some cephalo- metric analysis is indispensable for that purpose. The repo- sitioning of the jaw segments to correspond to the desired profile follows naturally. Then comes the operation plan- ning. Preliminary orthodontic treatment poses no problem to the experienced orthodontist, who has but to take the planning principles into account. Thus the cooperation be- tween orthodontist and surgeon gives mutual satisfaction and both may be equally proud of the results. Except for the temporomandibular joint, the surgical access to the facial skeleton is exclusively via intraoral inci- sions. For osteotomies in the maxillo-mandibular region, the surgeon needs no extraoral incisions. Unfortunately, extraoral incisions for the correction of a bird-face defor- mity are frequently used. The symmetrical bird-face deformity with true microman- dibulism exhibits a reversed similarity to true macroman- dibulism. The one is too small in all three dimensions while the other is too big in all aspects. It is, therefore, al- most self-evident that both, macromandibulism and mic- romandibulism, require the same osteotomies at the same sites in the mandible either to reduce the mandible or to increase it. Indeed we have applied the same osteotomies for correction of macromandibulism (Fig. 12)(Obwegeser, 1976). Other operation techniques for correcting the bird-face deformity could yield equally impressive results. In certain cases of so-called mandibular deficiency, notable correc-

264 J. Cranio-Max.-Fac. Surg. 16 (1988) H. L. Obwegeser
Fig.12a Fig.12b
Fig. 12 Diagram illustrating author's technique of correcting macromandibulism. The same operation sites and osteotomy techniques are used to correct micromandibulism. Only the repositioning of the segments takes place in a reverse direction (from Obwegeser, 1976).
tion can be achieved only by combined maxillary elevation and one-step advancement genioplasty and complementary closing rotation of the mandible (Bell, 1980; Epker and Fisch, 1983): Naturally, this procedure cannot produce a satisfactory correction of the real micromandibulism such as arises following early childhood ankylosis. It is better to remove a premolar from each side of the mandible in addi- tion to this procedure. This procedure can yield excellent results in medium-grade cases of micromandibulism (Sinn, 1980). The extreme forms of micromandibulism and retrogenia can also be corrected by means of the vertical (Bruhn, 1939; Converse, 1963; Ginestet, 1964) and step-shaped (von Eiselsberg, 1906; Pichler, 1927) osteotomies of the horizontal ramus - best just anterior to the mental forami- na - combined with advancement of the anterior segment, necessitating the interpositioning of bone for the bridging of osteotomy defects (Ginestet, 1964). Merville (1970) has published excellent results following correction of sym- metrical as well as asymmetrical cases of bird-face defor- mity by lengthening the body of the mandible. Naturally, these procedures necessitate bone grafts from the iliac crest. Gaps are created in the dental arches which necessi- tate dental bridgework as a consequence. We have also applied the above procedure in our unit, in several cases. Our co-worker Dr. Hadjianghelou will re- port on these. We will thus have comparable results for the two different ways of correcting bird-face deformity.
Conclusion
The adherence to clear planning principles appears to be very important in surgical correction of the so-called bird- face deformity. These principles helped us to develop ope- ration techniques which seem to correct the anomaly logi- cally. Besides the form, size and position of the body of the mandible, the planning must also consider the number of teeth which can be accommodated in the mandible. Reducing the number of the teeth creates room for man- dibular advancement: The additional lengthening of the mandibular base in the chin region creates not only a
mandible possessing a normal form and length, but a good occlusion is attained too. The planning must always con- sider the dentition and position of the maxillary base. Whether the operation is performed with or without preli- minary orthodontic treatment, the major precondition to the achievement of a result with an excellent occlusion and profile is the creation of enough room for mandibular advancement. Generally, a good result can be achieved in one surgical session by utilizing the described variations of the princi- pal operation technique. Occasionally, supplementary aug- mentation genioplasty is desirable. The correction of an asymmetrical bird-face deformity is facilitated by first making it into a symmetrical one. Based on our planning philosophy and the prevailing os- teotomy procedures, we believe we have developed a standard surgical approach which is adaptable to treat any particular case.
Acknowledgement I wish to thank my co-worker Dr. FiIli and my very good friend Mr. Peter Clarke, from Aberdeen (Great Britain), for their generous help in putting this paper into correct English.
References Bell, W.: Mandibular deficiency. In: Bell, W., W. Proffit, R. White
(eds.): Surgical correction of dentofacial deformities. Sauuders, Philadelphia (1980) 807-842
Bruhn, C., A. Lindemann: Eingriffe bei Progenie und Opisthogna- tie. In: Bruhn, C. (ed.): Chirurgische Gebif~-, Kiefer- und Gesichtsorthopfidie. Handbuch Zahnheilkunde. Vol 4. Bergmann, Miinchen (1939) 52
Converse, J. M.: Micrognathia. Brit. J. Hast. Surg. 16 (1963) 197 von Eiselsberg, A.: Ober Plastik bei Ektropium des Unterkiefers
(Progenie). Wien. Klin. Wochenschr. 19 (1906) 1505 Epker, B., L. Fisch: Surgical orthodontic correction of mandibular
deficiency. Part II. Am. J. Orthod. 8 (1983) 503 Ginestet, G.: Traitement de la micrognatie mandibulaire. Rev. Francl
Odonto-Stomat. 2 (1964) 175 Hofer, 0.: Die operative Behandlung der alveol/iren Retraktion des
Unterkiefers und ihre Anwendnngsm6glichkeit fiir Prognathie und Mikrogenie. Dtsch. Zahn-Mund-Kieferheilk. 9 (1942) 121

Variations o f a Standard Approach for Correction o f the Bird-Face Deformity J. Cranio-Max.-Fac. Surg. 16 (1988) 2 6 5
KiSle, H.: Surgical operations on the alveolar ridge to correct occlus- al abnormalities. Oral Surg., 12 (1959) 277, 413, 5151
Merville, L.: Le Traitement des micromandibulies. Ann. Chir. Plast. 15 (1970) 301
Neuner, 0.: Chirurgische Orthodontie. Schweiz. Mschr, Zahnheilk. 75 (1965) 940
Obwegeser, H. L.: In: Trauner, R., H.L. Obwegeser: The surgical correction of mandibular prognathism and retrognathia with con- sideration of genioplasty. Oral Surg., 10 (1957) 677
Obwegeser, H. L.: Die Kinnvergr6f~erung. Osterr. Zschr. Stomat. 55 (1958) 535
Obwegeser, H. L." Der offene Bif~ in chirurgischer Sicht. Schweiz. Mschr. Zahnheilk. 74 (1964) 668
Obwegeser, H. L.: Operative Behandlung der zahnlosen Progenie ohne intermaxill/ire Fixation. Schweiz. Mschr. Zahnheilk. 78 (1968a) 416
Obwegeser, H. L.: Die Bewegung des unteren Alveolarfortsatzes zur Korrektur von Kieferstellungsanomalien. Part h Dtsch. Zahn/irztl. Zschr. 23 (1968b) 175; Part II: Dtsch. Zahn/irztl. Zschr. 24 (1969) 5
Obwegeser, H. L.: Deformities of the jaws. In: Mustard6, J. (ed.): Plastic surgery in infancy and childhood. Livingstone, Edinburgh- London (1971) 60
Obwegeser, H. L.: Mandibular surgery. Brit. J. Oral Surg. 10 (1973) 251
Obwegeser, H. L.: Correction of the skeletal anomalies of oto-man- dibular dysostosis. J. Max. Fac. Surg. 2 (1974) 73
Obwegeser, H. L.: Fortschritte und Schwerpunkte der orthop/idi- schen Kiefer-Gesichtschirurgie. In: Schuchardt, K., G. Pfeifer (eds.): Fortschritte der Kiefer- und Gesichtschirurgie, Vol 2i. Thieme, Stuttgart (1976) 54
Obwegeser, H., M. Farmand: Unsere Behandlung der Kiefergelenk~ ankylose. Schweiz. Mscbr. Zahnheilk.: 7 (1982) 92
Pichler, H.: Ober Progenieoperation. Arch. Ktin. Chir. 1 (1927) 110 Sinn, D.: Mandibular deficiency in patients with juvenile rheumatoid
arthritis. In: Bell, W., W. Proffit, R. White (eds.): Surgical correc- tion of dentofacial deformities. Saunders, Philadelphia (1980) 833-842
Steinhduser, E. W.: Advancement of the mandible by sagittal ramus split and suprahyoid myotomy. J. Oral Surg. 31 (1973) 516
Wegener, A.: Eine klinische und r6ntgen-cephalometrische Nachun- tersuchung der Ergebnisse der chirurgischen Kinnvorverschiebe- plastik nach Obwegeser. Inaug. Diss. Med. Fakult/it der Univer- sit/it Z/irich, 1971
Prof. H. L. Obwegeser, MD, DMD Im Zelg CH-8603 Schwerzenbach Switzerland