Embed Size (px)
Citation preview

�������� ����� ��
Variations in Clinical Nurse Leaders’ Confidence with Performing the CoreRole Functions
Mattia J. Gilmartin RN,PhD
PII: S8755-7223(13)00188-9DOI: doi: 10.1016/j.profnurs.2013.11.002Reference: YJPNU 800
To appear in: Journal of Professional Nursing
Please cite this article as: Gilmartin, M.J., Variations in Clinical Nurse Leaders’ Con-fidence with Performing the Core Role Functions, Journal of Professional Nursing (2013),doi: 10.1016/j.profnurs.2013.11.002
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT1
Variations in Clinical Nurse Leaders’ Confidence with Performing the Core Role Functions
Mattia J. Gilmartin RN, PhD
Senior Research Scientist
New York University College of Nursing
726 Broadway 10th
floor
New York, NY. 10003
Tel: 212-992-7128
Email: [email protected]
This study was supported by a grant from the American Nurses Foundation/Nurses in Staff
Development. 2010-090, M. J. Gilmartin, RN, PhD, Principal Investigator.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT2
Variations in Clinical Nurse Leaders®’ Confidence with Performing the Core Role Functions
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT3
Abstract
Background: CNL practice, by definition, requires individuals to make career transitions.
CNLs must adjust to their new work role and responsibilities and doing so also entails individual
adjustment. Prior work has not examined the role of individual-level factors in effective CNL
role transition.
Aim: This study contributes to CNL implementation efforts by developing understanding of
personal and contextual factors that explain variation in individuals’ levels of self-confidence
with performing the key functions of the CNL role.
Design and Methods: Data were gathered using a cross-sectional survey from a national sample
of RNs certified as CNLs. Respondents’ perceptions of their confidence in performing CNL role
competencies were measured with the Clinical Nurse Leader Self-Efficacy Scale (CNLSES)
(Gilmartin & Nokes, in press). The CNLSES is a thirty-five item state-specific self-efficacy scale
with established measurement properties that assesses nurses’ perceptions of their ability to
function effectively as a CNL. Demographic data were also collected. Data were analyzed
using a general linear regression model (GLM).
Results: One hundred and forty-seven certified CNLs participated in the survey. Results
indicate that respondents vary in their confidence with performing the nine role competencies
associated with CNL practice. Results from regression analyses also show that respondents’
confidence in their abilities to carry out the core functions associated with the CNL role varied
significantly across geographic region, organizational type and by CNL graduate program model.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT4
Conclusions: The results of this study show important differences in CNLs’ levels of self-
confidence with the core competencies of their role. As a result, it may be important to develop
targeted career transition interventions to gain the full benefit of CNL practice.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT5
Variations in Clinical Nurse Leaders®’ Confidence with Performing the Core Role Functions
Introduced in 2004, the Clinical Nurse Leader (CNL®) is the first new nursing role in
more than thirty years (American Association of Colleges of Nursing, 2007). The goal of the
CNL role is to return expert clinicians to the point of care to strengthen the nursing professions’
contributions to improve the quality, safety and outcomes of health care in the United States. The
hallmark of CNL practice is the management of client centered care and clinical excellence at the
point of care (AACN, 2007; Reid & Dennison, 2012; Ott et al., 2009; Hix, McKeon & Walters,
2009).
Unlike other masters prepared roles in nursing, the CNL is an advanced generalist with
unit-level responsibility. Because of their generalist orientation, the scope of CNL practice
complements that of the front-line nurse manager, on the one hand, and the nurse practitioner
and clinical nurse specialist, on the other (AACN, 2007). Graduate education for the CNL role
extends the direct care skills acquired at the baccalaureate level to build competence in the area
of policy and organizations, outcomes management, nursing leadership and care management
(ANCC, 2007). CNLs are educated to assume responsibility for interdisciplinary care
coordination; managing clinical outcomes, with a particular focus on promoting health and
preventing disease in populations; and implementing clinical quality improvement and risk
management programs within the context of a clinical unit.
To promote the diffusion of the CNL role in both academic and practice settings, the
American Association of Colleges of Nursing (AACN) specified the development of CNL
program curricula; clinical and didactic experiences required for certification as a CNL; and
academic-service partnerships to serve as a mechanism for each partner to initiate the CNL role,
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT6
with the goal of hiring CNL program graduates into formal CNL positions at the partner
organization (Stanley, Hoiting, Burton, Harris & Norman, 2007). The White Paper on the
Education and Role of the Clinical Nurse Leader (2007) outlined these requirements, that also
are described elsewhere (Bartels & Bednash, 2005; Stanley, Hoiting, Burton, Harris & Norman,
2007; Torabeni & Miller, 2008).
Although clinical practicum experiences are a common feature of nursing education
programs, the role transition experience for individuals pursuing the CNL role differ in important
ways from experiences provided in other graduate programs in nursing. Ideally, CNL education
and transition to practice occur within the context of an academic-service partnership (AACN,
2007). The academic-service-partnership model serves to promote CNL role implementation by
aligning academic and organizational goals; each partner is committed to educating and
employing nurses to lead and manage clinical improvement initiatives. CNL students complete
between 400 and 500 clinical contact hours during the program, 300 to 400 of which are
structured as an immersion experience in the CNL role with a dedicated preceptor and a faculty
partner over a ten to fifteen week period (AACN, 2007). During the immersion experience,
students have the option to select a new clinical practice area for the practicum experience as a
means to promote transitions into a new practice area after graduation (Bombard, Chapman,
Dole, Wright, Shippee-Rice & Kasik, 2010).
Prior studies examining the transition experiences of nurses pioneering the CNL role
provide important information regarding organizational factors that promote or hinder the
adoption of the CNL role in clinical settings (Sherman, 2010; Stanton, Lammon & Williams,
2011; Moore & Leahy, 2012; Bombard et al., 2010). Two recent qualitative studies suggest that
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT7
the CNL role is implemented differently across organizations and practice areas (Stanton et al.,
2011; Sherman, 2011).
The purpose of this study is to develop understanding of factors that account for variation
in individuals’ self-efficacy in the CNL role. This study contributes to CNL implementation
efforts by developing understanding of personal and contextual factors that explain variation in
individuals’ levels of self-confidence with performing the key functions of the CNL role.
Understanding differences in CNLs’ levels of self-confidence with the core competencies of the
role will provide important information to develop targeted career transition interventions to gain
the full benefit of CNL practice.
Role Transitions of Clinical Nurse Leaders
CNL practice, by definition, requires individuals to make career transitions that require
adjustment to new professional work roles and responsibilities. Doing so also entails individual
adjustment. Prior research suggests that experienced nurses moving into advanced practice roles
experience difficulty during role transition because they are expected to function at a higher,
more independent, practice level than previously demonstrated in traditional staff nurse roles
(Jones, 2005; Sherman, 2010). More generally, an individual’s ability to build a successful
career is based on her or his ability to transition to increasingly complex work roles (Nicholson,
1984; Ashforth & Saks, 1995).
Work role transitions entail two interdependent adjustment processes: personal
development and role development. Personal development includes cognitive and psychological
changes in knowledge, skills, confidence, and work identity; motivation for feedback to improve
work performance and prior professional socialization experiences. In contrast, role
development is reflected in the design of the job within a specific organizational content.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT8
Managers are typically responsible for attending to the required changes in organizational
systems, structures, reporting relationships, politics, culture and resources needed to promote the
adoption of a new work role (Nicholson, 1984; Edwards, 2008). In sum, the extent to which an
individual is able to successfully transition to a new work role is predicated on personal
characteristics that make her or him well suited for the job, on the one hand, and changes in
organizational content and job design to promote person-job fit, on the other (Ashforth & Saks,
1995; Stephens, 1994; Edwards, 2008).
Self-confidence is an important factor associated with successful role transitions. Self-
confidence is an attitude that enables individuals to have positive, yet realistic, views of
themselves and their situations. Self-confident people trust their own abilities, have a general
sense of control in their lives, and believe that, within reason, they will be able to do what they
wish, plan, and expect (Stakjovic & Luthans, 1998). Prior research establishes that self-
confidence is an important factor associated with a number of important work outcomes
including successful career transitions, job satisfaction, job performance, and voluntary turnover
(Stakjovic & Luthans, 1998; Judge, Erez & Bono, 1998).
Variations in nurses’ self-confidence associated with transitioning into the CNL role is
likely to be influenced by a number of personal and contextual factors. First, because nursing is
a contextually situated practice, prior exposure to a particular clinical problem or practice
situation builds competence and confidence in the ability to respond appropriately to similar
situations (Benner, 2009; Tanner, 2006). Recent analyses of the content of RNs’ daily work
suggest that nurses do not have the time for care planning and coordination activities (Lucero,
Lake & Aiken, 2009; Chow, 2008), lack skills either to assess the quality of care or integrate
evidence into clinical decision making (Kovner, Brewer, Yingrengreung & Fairchild, 2010), or
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT9
work in organizations that have been slow to adopt quality and process improvement techniques
into daily routines (Watcher, 2010). Thus, even though many CNLs are experienced staff nurses,
their exposure to, and confidence with, the core activities of the CNL role may be limited.
Similarly, experience in the CNL role is likely to affect nurses’ self-confidence in their abilities
to perform the role competencies.
Second, educational preparation may affect nurses’ self-confidence with performing the
core functions of the CNL role. CNL program curricula conform to the Institute of Medicine’s
recommendations to promote clinicians’ effectiveness in complex organizational settings
(Committee on the Quality of Health Care in America, 2001). There are currently five
educational entry points for CNL practice. These include a traditional master’s program for
individuals with a bachelor’s degree in nursing, including a small subset of programs offering
master’s credits for a post-BSN residency program; a direct-master’s entry option for individuals
with a bachelor’s degree in another field; RN-MSN program designed for individuals with
associate degrees in nursing; and a post-master’s certificate option for individuals with master’s
preparation in another area of study.
Currently, more than 50 percent of CNLs are graduates of the direct master’s entry
programs, or Model C programs (AACN, 2012). Research on direct master’s entry programs
suggests that non-nurse college graduates successfully develop into advance practice registered
nurses (APRNs) and certified nurse midwives (CNMs) (Pellico, Terrill, White & Rico, 2012).
As noted previously, the care planning, outcomes management and process improvement skills
associated with CNL practice may represent new practice competencies for most CNL program
graduates. Therefore, graduates from the Model C direct graduate entry programs are likely to
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT10
be as confident in their abilities to carry out the core functions of the CNL role as nurses
prepared for the CNL role designed for individuals with a prior nursing education.
Third, organizational context may shape individuals’ perceptions of their ability to
perform the CNL role competencies. According to the AACN, more than 200 health care
organizations in the United States have partnered with schools of nursing to adopt the CNL role
(AACN, 2012). The CNL role has been implemented in a variety of settings, including for-profit
and not-for-profit hospitals, and most notably, Veteran’s Health Administration health system
(Ott, Haddock, Fox, Shinn, Walter, et al. 2009; VA Strategic Plan, 2009),
Differences in organizational ownership, mission and strategy, including the maturity of
quality improvement programs (Watcher, 2010) and nursing practice models are likely to shape
the environment for CNL practice that, in turn, will influence nurses’ perceptions of their ability
to perform the core functions of the CNL role. Thus, CNLs’ perceptions of their confidence with
carrying out the role competencies are likely to vary by organizational context.
Finally, geographic location may also influence nurses’ perceptions of their confidence
with carrying out the CNL role functions. CNLs from regions with a larger concentration of
CNL programs and organization that have adopted the role are likely to be more confident in
their abilities to function in the CNL role because there is a community of practice for learning
and consultation.
Design and Methods
I gathered cross-sectional survey data from a national sample of registered nurses who
passed the national CNL certification exam administered by the Commission for Nurse
Certification (CNC), an autonomous arm of the AACN.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT11
Sample. The population (n=1378) of registered nurses certified as CNLs in March of 2011
received an invitation to participate in the study sent to the email address listed in the CNC
database. The invitation included a link to the CNLSES survey that was created and managed
using the Qualtrics survey software (Qualtrics.com). The CNLSES survey was open from March
to September 2011. Eligible participants received three emailed reminders sent at six week
intervals until the survey site was closed. The study was reviewed and approved by the
Institutional Review Board at ABC University.
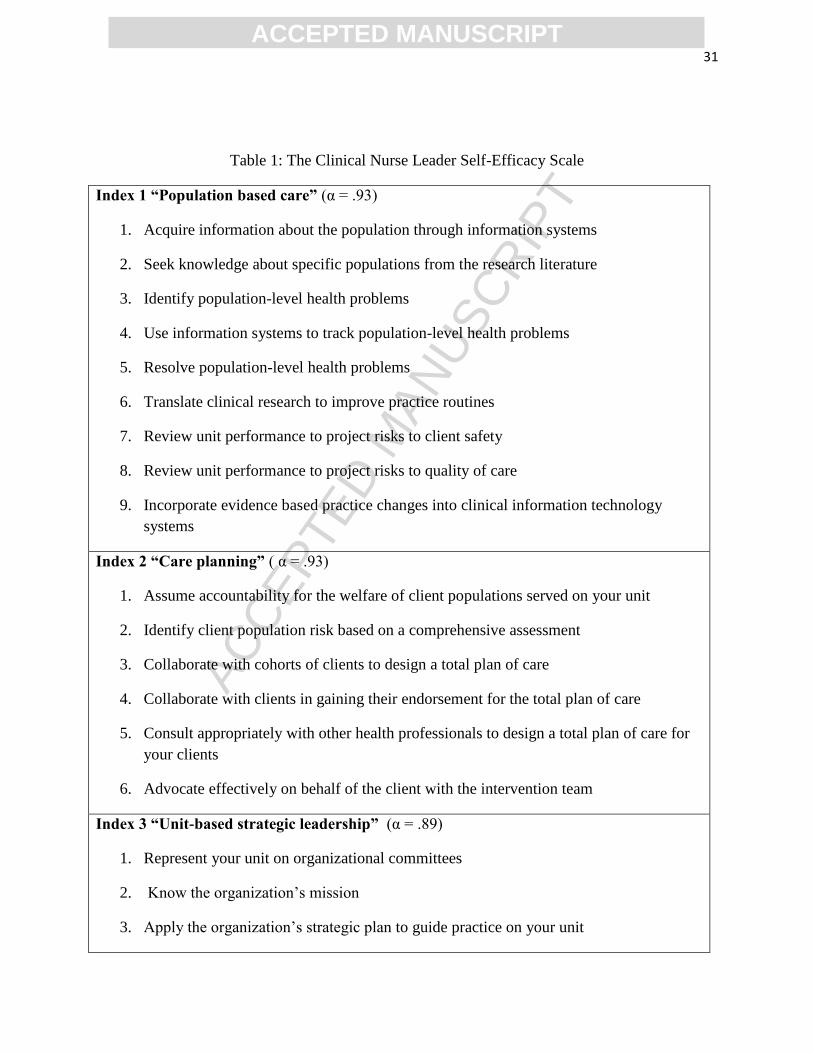
Instruments and Variables. Respondents’ perceptions of their confidence in performing practice
competencies associated with the CNL role were measured with the Clinical Nurse Leader Self-
Efficacy Scale (CNLSES) (Gilmartin & Nokes, in press). The CNLSES is a thirty-five item
state-specific self-efficacy scale that assesses nurses’ perceptions of their ability to function
effectively as a CNL. The CNLSES items are presented in Table 1. Based on Bandura’s (2006)
well-established survey assessment of self-efficacy, the CNLSES assess individuals’ confidence
in performing thirty-five CNL role competencies using a 5 point Likert scale (1= not at all
confident through 5= extremely confident). Respondents rated their self-confidence in
performing each of the thirty-five role activities on the day that they completed the CNLSES
survey. Because the survey was sent to all certified CNLs, respondents serving as program
faculty were asked to rate their self-confidence in teaching each of the thirty-five CNL practice
competencies.
The CNLSES reflects the AACN’s prescribed CNL practice competencies in the domains
of 1). nursing leadership: to actively manage care coordination activities; 2). clinical outcomes
management: to promote evidence based practice and data-based clinical decision making; and,
3). care environment management: to promote clinical quality and safety (AACN, 2007). The
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT12
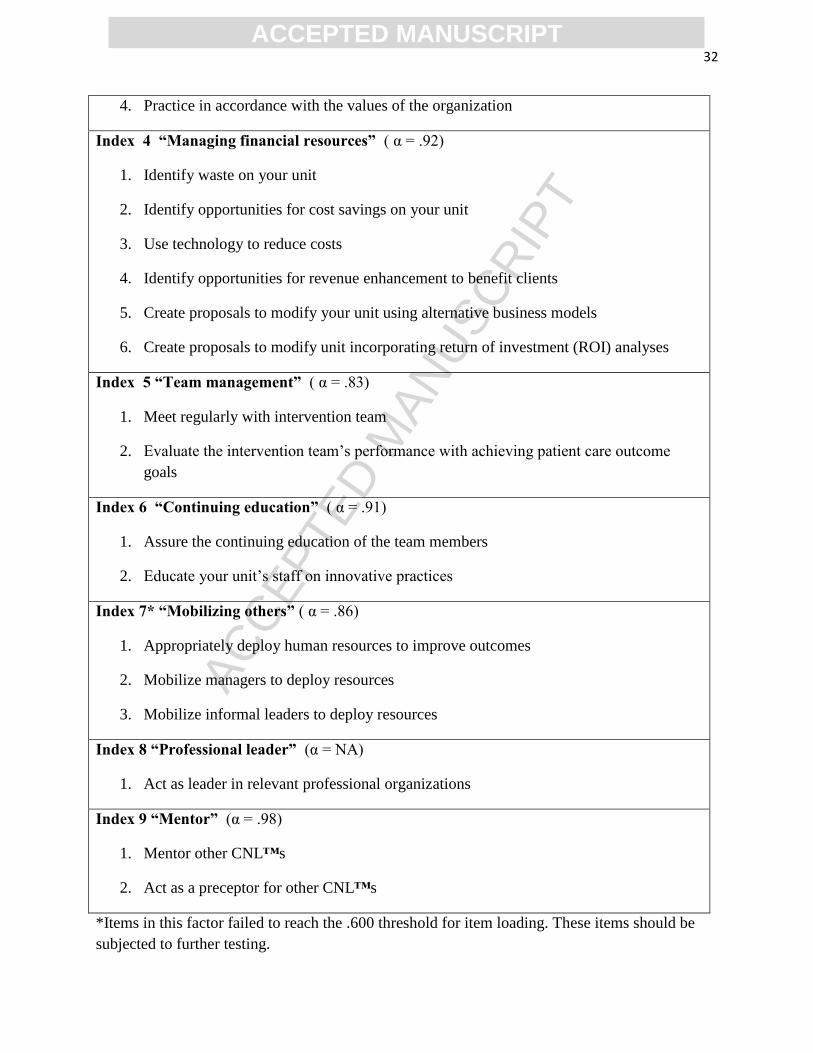
nine indices in the CNLSES are 1). population based care (9 items, α .93); 2). care planning (6
items, α .93); 3). unit-based strategic leadership (4 items, α .89); 4). managing financial
resources (6 items, α .92); 5). team management (2 items, α .83); 6). continuing education (2
items, α .91); 7). mobilizing others (3 items, α .86); 8). professional leader (1 item, N/A), and; 9).
mentor (2 items, α .98). For example, a question from the population-based care index is: “In
your practice as a CNL how confident are you that you can translate clinical research to improve
practice routines.” A question from the unit-based strategic leadership index is: “In your practice
as a CNL how confident are you that you can apply the organization’s strategic plan to guide
practice on your unit?”
----------------
Insert Table 1 around here
-----------------
Dependent Variables.
Clinical Nurse Leader Role Competencies. The nine role competencies associated with CNL
practice is the dependent variable.
Predictor Variables
1) Experience as a Clinical Nurse Leader. Measured as the time employed as a Clinical
Nurse Leader in years and months.
2) Graduate Program Model. There are five types of master’s degree programs preparing
Clinical Nurse Leaders recognized by the AACN. These include: Program Model A designed
for graduates holding a bachelor’s of science degree in nursing (BS); Program Model B
designed for BS graduates that includes a post-BS residency that awards master’s credit;
Program Model C designed for individuals with a bachelor’s degree in another discipline
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT13
(i.e., direct master’s entry program); Program Model D designed for associate degree
graduates (RN-MSN program); Program Model E awarding a post-master’s certificate for
individuals with a master’s degree in nursing in another area of study. These data were
collapsed into the categories: Model A that included responses from those attending both
Model A and B programs; Model C programs; the Model D, E and N/A categories were used
as the referent group in the regression models.
3) Year Graduated from CNL program. Measured as the year graduated from a CNL
program
4) Years of Experience in Nursing. Measured as the calendar year graduated from a basic
nursing education program to become a registered nurse.
5) Organizational Ownership. Organizational ownership was measured in one of four
categories: for-profit, not-for-profit, public and Veteran’s Administration. The VA was used
as the referent group in the regression models because it is an early adopter of the CNL role.
The not-for-profit and public ownership categories were merged into one category for
regression analysis.
6) Employed in a position with a CNL title. Measured as a binary Yes/No categorical
variable. CNL job title = 1; No or Not Applicable = 0. Respondents working as CNL
program faculty were included in the No or Not Applicable category.
7) Geographic region. Measured as a categorical variable using the United States Census
regions. Collapsed into four regions: Midwest, Northeast, South and West. The Western
region was used as the referent group in the regression model.
Data Analysis
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT14
Data were analyzed using a general linear regression model (GLM) to account for the use
of a dependent variable measured on an ordinal scale with predictor variables measured on
categorical, interval, and ordinal scales. I checked for potential multicollinearity among the
predictor variables and found none. Analyses were conducted using Statistical Analysis
Software (SAS) version 9.1.
Results
One hundred and ninety seven (n=197) surveys were returned. Of the returned surveys,
50 had missing data for all the items, suggesting that respondents activated the survey link and
decided not to complete the survey after it was launched. These 50 cases with missing data for all
questions were deleted from the data set, leaving a final sample of 147 cases and a response rate
of 9.4% (147 respondents/1378 eligible participants). This response rate compares reasonably
well with the rate obtained for the Commission for Nurse Certification’s 2011 job analysis
survey (258 respondents/1560 eligible participants; 16.7% response rate) (Tan, 2011). So as to
maintain statistical power, the 22 respondents serving as CNL program faculty were retained in
the analytic sample. I conducted analyses comparing the characteristics of respondents to the
population of CNLs; results from these analyses (reported below) indicate that the sample largely
represents the CNL population. .
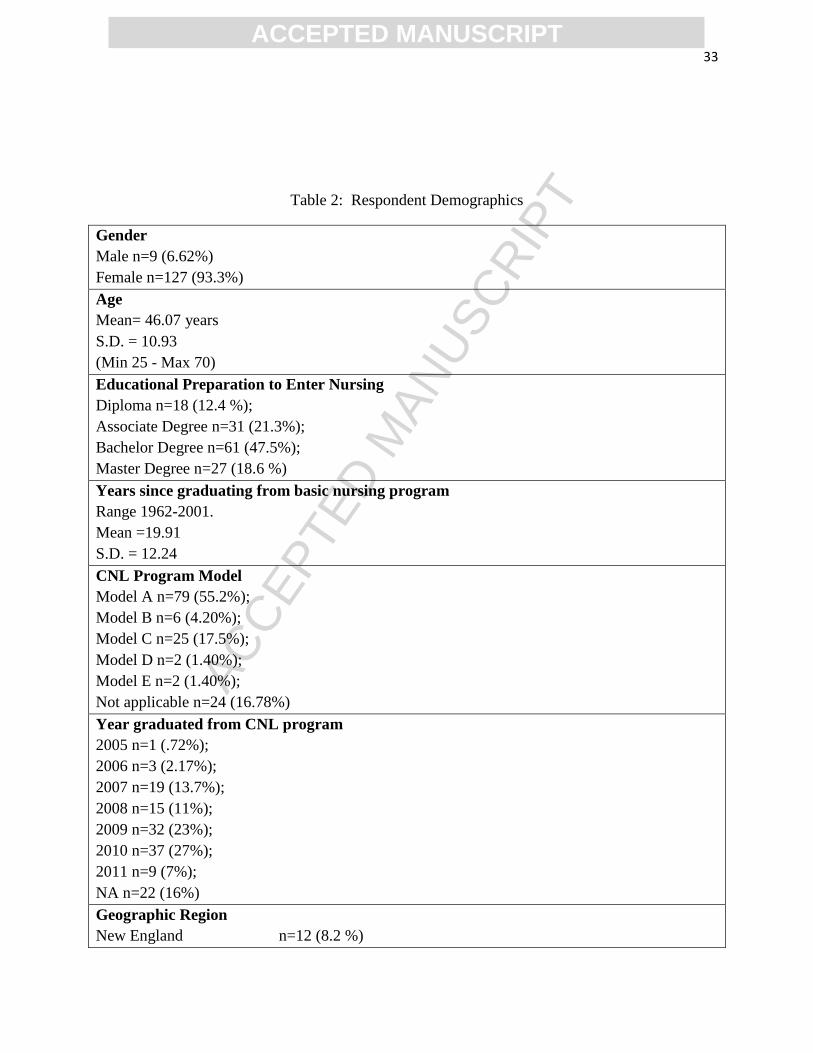
Sample. The respondents are predominately female (93% of respondents); hold a
Bachelor’s of Science degree (BS) as their first degree in nursing (69% of respondents) and have
an average of 19.9 years (s.d. =12.24 years) of experience in nursing. Fifty-five percent of the
respondents attended a Model A CNL program, a master’s degree program designed for
graduates with a bachelor’s degree in nursing, with nearly 50% of the respondents graduating
from a CNL program in 2009 or 2010. Twenty-one percent of the respondents work for the U.S.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT15
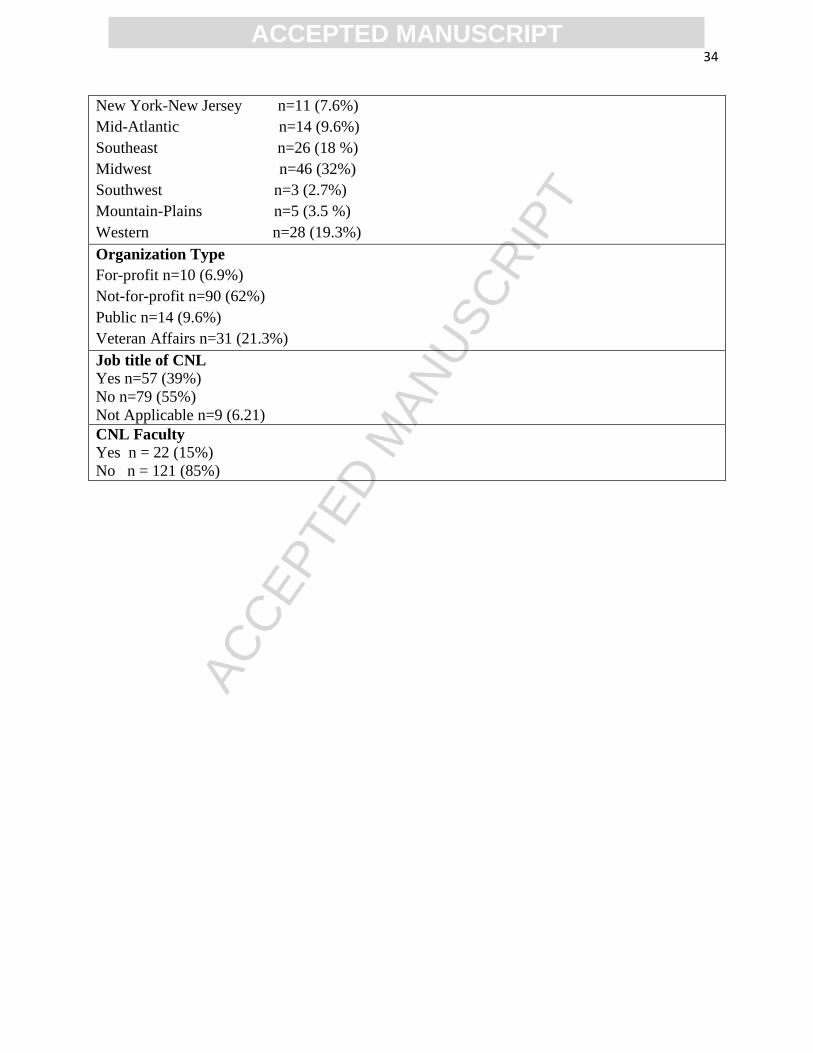
Department of Veteran’s Affairs and 32% of respondents live in the Midwestern region of the
United States. The demographic characteristics of the respondents are reported in Table 2.
---------------------------
Insert Table 2 around here
------------------------------
The sample of respondents is largely representative of the population of CNLs, according
to AACN data, with a slight over-representation of respondents from the Midwest region of the
United States. According to 2012 AACN data, there are 28 CNL programs in this region,
representing approximately 28% of the total number of CNL programs.
For the employment setting, the VA is over represented in the sample as compared to the
proportion of VA hospitals in the population of US hospitals. This is expected because the VA
has been an early adopter of the CNL role, with a national strategic agenda to integrate CNLs at
each facility across the national network of one hundred and fifty three VA hospitals by 2016
(Veterans’ Administration, 2009). This sample has a larger percentage of male respondents than
the general RN population (9% in the CNL sample versus 5% in the 2008 RN population survey
estimates). As expected, due to the direct master’s entry CNL program model, the sample has a
larger percentage of nurses prepared with a master’s degree as their initial education for entering
the profession, than the general nursing population. According to the 2008 RN Population
Survey, 13, 235 individuals or 0.4 % of the RN population hold a master’s degree as their initial
educational preparation (US Department HHS, 2008).
---------------------------
Insert Table 3 around here
------------------------------
Respondent’s confidence with performing the CNL role competencies.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT16
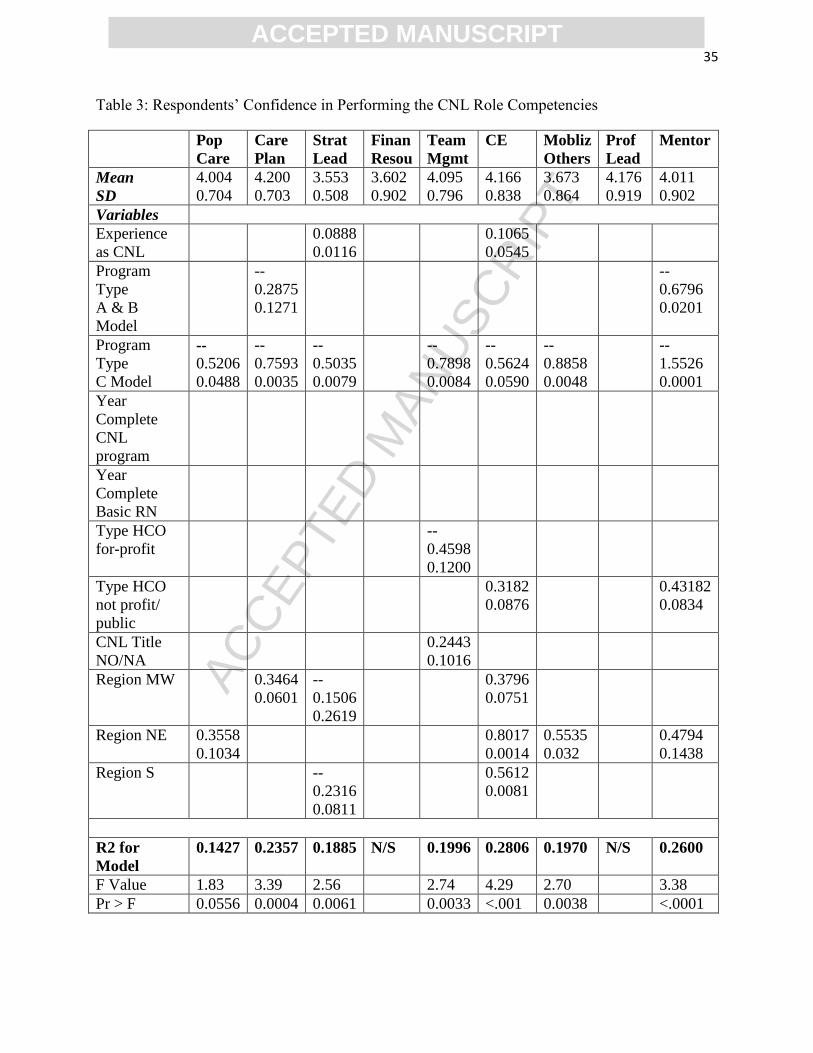
Table 3 shows results from the GLM regression models. Overall, 7 of 9 models were
statistically significant, accounting for 14-28% of the variation. Respondents’ demonstrated
variation in their confidence with performing the nine role competencies associated with CNL
practice measured by the CNLSES. The mean score and standard deviation for each of the nine
dependent variables suggests that not all respondents were equally confident in their abilities to
perform the CNL role competencies. Respondents’ were least confident in their abilities to
function as a unit-based strategic leader (mean = 3.55, s.d.=0.508) and most confident in their
abilities to develop and implement a total plan of care for individual clients (mean=4.20, s.d. =
0.703).
Experience in the CNL role. Experience in the CNL role was a significant predictor for
two of the nine role competencies. Respondents with longer experience as a CNL were more
confident in performing the role functions associated with unit-based strategic leadership and
assuring the continuing education of unit staff than other respondents.
Educational Preparation . Graduates from the Model A and B CNL master’s programs
designed for individuals with a bachelor’s degree in nursing were less confident in performing
care planning or serving as mentors for other CNLs, as compared to respondents graduating from
the D and E model programs or those serving as program faculty. Respondents graduating from
the direct master’s entry Program Model C, designed for individuals with a bachelor’s degree in
another field, were less confident in performing seven of the nine role competencies associated
with the CNL role. Compared to others, the Model C program graduates were less confident in
performing activities associated with population based care; care planning; unit-based strategic
leadership; team management; continuing education; mobilizing others and serving as a mentor
to other CNLs.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT17
Organizational Type. CNLs working in for-profit organizations were less confident in
their team management abilities than the respondents working in the VA organizations. In
comparison, CNLs working in not-for profit or public hospitals were more confident in their
abilities related to ensuring the continuing education of the nursing staff and serving as a mentor
to other CNLs than respondents employed in other organizations.
Position using the skills of a CNL. Respondents who did not hold a formal job title of
CNL, but used the knowledge and skills associated with CNL practice, were more confident in
their abilities to effectively manage the care team than respondents employed in a formal CNL
position.
Geographic Region. Respondents reported differences in their confidence to carry out the
CNL role competencies that varied by geographic region. Respondents employed in the
Midwestern region of the United States were more confident in performing the care planning
activities and ensuring the continuing education of unit staff than other respondents/respondents
from the Western region (referent group). At the same time, respondents from the Midwestern
region were less confident in their abilities to function effectively as a unit-based strategic leader
than other respondents. Respondents from the Northeastern region of the United States were
more confident in their abilities to perform effectively in the population-based care, continuing
education, mobilizing others and mentoring role competencies than other respondents. Finally,
respondents living in the Southern region of the United States were less confident in their unit
based strategic leadership abilities on the one hand, and more confident in their abilities to ensure
the continuing education of unit staff than other respondents, on the other.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT18
Discussion
The findings from this study have implications for research, education and practice to
inform strategies that promote effective role transitions to gain the full benefit of CNL practice.
Using self-report data from a national sample of nurses certified as CNLs, this study adds to the
literature on the implementation of the CNL role by empirically identifying personal and
contextual factors that explain variation in individuals’ levels of self-confidence in performing
the key functions of the CNL role. The results of this study point to a number of new avenues
for research on CNL role implementation.
Psychological Factors. The findings from this study extend prior work on the role that
psychological factors play in the day-to-day work performance of nurses pursuing careers as
CNLs (Dzurec, Allchin, Engler, Szarlan, Polifroni & Brewer, 2006). In particular, self-
confidence is an important psychological factor associated with successful career transitions
(Stakjovic & Luthans, 1998; Stephens, 1994), and my results show how self-confidence varies
among CNLs. There has been only one other prior study of the role of psychological factors
associated with CNL performance: Dzurec and colleagues (2006) examined data from a sample
of direct master’s entry CNL students and found that, in comparison to traditional undergraduate
nursing students, the CNL students were less depressed, less fatigued and more pessimistic in
their outlook.
Future studies should extend the work above by including key measures of individual
characteristics such as the as the Big 5 Personality traits (i.e., extraversion, agreeableness,
conscientiousness, emotional stability, and openness) (McCrae & Costa, 1987); core self-
evaluation traits (i.e.: self-esteem, generalized self-efficacy, locus of control, and emotional
stability) (Judge & Bono, 2001), or openness to change (Oreg, 2003).
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT19
Educational preparation to become a CNL. Contrary to expectations, respondents who
graduated from, direct graduate entry Model C programs had low levels of confidence in
performing seven of the nine competencies associated with the CNL role as compared to
graduates of other program models. According to data from the Commission for Nursing
Certification, there are currently 913 graduates from Model C programs, comprising
approximately 56% of the CNL population (ANCC, 2012). This result suggests the need for a
focused intervention and career transition strategy to bolster self-confidence in this group of
CNLs.
Master’s entry programs in nursing, usually completed in three years of study are
designed for individuals with a degree in another field who are entering nursing as a career
change. First developed in the 1960s (Pellico et al., 2012) these programs seek to reduce the time
it takes to produce new nurses with the goal of meeting the national demand for advanced
practice nurses. Pellico and colleagues’ (2012) recent integrated review of graduate entry
programs in nursing suggests that non-nurse college graduates successfully develop into APRNs
and CNMs. This evidence bodes well for graduates of the Model C CNL programs. Although
the literature suggests that individuals do successfully transition into new nursing roles,
understanding of the career transition process for direct master’s entry graduates is limited.
It is important to note that the current research on the transitions of non-nurse master’s
entry to practice graduates focuses on the well-established advanced practice RN and Certified
Nurse Midwife nursing roles. Respondents’ relative low levels of self-confidence may be related
to the development of the CNL role, rather than the personal adjustment component associated
with career transitions. That is, given the newness of the CNL role and the lack of knowledge on
the part of other nurses, health professionals and managers regarding the scope of practice and
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT20
potential benefits to patients and the organization (Sherman, 2010; Moore & Leahy, 2012),
CNLs may be placed in a situation of justifying the CNL role and their credentials to function in
the role, a situation that is likely to diminish self-confidence. More research focused on the
direct-graduate entry to practice group of CNLs is warranted to understand the relationship of
personal adjustment and role development on the career transitions of non-nurses into a high
profile clinical leadership position.
Organizational Context. Results from this study suggest that organizational ownership is
associated with CNLs’ confidence in performing difference aspects of the role. Ownership is a
variable that researchers commonly use as a proxy for an organization’s mission, values, and
strategy (Reuf & Scott, 1998). Differences in organizational ownership may be related to
variation in the goals of CNL practice, which, in turn, may affect CNLs’ confidence in their
ability to achieve these goals. For example, the Chief Nurse Officer that adopts the CNL role to
improve performance and reimbursement rates associated with the Hospital Consumer
Assessment of Healthcare Providers and Systems Survey (HCAHPS) (Center for Medicare
Services, U.S. Department Health and Human Services, 2010) core measures and nurse sensitive
outcomes will design the CNL role differently than the Chief Nurse Officer who seeks to
improve staff engagement and nurse-physician communication and collaboration.
Future research examining relationships between organizational ownership and CNL self-
efficacy should develop understanding of the mechanisms associated with CNLs’ confidence in
performing their core role functions. Similarly, future studies should include key variables not
only to account for the nursing practice environment, but also organizational strategy and
performance as important contextual factors that may account for variations in the design of the
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT21
CNL role, and by extension, a determinant of an individual’s confidence in performing the core
role functions (Nicholson, 1984; Stephens, 1994).
Another aspect of the organizational context that merits further study is the content and
structure of CNL academic-service partnerships used to formalize and institutionalize the CNL
role (De Geest, Dobbels, Schonfeld, Duerinckx, Sveinbjarnardottir & Denjaerynck, 2013).
According to the AACN (2007), the purpose of academic-service partnerships is to promote the
rapid diffusion and adoption of the CNL role into practice settings. In the ideal model, the
academic partner is responsible for ensuring that graduates possess the knowledge, skills and
abilities to effectively lead care coordination, quality improvement and clinical outcome
management activities. In turn, the service partner is responsible for creating a receptive
environment for CNL practice by attending to changes in organizational systems and structures;
including role descriptions, reporting relationships, staff education, and performance
expectations (Smith & Dabbs, 2007; AACN CNL Tool Kit, no date).
More than fifty percent of the respondents participating in this study do not hold a job
title of CNL, suggesting that they are employed in organizations that have not formally adopted
the CNL role. More work to understand the nature of the academic-service partnership that are
both committed to the CNL initiative and aligned to educate and employ nurses as CNLs will be
important to understand the adoption and diffusion of the CNL role over time and across
organizations.
CNL Job Title. Interestingly, holding a formal job title of CNL was not a significant
predictor of respondent’s confidence with performing core competencies associated with the
CNL role. This finding provides some evidence supporting a shift away from conceptualizing the
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT22
CNL as a formal unit-based role with responsibilities for microsystem functioning to
conceptualizing the core knowledge associated with CNL practice as a skill set with applications
to a range of existing positions with responsibility for clinical quality, safety and performance
improvement. More research is needed to understand differences in the practice patterns and the
associated self-confidence with the role competencies of nurses employed in formal CNL
positions with those who bring new knowledge of leadership, outcomes management and
performance improvement gained through graduate education as a CNL to other clinical or
management positions.
Regional differences. The results suggest that CNL’s confidence with performing the key
competencies associated with the role vary by geographic region. For example, respondents
working in the Northeastern region of the United States were more confident in their abilities to
perform the population based care, continuing education for unit staff, mobilizing others and the
mentoring functions associated with the CNL role than others. In comparison, respondents from
the Midwest region of the United States were more confident in their abilities for care planning
and ensuring continuing education for staff, but were less confident in their abilities to function
as a unit-level strategic leader than other respondents. These findings point to local variations
within communities of practice that warrant further study.
Faculty self-confidence. More research is needed on CNL program faculty members’
confidence with teaching the core role competencies. To date, no studies have examined faculty
members’ mastery of the key knowledge and skills associated with CNL practice. Quality
improvement, patient safety, and organizational performance are relatively new content in the
educational curricula of the health professions (Institute of Medicine, 2001; 2003; Cronenwett,
Sherwood, Barnsteiner, Disch, Johnson, et al., 2007). Because CNL program faculty are on the
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT23
forefront of educating a new generation nurses as point-of-care quality and safety clinicians
(Reid & Dennison, 2012), there are likely to be variations in faculty confidence with teaching the
prescribed curriculum outlined in the Clinical Nurse Leader White Paper (2007). For example,
nurse faculty may be very confident with teaching advanced care planning and risk reduction
strategies, because the nursing process is an important foundation for professional practice and a
core element of undergraduate and graduate curricula. In comparison, nurse faculty may have
less exposure and familiarity with teaching CNLs how to assess unit (microsystem) performance
and to develop a successful change management plan focused on improving a particular practice
problem (McKeon, Norris, Web, Hix, Ramsey & Jacobs, 2009). More research focusing on
CNL faculty would be useful to understand the contributions of faculty expertise to the personal
development aspect of the work role transitions of their students.
Person by Environment Interaction Effects. Finally, my results point to a number of new
avenues for research examining interactions among both personal characteristics and the
organizational environment that may affect nurses’ transitions into the high profile CNL role.
For instance, consider the relationships among personality, work experience and organizational
support for the CNL role. It may be that an expert staff nurse with a strong belief in his ability to
control his future (i.e., high internal locus of control) working in a hospital with a formal CNL
academic-service partnership may be more confident in his abilities to function in the CNL role
than a less experienced nurse, who believes that her career is in the hands of others (i.e., high
external locus of control), despite working in a hospital with a formal CNL partnership. New
studies with larger sample sizes should focus on understanding how personal and organization
characteristics interact to promote or hinder nurses’ transitions into the CNL role.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT24
Limitations
Of the population of certified CNLs, the final sample of respondents is relatively small.
Despite this limitation, the sample reflects the demographic characteristics of the population of
nurses credentialed as CNLs. Further, the response rate is acceptable for a non-solicited on-line
survey (Cook, Heath &Thompson, 2000) and is similar to the response rate for the recent CNL
job analysis survey conducted by the Commission on Nurse Certification during approximately
the same time period that this survey was in the field (Tan, 2011).
Conclusions
This study contributes to the literature on the implementation of the CNL role by
identifying key variables associated with the personal adjustment and role development involved
in successful career transitions to the CNL role. Respondents’ confidence in their ability to carry
out the core functions associated with the CNL role varied across practice competency,
geographic region, and organizational type and by the type of graduate program model attended
to become a CNL. This evidence can be used by nurse managers and program faculty to develop
targeted interventions to bolster CNL’s self-confidence in performing the core competencies
associated with their role. Because self-confidence is an important predictor of successful career
transitions, it is important to understand variations in CNLs’ confidence in their ability to
function in the role to promote the overall performance, job satisfaction and retention of the
nurses pioneering this innovative clinical leadership role.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT25
References
American Association of Colleges of Nursing. CNL Programs. Retrieved from
http://www.aacn.nche.edu/cnl/about/cnl-programs (Accessed on October 30, 2012).
American Association of Colleges of Nursing. CNL Statistics. Retrieved from
http://www.aacn.nche.edu/leading-initiatives/cnl/cnl-certification/pdf/CNLStats.pdf
(Accessed on October 30, 2012).
American Association of Colleges of Nursing (2007a). White paper on the role of the Clinical
Nurse Leader SM
Washington D.C.: American Association of Colleges of Nursing.
American Association of Colleges of Nursing (no date). CNL Tool Kit. Retrieved from
http://www.aacn.nche.edu/cnl/CNLToolKit.pdf (Accessed on October 30, 2012).
Ashforth, B.E. & Saks, A.M. (1995). Work-role transitions: A longitudinal examination of the
Nicholson model. Journal of Occupational and Organizational Psychology, 68, 157-175.
Bandura, A. (2006). Guide for creating self-efficacy scales. In F. Pajares & T. Urdan (Eds.),
Self-Efficacy Beliefs of Adolescents. Greenwich CT: Information Age Publishing, 307-
337.
Bartels, J. & Bednash, G. (2005). Answering the call for quality nursing care and patient safety:
A new model for nursing education. Nursing Administration Quarterly, 29(1), 5-13.
Benner, P. (2009). Educating Nurses: A Call for Radical Transformation. Carnegie Foundation,
New York.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT26
Bombard, E., Chapman, K., Doyle, M., Wright, D., Shippee-Rice, R., & Kasik, D.R. (2012).
Answering the questions, “What is a Clinical Nurse Leader?” Transition experiences of
four direct-entry master’s students. Journal of Professional Nursing, 26(6), 332-340.
Center for Medicare Services, U.S. Department for Health and Human Services. Retrieved from:
http://www.hcahpsonline.org/files/HCAHPS%20Fact%20Sheet%202010.pdf. Accessed on July 25,
2012.
Chow M.P. (2008). It's about time ... and motion. Study reveals how to improve nurses'
productivity and efficiency. Mater Manage Health Care, 17(9):15-7.
Committee on the Quality of Health Care in America (Eds.) (2001). Crossing the quality chasm:
A new health system for the 21st century. Washington D.C.: National Academy of
Sciences Press.
Cook, C., Heath, F., & Thompson, R.L. (2000). A meta-analysis of response rates in web or
internet-based surveys. Education and Psychological Measurement, 60(6), 821-836.
Cronenwett, L., Sherwood, G., Bernsteiner, J., Disch, J., Johnson, J., et al. (2007). Quality and
safety education for nurses. Nursing Outlook, 55(4), 121-131.
De Geest, S., Dobbels, F., Schonfeld, S., Duerunckx, N., Sveinbjaranadottir, E.K., &
Denkhaerynck, K. (in press). Academic service partnerships: What do we learn from
around the globe? A systematic literature review. Nursing Outlook.
Drenkard, K.N. (2004). The clinical nurse leader: A response from practice. Journal of
Professional Nursing, 20 (2), 89-96.
Dzurec, L.C., Allchin, L., Engler, A.J., Szarlan, J., Polifroni, E.C., & brewer, T. (2006). Toward
a qualified yes: personal characteristics of postbaccalaureate nursing students and
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT27
implementation of the Clinical Nurse Leader role. Journal of Professional Nursing, 22(1),
15-22.
Edwards, J.R. (2008). Person-environment fit in organizations: An assessment of theoretical
progress. The Academy of Management Annals, 2(1), 167-230.
Gilmartin, M.J. & Nokes, K. (in press). The Clinical Nurse Leader Self Efficacy Scale: Results
of a pilot study. Nursing Economic$
Hix, C., McKeon, L., & Walters, S. (2009). Clinical Nurse Leader impact on Clinical
Microsystem outcomes. Journal of Nursing Administration, 39(2), 71-76. doi:
10.1097/NNA.0b013e318195a612
Institute of Medicine. (2003). Health professions education: A bridge to quality. Washington,
D.C. : National Academies Press.
Jones, L. M. (2005). Role development and effective practice in specialist and advanced practice
roles in acute care settings: Systematic review and meta-analysis. Journal of Advanced
Nursing, 49(2), 191-209.
Judge, T.A. & Bono, J.E. (2001). Relationship of core self-evaluations traits—Self-esteem,
generalized self-efficacy, locus of control and emotional stability—with job satisfaction
and job performance: A meta-analysis. Journal of Applied Psychology, 86(1), 80-92.
Kovner, C.T., Brewer, C.S., Yingrengreung S., Fairchild, S. (2010). New nurses' views of quality
improvement education. Joint Commission Journal on Quality and Patient Safety,
36(1):29-35.
Lucero R.J., Lake E.T., & Aiken L.H., (2009). Variations in nursing care quality across
hospitals. Journal of Advanced Nursing, 65(11):2299-310.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT28
McCrae, R.R., & Costa, P.T. (1987). Validation of the five-factor model of personality across
instruments and observers. Journal of Personality and Social Psychology, 52, 81-90.
McKeon, L.M., Norris, T.L., Webb, S., Hix, C. Ramsey, G., & Jacob, S.R. (2009). Teaching
Clinical Nurse Leaders how to diagnose clinical microsystems. Journal of Professional
Nursing, 25(6), 373-378.
Moore, L.W. & Leahy, C. (2012). Implementing the new clinical nurse leader role with gleaning
insights from the past. Journal of Professional Nursing, 28(3), 139-146.
Nicholson, N. (1984). A theory of work role transitions. Administrative Science Quarterly, 29(2),
172-191.
Oreg, S. (2003). Resistance to change: Developing an individual difference scale. Journal of
Applied Psychology, 88(4), 680-693.
Ott, K.M., Haddock, K.S., Fox, S.E., Shinn, J.K., Walters, S.E., Hardin, J.W., Durand, K. &
Harris, J.L. (2009). The clinical nurse leader ®: Impact on practice outcomes in the
Veterans Health Administration. Nursing Economics, 27 (6), 363-373.
Pellico, L.H, Terrill, E., White, P., & Rico, J. (2012). Integrative review of graduate entry
programs in nursing. Journal of Nursing Education, 51(1), 29-37. doi:
10.3928/01484834-20111130-01. Accessed July 28, 2012.
Poulin-Tabor, D., Quirk, R.L., Wilson, L., Orff, S., Gallant, P., Swan, N., et al. (2008).
Pioneering a new role: The beginning, current practice and future of the clinical nurse
leader. Journal of Nursing Management, 16, 623-628.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT29
Reid, K., & Dennison, P., (2012). "The Clinical Nurse Leader (CNL)®: Point-of-Care Safety
Clinician" OJIN: The Online Journal of Issues in Nursing Vol. 16, No. 3, Manuscript 4.
Accessed May 30, 2012. doi: 10.3912/OJIN.Vol16No03Man04
Reuf, M. & Scott, W.R. (1998). A multidimensional model of organizational legitimacy:
Hospital survival in changing institutional environments. Administrative Science
Quarterly, 43(4), 877-904.
Sherman, R.O. (2010). Lessons in innovation: Role transition experiences of Clinical Nurse
Leaders. Journal of Nursing Administration, 49(12), 547-554.
Smith, D.S. & Dabbs, M.T. (2007). Transforming the care delivery model in preparation for the
clinical nurse leader. Journal of Nursing Administration, 37(4), 157-160.
Stakjovic , A.D. & Luthans, F. (1998). Self- efficacy and work-related performance: A meta-
analysis. Psychological Bulletin, 124(2): 240-260.
Stanley, J.M., Hoiting, T., Burton, D., Harris, J., & Norman, L. (2007). Implementing innovation
through education-practice partnerships. Nursing Outlook, 55(2), 67-73.
Stanton, M.P, Lammon, C.A., & William, E.S. (2011). The Clinical Nurse Leader: A
comparative study of the American Association of Colleges of Nursing vision to role
implementation. Journal of Professional Nursing, 27(2), 78-83.
Stephens, G. K. (1994). Crossing internal career boundaries: The state of research on subjective
career transitions. Journal of Management, 20(2), 479-501.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT30
Tan, R.J.B. (2011). Job analysis summary report 2011. Commission for Nurse Certification,
Washington, D.C.
Tanner, C.A. (2006). Thinking like a nurse: A research-based model of clinical judgment in
nursing. Journal of Nursing Education, 45(6), 204-211.
Tornabeni, J. & Miller, J.F. (2008). The power of partnership to shape the future of nursing: The
evolution of the clinical nurse leader. Journal of Nursing Management, 16(5), 608-613.
U.S. Department of Health and Human Services, Health Resources and Services Administration
(2010). The Registered Nurse Population: Initial Findings from the 2008 National
Sample Survey of Registered Nurses. Washington, D.C.
Veterans’ Administration (2009). Office of Nursing Services 2009 Annual Report. Veterans’
Administration: Washington D.C.
Watcher, R.M. (2010). Patient safety at ten: Unmistakable progress, troubling gaps. Health
Affairs, 29(1): 165-173.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT31
Table 1: The Clinical Nurse Leader Self-Efficacy Scale
Index 1 “Population based care” (α = .93)
1. Acquire information about the population through information systems
2. Seek knowledge about specific populations from the research literature
3. Identify population-level health problems
4. Use information systems to track population-level health problems
5. Resolve population-level health problems
6. Translate clinical research to improve practice routines
7. Review unit performance to project risks to client safety
8. Review unit performance to project risks to quality of care
9. Incorporate evidence based practice changes into clinical information technology
systems
Index 2 “Care planning” ( α = .93)
1. Assume accountability for the welfare of client populations served on your unit
2. Identify client population risk based on a comprehensive assessment
3. Collaborate with cohorts of clients to design a total plan of care
4. Collaborate with clients in gaining their endorsement for the total plan of care
5. Consult appropriately with other health professionals to design a total plan of care for
your clients
6. Advocate effectively on behalf of the client with the intervention team
Index 3 “Unit-based strategic leadership” (α = .89)
1. Represent your unit on organizational committees
2. Know the organization’s mission
3. Apply the organization’s strategic plan to guide practice on your unit
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT32
4. Practice in accordance with the values of the organization
Index 4 “Managing financial resources” ( α = .92)
1. Identify waste on your unit
2. Identify opportunities for cost savings on your unit
3. Use technology to reduce costs
4. Identify opportunities for revenue enhancement to benefit clients
5. Create proposals to modify your unit using alternative business models
6. Create proposals to modify unit incorporating return of investment (ROI) analyses
Index 5 “Team management” ( α = .83)
1. Meet regularly with intervention team
2. Evaluate the intervention team’s performance with achieving patient care outcome
goals
Index 6 “Continuing education” ( α = .91)
1. Assure the continuing education of the team members
2. Educate your unit’s staff on innovative practices
Index 7* “Mobilizing others” ( α = .86)
1. Appropriately deploy human resources to improve outcomes
2. Mobilize managers to deploy resources
3. Mobilize informal leaders to deploy resources
Index 8 “Professional leader” (α = NA)
1. Act as leader in relevant professional organizations
Index 9 “Mentor” (α = .98)
1. Mentor other CNL™s
2. Act as a preceptor for other CNL™s
*Items in this factor failed to reach the .600 threshold for item loading. These items should be
subjected to further testing.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT33
Table 2: Respondent Demographics
Gender
Male n=9 (6.62%)
Female n=127 (93.3%)
Age
Mean= 46.07 years
S.D. = 10.93
(Min 25 - Max 70)
Educational Preparation to Enter Nursing
Diploma n=18 (12.4 %);
Associate Degree n=31 (21.3%);
Bachelor Degree n=61 (47.5%);
Master Degree n=27 (18.6 %)
Years since graduating from basic nursing program
Range 1962-2001.
Mean =19.91
S.D. = 12.24
CNL Program Model
Model A n=79 (55.2%);
Model B n=6 (4.20%);
Model C n=25 (17.5%);
Model D n=2 (1.40%);
Model E n=2 (1.40%);
Not applicable n=24 (16.78%)
Year graduated from CNL program
2005 n=1 (.72%);
2006 n=3 (2.17%);
2007 n=19 (13.7%);
2008 n=15 (11%);
2009 n=32 (23%);
2010 n=37 (27%);
2011 n=9 (7%);
NA n=22 (16%)
Geographic Region
New England n=12 (8.2 %)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT34
New York-New Jersey n=11 (7.6%)
Mid-Atlantic n=14 (9.6%)
Southeast n=26 (18 %)
Midwest n=46 (32%)
Southwest n=3 (2.7%)
Mountain-Plains n=5 (3.5 %)
Western n=28 (19.3%)
Organization Type
For-profit n=10 (6.9%)
Not-for-profit n=90 (62%)
Public n=14 (9.6%)
Veteran Affairs n=31 (21.3%)
Job title of CNL
Yes n=57 (39%)
No n=79 (55%)
Not Applicable n=9 (6.21)
CNL Faculty
Yes n = 22 (15%)
No n = 121 (85%)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT35
Table 3: Respondents’ Confidence in Performing the CNL Role Competencies
Pop
Care
Care
Plan
Strat
Lead
Finan
Resou
Team
Mgmt
CE Mobliz
Others
Prof
Lead
Mentor
Mean
SD
4.004
0.704
4.200
0.703
3.553
0.508
3.602
0.902
4.095
0.796
4.166
0.838
3.673
0.864
4.176
0.919
4.011
0.902
Variables
Experience
as CNL
0.0888
0.0116
0.1065
0.0545
Program
Type
A & B
Model
--
0.2875
0.1271
--
0.6796
0.0201
Program
Type
C Model
--
0.5206
0.0488
--
0.7593
0.0035
--
0.5035
0.0079
--
0.7898
0.0084
--
0.5624
0.0590
--
0.8858
0.0048
--
1.5526
0.0001
Year
Complete
CNL
program
Year
Complete
Basic RN
Type HCO
for-profit
--
0.4598
0.1200
Type HCO
not profit/
public
0.3182
0.0876
0.43182
0.0834
CNL Title
NO/NA
0.2443
0.1016
Region MW 0.3464
0.0601
--
0.1506
0.2619
0.3796
0.0751
Region NE 0.3558
0.1034
0.8017
0.0014
0.5535
0.032
0.4794
0.1438
Region S --
0.2316
0.0811
0.5612
0.0081
R2 for
Model
0.1427 0.2357 0.1885 N/S 0.1996 0.2806 0.1970 N/S 0.2600
F Value 1.83 3.39 2.56 2.74 4.29 2.70 3.38
Pr > F 0.0556 0.0004 0.0061 0.0033 <.001 0.0038 <.0001