Embed Size (px)
Citation preview
Variation in Antipsychotic Medication Use and Expenditures Across State Medicaid Programs
Jacqueline R. Chaudhry
The Big Picture: Objectives Provide accurate national and state level
estimates of the prevalence, level, type and pattern of antipsychotic medication use and expenditures among all fee-for-service adult Medicaid recipients and variability
Examine the role of state Medicaid policies, health care resources, patient demographic, clinical characteristics in explaining the interstate variation in antipsychotic use and expenditures
The Big Picture: Background Geographic variation in medical care
is well documented in the United States
Most studies focus on non-drug health service use and expenditures
Little research has examined the variation in prescription drug use and expenditures, especially in the Medicaid population
Medicaid Medicaid is the United States
major public health insurance for low income Americans
Medicaid finances 52 million people including children and many of the sickest people in the nation (CMS 2004: KFF 2005)
Medicaid is administered by the state with funding from the state and federal government
State Medicaid programs vary widely in terms of eligibility and benefits design and in use of prescription drugs
Many states have adopted cost containment strategies targeting Medicaid prescription drug spending
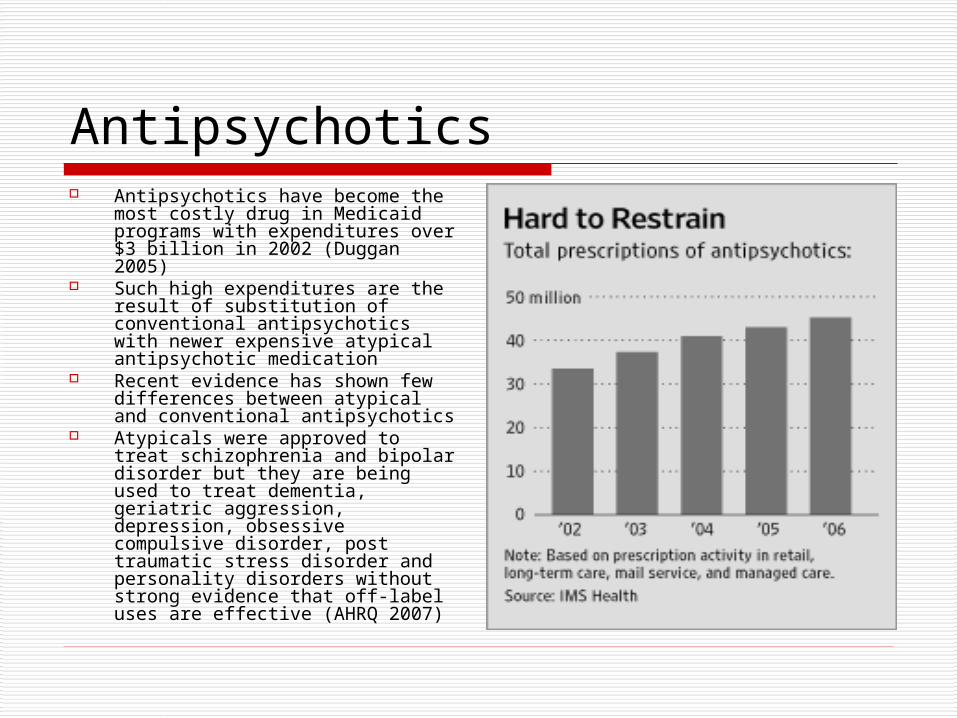
Antipsychotics Antipsychotics have become the
most costly drug in Medicaid programs with expenditures over $3 billion in 2002 (Duggan 2005)
Such high expenditures are the result of substitution of conventional antipsychotics with newer expensive atypical antipsychotic medication
Recent evidence has shown few differences between atypical and conventional antipsychotics
Atypicals were approved to treat schizophrenia and bipolar disorder but they are being used to treat dementia, geriatric aggression, depression, obsessive compulsive disorder, post traumatic stress disorder and personality disorders without strong evidence that off-label uses are effective (AHRQ 2007)
State Medicaid Drug Cost Containment Strategies Co-payments
Increased Co-payments
Tiered co-payments Prior Authorization Preferred Drug Lists Step Therapy
Requirements Incentives to use
generic drugs Monthly Prescription
Drug Limits
The Big Picture: Our Study
Our study will be the first to comprehensively examine the geographic variation in Medicaid antipsychotic use and expenditures and factors contributing to the variation in use of prescription drugs across states.
The Details in the Picture: State Medicaid Policy Surveys
To develop analysis concerning state Medicaid policies there had to be a thorough undertaking of each state’s policy
A survey had to be developed for each state concerning its Medicaid cost containment policies and antipsychotic policies from 2001-2007
The Survey: Objectives Determine state Medicaid prescription
policies specifically for antipsychotic medications
State co-payment Prior Authorization Preferred Drug Lists Step therapy limits Monthly Prescription Limits Generic substitution
Relate the role of state Medicaid policies to interstate variation in antipsychotic use and expenditure
The Survey: Methods The state surveys link three
different data sources including Centers for Medicare and Medicaid Services quarterly data, National Pharmaceutical Council data and published literature.
The surveys are now in the process of being reviewed and completed by state Medicaid officials.
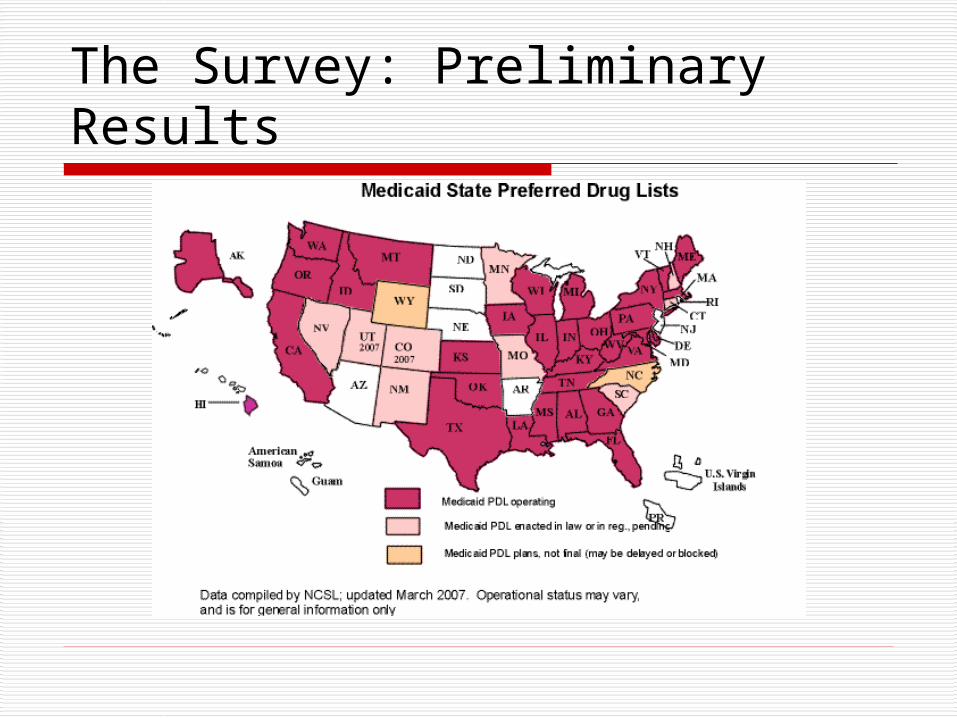
The Survey: Preliminary Results Preliminary results indicate that 18 states have had
an increase in co-payments from 2001 to 2007. Preliminary results also indicate that 32 states have a
preferred drug list and of the 32 states, 9 states exempt typical antipsychotic drugs and 13 states exempt atypical antipsychotics.
Prior authorization policies are in place in 50 states, 39 exempt antipsychotic drugs.
Preliminary results suggest 50 states have generic drug policies, however 9 states exclude antipsychotic drugs from the mandate.
18 states have prescription limits and 5 states exclude antipsychotic drugs from prescription limits.
5 states have fail first drug policies for antipsychotics.
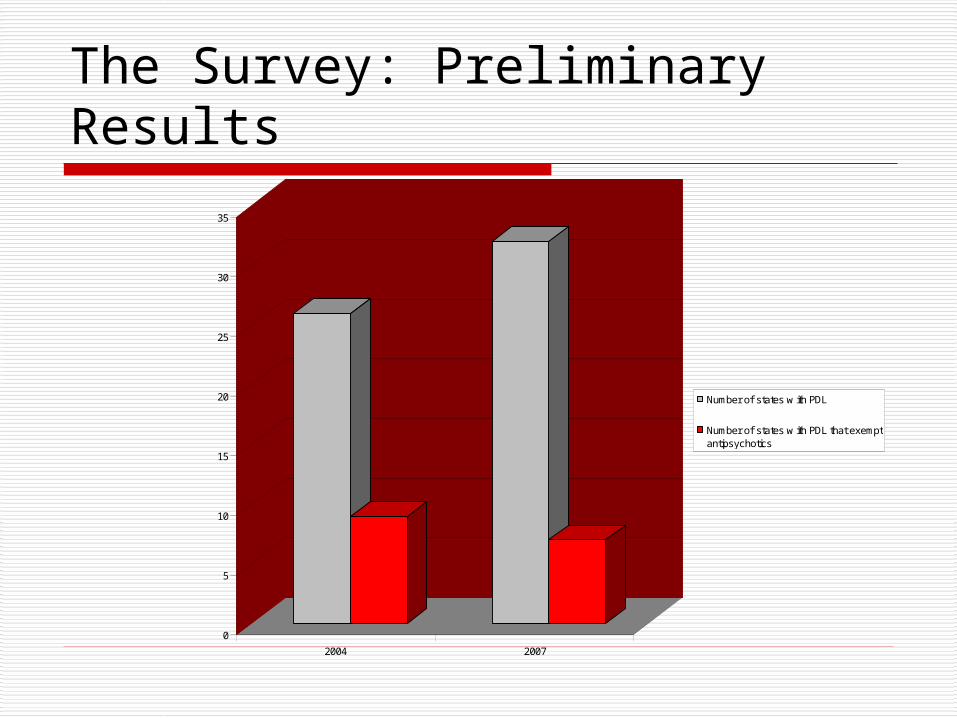
The Survey: Preliminary Results
0
5
10
15
20
25
30
35
2004 2007
Number of states w ith PDL
Number of states w ith PDL that exemptantipsychotics
The Survey: Preliminary Results
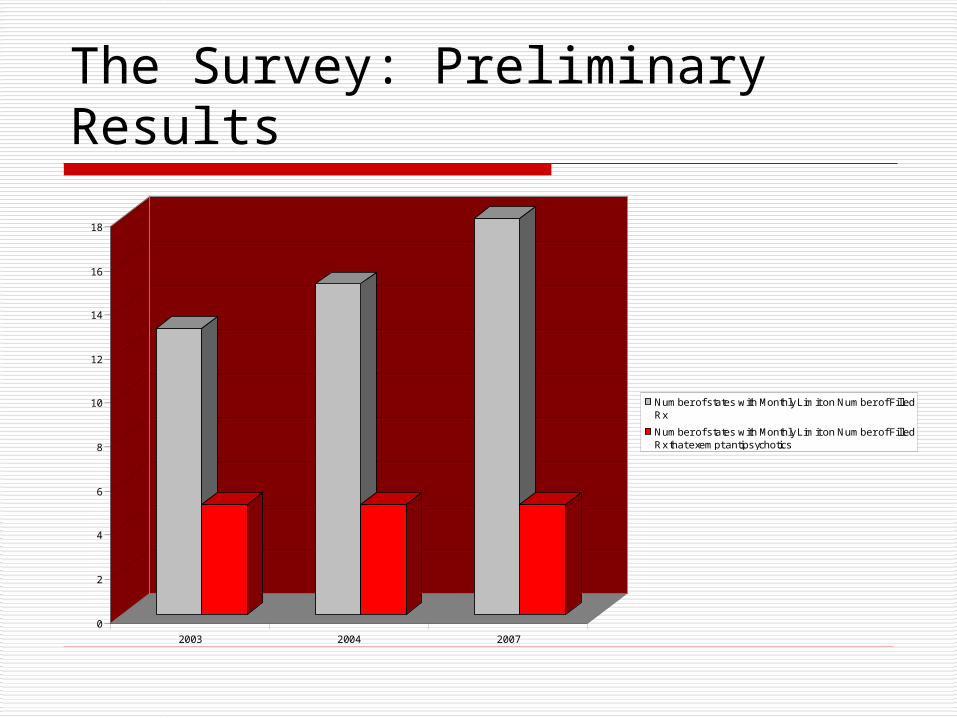
The Survey: Preliminary Results
0
2
4
6
8
10
12
14
16
18
2003 2004 2007
Number of states with Monthly Limit on Number of FilledRx
Number of states with Monthly Limit on Number of FilledRx that exempt antipsychotics
The Survey: Conclusion Increased use of cost
containment policies between 2001-2007 Co-payment Preferred Drug Lists Generic drug policies Monthly limit on
number of filled prescription
Putting the Details back in the Big Picture: Policy Implications
Understanding the impact of state Medicaid policy differences on antipsychotic medication use will be important to insuring rational prescription policies, efficiency of the Medicaid program and optimal care of Medicaid patients.
These findings will have implications for state policymakers debating further changes in Medicaid prescription policies to control antipsychotic expenditures.
Acknowledgements
Dr. Jalpa Doshi, Ph.D Karunya Manikonda Alex Li Summer Undergraduate Minority
Research Program (SUMR) Program Director, Joanne Levy, MBA Leonard Davis Institute of Economics
(LDI)
Special thanks to the following organizations for their support:
The University of Pennsylvania Provost’s Diversity Fund
The Center for Health Equity Research and Promotion (CHERP)
Pennsylvania Department of HealthOffice of Health Equity
Thank You! Questions?