Embed Size (px)
Citation preview

Antipsychotic Agents
Dr. Akshil Mehta
•1•2/28/2015

Psychosis
Psychosis is a thought disorder characterized by disturbances of reality and perception, impaired cognitive functioning, and inappropriate or diminished affect (mood).
•2

Psychosis:
Psychosis can be broadly
Categorized in to four groups:
•3

1. Acute and chronic organic brain syndromes (cognitive disorders) such as, Delirium and dementia, prominent features of confusion, disorientation, defective memory and disorganized behavior.
2. Functional disorders such as, memory and orientation mostly retained by emotion, thought, reasoning and behavior are altered.
3. Schizophrenia (split mind) i.e. splitting of perception and interpretation from reality- hallucination, inability to think coherently. Schizophrenia is often described in terms of positive or negetive (deficit) symptoms.. Schizophrenia is a particular kind of psychosis characterized mainly by a clear sensorium but a marked thinking disturbance.
4. Paranoid state i.e. fixed delusions (false beliefs) and loss of insight in to abnormality. •4

Schizophrenia
• Onset of schizophrenia is in the late teens -early ‘20s.
• 0.7-1% population
• Genetic predisposition -- Familial incidence.
• Multiple genes are involved.
• May or may not be present with anatomical changes.
•5

Onset Age
• Males: early 20s
• Females: late 20s
•6

Schizophrenia
• A thought disorder.
• The disorder is characterized by a divorcement from reality in the mind of the person (psychosis).
•7

•Positive Symptoms•Hallucinations•Delusions (bizarre, persecutory)•Disorganized Thought•Perception disturbances•Inappropriate emotions
•Negative Symptoms•Blunted emotions•Anhedonia•Lack of feeling
•Cognition•New Learning•Memory
•Mood Symptoms•Loss of motivation•Social withdrawal•Insight•Demoralization•Suicide
Schizophrenia - symptoms
•FUNCTION
•8

Etiology of Schizophrenia
Idiopathic
Biological Correlates
1) Genetic Factors
2) Neurodevelopmental abnormalities.
3) Environmental stressors.
•9

Etiology of Schizophrenia
Characterized by several structural and functional abnormalities in the brains of schizophrenic patients:
1) Enlarge cerebral ventricles.
2) Atrophy of cortical layers.
3) Reduced volume of the basal ganglia.
•10

Brain Morphology & Schizophrenia
Some schizophrenia patients exhibit morphological changes in the brain like
enlargement of fluid-filled ventricles.
•11

DSM-IV Diagnosis
• Schizophrenia
– Symptoms > 6 months
• Schizophreniform disorder
– Symptoms 1 month - 6 months
• Brief psychotic disorder
– Symptoms 1 day - 1 month
•12

DSM V Diagnosis of Schizophrenia• Two or more of the following, including 1, 2, or 3
1. Delusions
2. Hallucinations
3. Disorganized speech
4. Grossly abnormal psychomotor behavior
5. Negative symptoms
• Duration: 1 month during last 6
• Social/occupational dysfunction
• Exclusion: medical condition or drug
•13

•14
Early treatments of psychosis
•Bethlehem Asylum 'Bedlam‘, one of the first asylums
(1403) •18th
century asylum
•National Library of Medicine
•Jerrold & Quenzer, Psychopharmacology,
•Sinauer, c2005, p. 445

History of Antipsychotic treatments
Schizophrenia has been around perhaps, since the beginning of humankind, however, it was not until the last century that it was established as a separate entity amongst other mental disorders.
Many treatments have been devised:
Hydrotherapy: “The pouring of cold water in a stream, from a height of at least four feet onto the forehead, is one of the most certain means of subsiding violent, maniacal excitement that we have ever seen tried”... wrote an anonymous physician in the early 1800’s.
•15

Prefrontal lobotomy, Electroconvulsive therapy
• Dr. Egas Moniz –Developed prefrontal lobotomy technique
• 1935 – heard about work on a chimp “Becky” –Performed surgery on many patients
• they were just calmer, but also more sluggish and apathetic
• Awarded the Nobel Prize in Physiology and Medicine
• Next 15 years - 50,000 lobotomies
•16

•17

HISTORY OF ANTIPSYCHOTICS• Anti-psychotics were discovered accidentally by a French
naval surgeon, Henri Laborit. Laborit was interested in circulatory shock, not schizophrenia.
• Laborit experimented with a variety of drugs to combat shock syndrome.
• One of the drugs was an agent called Pomethazine. His primary reason for using the drug was for its effects on the ANS, however, he discovered the secondary properties of the drug– The drug made patients drowsy, reduced pain, and created
a feeling of euphoric quietude.” This drug had psychological effects.
• Laborit’s observation were used to modify the formula of Promethazine into the first effective anti-psychotic medication, Chloropromazine (Thorazine).
• Heinrichs, R. W., (2001). In Search of Madness: Schizophrenia and Neuroscience. Oxford University Press: New York.
•18

•19
•Consequence of antipsychotic drug discovery
•Jerrold & Quenzer, Psychopharmacology, Sinauer, c2005, p. 445

Pharmacodynamics
Anatomic Correlates of Schizophrenia...
Areas Associated with Mood and Thought Processes:
Frontal cortex
Amygdala
Hippocampus
Nucleus accumbens
Limbic Cortex•20

Dopamine System
There are four major pathways for the dopaminergic system in the brain:
I. The Nigro-Stiatal Pathway.
II. The Mesolimbic Pathway.
III. The Mesocortical Pathway.
IV. The Tuberoinfundibular Pathway.
•21

•22
•Anatomy of dopamine neurons
•Brody, Larner & Minneman, Human Pharmacology, Mosby, c1998, p. 343

•23
Functional neuroanatomy of DA in the CNS
• Nigrostriatal pathway: motor planning and execution, habit
formation, learning, habituation, memory
• Mesolimbic: complex target-oriented behavior, integrating
emotional responses, motor and sensory processing
• Mesocortical: cognition; orchestration of thoughts and actions in
accordance with internal goals
• Tuberoinfundibular: tonic inhibition of prolactin release, increase
growth hormone release
• Chemoreceptor trigger zone: emesis & nausea

Dopamine System
• DOPAMINE RECEPTORS– There are at least 5 subtypes of receptors:
– D1 and D5: mostly involved in postsynaptic inhibition.
– D2, D3, and D4: involved in both pre-and postsynaptic inhibition.
D2: the predominant subtype in the brain:
regulates mood, emotional stability in the limbic system and movement control in the basal ganglia.
•25

•26

•27
•Synthesis:
•TH – tyrosine hydroxylase
•AADC – aromatic acid decarboxylase
•Metabolism:
•MAO – monoamine oxidase
•COMT – catechol-O-
methyltransferase
•Metabolites:
•DOPAC – dihydroxyphenylacetic acid
•HVA: homovanillic acid
•Feldman et al., Principles of Neuropsychopharmacology, 1997

•28

Schizophrenia - Dopamine Hypothesis
Repeated administration of stimulants like amphetamines and cocaine, which enhance central dopaminergic neurotransmission, can cause a psychosis that resembles the positive symptoms of schizophrenia
Low doses of amphetamine can induce a psychotic reaction in schizophrenics in remission
Stress, a major predisposing factor in schizophrenia, can produce a psychotic state in recovered amphetamine addicts.
Carlsson and Lindqvist (1963) first proposed that drugs such as chlorpromazine and haloperidol alleviate schizophrenic symptoms by blocking DA receptors and thereby reduce DA function.
Thess antipsychotic medications, which have been the main stay for treatment for nearly 50 years, have in common their ability to block dopamine D2 receptors
•29

A strong correlation between the affinity of antipsychotic drugs for DA receptors and their clinical potency
But no clear and consistent abnormality in DA function has been detected in schizophrenic patients.
Some early studies with postmortem tissue revealed increased numbers of DA receptors (in particular D2-like) in schizophrenic patients, but there are serious problems with these findings. But long-term administration of antipsychotics produces increases in D2 receptors in animals.
The reduction in cortical dopamine transmission (both at the pre-and postsynaptic level) in the chronic Phencyclidine model seems to be consistent with some findings in schizophrenic patients
Reduced cortical dopamine transmission induced by long-term PCP exposure may be associated with a hyperactivity of subcortical dopamine systems
Schizophrenia - Dopamine Hypothesis
•30

Dopamine Theory of Schizophrenia
Dopamine Correlates:
• Antipsychotics reduce dopamine synaptic activity.
• These drugs produce Parkinson-like symptoms.
• Drugs that increase DA in the limbic system causepsychosis.
• Drugs that reduce DA in the limbic system(postsynaptic D2 antagonists) reduce psychosis.
• Increased DA receptor density (Post-mortem, PET).
• Changes in amount of homovanillic acid (HVA), a DAmetabolite, in plasma, urine, and CSF.
•31

Dopamine Theory of Schizophrenia
Evidence against the Theory?
• Antipsychotics are only partially effective in most (70%) and ineffective for some patients.
• Phencyclidine, an NMDA receptor antagonist, produces more schizophrenia-like symptoms in non-schizophrenic subjects than DA agonists.
• Atypical antipsychotics have low affinity for D2 receptors.
• Focus is broader now and research is geared to produce drugs with less extrapyramidal effects.
•32

Other transmitter systems involved..
• Glutamatergic system dysfunction• e.g. effect of phencyclidine – blocker of NMDA type of
glutamate receptors
• G-protein signaling abnormalities
• Serotoninergic system abnormalities• most antipsychotics also affect serotonin receptors
Dopamine and serotonin theory of schizophrenia
•33

correlation between DA affinity and antipsychotic efficacy has become weaker as a result of recently developed atypical antipsychotic medications that also show substantial affinity for 5HT2 receptors
Alteration of 5-HT transmission in the brains of schizophrenics patients have been reported in post-mortem studies and serotonin-agonists challenge studies
There are widespread and complex changes in the 5-HT system in schizophrenics patients
These changes suggest that 5-HT dysfunction is involved in the pathophysiology of the disease
Schizophrenia - Serotonin Hypothesis
•35

•Prefrontal Cortex
•Limbic
System
•GABA/ACh
•Striatum
•Ventral Tegmental Area
(A10)
•Substantia Nigra
(A9)
•DorsalRaphe
•MedianRaphe
•5-HT2A antagonists release
dopamine from inhibition and decrease
EPS
•Blockade of D2 receptors
by conventional APDs
causes EPS
•Motor Outputs
•GABA
Glutamate
•Dopamine (DA)
•Serotonin (5-HT)
•Serotonin-Dopamine Interactions
•36

• Preclinical as well as clinical studies provide evidence of hypofunction of NMDA receptors as a contributory process in the pathophysiology of schizophrenia
• Several clinical trials with agents that act at the glycinemodulatory site on the NMDA receptor have revealed consistent reductions in negative symptoms and variable effects of cognitive and positive symptoms
• These studies also provide evidence that suggests the effects of clozapine on negative symptoms and cognition may be through activation of the glycine modulatory site on the NMDA receptor.
Schizophrenia - Glutamate Hypothesis
•38

•Limbic
System
•Ventral Tegmental Area
(A10)
•Substantia Nigra
(A9)
•DorsalRaphe
•MedianRaphe
•Prefrontal Cortex
•Striatum
•NMDA antagonists elevate extracellular brain levels of 5-HT in the
prefrontal cortex
•NMDA antagonists reduce burst
firing of VTA DA neurons
•NMDA antagonists
increase the firing of DA
in limbic areas
•5-HT2A antagonists restore dopaminergic
function in the prefrontal cortex
•5-HT2 antagonists block the
effects of NMDA antagonists
•Dopamine (DA)
•Glutamate
•Serotonin (5-HT)
•GABA
•Serotonin-Glutamate-Dopamine Interactions
•39

•40
Ligand-gated channel subtypes of the glutamate receptor
•Jerrold & Quenzer, Psychopharmacology, Sinauer, c2005 , p. 167

•41
NMDA Hypothesis of Schizophrenia
• Reducing glutamate worsens psychotic symptoms
– Competitive NMDA antagonists induce both positive and negative symptoms in healthy and schizophrenic subjects
– NMDA antagonists worsen symptoms in unmedicated patients with schizophrenia
– Chronic treatment with antipsychotic drugs can block effects of NMDA antagonists
– Decreased levels of glutamate in CSF, prefrontal cortex and hippocampus of schizophrenics
• NMDA agonists improve symptoms in schizophrenia

ANIMAL MODEL OF SCHIZOPHRENIA
• High doses of amphetamine produce a syndrome of repetitive behaviours (sniffing, head movements, gnawing and licking) known as stereotypy or stereotyped behaviour.
• Because stereotyped behaviour also occurs in humans after higher doses of amphetamine and is similar to the repetitions of meaningless behaviour seen in schizophrenia, the amphetamine-induced stereotypy has been used as an animal model of schizophrenia.
• DA receptor antagonists block amphetamine stereotypy and there is a strong correlation between their potency in this model and in ameliorating schizophrenic symptoms.
• Other more complicated models are based on attentional and cognitive abnormalities observed in schizophrenia.
•42

Schizophrenia Pathophysiology
Schizophrenia Pharmacologic Pathophysiology Profile of APDs
Past Excess dopaminergic Dopamine D2-receptor activity antagonists
Present
Renewed interest in the Combined 5-HT2/D2role of serotonin (5-HT) antagonists
Future
Imbalance in cortical More selective antagonistscommunication and Mixed agonist/antagonists cortical-midbrain Neuropeptide analogs integration, involving multiple neurotransmitters
•43

Antipsychotics treatment
Antipsychotics/Neuroleptics• Antipsychotics are the drugs currently used in
the prevention of psychosis.• They have also been termed neuroleptics,
because they suppress motor activity and emotionality.
** These drugs are not a cure **
• Schizophrenics must be treated with medications indefinitely, in as much as the disease in lifelong and it is preferable to prevent the psychotic episodes than to treat them.
•44

Antipsychotic treatments
In 1940’s Phenothiazenes were isolated and were used as pre-anesthetic medication, but quickly were adopted by psychiatrists to calm down their mental patients.
In 1955, chlorpromazine was developed as an antihistaminic agent by Rhône-Pauline Laboratories in France. In-patients at Mental Hospitals dropped by 1/3.
•45

Antipsychotics/Neuroleptics
Although the antipsychotic/neuroleptics are drugs used mainly in the treatment of schizophrenia, they are also used in the treatment of other psychoses associated with depression and manic-depressive illness, and psychosis associated with Alzheimer’s disease. These conditions are life-long and disabling.
•46

Antipsychotics/Neuroleptics
NON-compliance is the major reason for relapse.
•47

ANTIPSYCHOTICS
• Pre-90’s– “Typical”, conventional, traditional neuroleptics, major
tranquilizors
– Modeled on D2 antagonism
– EPS/TD
• Post-90’s– “Atypical”, novel, 2nd generation
– Modeled on 5-HT2/D2 antagonism
– Less EPS, prolactin effects
– Weight gain, sedation, diabetes
•48

Antipsychotic/Neuroleptics
Three major groups :
1) Phenothiazines
2) Thioxanthines
3) Butyrophenones
OLDER DRUGS
•49

Antipsychotics/Neuroleptics
Dopamine Synapse
DA
L-DOPA
Tyrosine
Tyrosine
• Old antiphsychotics/neuroleptics are D2
dopamine receptor antagonists. Although they are also effective antagonists at ACh, 5-HT, NE receptors.
dopamine
receptor
antagonist
D2
•50

Antipsychotics/Neuroleptics
• It appears that the specific interaction of antipsychotic drugs with D2 receptors is important to their therapeutic action.
• The affinities of most older “classical” agents for the D2 receptors correlate with their clinical potencies as antipsychotics.
•51

•52
•The potency of antipsychotic drugs in binding to the D2 family of
receptors is proportional to the potency of the drugs in treating
schizophrenia
•This is not true for the potency
of the drugs in blocking histamine
H1, serotonin or α-adrenergic
receptors
•Adapted from Nestler Hyman & Malencka, Molecular Neuropharmacol.ogy, McGraw Hill, c2001, p. 402

Antipsychotics/Neuroleptics
• Both D1 and D2 receptors are found in high concentrations in the striatum and the nucleus accumbens.
• Clozapine has a higher affinity for the D4 receptors than for D2.
• Recently it has been found that most antipsychotic drugs may also bind D3 receptors (therefore, they are non-selective).
•53

Antipsychotics/Neuroleptics
• Antipsychotics produce catalepsy (reduce motor activity).
– BLOCKADE OF DOPAMINE RECPTORS IN BASAL GANGLIA.
• Antipsychotics reverse hyperkinetic behaviors (increased locomotion and stereotyped behavior).
– BLOCKADE OF DOPAMINE RECPTORS IN LIMBIC AREAS.
• Antipsychotics prevent the dopamine inhibition of prolactin release from pituitary.
– BLOCKADE OF DOPAMINE RECEPTORS IN PITUITARY.
hyperprolactinemia•54

Pharmacokinetics
Absorption and Distribution
• Most antipsychotics are readily but incompletely absorbed.
• Significant first-pass metabolism.• Bioavailability is 25-65%.• Most are highly lipid soluble.• Most are highly protein bound (92-98%).• High volumes of distribution (>7 L/Kg).• Slow elimination.**Duration of action longer than expected, metabolites are present
and relapse occurs, weeks after discontinuation of drug.**
•55

Pharmacokinetics
Metabolism
• Most antipsychotics are almost completely metabolized.
• Most have active metabolites, although not important in therapeutic effect, with one exception. The metabolite of thioridazine, mesoridazine, is more potent than the parent compound and accounts for most of the therapeutic effect.
•56

Pharmacokinetics
Excretion
• Antipsychotics are almost completely metabolized and thus, very little is eliminated unchanged.
• Elimination half-lives are 10-24 hrs.
•57

Antipsychotic/Neuroleptics
1) Phenothiazines
Chlorpromazine Thioridazine Fluphenazine
Trifluopromazine Piperacetazine Perfenazine
Mesoridazine Acetophenazine
Carphenazine
Prochlorperazine
Trifluoperazine
• Aliphatic Piperidine Piperazine*
* Most likely to cause extrapyramidal effects.
•58

Antipsychotic/Neuroleptics
[Drug dose]
Piperazine
Aliphatic
Piperidine
•59

Antipsychotic/Neuroleptics
2) Thioxanthines
Thiothixene
Chlorprothixene
Closely related to phenothiazines
•60

Antipsychotic/Neuroleptics
3) Butyrophenones
Haloperidol
Droperidol
•61

Antipsychotic/Neuroleptics
[Drug dose]
Phenothiazine
Thioxanthene
Butyrophenone
•62

Antipsychotics/Neuroleptics
The acute effects of antipsychotics do not explain why their therapeutic effects are not evident until 4-8 weeks of treatment.
Possible reasons are…
•63

Antipsychotics/Neuroleptics
Presynaptic Effects
Blockade of D2 receptors
Compensatory Effects Firing rate and activity of nigrostriatal and mesolimbic DA
neurons.
DA synthesis, DA metabolism, DA release.
Postsynaptic Effects
Depolarization BlockadeInactivation of nigrostriatal and mesolimbic DA neurons.
Receptor Supersensitivity •64

Adverse Effects Summary
• Sedation - initially considerable; tolerance usually develops after a few weeks of therapy; dysphoria
• Postural hypotension - results primarily from adrenergic blockade; tolerance can develop
• Anticholinergic effects - include blurred vision, dry mouth,constipation, urinary retention; results from muscariniccholinergic blockade
• Endocrine effects - increased prolactin secretion can causegalactorhea; results from antidopamine effect
• Hypersensitivity reactions - jaundice, photosensitivity,rashes, agranulocytosis can occur
• Idiosyncratic reactions - malignant neuroleptic syndrome• Weight gain• Neurological side effects - see next
•65

Antipsychotics & Tardive Dyskinesia
•Chronic blockade of D2 receptors leads
•them to up-regulate.
•This may cause involuntary
movements.
•tardive: slow or belated onset
•dyskinesia: presence of involuntary movements, tongue thrusts, lip smacking,
• eye blinking
•Potentially permanent! •66

TD = Extrapyramidal Symptoms (Long-Term)
•Brodal (2010). The central nervous system. p. 83.•67

Extrapyramidal Symptoms (Short-term)
• Pseudo-Parkinsonism:
– tremor
– rigidity
– bradykinesia
• dystonia: involuntary muscle spasms
– torticollis: abnormal head or neck position
• akathisia: severe sensation of restlessness, strong desire to move
•68

Dopamine Inhibits Acetylcholine
•Stahl, S. (2008). Essential Psychopharmacology, p. 338.•69

D2 Inhibition & Increased ACh
•Stahl, S. (2008). Essential Psychopharmacology, p. 339.•70

Solution: Anti-cholinergics
•Stahl, S. (2008). Essential Psychopharmacology, p. 339. •71

Dopamine Inhibits Prolactin
•Stahl, S. (2008). Essential Psychopharmacology, p. 334.
•Consequences
•amenorrhea
•galactorhea
•↓ sex interest
•gynecomastia
•72

Dopamine & Mood
• Dopamine projections to nucleus accumbens
• Increasing dopamine increases reward
• anti-psychotics block this pathway
•73

Non-Selectivity of FGA
•74

Haloperidol
• MOA: D2 antagonist, α1 antagonist
• Indications: acute psychosis/schizophrenia
• Adverse Effects: extrapyramidal symptoms (EPS), hypotension
•75

REACTION FEATURES TIME OF
MAXIMAL RISK
PROPOSED
MECHANISM
TREATMENT
Acute dystonia Spasm of muscles of tongue,
face, neck, back; may mimic
seizures; not hysteria
1 to 5 days Unknown Antiparkinsonian agents are
diagnostic and curative
Akathisia Motor restlessness; not
anxiety or "agitation"
5 to 60 days Unknown Reduce dose or change drug:
antiparkinsonian agents,b
benzodiazepines or
propranololc may help
Parkinsonism Bradykinesia, rigidity,
variable tremor, mask facies,
shuffling gait
5 to 30 days Antagonism of
dopamine
Antiparkinsonian agents
helpful
Neuroleptic
malignant
syndrome
Catatonia, stupor, fever,
unstable blood pressure,
myoglobinemia; can be fatal
Weeks; can persist for
days after stopping
neuroleptic
Antagonism of
dopamine may
contribute
Stop neuroleptic
immediately: dantrolene or
bromocriptined may help:
antiparkinsonian agents not
effective
Perioral tremor
("rabbit" syndrome)
Perioral tremor (may be a
late variant of parkinsonism)
After months or years
of treatment
Unknown Antiparkinsonian agents
often help
Tardive dyskinesia Oral-facial dyskinesia;
widespread choreoathetosis
or dystonia
After months or years
of treatment (worse on
withdrawal)
Excess function of
dopamine
hypothesized
Prevention crucial; treatment
unsatisfactory
a. Many drugs have been claimed to be helpful for acute dystonia. Among the most commonly employed treatments are diphenhydramine hydrochloride, 25 or 50 mg
intramuscularly, or benztropine mesylate, 1 or 2 mg intramuscularly or slowly intravenously, followed by oral medication with the same agent for a period of days to
perhaps several weeks thereafter. b. Propranolol often is effective in relatively low doses (20-80 mg per day). Selective beta1-adrenergic receptor antagonists are less
effective. c. Despite the response to dantrolene, there is no evidence of an abnormality of Ca2+ transport in skeletal muscle; with lingering neuroleptic effects,
bromocriptine may be tolerated in large doses (10-40 mg per day).
Neurological Side Effects of antipsychotics
•77

FGA Side effects
Weight gain – 40% - weight gain now attributed to ratio of binding to D2 and 5-HT2 receptors; possibly also histamine (for newer antipsychotics anyway)
Sexual dysfunction
result from NE and SE blockade
erectile dysfunction in 23-54% of men
retrograde ejaculation in
loss of libido and anorgasmia in men and women
Seizures - <1% for generalized grand mal
•78

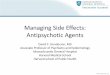
•ESTIMATED MEAN WEIGHT GAIN AT 10 WEEKS
•Allison DB, •Mentore •JL, •Heo •M, et al: Weight gain associated with conventional
•and newer •antipsychotics •: a meta•- •Analysis. AJP, 1999.
•0
•1
•2
•3
•4
•5
•-1
• Mean c
hange in b
ody w
eig
ht
(kg)
•A comprehensive literature search identified 78 studies that included data on weight change in patients treated with a specific antipsychotic.
•For each agent a meta-analysis and random effects regression estimated the change in weight at 10 weeks of treatment.
•79

Summary: Pros & Cons• FGAs have strong efficacy against + symptoms.
• FGAs either do not help – symptoms or exacerbate them.
• The primary concern with FGAs is long-term development of tardive dyskinesia although acute EPS impair the quality of life of schizophrenics.
•Stahl, S. (2008). Essential Psychopharmacology, p. 369. •80

ARRIVAL OF THE ATYPICAL ANTIPSYCHOTIC
• “German psychiatrists working with G. Stille at Wander Pharmaceuticals in Bern, Switzerland, in the early 1960s worked to refute that EPS and antipsychotic efficacy were linked. Their work led to the introduction of Clozapine, an antipsychotic with no EPS.”
• Clozapine was briefly marketed and quickly withdrawn for two reasons:– The embarrassment of not having any EPS, and
– Agranulocytosis
•81

Antipsychotic/Neuroleptics
Pimozide
Molindone
Loxapine
Clozapine
Olanzapine
Qetiapine
Risperidone
Sertindole
Ziprasidone
Olindone
Newer Drugs
•82

Atypical antipsychotics
MARTA (multi acting receptor targeted agents)
• clozapine, olanzapine, quetiapine
SDA (serotonin-dopamine antagonists)
• risperidone, ziprasidone, sertindole
Selective D2/D3 antagonists
• sulpiride, amisulpiride
•83

NEUROBIOLOGY OF CLOZAPINE
•Here you can see that Clozapine will not bind to any Dopamine
receptor, it is selective, it has an affinity for the D4 receptor subtype.
•84

Atypical (Second Generation)
• Mechanism of Action
– Dissociate more rapidly from the D2 receptor
•Stahl, S. (2008). Essential Psychopharmacology, p. 369-370.•85

MOA of Atypical Antipsychotics
• Dissociate more rapidly from the D2 receptor
– ↓ acute EPS, ↓ hyperprolactinemia
•Stahl, S. (2008). Essential Psychopharmacology, p. 371. •86

MOA of Atypicals• Atypicals
– Dissociate more rapidly from the D2 receptor
– Block the 5-HT2A (and so many other!) receptors
•Stahl, S. (2008). Essential Psychopharmacology, p. 384.
•87

•88

Risks with long-term Atypicals
•Mechanism: 5-HT2C
•Mechanism: X
•$515 Million
•89

• SGAs produce less acute EPS than FGA but also cause diabetes.
• No clear consensus exists in the choice between FGA and SGA.
• Using agents at above recommended doses or combining drugs are common clinically but are not well studied.
•90

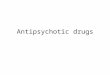
•Receptor/Adverse Effect
•X: diabetes
•M1: sedation
•H1: sedation, appetite
•α1: sedation
•5-HT2C: appetite
•Stahl, S. (2008). Essential Psychopharmacology, p. 384.•91

Neuroleptic Malignant Syndrome
Is a rare but serious side effect of neuroleptic(antipsychotic) therapy that can be lethal. It can arise at any time in the course of treatment and shows no predilection for age, duration of treatment, antipsychotic medication, or dose.
•94

Neuroleptic Malignant Syndrome
• Occurs in pts. hypersensitive to the Ex.Py. effects of antipsychotics.
• Due to excessively rapid blockade of postsynaptic dopamine receptors.
• The syndrome begins with marked muscle rigidity.
• If sweating is impaired, a fever may ensue. The stress leukocytosis and high fever associated with this syndrome may be mistaken for an infection.
• Autonomic instability with altered blood pressure and heart rate is another midbrain manifestation.
• Creatine kinase isozymes are usually elevated, reflecting muscle damage.
•95

Antipsychotic/Neuroleptics
Neuroleptic Malignant Syndrome
Treatment Vigorous treatment with antiparkinsonian drugs is
recommended as soon as possible.
Muscle relaxants such as diazepam, dantrolene or bromocriptine may be helpful.
•96

Antipsychotic/Neuroleptics
Drug Interactions• Additive effects with sedatives.
• Additive effects with anticholinergics.
• Additive effects with antihistaminergics.
• Additive effects with -AR blocking drugs.
• Additive effects with drugs with quinidine-like action (thioridazine).
•97

•98

• The most important are those on the cardiovascular,
• central and autonomic nervous systems, and endocrine system. Other dangerous
• effects are seizures, agranulocytosis, cardiac toxicity, and pigmentary degeneration of the retina, all
• of which are rare
TOXIC REACTIONS AND ADVERSE EFFECTS
•99

•100

Psychosis-Producing Drugs
1) Levodopa
2) CNS stimulants
a) Cocaine
b) Amphetamines
c) Khat, cathinone, methcathinone
3) Apomorphine
4) Phencyclidine
•108

•113