Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 41, No. 1, 1962
ADRENOCORTICOTROPICHORMONEIN HUMANPLASMA*
By VERNONK. VANCEJWILLIAM J. REDDY, DONH. NELSONi: ANDGEORGEW. THORN
(From the Department of Medicine, Harvard Medical School, andd the Peter Bent BrighamHospital, Boston, Mass.)
(Submitted for publication October 24, 1960; accepted September 21, 1961)
Utilizing the bioassay of Sayers, Sayers andWoodbury (1), based upon adrenal ascorbic aciddepletion in the hypophysectomized rat, Paris (2),Taylor (3), and Sydnor (4, 5) and their co-work-ers, were unable to find detectable levels of ACTHin normal subjects. Gaarenstroom and his col-leagues (6) observed detectable quantities in 7 of33 normal subjects. Others (7-12) have reportedvery high concentrations. Sayers (13) discountedthese latter reports as being inconsistent with theobservation (14) that ACTH causes a maximaladrenal response in doses calculated to give muchlower plasma concentrations. He concluded thatthe normal concentration is less than 0.5 mUper100 ml of blood. Fujita (15) concluded from hisstudies that the normal concentration of ACTHinwhole blood was 1.0 mUper 100 ml.
The bioassay, using the secretion of adrenal ster-oids in the hypophysectomized dog after adminis-tration of a test substance (16), provided a moredirect method of measuring ACTH, but thismethod was not sensitive enough to allow meas-urement of ACTH in the plasma of normal hu-mans. The development of a method for the meas-urement of corticosterone1 in small quantities ofrat plasma (17, 18) permitted the application ofthy principle of measurement of adrenal venouscorticosteroids to the hypophysectomized rat (19).The rat bioassay for ACTHproved to be sensi-
* Supported in part by grants from the John A. Hart-ford Foundation, Inc., the United States Public HealthService, and the United States Army Medical Researchand Development Command, Department of the Army(DA-49-007-MD-135).
t This work was done as an Advanced Research Fel-low of the American Heart Association.
t Investigator, Howard Hughes Medical Institute.Present address: Department of Medicine, University ofSouthern California, School of Medicine, Los Angeles,Calif.
1 Corticosterone: 11 ,,21 -dihydroxy-4-pregnene-3,20-di-one.
tive to 0.01 mUper 100 g, or 0.02 mUper 200 grat.
The present study applies the rat bioassay tothe measurement of ACTH in the plasma of nor-mal subjects, patients with pituitary or adrenaldisorders or both, and subjects or patients givensubstances which presumably stimulate the pitui-tary-adrenal axis.
MATERIALS AND METHODS
Subjects and patients. Thirteen normal adult labora-tory workers, 7 patients with Cushing's syndrome due toadrenal hyperplasia, 4 with ACTH-producing pituitarytumors following adrenalectomy for adrenal hyperplasia,14 with hypoadrenalcorticism, and 3 with panhypopitui-tarism were studied. All patients and subjects were stud-ied on the Metabolic Ward of the Peter Bent BrighamHospital with the following exceptions: plasma fromPatient M.R. was kindly supplied by Drs. FrederickGoetz and Walter Moran; plasma from Patients L.C.and R.A. was kindly supplied by Drs. Arnold Relmanand James Hudson; plasma from Patient R.F. was kindlysupplied by Dr. William Daughaday.
Preparation of plasma for assay. Blood for baselinestudies was drawn between 8 and 9 a.m. into a syringepreviously moistened with heparin, immediately placed inplastic tubes and centrifuged at high speed in a cold room(0 to 4° C) for 10 minutes. The plasma was separatedinto a test tube which was sealed and kept frozen untilthe assay for ACTH. All tubes and pipets were rinsedwith 0.01 N HCl in 0.9 per cent saline solution prior totheir use. Some of the normal specimens were preparedby lyophilizing 10-ml aliquots of plasma and diluting thedried portion to 5 ml with 0.01 N HCl.
Assay of ACTH. Assays were performed by a slightmodification of the method of Lipscomb and Nelson (19).Female Sprague-Dawley rats weighing 200 to 225 gwere anesthetized with ether. Anesthesia was maintainedby cannulating the trachea with one end of a polyethylenecatheter and placing the other end in a test tube containinga sponge saturated with ether. Hypophysectomy wasperformed via the transpharyngeal approach under directobservation with a dissecting microscope. Two hourslater the animal was reanesthetized and a cut-down wasperformed on the right femoral vein. The inferior epi-gastric vein was dissected free, clamped, and divided dis-
20
ACTH IN HUMANPLASMA
tal to the clamp. Applying light traction to the clampanchored the femoral vein, facilitating venipuncture.The test solution was injected into the femoral veinwithin 30 seconds. Three minutes after injection theperitoneal cavity was entered through a wide transverseincision. The stomach, spleen and intestines were packedto the right and the liver suspended with a saline-moist-ened sponge, allowing good visualization of the left re-nal and adrenal veins and the left adrenal gland. Therenal vein was grasped with forceps, and exactly 5 min-utes after injection of the test solution the left adrenalvein was cannulated (20) by advancing a 21- to 23-gageneedle through the renal vein into the adrenal vein untilit was lodged in the vein. Adrenal venous blood wasthen drawn for 4 minutes into a tuberculin syringe whichpreviously had been moistened with heparin and attachedto the needle. No attempt was made to ligate the non-adrenal tributaries to the adrenal vein, although some ofthem were bypassed by advancing the needle as far aspossible into the adrenal vein. The blood drawn wasthus a mixture of adrenal and systemic venous blood(21). The blood was placed in a hematocrit tube, cen-trifuged, and the plasma was separated. Total plasmaremoved in 4 minutes was computed from the readings onthe hematocrit tube of the total and cellular componentsof the blood and from the known total volume of thepreviously calibrated hematocrit tube; 0.2-ml aliquots ofplasma were analyzed for corticosterone concentrationby estimation of H2SO4-induced fluorescence (17, 18) andminute output of corticosterone was computed.
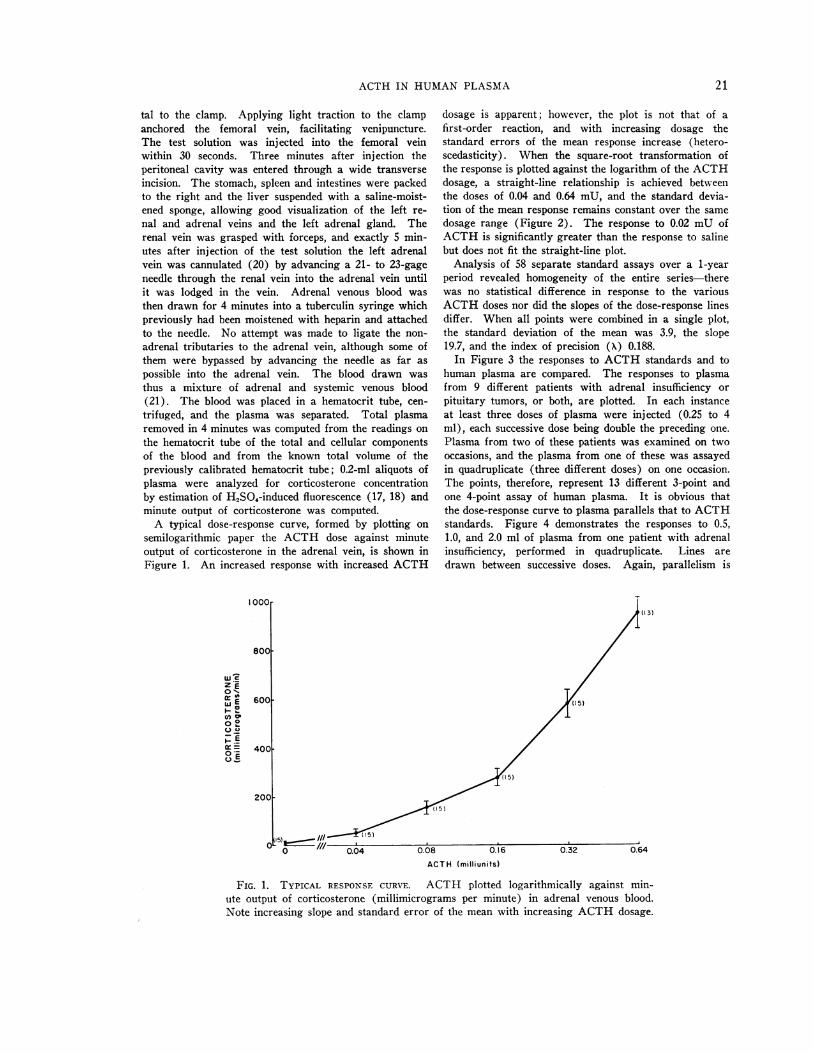
A typical dose-response curve, formed by plotting onsemilogarithmic paper the ACTH dose against minuteoutput of corticosterone in the adrenal vein, is shown inFigure 1. An increased response with increased ACTH
'0oor
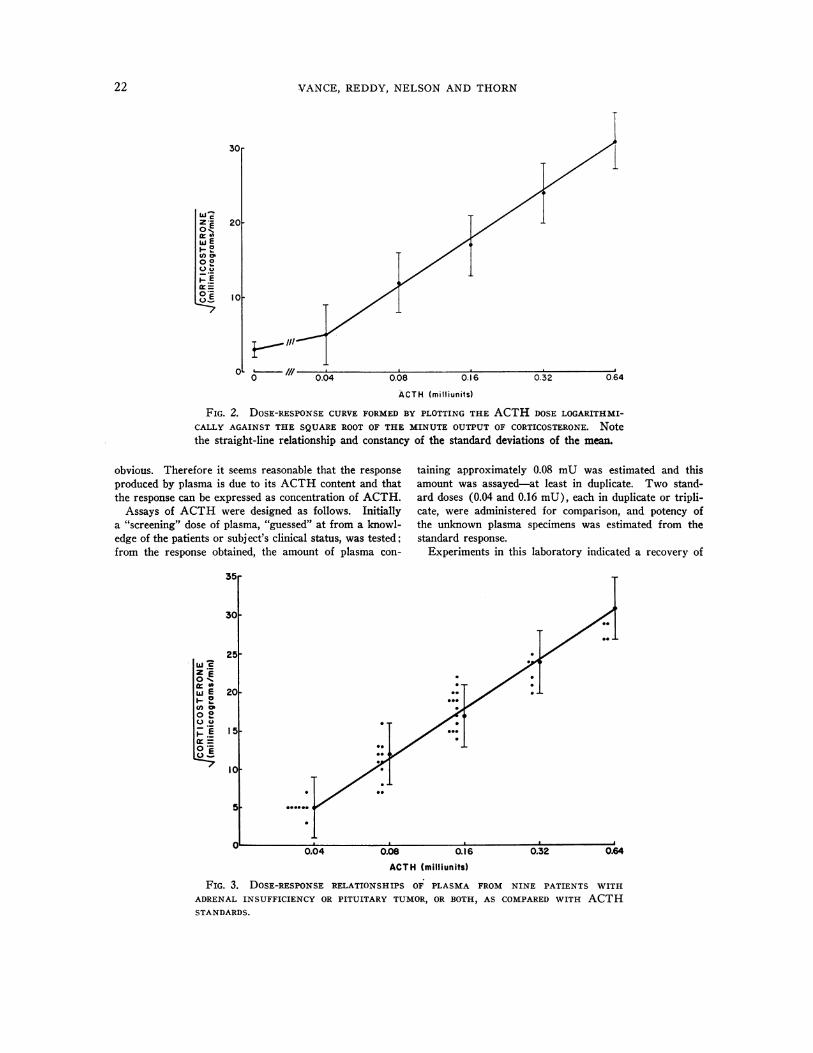
dosage is apparent; however, the plot is not that of afirst-order reaction, and with increasing dosage thestandard errors of the mean response increase (hetero-scedasticity). When the square-root transformation ofthe response is plotted against the logarithm of the ACTHdosage, a straight-line relationship is achieved betweenthe doses of 0.04 and 0.64 mU, and the standard devia-tion of the mean response remains constant over the samedosage range (Figure 2). The response to 0.02 mUofACTHis significantly greater than the response to salinebut does not fit the straight-line plot.
Analysis of 58 separate standard assays over a 1-yearperiod revealed homogeneity of the entire series-therewas no statistical difference in response to the variousACTHdoses nor did the slopes of the dose-response linesdiffer. When all points were combined in a single plot,the standard deviation of the mean was 3.9, the slope19.7, and the index of precision (X) 0.188.
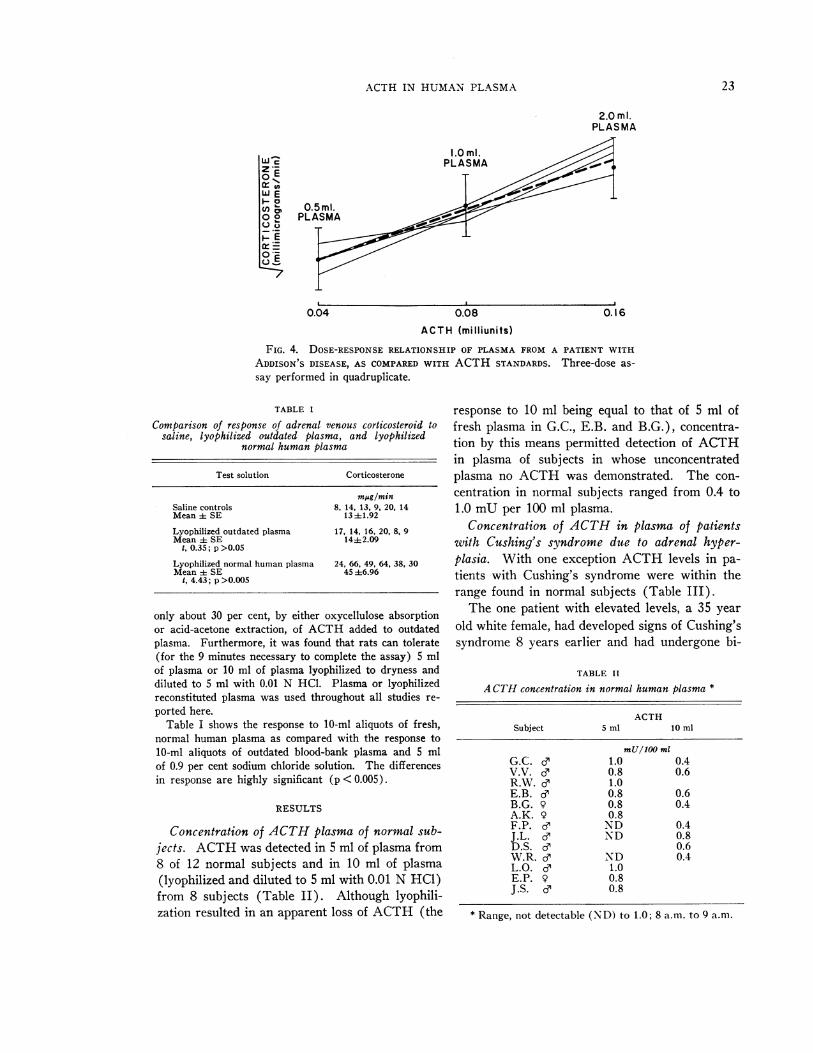
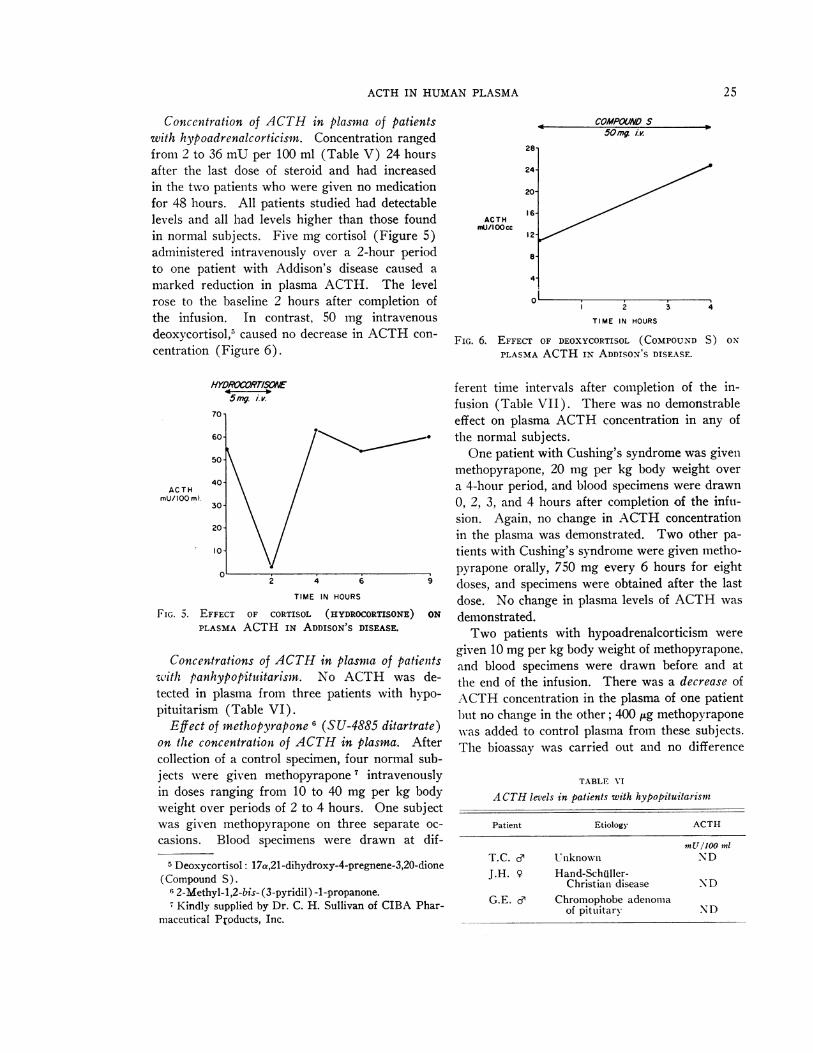
In Figure 3 the responses to ACTH standards and tohuman plasma are compared. The responses to plasmafrom 9 different patients with adrenal insufficiency orpituitary tumors, or both, are plotted. In each instanceat least three doses of plasma were injected (0.25 to 4ml), each successive dose being double the preceding one.Plasma from two of these patients was examined on twooccasions, and the plasma from one of these was assayedin quadruplicate (three different doses) on one occasion.The points, therefore, represent 13 different 3-point andone 4-point assay of human plasma. It is obvious thatthe dose-response curve to plasma parallels that to ACTHstandards. Figure 4 demonstrates the responses to 0.5,1.0, and 2.0 ml of plasma from one patient with adrenalinsufficiency, performed in quadruplicate. Lines aredrawn between successive doses. Again, parallelism is
(13)
800O
c c
Z E0 -,cr GA
O °P0 .2,I_ E
cr=oi*_ 600
4001
'15)
2001
0.04 0.08 0.16
ACTH (milliunits)
0.32 0.64
FIG. 1. TYPICAL RESPONSECURVE. ACTH plotted logarithmically against min-ute output of corticosterone (millimicrograms per minute) in adrenal venous blood.Note increasing slope and standard error of the mean with increasing ACTHdosage.
21
VANCE, REDDY, NELSONAND THORN
30r
WEir 0wE
o °pt0
.
I-E0. =0 Eg
20I
101
0
i- ill
0 0.04 0.08 0.16
ACTH (milliunits)
FIG. 2. DOSE-RESPONSECURVEFORMEDBY PLOTTING THE ACTHDOSE LOGARITHMI-
CALLY AGAINST THE SQUAREROOT OF THE MINUTE OUTPUTOF CORTICOSTERONE. Notethe straight-line relationship and constancy of the standard deviations of the mean.
obvious. Therefore it seems reasonable that the response
produced by plasma is due to its ACTHcontent and thatthe response can be expressed as concentration of ACTH.
Assays of ACTHwere designed as follows. Initiallya "screening" dose of plasma, "guessed" at from a knowl-edge of the patients or subject's clinical status, was tested;from the response obtained, the amount of plasma con-
taining approximately 0.08 mU was estimated and thisamount was assayed-at least in duplicate. Two stand-ard doses (0.04 and 0.16 mU), each in duplicate or tripli-cate, were administered for comparison, and potency ofthe unknown plasma specimens was estimated from thestandard response.
Experiments in this laboratory indicated a recovery of
35r
30[
251W 'Z *E
,,, E0%
(n P020 °.
0 .2
._-
=
,-g
20pa
10-
5
0.04 0.08 0.16 0.32 0.64
ACTH (milliunits)
FIG. 3. DOSE-RESPONSERELATIONSHIPS OF PLASMA FROM NINE PATIENTS WITH
ADRENAL INSUFFICIENCY OR PITUITARY TUMOR, OR BOTH, AS COMPAREDWITH ACTHSTANDARDS.
0.32 0.64
22
ACTH IN HUMANPLASMA
2.0 ml.PLASMA
1.0 ml.PLASMA
0.04 0.08
ACTH (milliunits)
FIG. 4. DOSE-RESPONSERELATIONSHIP OF PLASMA FROMA PATIENT WITH
ADDISONS DISEASE, AS COMPAREDWITH ACTHSTANDARDS. Three-dose as-
say performed in quadruplicate.
TABLE 1
Comparison of response of adrenal venous corticosteroid tosaline, Iyophilized outdated plasma, and Iyophilized
normal human plasma
Test solution Corticosterone
mjsg/minSaline controls 8, 14, 13, 9, 20, 14Mean i SE 13±1.92
Lyophilized outdated plasma 17, 14, 16, 20, 8, 9Mean ± SE 14+2.09
1, 0.35; p >0.05
Lyophilized normal human plasma 24, 66, 49, 64, 38, 30Mean ±t SE 45 46.96
t, 4.43; p >0.005
only about 30 per cent, by either oxycellulose absorptionor acid-acetone extraction, of ACTHadded to outdatedplasma. Furthermore, it was found that rats can tolerate(for the 9 minutes necessary to complete the assay) 5 mlof plasma or 10 ml of plasma lyophilized to dryness anddiluted to 5 ml with 0.01 N HCL. Plasma or lyophilizedreconstituted plasma was used throughout all studies re-
ported here.Table I shows the response to 10-ml aliquots of fresh,
normal human plasma as compared with the response to10-ml aliquots of outdated blood-bank plasma and 5 mlof 0.9 per cent sodium chloride solution. The differencesin response are highly significant (p < 0.005).
RESULTS
Concentration of ACTHplasma of normal sub-jects. ACTHwas detected in 5 ml of plasma from8 of 12 normal subjects and in 10 ml of plasma(lyophilized and diluted to 5 ml with 0.01 N HCl)from 8 subjects (Table II). Although lyophili-zation resulted in an apparent loss of ACTH (the
response to 10 ml being equal to that of 5 ml offresh plasma in G.C., E.B. and B.G.), concentra-tion by this means permitted detection of ACTHin plasma of subjects in whose unconcentratedplasma no ACTHwas demonstrated. The con-centration in normal subjects ranged from 0.4 to1.0 mUper 100 ml plasma.
Concentration of ACTH in plasma of patientswith Cushing's syndrome due to adrenal hyper-plasia. With one exception ACTH levels in pa-tients with Cushing's syndrome were within therange found in normal subjects (Table III).
The one patient with elevated levels, a 35 yearold white female, had developed signs of Cushing'ssyndrome 8 years earlier and had undergone bi-
TABLE II
ACTHconcentration in normal human plasma *
ACTHSubject 5 ml 10 ml
mU/100 mlG.C. o, 1.0 0.4V.V. e 0.8 0.6R.W. e 1.0E.B. o, 0.8 0.6B.G. 9 0.8 0.4A.K. 9 0.8F.P. e ND 0.4J.L. e ND 0.8D.S. d 0.6W.R. , ND 0.4L.O. e 1.0E.P. 9 0.8J.S. e 0.8
* Range, not detectable (ND) to 1.0; 8 a.m. to 9 a.m.
Z(._
c
z vi0
0
0.cam
en CD
_ ._
,- E
°E
0.5 ml.PLASMA
0.16
23

VANCE, REDDY, NELSONAND THORN
TABLE III
ACTHlevels in Cushing's syndrome
Patient ACTH
mU/100 ml plasmaF.C. o, 0.6G.T. 9 0.8M.R. cP 0.8G.A.* 9 2.2-4.0F.G. 9 0.8F.S. 9 0.8M.F. 9 0.8
* Recurrent Cushing'sadrenalectomy.
syndrome following subtotal
lateral adrenalectomy three years previously. Theleft adrenal gland was ruptured during removal.Postoperative steroid excretion was low and shewas given cortisone 2 maintenance therapy. How-ever, there was no remission of the signs of Cush-ing's syndrome, but rather a progression; on ad-mission she presented the classical clinical andlaboratory signs of the disease. Skull X-rays weresuggestive of sellar enlargement, and laminogramsof the left suprarenal area suggested a suprarenalmass. This area was explored and 6 g of histo-logically hyperplastic adrenal tissue was removed.Postoperative steroid excretion was consistent withtotal adrenalectomy, and substitution therapy wasprescribed. There was marked amelioration of thesigns of Cushing's syndrome. Unfortunately thepatient died of a coronary occlusion at home 3months postoperatively. No postmortem examina-tion was performed. Because of the elevatedplasma ACTH and suggestive skull X-rays, thepresence of a pituitary tumor was suspected.
Concentration of ACTH in plasma of patientswith ACTH-producing tumors of the pituitarygland. Plasma levels ranged from 12 to 330 mU
TABLE IV
Plasma A CTHin patients with pituitary tumors
ACTH
Aftersuppres- Hypo-sion with X-ray, phys-
Patient Initial cortisol Rx ectomy
mU/100 ml mU/100 mlN.C. 12 1 1L.C. 330 6 12E.C. 32 32 30R.F. 26
2 Cortisone: 17a,21-dihydroxy-4-pregnene-3,11,20-trione.
per 100 ml among the four patients studied (TableIV). Patient L.C., with the highest initial con-centration, had marked suppression of plasmaACTH after the intravenous infusion of 20 mgcortisol 3 over a 4-hour period and a marked re-duction also followed pituitary irradiation. Pa-tient N.C., with recurrent Cushing's syndrome fol-lowing subtotal adrenalectomy, was deeply pig-mented and plasma ACTHwas found to be ele-vated. Routine skull films were normal, but sub-sequent laminograms revealed asymmetrical en-largement of the sella turcica. Intravenous corti-sol caused a reduction in plasma ACTH. Afterpituitary irradiation there was amelioration of the
TABLE V
Plasma ACTHin patients with hypoadrenalcorticism
ACTHPatient 24 hrs after steroid
mU/100 mlAddison's diseaseM.McG. 9 19M.L. 9 2
55 (48 hrs)H.H.W. e 3L.W. e 2E.D. e 4M.C. 9 14
20 (48 hrs)M.M. 9 36F.L. 9 2
AdrenalectomyD.L. 9 2L.D. 9 3B.A. 9 4A.K. 9 12A.C. 9 4R.A. o 3
clinical and laboratory signs of Cushing's syn-drome, a loss of pigmentation, and a marked re-duction of plasma ACTH. Patient E.C. had nodecrease in plasma ACTHafter intravenous cor-tisol; hypophysectomy was attempted but only aportion of the tumor could be removed. Therewas no decrease in plasma ACTHpostoperatively.Tissue culture of the tumor was done 4 and ACTHwas found in aliquots from three consecutivechanges of culture medium. Histologically, thetumor was a chromophobe adenoma.
3 Cortisol: 11,6,17a,21-trihydroxy-4-pregnene-3,20-dione.4 By Dr. Daniel Pugh, Laboratory for Surgical Re-
search, Peter Bent Brigham Hospital and Harvard Medi-cal School, Boston, Mass.
24
ACTH IN HUMANPLASMA
Concentration of ACTH in plasma of patientswith hYpoadrenalcorticisn. Concentration rangedfrom 2 to 36 mUper 100 ml (Table V) 24 hoursafter the last dose of steroid and had increasedin the two patients who were given no medicationfor 48 hours. All patients studied had detectablelevels and all had levels higher than those foundin normal subjects. Five mg cortisol (Figure 5)administered intravenously over a 2-hour periodto one patient with Addison's disease caused a
marked reduction in plasma ACTH. The levelrose to the baseline 2 hours after completion ofthe infusion. In contrast, 50 mg intravenousdeoxycortisol,5 caused no decrease in ACTHcon-
centration (Figure 6).
HYDRORTISONtE5mg. iv.
70 -
60
50-
40-
ACTH
mU/1OOml.
30
20-
10-
2 4 6 9
TIME IN HOURS
FIG. 5. EFFECT OF CORTISOL (HYDROCORTISONE) ON
PLASMA ACTH IN ADDISON'S DISEASE.
Concentrations of ACTHin plasma of patientswith panhypopituitarism. No ACTH was de-tected in plasma from three patients with hypo-pituitarism (Table VI).
Effect of mnethopyrapone 6 (SU-4885 ditartrate)on the concentration of ACTHin plasma. Aftercollection of a control specimen, four normal sub-jects were given methopyrapone 7 intravenouslyin doses ranging from 10 to 40 mg per kg bodyweight over periods of 2 to 4 hours. One subjectwas given methopyrapone on three separate oc-
casions. Blood specimens were drawn at dif-
5 Deoxycortisol: 17a,21-dihydroxy-4-pregnene-3,20-dione(Compound S).
6 2-Methyl-1,2-bis- (3-pyridil) -1-propanone.
dKindly supplied by Dr. C. H. Sullivan of CIBA Phar-maceutical Products, Inc.
COMPOUNDS50mg. i;.
28
24
ACTHmU/I 00cc
20
16
12
8'
4.
2
TIME IN HOURS
3 4
FIG. 6. EFFECT OF DEOXYCORTISOL (COMPOUNDS) ONPLASMAACTH IN- ADDISON'S DISEASE.
ferent time intervals after completion of the in-fusion (Table VII). There was no demonstrableeffect on plasma ACTH concentration in any ofthe normal subjects.
One patient with Cushing's syndrome was givenmethopyrapone, 20 mg per kg body weight overa 4-hour period, and blood specimens were drawn0, 2, 3, and 4 hours after completion of the infu-sion. Again, no change in ACTHconcentrationin the plasma was demonstrated. Two other pa-tients with Cushing's syndrome were given metho-pyrapone orally, 750 mg every 6 hours for eightdoses, and specimens were obtained after the lastdose. No change in plasma levels of ACTHwasdemonstrated.
Two patients with hypoadrenalcorticism weregiven 10 mgper kg body weight of methopyrapone.and blood specimens were drawn before and atthe end of the infusion. There was a decrease ofACTHconcentration in the plasma of one patientl)tlt no change in the other; 400 jig methopyraponewas added to control plasma from these subjects.The bioassay was carried out and no difference
TABLE VI
A CTHlevels in patients with hypopituitarisnm
Patient Etiology ACTH
mU/100 mlT.C. Uiinknowni ND
J.H. 9 Hand-Schuhler-Christian disease ND
G.E. d Chromophobe adenomiaof pituitary ND
25

VANCE, REDDY, NELSONANDTHORN
TABLE VII
Effect of methopyrapone on plasma ACTH
Plasma ACTH
Methopyrapone Hours after end of infusion
Subject Diagnosis Dose Time Control 0 1 1 2 4
mg/kg hrs mU/100 mlB.G. Normal 10 2 1.0 ND ND ND NDA.K. Normal 10 2 1.0 ND NDB.G. Normal 20 2 1.0 ND ND ND NDB.G. Normal 20 4 1.0 0.8 ND ND 1.0J.S. Normal 30 4 1.0 0.8 1.0 1.0E.P. Normal 40 4 0.8 0.8 0.8 1.6M.L. Addison's 10 2 40.0 24 26 28M.C. Addison's 10 2 14.0 13 13 13 14F.S. Cushing's 20 4 0.8 1.0 1.0 ND
was found between the samples with and withoutadded methopyrapone.
Effect of purified- lipopolysaccharide pyrogenon concentration of ACTH in plasma. Lipexal,in doses of 0.1 ptg (0.2 ml) and 0.25 /Ag (0.5 ml)was administered intravenously to one normal sub-ject on two different occasions. Elevations of tem-perature to 101.80 and 102.40 F, respectively, oc-curred 90 and 120 minutes after injection on bothoccasions and persisted for 5 to 6 hours. Therewas no demonstrable increase in plasma ACTHconcentration on either occasion (Table VIII).
DISCUSSION
ACTHwas found in the plasma of 13 normalsubjects in concentrations ranging from 0.4 to 1.0mUper 100 ml plasma (Table II). These valuesare of the same magnitude as those predicted bySayers (13) and found by Fujita (15).
In patients with Cushing's syndrome, concen-trations were within the normal range with one
Effect of Lipexal on
TABLE VIII
plasma ACTH in a normal subject
ACTHTime after
injection Lipexal, lyg Lipexal, 2.5 pAg
mU/100 ml0 1.0 0.85 min 0.8 0.8
15 min 0.8 0.860 min ND 0.890 min 0.8 ND
2 hrs 1.4 1.03 hrs 1.0 1.05 hrs 1.0
8Kindly supplied as
Jr., of the Wander Co.Lipexal by Dr. Fred H. Schultz,
exception. As mentioned, a pituitary tumor wassuspected but not proven in this patient. Thefinding of elevated levels in a patient with Cush-ing's syndrome should suggest the presence of apituitary tumor and, if the tumor cannot be dem-onstrated radiologically, the possibility of an oc-cult tumor must be considered and follow-upX-rays taken periodically.
The patients with proven pituitary tumors fol-lowing adrenalectomy for Cushing's syndromepresented here have not been reported previously.As was expected, all were found to have elevatedlevels of ACTHin the plasma. In contrast to thegroup of patients previously reported by Nelsonand co-workers, (22-24), only one of the presentgroup had a level of ACTH higher than thosefound in some patients with Addison's disease.There appeared to be a correlation between theability to cause a decrease in plasma ACTHwithcortisol and the response to irradiation or hypo-physectomy, or both, in the three patients in whomthe suppression test was performed. Althoughone cannot generalize from this small series, thesuppression test may have prognostic value.
The concentrations found in patients with hypo-adrenalcorticism are of the same order as thosefound by Sydnor, Sayers, Brown and Tyler (4)and by Bethune, Nelson and Thorn (25). How-ever, in the current study, all of the patients haddetectable levels and all of the levels were higherthan those found in normal subjects. The dif-ference can be explained by the much greater sen-sitivity of the present bioassay. The finding ofelevated levels in patients suspected of having Ad-dison's disease appears to be diagnostic of thatcondition.
26

ACTH IN HUMANPLASMA
The three highest plasma ACTHvalues in pa-tients with hypoadrenalcorticism were in thosewith Addison's disease. However, there was noapparent difference between the levels in patientswith Addison's disease and those who had beenadrenalectomized. Williams, Island, Oldfield andLiddle (26) have reported that patients who havepreviously been adrenalectomized for Cushing'ssyndrome have definitely higher plasma ACTHconcentrations after being given sufficient oralcortisol to maintain normal cortisol levels thanhave patients with Addison's disease. These find-ings are surprising in view of the present obser-vation that patients with Cushing's syndrome donot have elevated levels, and that in certain casesthe secretion of ACTH by pituitary tumors iseasily suppressed by the intravenous infusion ofcortisol.
Increases in plasma 17-hydroxycorticosteroidsor urinary 17-hydroxycorticosteroids or both, or of17-ketosteroids or 17-ketogenic steroids after ad-ministration of methopyrapone have been reportedby Liddle (27) and Jenkins (28) and their col-leagues, and by Gold, Di Raimondo and Forsham(29). These authors have postulated an increasedACTHsecretion secondary to a decreased cortisolsecretion as the mechanism of this response. In-creases in plasma or urinary steroids after the in-fusion of bacterial pyrogens, presumably due toincreased secretion of ACTHby the pituitary, alsohave been demonstrated (30-32).
In this study neither methopyrapone nor Lipexalcaused a clear-cut increase in plasma ACTHcon-centration. By the present technique a rise ofplasma ACTHcan be demonstrated readily afterdiscontinuing intravenously administered cortisol(ascending line of curve, Figure 5), or discontinu-ing maintenance therapy in patients with Addi-son's disease. The failure to demonstrate an in-crease of plasma ACTHafter methopyrapone sug-gests that this compound does not act simply bysuppression of cortisol production. The lack ofACTHresponse cannot be attributed to the pres-ence of methopyrapone itself in the plasma sam-ples, since the bioassay of ACTHwas not affectedby the addition of methopyrapone to plasma invitro. Since deoxycortisol did not lower theACTH level when 50 mg was infused over a4-hour period in a patient with Addison's disease,it does not seem likely that the increase in deoxy-
cortisol secretion associated with methopyraponeadministration would inhibit a measurable rise inACTH. In contrast to the reported observationthat plasma ACTH increases in the adrenalecto-mized dog after infusion of methopyrapone (33),no increase was noted in two patients with hypo-adrenalcorticism.
In the above situations it is possible that a slightincrease in ACTH did occur which the bioassaywas not capable of detecting. It is also possiblethat there was an increase in ACTHproductionthat was not reflected in an increase in the plasmalevel because of a corresponding increase in therate of removal. In view of the data presented itappears most likely that the increase in steroidsecretion after methopyrapone or bacterial pyro-gens is due to a direct effect of these substanceson the adrenal cortex. However, the presence ofACTHappears to be necessary in order to dem-onstrate an effect of methopyrapone-as indicatedby a negative response in patients with hypopitui-tarism and in patients or subjects receiving sup-plementary fluorocortisol.9
SUMMARY
Adrenocorticotropic hormone was assayed bythe measurement of corticosterone in the adrenalvenous plasma of the hypophysectomized rat afterthe intravenous administration of plasma. Theassay is more sensitive than are previous tech-niques, enabling the detection of 0.04 mU ofACTH. Plasma from normal subjects was foundto contain ACTH in levels ranging from 0.4 to1.0 mUper 100 ml. Patients with Cushing's syn-drome due to adrenal cortical hyperplasia did nothave elevated levels. All the patients with hypo-adrenalcorticism have elevated levels, and noACTHwas detected in patients with panhypopi-tuitarism. No elevations of plasma ACTHwerenoted after administration of methopyrapone(SU-4885) or a bacterial pyrogen.
ACKNOWLEDGMENT
The authors wish to acknowledge the technical as-sistance of Miss Beatrix Gassmann and the assistance ofDr. Paul Munson and Mrs. Elizabeth A. Moore in thestatistical evaluation of data.
9 Fluorocortisol: 9ca,fluoro-11,17a-21-trihydroxy-4-preg-nene-3,20-dione.
27

VANCE, REDDY, NELSONAND THORN
REFERENCES1. Sayers, M. A., Sayers, G., and Woodbury, L. A.
The assay of adrenocorticotrophic hormone by theadrenal ascorbic acid-depletion method. Endo-crinology 1948, 42, 379.
2. Paris, J., Upson, M., Jr., Sprague, R. G., Salassa,R. M., and Albert, A. Corticotrophic activity ofhuman blood. J. clin. Endocr. 1954, 14, 597.
3. Taylor, A. B., Albert, A., and Sprague, R. G.Adrenocorticotrophic activity of human blood.Endocrinology 1949, 45, 335.
4. Sydnor, K. L., Sayers, G., Brown, H., and Tyler,F. H. Preliminary studies on blood ACTH inman. J. clin. Endocr. 1953, 13, 891.
5. Sydnor, K. L., and Sayers, G. A technique for de-termination of adrenocorticotrophin in blood.Proc. Soc. exp. Biol. (N. Y.) 1952, 79, 432.
6. Gaarenstroom, J. H., Groen, A., and De Wied, D.The relation between "ACTH-content" of the bloodand the urinary excretion of 17-ketosteroids. Actaendocr. (Kbh.) 1954, 17, 89.
7. Moruzzi, G., Rossi, C. A., Montanari, L., and Mar-tinelli, M. Blood ACTH in man: "Active" and"activable" fractions. J. clin. Endocr. 1954, 14,1144.
8. Montanari, L., Martinelli, M., Rossi, C. A., andMoruzzi, G. Adrenocorticotrophic activity ofplasma. J. Amer. med. Ass. (Correspondence)1951, 147, 525.
9. Rossi, C. A., Montanari, L., Martinelli, M., andMoruzzi, G. Ultrafilterable ACTHactivity of hu-man plasma. J. Amer. med. Ass. (Correspondence)1952, 149, 1242.
10. Bornstein, J., and Trewhella, P. Adrenocorticotrophicactivity of blood-plasma extracts. Lancet 1950, 2,678.
11. Parrott, D. M. V. ACTH-like activity of plasmaextracts. J. Endocr. 1951, 7, lxxx.
12. Gray, C. H., and Parrott, D. M. V. Observationson a method of measuring adrenocorticotrophichormone in plasma. J. Endocr. 1953, 9, 236.
13. Sayers, G. Blood ACTH. J. clin. Endocr. (Edi-torial) 1955, 15, 754.
14. Renold, A. E., Jenkins, D., Forsham, P. H., andThorn, G. W. The use of intravenous ACTH: Astudy in quantitative adrenocortical stimulation.J. clin. Endocr. 1952, 12, 763.
15. Fujita, T. Determination of corticotrophin (ACTH)in human blood and urine by a modified oxycellulosemethod. J. clin. Endocr. 1957, 17, 512.
16. Nelson, D. H., and Hume, D. M. Corticosteroidsecretion in the adrenal venous blood of the hy-pophysectomized dog as an assay for ACTH.Endocrinology 1955, 57, 184.
17. Silber, R. H., Bush, R. D., and Oslapas, R. Prac-tical procedure for estimation of corticosterone orhydrocortisone. Clin. Chem. 1958, 4, 278.
18. Guillemin, R., Clayton, G. W., Smith, J. D., and Lip-scomb, H. S. Measurement of free corticosteroidsin rat plasma; physiological validation of a method.Endocrinology 1958, 63, 349.
19. Lipscomb, H., and Nelson, D. H. Measurement ofcorticosterone in rat adrenal venous plasma as abioassay for ACTH. Fed. Proc. 1959, 18, 373.
20. Munson, P. L., and Toepel, W. Detection of minuteamounts of adrenocorticotropic hormone by theeffect of adrenal venous ascorbic acid. Endocrinol-ogy 1958, 63, 785.
21. Sapirstein, L. A., and Goldman, H. Adrenal bloodflow in the albino rat. Amer. J. Physiol. 1959,196, 159.
22. Nelson, D. H., Meakin, J. W., Dealy, J. B., Jr.,Matson, D. D., Emerson, K., Jr., and Thorn, G. W.ACTH-producing tumor of the pituitary gland.New Engl. J. Med. 1958, 259, 161.
23. Nelson, D. H., Meakin, J. W., and Thorn, G. WV.ACTH-producing pituitary tumors followingadrenalectomy for Cushing's syndrome. Ann. in-tern. Med. 1960, 52, 560.
24. Nelson, D. H., and Meakin, J. W. A new clinicalentity in patients adrenalectomized for Cushing'ssyndrome (abstract). J. clin. Invest. 1959, 38,1028.
25. Bethune, J. R., Nelson, D. H., and Thorn, G. W.Plasma adrenocorticotrophic hormone in Addison'sdisease and its modification by administration ofadrenal steroids. J. clin. Invest. 1957, 36, 1701.
26. Williams, W. C., Jr., Island, D., Oldfield, R. A. A.,Jr., and Liddle, G. WV. Blood corticotropin(ACTH) levels in Cushing's disease. J. clin.Endocr. 1961, 21, 426.
27. Liddle, G. W., Estep, H. L., Kendall, J. W., Jr., Wil-liams, W. C., Jr., and Townes, A. W. Clinicalapplication of a new test of pituitary reserve.J. clin. Endocr. 1959, 19, 875.
28. Jenkins, J. S., Pothier, L., Reddy, W. J., Nelson,D. H., and Thorn, G. W. Clinical experience withselective inhibition of adrenal function. Brit. med.J. 1959, 1, 398.
29. Gold, E. M., Di Raimondo, V. C., and Forsham,P. H. Quantitation of pituitary corticotropin re-serve in man by use of an adrenocortical 11-beta-hydroxylase inhibitor (SU-4885). Metabolism1960, 9, 3.
30. Melby, J. C., De Wall, R. A., Storey, J. L., andEgdahl, R. H. The production and catabolism ofcortisol in experimental endotoxin shock. J. clin.Invest. 1957, 36, 914.
31. Farmer, T. A., Herod, J. W., Pittman, J. A., andHill, S. R. Studies on adrenal cortical and an-terior pituitary responsiveness. Proc., Forty-sec-ond Meeting, Endocrine Society, Miami Beach,Fla., June 1960, abstract 27.
32. Egdahl, R. H., Melby, J. C., and Spink, W. WV.Adrenal cortical and body temperature responsesto repeated endotoxin administration. Proc. Soc.exp. Biol. (N. Y.) 1959, 101, 369.
33. Ganong, W. F., and Gold, E. M. Changes in bloodACTHlevels following administration of SU-4885to adrenalectomized dogs (abstract). Physiologist1960, 3, 63.
28





























