-
Changes in Visual Acuity in a Population The Beaver Dam Eye
Study
Ronald Klein, MD, Barbara E. K. Klein, MD, Kristine E. Lee,
MS
Purpose: To describe the change in visual acuity over a 5-year
period in persons participating in a large population-based
study.
Methods: Best-corrected visual acuity was measured, after
refraction, with 10gMAR charts using a modification of the Early
Treatment Diabetic Retinopathy Study protocol in 3684 persons
living in Beaver Dam, Wisconsin, who ranged in age from 43 to 86
years at the time of a baseline examination from 1988 to 1990, and
at a follow-up examination from 1993 to 1995.
Results: The change in the number of letters read correctly over
the 5-year period varied from 0.4 4.9 (mean standard deviation) in
people between 43 and 54 years of age to -5.2 15.4 in people 75
years of age or older at baseline. Over the 5-year period, vision
became impaired (20/40 or worse in the better eye) in 2.9% of the
pop-ulation and severely impaired (20/200 or worse in the better
eye) in 0.3%. The visual angle doubled in 1.7% of the population,
and 2.4% had improved vision. People 75 years of age or older at
baseline were 12.5 times (95% confidence interval [CI], 8.6-18.2; P
< 0.001) more likely to have impaired vision, 9.7 times (95% CI,
5.9-16.0; P < 0.001) more likely to have doubling of the visual
angle, and 78 times more likely (95% CI, 9.9-614.1; P < 0.001)
to have severe visual impairment than people younger than 75 years
of age at baseline. People 75 years of age or older who were living
in nursing homes or group homes were 3.8 times more likely to have
impaired vision, 3.3 times more likely to have severely impaired
viSion, and 5.7 times more likely to have a doubling of the visual
angle than those not residing in a nursing home or a group
home.
Conclusion: These data provide precise population-based
estimates of incidence of visual loss over a wide spectrum of ages
and show that decreased visual acuity in people 75 years of age is
a common finding, especially in those who are in nursing homes or
group homes. Ophthalmology 1996; 1 03: 1169-1178
Originally received: November 27. 1995. Revision accepted: May
I. 1996. From the Department of Ophthalmology and Visual Sciences.
University of Wisconsin Medical School. Madison. Supported by
National Institutes of Health grant EY06594 (Drs. R Klein and BEK
Klein). Bethesda. Maryland. and. in part. by the Research to
Prevent Blindness (Dr. R Klein) Senior Scientific Investigator
Award. New York. New York. Each author states that he/she has no
proprietary interest in any aspect of this work. Reprint requests
to Ronald Klein. MD. MPH. Department ofOphthal-mology and Visual
Sciences. University of Wisconsin-Madison. 610 North Walnut St. 460
WARF. Madison. WI 53705-2397.
Recent population-based studies have provided data on the
prevalence and severity ofloss of vision in the United States. I- 3
These data show a significant increase in the prevalence of
impaired vision with increasing age, es-pecially in those 75 years
of age or older. However, esti-mates of the incidence of loss of
vision are few and are limited by the small size or the select
nature of the groups studied and by the lack of objective data.4- 7
Reliable in-cidence rates ofloss of vision have important public
health implications, including the ability to project needs for
ser-vices and costs, defining etiologic relations, and assessing
the effect of treatment. The purpose of this report is to
1169
-
Ophthalmology Volume 103, Number 8, August 1996
describe the change in visual acuity over a 5-year period in
persons participating in the Beaver Dam Eye Study, a
population-based study of older adults.
Methods
Population Methods used to identify the population and
descriptions of the population have appeared in previous
reports.38.9 In brief, a private census of the population of Beaver
Dam, Wisconsin, was performed from September 15, 1987, to May 4,
1988. Eligibility requirements for entry into the study included
living in the city or township of Beaver Dam and being 43 to 84
years of age at the time of the census. A total of 5924
individuals, both institutionalized and noninstitutionalized, were
eligible for inclusion in the study. Of these individuals, 4926
participated in the examination phase between March 1, 1988, and
Septem-ber 14, 1990. Ninety-nine percent of the population was
white. Of those who did not participate, 227 (3.8%) had died before
the examination, 99 (1.7%) had moved out of the area, 18 (0.3%)
could not be located, 276 (4.7%) permitted an interview only, and
378 (6.4%) refused to participate. Comparisons between participants
and non-participants at the time of the baseline examination have
appeared elsewhere.3
The members of the cohort who were eligible to par-ticipate at
baseline had been divided randomly into ten groups to be examined
sequentially over the course of the study. Surviving members of the
cohort were invited to participate in a 5-year follow-up
examination in the same order as at baseline examination. Of the
4926 people who participated at the baseline examination, 385
(7.8%) died before March 1, 1993, the beginning of the 5-year
follow-up examination. Of the 4541 surviving persons who had,
participated in the baseline examination, 3684 (81.1 %)
participated in the follow-up examination from March 1, 1993,
through June 14, 1995. One hundred seventy-one (3.8%) died after
the start of the follow-up but before ex-amination. Four could not
be located. Two hundred fifty-nine (5.7%) permitted an interview
only (48 of whom moved out of the area) and 423 (9.3%) refused to
partic-ipate (44 of whom moved out of the area). Both the mean and
median times between the baseline and 5-year follow-up examinations
were 4.8 years (standard deviation, 0.4 years).
Of the 3684 people examined at baseline and at follow-up, 92
were living in a nursing home or a group home at follow-up. Of
these people, 24 were in a nursing home or a group home at
baseline. One person was in a nursing home at baseline but moved
home by follow-up.
Comparisons between participants and nonparticipants at
follow-up are presented in Table 1. The 686 nonpar-ticipants who
were alive at follow-up were more likely to be older than the
participants (Table 1). After controlling for age at baseline,
these nonparticipants were.more likely at baseline to have retired
and had fewer years of education completed, a history of never
drinking alcohol, lower in-
1170
come, poorer visual acuity, a history of cardiovascular disease,
more packyears smoked, a higher serum choles-terollevel, and higher
systolic and diastolic blood pressure than persons who
participated. There were no statistically significant differences
in the presence of age-related mac-ulopathy at baseline between
participants and nonparti-cipants.
Procedures Similar procedures were used at both the baseline and
follow-up examinations. Letters from primary care phy-sicians or
from the principal investigators, if no primary care physician was
identified, were sent to those who were eligible. The letters
described the study and invited eligible people to participate.
This was followed by a call from the study coordinator, who
provided further information about the study and made an
appointment for the ex-amination. People who were not interested in
participating in the examination were asked to respond by telephone
to the questionnaire that was administered at the time of
examination.
Human experimentation committee approval was granted and
informed consent was obtained from each participant at the
beginning of the examination. The parts of the examination
pertinent to this report consisted of a standardized refraction and
measurement of the visual acuity using the Humphrey 530 refractor
(Allergan Hum-phrey, San Leandro, CA). At follow-up only, before
re-fraction, the participants first were asked to read the Early
Treatment Diabetic Retinopathy Study chart R with their current
prescription without covering either eye. The number ofletters
correctly read was recorded. At baseline and follow-up, the
refraction obtained using the refractor was placed in a trial lens
frame and the best-corrected visual acuity was remeasured following
the Early Treat-ment Diabetic Retinopathy Study protocol using
chart R and modified for a 2-m distance. 3. IO If the
best-corrected visual acuity was 20/40 or worse, an Early Treatment
Diabetic Retinopathy Study refraction was performed and the visual
acuity was measured. The interobserver vari-ation among the
examiners for obtaining the refractive error or the best-corrected
visual acuity was low and not clinically significant (data not
shown). . At both examinations, visual acuity was obtainable
and
considered reliable in both eyes in 3480 persons, in the right
eye only in 41 persons, and in the left eye only in 47 persons.
Visual acuity was obtainable and considered reliable in at least
one eye at both visits for 17 of those in a nursing home or a group
home at both visits (11 were older than 75 years of age) and 55 of
those in a nursing home or a group home at follow-up only (39 were
older than 75 years of age).
Definitions For each eye, visual acuity was recorded as the
number of letters correctly identified (range, 0 [
-
Klein et al . Changes in Visual Acuity
Table 1. Distribution of Baseline Characteristics among
Participants and Nonparticipants in Beaver Dam II
Nonparticipants
Participants Alive Dead
Crude Crude Age-adjusted Crude Age-adjusted Characteristic %
(no.) % (no.) P' % (no.) Pt
Age at baseline (yrs) 43-54 34.7 (1277) 30.5 (209) 9.4 (16)
55-64 28.8 (1063) 24.9 (171)
-
Ophthalmology Volume 103, Number 8, August 1996
20/320, 20/400, 20/500, 20/640, 20/800, hand motions, light
perception, and no light perception. Levels of im-pairment in
visual function were defined by the best-cor-rected visual acuity
in the eye, or, for a participant, in the better eye. The
definitions were no impairment (better than 20/40, 41-70 letters
correct), any visual impairment (20/40 or worse, 40 or fewer
letters correct), and severe impairment (20/200 or worse, 5 or
fewer letters correct).
Persons were at risk for vision becoming impaired if their
visual acuity was better than 20/40 in one or both eyes at
baseline. Similarly, persons were at risk for severe loss of vision
if their visual acuity was better than 20/200 in one or both eyes
at baseline. Loss of vision over the 5-year period is defined as a
doubling of the visual angle, a loss of 15 letters (e.g., a change
from baseline to follow-up from 60 to 45 letters read correctly,
corresponding to a change in visual acuity from 20/16 to 20/32).
For each person, loss of vision was defined according to these
cri-teria in the better eye. Persons with visual acuity of no light
perception at baseline were, therefore, not at risk to lose vision.
The incidence of monocular impairment was defined as visual acuity
declining from better than 20/40 visual acuity in both eyes at
baseline to 20/40 or worse in one eye only at follow-up. The
incidence of severe monocular impairment was defined as visual
acuity de-clining from better than 20/200 in both eyes at baseline
to 20/200 or worse in one eye only at follow-up. Improve-ment in
vision was defined as vision improving by 15 or more letters
(halving of the visual angle). People had im-provement in vision
ifthere were 55 letters or more (visual acuity, 20/20 or worse) in
at least one eye. Improvement was computed for visual acuity
measured in the worse eye. Age was defined as the age at the time
of the baseline examination.
Statistical Methods Comparisons of participants and
nonparticipants were done using analysis of variance and the
Cochran-Mantel-Haenszel test of independence to adjust for age
groups with continuous (i.e., blood pressure) and categorical
(i.e., visual acuity) characteristics, respectively. Student's t
test and analysis of variance were used to compare the change in
the number ofletters read between eyes and age groups,
respectively. Linear regression analyses were used to compute
estimates of age-adjusted (continuous and qua-dratic) and
sex-adjusted change. Chi-square and Cochran-Mantel-Haenszel tests
were used to compute unadjusted and age-group-adjusted comparisons
of incidence, re-spectively. Unless noted, all results were
unadjusted for any confounders. SAS was used for all analyses. I
1.12
Results
The mean age of the participants at baseline was 60.4 years, and
56.8% were women (Table 1). The mean num-ber of years of school
completed was 12, and the median income was $25,000. Other
characteristics of the partic-ipants at baseline are presented in
Table 1.
1172
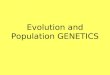
The decrease in the number of letters read correctly (mean
standard deviation) over the 5-year period was small--0.9 8.6
letters in the right eye and -1.3 8.9 letters in the left eye.
There was a significant inverse re-lation between the change in the
number of letters read correctly between examinations and
increasing age. In the right eye, the change in the number
ofletters read correctly varied from 0.4 4.9 in people 43 to 54
years of age to -5.2 15.4 in people 75 years of age or older at
baseline (Fig 1). Similar relations between age and change in the
number of letters read correctly between examinations were found in
the left eye. Age-adjusted changes in visual acuity scores (mean
standard error) over the 5-year pe-riod were slightly higher in
right eyes of men (-0.7 0.3) versus women (0.0 0.2). Regarding
changes in visual acuity in left eyes, there was no difference
between men (-0.8 0.3) and women (-0.8 0.2). After controlling for
sex, the amount of change in visual acuity score (logMAR) increased
quadratically with age. In people 55 years of age at baseline,
there was no change in visual acuity score over the 5-year period
(letters gained in right eyes, 0.3 0.2; letters lost in left eyes
0.1 0.2). In persons 65 years of age at baseline, the visual acuity
score dimin-ished by 1.0 0.2 letter in right eyes and 1.6 0.2
letters in left eyes. In persons 75 years of age at baseline, the
visual acuity score diminished by 3.5 0.3 letters in right eyes and
4.1 0.3 letters in left eyes.
The incidence of visual impairment (right eye versus left eye,
4.9% versus 5.4%; P = 0.35) or doubling of the visual angle (right
eye versus left eye, 2.8% versus 3.0%; P = 0.53) was similar for
right and left eyes. The 5-year incidence of the development of
monocular visual im-pairment (either eye) was 5.6%; for severe
monocular vi-sual impairment it was 1.0%; and for doubling of the
visual angle it was 4.1 % (Table 2). The 5-year incidence of
im-provement in vision in one eye only (either eye) (defined by an
increase of 15 or more letters read correctly at fol-low-up
compared with baseline) was 5.1%. The 5-year incidence of monocular
impairment, severe monocular visual impairment, and doubling of the
visual angle in one eye only increased with increasing age, whereas
im-provement of visual acuity in one eye only did not change
~ 0 III -1
"0 m
-2 .c E " Z .5 III
-4 Cl c III
.J:: -5 0
-6 43-54 55-64 65-74 75+
Age (years) Figure 1. Five-year change in the number of letters
read correctly in the right eye by age and sex in the Beaver Dam
Eye Study.
-
.....
..... ~
Tabl
e 2.
Five
-yea
r Inc
iden
ce o
f Mon
ocul
ar C
hang
es i
n V
isio
n by
Age
an
d Se
x in
the
Bea
ver D
am E
ye S
tudy
Dou
blin
g o
f V
isua
l A
ngle
V
isua
l Im
pair
men
t Se
vere
Im
pair
men
t Im
prov
emen
t
No. o
f Par
ticip
ants
No
. of P
artic
ipan
ts
No. o
f Par
ticip
ants
No
. of P
artic
ipan
ts
Age
(yrs)
a
t Ri
sk
(%)
Pt
at
Risk
(%
) Pt
a
t Ri
sk
(%)
Pt
at
Risk
(%
) Pt
Fe
mal
e 43
-54
650
(0.8)
626
(1.3)
648
(0.0)
153
(4.6)
55-6
4 53
7 (2.
8) 50
7 (3.
0) 53
3 (0.
6) 19
7 (4.
6) 65
-74
521
(6.0)