Embed Size (px)
Citation preview

Utility of PI based mono or bitherapy
Bonaventura Clotet MD PhDHospital Germans Trias i Pujol; Badalona
Irsicaixa Retrovirology lab & Foundation
Barcelona; Catalonia

Dr Bonaventura Clotet
• Transparency declaration
• I have served during the past 2 years as a consultant on advisory boards or participated in speakers’ bureaus or conducted clinical trials with Gilead, ViiV and Merck (MSD)

The Highest the BL VL
The longest it takes to
reach VL<50 c/ml
To maintain viral suppression
how much potency and how many
drugs are required?
3 or 2 drugs?
BL VL matters?

Antiretroviral therapy, 29 years of continuous improvement,30 drugs, 6 classes…
1981 1990 2000 2010
2008
2007
2005
2003
2001
1999
1998
1997
1996
1987
1992
1991
1983
AIDS,1st cases Didanosine
ZalcitabineZidovudine
Stavudine, Lamivudine, saquinavir, ritonavir, indinavirDelavirdine
Nevirapine, nelfinavirEfavirenz, abacavir, amprenavir
Lopinavir/r
Emtricitabine
TipranavirMaraviroc, raltegravir, darunavir
Etravirine
Tenofovir
2002
2004
Enfuvirtide, fosamprenavir, atazanavir
Rilpivirine
2012
Trizivir* Atripla* Eviplera*
NRTIsNNRTIsPIsFusion inhibitorCCR5 inhibitorIntegrase inhibitor
* STR (single tablet regimen)
1981
HIV discovery
2013
2016
ElvitegravirDolutegravir
Stribild*
Modified from F Raffi
TAF, 744-Cabotegravir
Triumeq*
2017
Long-Acting
Injectables
1920
DRV/cobi

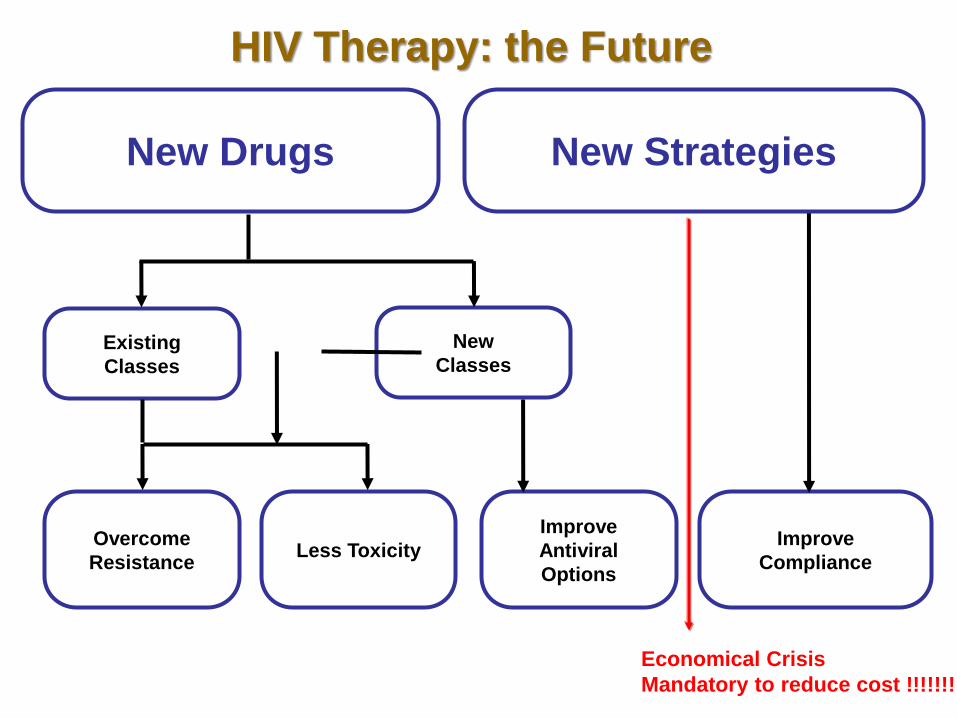
New Drugs
Less Toxicity
Improve
Antiviral
Options
Overcome
Resistance
Existing
Classes
New
Classes
Improve
Compliance
New Strategies
HIV Therapy: the Future
New Drugs
Less Toxicity
Improve
Antiviral
Options
Overcome
Resistance
Existing
Classes
New
Classes
Improve
Compliance
New Strategies
HIV Therapy: the Future
Economical Crisis
Mandatory to reduce cost !!!!!!!


1-Stopping testing CD4 if > 350
2-Use of generic compounds
3-Switch to PI monotherapy
But always maintaining
high standards of clinical care

Cost per month in Spain
Fuente: Documento de consenso de Gesida/Plan Nacional sobre el Sida respecto al tratamiento antirretroviral en adultos infectados por el virus de la inmunodeficiencia humana (Actualización enero 2013)
€

Cost per month in Spain
PI mono
€

CLINICAL
EXPERIENCE
WITH
PI BITHERAPY
Dual therapy with Lopinavir/ Ritonavir (LPV/r) and Lamivudine
(3TC) is non-inferior to standard triple drug therapy in Naïve HIV-1
infected subjects : 48-week results of the GARDEL Study.ClinicalTrials.gov : # NCT01237444
Pedro Cahn on behalf of the GARDEL study group

Objectives• To compare the efficacy and safety of a dual therapy (DT)
combination of LPV/r 400/100 mg BID+3TC 150 mg BID to a tripletherapy (TT) with LPV/r 400/100 mg BID+3TC or FTC and a thirdinvestigator-selected NRTI in fixed-dose combination in ARV-naïvepatients.
• Primary endpoint
% of patients with HIV-1 RNA< 50 copies/mL in an ITT-exposed analysis at 48 weeks (FDA-snapshot algorithm).*
• Secondary objectives
– % of patients with HIV-1 RNA< 400 copies/mL (ITT-e at 24 weeks by FDA-snapshot algorithm).
– Safety, tolerability and resistance
– Immunologic responses
* Alpha 0.05, power 80%, 2-sided 95% CI, 12% margin
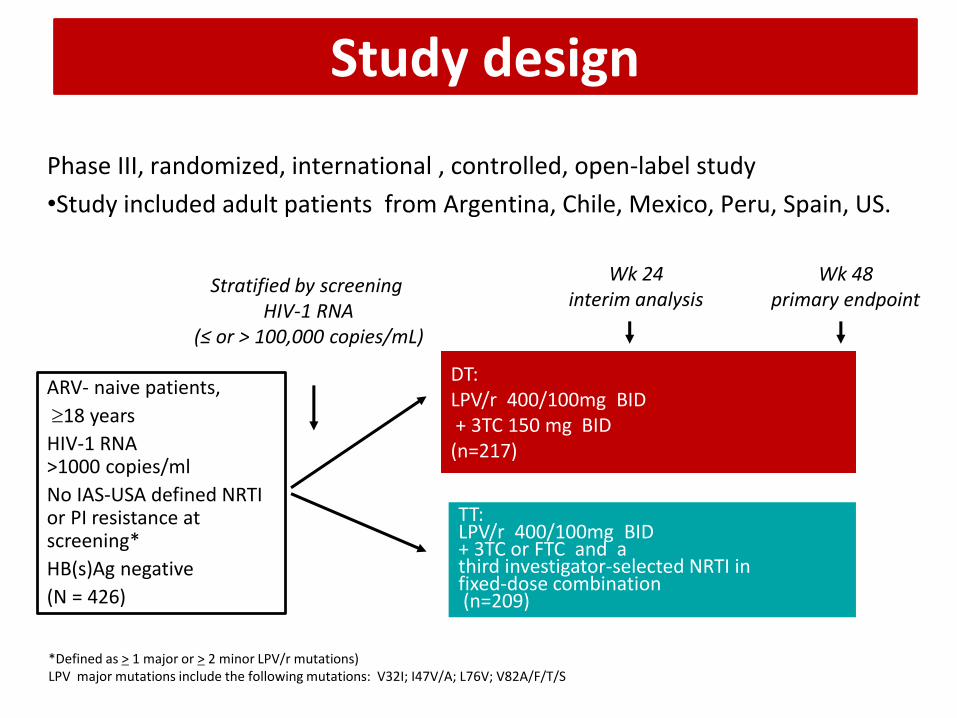
Study design
Phase III, randomized, international , controlled, open-label study
•Study included adult patients from Argentina, Chile, Mexico, Peru, Spain, US.
DT:LPV/r 400/100mg BID+ 3TC 150 mg BID(n=217)
TT:LPV/r 400/100mg BID+ 3TC or FTC and a third investigator-selected NRTI in fixed-dose combination(n=209)
ARV- naive patients,
18 years
HIV-1 RNA >1000 copies/ml
No IAS-USA defined NRTI or PI resistance at screening*
HB(s)Ag negative
(N = 426)
Stratified by screening HIV-1 RNA
(≤ or > 100,000 copies/mL)
Wk 48 primary endpoint
*Defined as > 1 major or > 2 minor LPV/r mutations) LPV major mutations include the following mutations: V32I; I47V/A; L76V; V82A/F/T/S
Wk 24 interim analysis

Patient Disposition at Week 48543 SCREENED
426 RANDOMIZED
(10 not exposed)
Completed W 48
198 (92.5%)
Completed W 48
175 (85.7%)
Discontinued
16 (7.5%)
Discontinued
27 (14.3%)
Dual therapy (DT) 214
Triple therapy (TT) 202
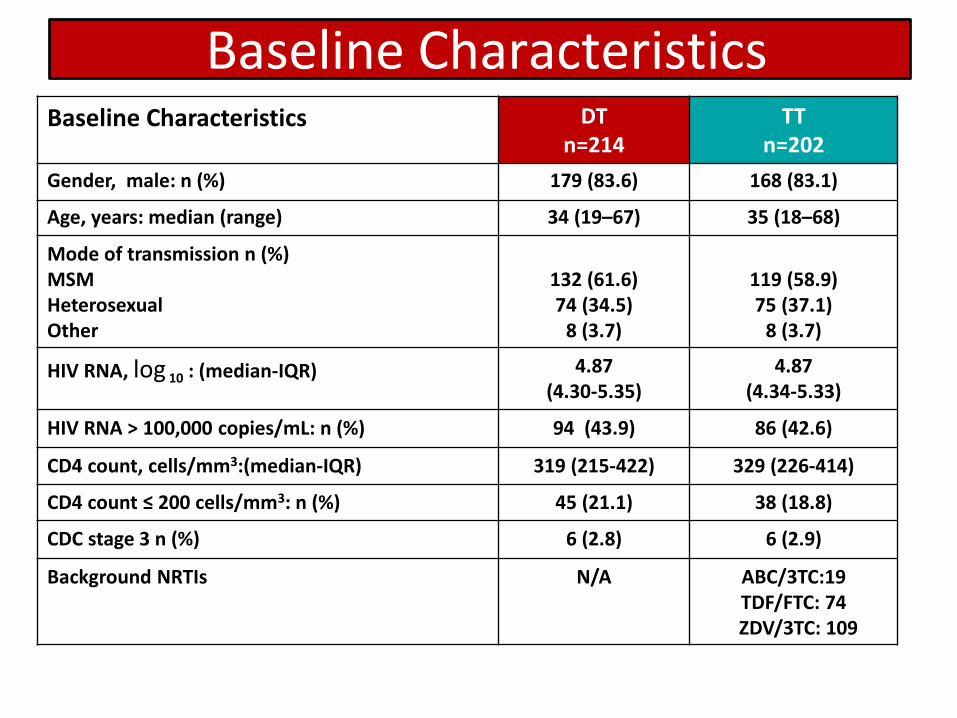
Baseline CharacteristicsBaseline Characteristics DT
n=214TT
n=202
Gender, male: n (%) 179 (83.6) 168 (83.1)
Age, years: median (range) 34 (19–67) 35 (18–68)
Mode of transmission n (%)MSMHeterosexualOther
132 (61.6)74 (34.5)
8 (3.7)
119 (58.9)75 (37.1)
8 (3.7)
HIV RNA, log 10 : (median-IQR) 4.87 (4.30-5.35)
4.87(4.34-5.33)
HIV RNA > 100,000 copies/mL: n (%) 94 (43.9) 86 (42.6)
CD4 count, cells/mm3:(median-IQR) 319 (215-422) 329 (226-414)
CD4 count ≤ 200 cells/mm3: n (%) 45 (21.1) 38 (18.8)
CDC stage 3 n (%) 6 (2.8) 6 (2.9)
Background NRTIs N/A ABC/3TC:19TDF/FTC: 74ZDV/3TC: 109

Viral load <400 copies/mL at week 24 and 48 (ITTe)
91,6%85,6%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BSL W4 W8 W12 W24 W36 W48
DT TT
(p= 0.078, difference +5,9%[CI95%:-0,6% to +12,5%])
93.5%
90.6%

Viral load <50 copies/mL at week 48 (ITTe)
(p= 0.171, difference +4.6% [CI95%:-2.2% to +11.8%])

Viral load <50 copies/mL at week 48 (ITTe), baseline VL
> 100.000 copies/mL
(p= 0.145, difference +9.3% [CI95%:-2.8% to +21.5%])
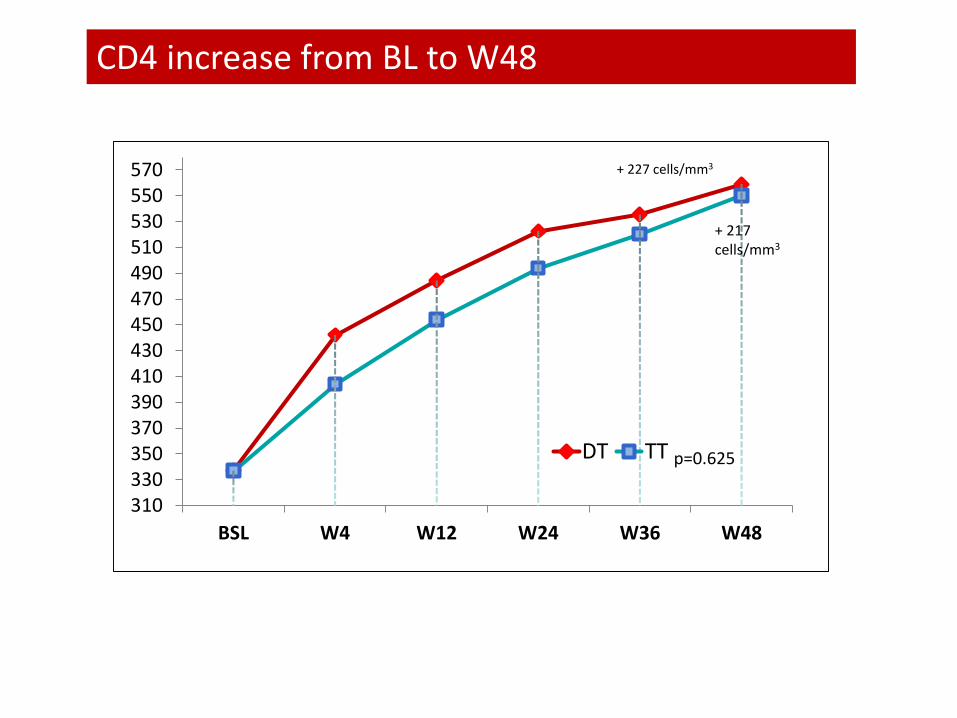
CD4 increase from BL to W48
310330350370390410430450470490510530550570
BSL W4 W12 W24 W36 W48
DT TT
+ 227 cells/mm3
+ 217 cells/mm3
p=0.625

DT (n=214)
TT(n=202)
P[IC95%]
HIV – RNA < 50 copies/mL (n; %)
189 (88.3%) 169 (83.7%) 0.171[-2.2% ; +11.8%]
HIV – RNA >50 copies/mL (n; %)
10 (4.7%) 12 (5.9%)0.720
[-6.1%; +3.5%]
No Virologic data at week 48 windowReasons:Discontinued study due to adverse event or death
2 (0.9 %)* 10 (4.9 %)**0.03
[-7.8%; -3.0%]
Discontinued study for other reasons***
13 (6.1%) 11 (5.4%)0.948
[-4.3; +5.6]
Virologic Outcome at W48
*** (Non compliance with study procedures, consent withdrawal, adherence, opportunistic infection, lost to follow-up, pregnancy)
* 1 death: Sepsis, 1 nephrotic syndrome ** 2 Rash, 3 anemia, 5 GI intolerance

A DT (N=214)
TT(N=202)
# pts with selected treatment-emergent Grade 3-4 laboratory abnormalities, n (%)
Hemoglobin 2 (0.9%) 2 (1.0%)
WBC 0 0
Platelet count 4 (1.9%) 3 (1.5%)
SGPT/ALT 0 0SGOT/AST 1 (0.5%) 0Creatinine 0 0Glucose 0 3(1.5%)
Total Cholesterol 18 (8.4%) 14 (6.9%)
Triglycerides 8 (3.7%) 17 (8.4%)
LDL-cholesterol 21 (9.8%) 13 (6.4%)
Selected Laboratory Abnormalities
p= NS in all laboratory abnormalities shown
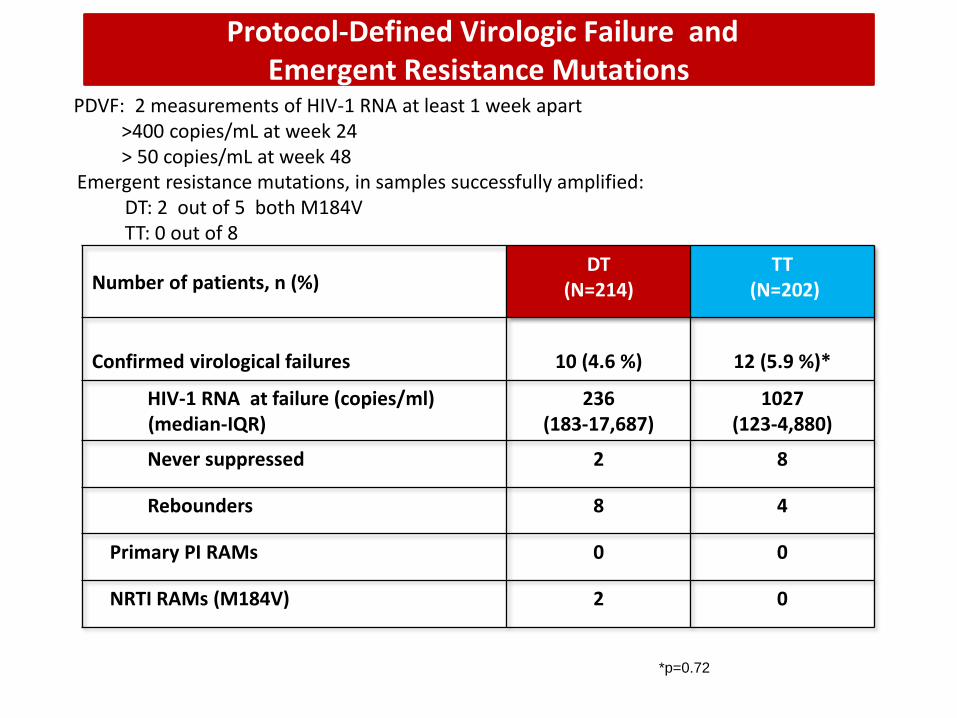
Protocol-Defined Virologic Failure and Emergent Resistance Mutations
Number of patients, n (%)DT
(N=214)TT
(N=202)
Confirmed virological failures 10 (4.6 %) 12 (5.9 %)*
HIV-1 RNA at failure (copies/ml)(median-IQR)
236(183-17,687)
1027(123-4,880)
Never suppressed 2 8
Rebounders 8 4
Primary PI RAMs 0 0
NRTI RAMs (M184V) 2 0
*p=0.72
PDVF: 2 measurements of HIV-1 RNA at least 1 week apart>400 copies/mL at week 24 > 50 copies/mL at week 48
Emergent resistance mutations, in samples successfully amplified:DT: 2 out of 5 both M184V TT: 0 out of 8
• Our results demonstrate that DT with LPV/r+3TC was non-inferior to triple therapy after 48 weeks of treatment, regardless of baseline viral load.
• The DT regimen showed fewer discontinuations due to safety and tolerability .
• Virologic failure, occurring at similarly low levels in both treatment arms, did not result in PI resistance development, preserving a wide range of drugs for 2nd line ARV therapy.
• These results suggest that a dual LPV/r+3TC regimen warrants further clinical research and consideration as a potential therapeutic option for ARV naïve subjects.
GARDEL: conclusions

Poster Number
LBPE17
JM Gatell1, JR Arribas2, PM Girard3, R Landman4, J Pich1, J Mallolas1, M Martínez1, FX Zamora2,V Estrada5, M Crespo6, D Podzamczer7, J Portilla8, F Dronda9, JA Iribarren10, P Domingo11, FPulido12, M Montero13, H Knobel14, A Cabié15, L Weiss16 on behalf of the OLE Study Group
1Hospital Clínic, Barcelona, Spain 2Hospital La Paz, Madrid, Spain 3Hospital St Antoine, Paris, France 4Hospital Bichat Claude Bernard,Paris, France 5Hospital Clínico San Carlos, Madrid, Spain 6Hospital Vall d’Hebrón, Barcelona, Spain 7Hospital Universitrario deBellvitge, Barcelona, Spain 8Hospital General Universitario de Alicante, Alicante, Spain 9Hospital Universitario Ramón y Cajal,Madrid, Spain 10Hospital de Donostia, Donostia, Spain 11Hospital de Sant Pau, Barcelona, Spain 12Hospital Doce de Octubre, Madrid,Spain 13Hospital La Fe, Valencia, Spain 14Hospital del Mar, Barcelona, Spain 15Hospital La Meynard, Martinique, France 16HospitalEuropeen Georges-Pompidou, Paris, France
OLE= Only Lopinavir and Epivir
Non-inferiority of Dual-Therapy (DT) withLopinavir/ritonavir (LPV/r) plus Lamivudine (3TC) vs.Triple-Therapy (TT) with LPV/r plus TwoNucleos(t)ides (NRTIs) for Maintenance of HIV-1 ViralSuppression: 48-Week Results of the OLE Study

Secondary endpoint
Difference (95% CI)
0.05% (-5.3% to + 5.1%)
Difference (95% CI)
0.3% (- 8.5 to + 8.3%)
Difference (95% CI)
-0.25% (- 8.2 to + 7.6%)
Protocol defined VF: 2 consecutive VL>= 50 copies/ml; VF or any blip: any detectable VL >= 50 copies/ml
97.3% 97.3%
87.3% 87.6%89.8% 90.1%
Protocol defined VF Any blip Protocol defined
VF or any blip

27
LPV/r + RAL vs. LPV/r + TDF/FTC in NAIVE PROGRESS STUDY
Met Primary Endpoint of Noninferiority • Primary endpoint: plasma HIV-1 RNA <40 copies/mL at week 48 (FDA-TLOVR)
• FDA-TLOVR week 48: LPV/r + RAL=83.2%, LPV/r + TDF/FTC=84.8%
• P=0.850, difference -1.6%, 95% exact confidence interval (CI) -12.0%, 8.8%
• Safety and tolerability were similar at week 48
LPV/r 400/100 mg BID
+ TDF/FTC 300/200 mg QD
(n=105)
Inclusion Criteria for PROGRESS (M10-336)• HIV-1 infection
• ARV-naïve
• Plasma HIV-1 RNA >1000 copies/mL
• Any CD4+ T-cell count
ScreeningWeek 96
LPV/r 400/100 mg BID
+ RAL 400 mg BID
(n=101)Week 48
Primary
Efficacy
Endpoint
* 3 subjects were randomized but not dosed
PROGRESS 96 Week Results
April 9, 2011

28PROGRESS 96 Week Results
April 9, 2011
LPV/r + RAL vs. LPV/r + TDF/FTC in NAIVE PROGRESS STUDY

29
Number and % of Subjects with Moderate or Severe Drug-Related Adverse Events*
* Occurring in ≥2.0% in either treatment group
† Hypercholesterolaemia includes blood cholesterol increased, hypertriglyceridaemia includes blood triglycerides increased
P>0.05 for LPV/r + RAL vs. LPV/r + TDF/FTC comparison for each adverse event based on Fisher's exact test
LPV/r + RAL
(N=101)
n (%)
LPV/r + TDF/FTC
(N=105)
n (%)
Any adverse event 31 (30.7) 36 (34.3)
Diarrhea 8 (7.9) 17 (16.2)
Hypercholesterolaemia† 10 (9.9) 7 (6.7)
Hypertriglyceridaemia† 9 (8.9) 5 (4.8)
Alanine Aminotransferase Increased 3 (3.0) 1 (1.0)
Hyperlipidaemia 3 (3.0) 1 (1.0)
Asthenia 0 (0) 3 (2.9)
Regurgitation 0 (0) 3 (2.9)
PROGRESS 96 Week Results
April 9, 2011

30
Proportion of Subjects with ≥5% Decrease
from Baseline in Total Bone Mineral Density

CLINICAL
EXPERIENCE
WITH
PI MONOTHERAPY

LPV/r monotherapy: Better if latter....
1. Delfraissy JF, et al. AIDS 2008;22:385–93; 2. Cameron DW, et al. J Infect Dis 2008;198:234–40;
3. Arribas J, et al. J Acquir Immune Defic Syndr 2005;40:280–7
Discontinued
On study, HIV-1 RNA >400
On study, HIV-1 RNA 50–400
On study, HIV-1 RNA <50
.
MONARK1
Initial therapy
M03-6132
Induction/Maintenance
0
20
40
60
80
100
0 16 32
Wk
48 0 16 32 48 64 80 96
Wk Wk
36 4812
OK043
Simplification
0 24
Patients
(%
)
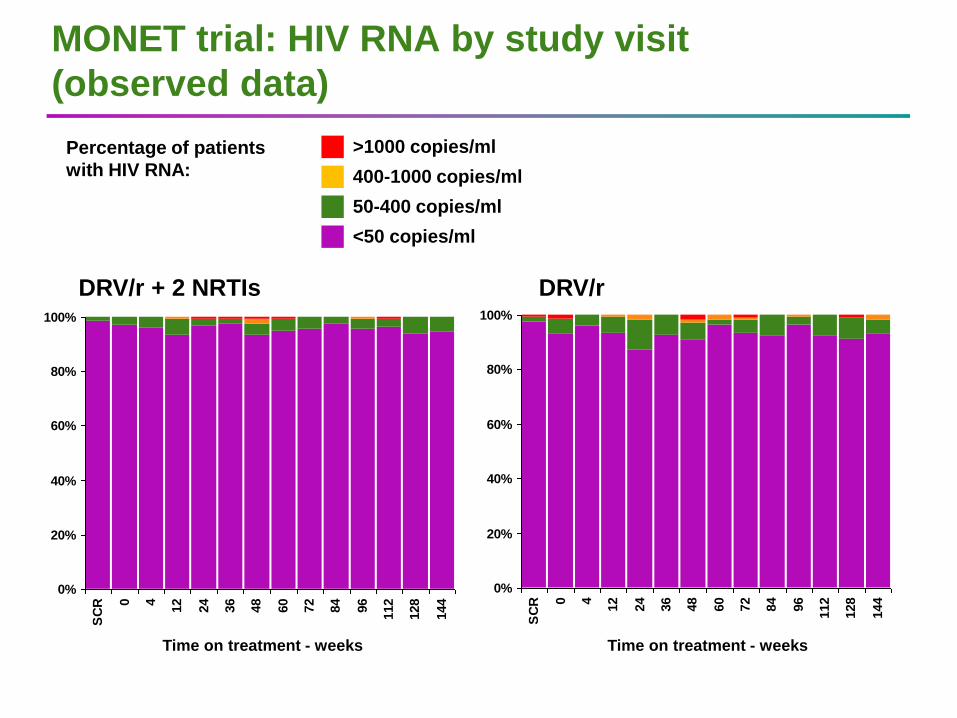
MONET trial: HIV RNA by study visit
(observed data)
>1000 copies/ml
400-1000 copies/ml
50-400 copies/ml
<50 copies/ml
DRV/r + 2 NRTIs DRV/r
0%
20%
40%
60%
80%
100%
SC
R 0 4
12
24
36
48
60
72
84
96
112
128
144
0%
20%
40%
60%
80%
100%
SC
R 0 4
12
24
36
48
60
72
84
96
112
128
144
Time on treatment - weeks Time on treatment - weeks
Percentage of patients
with HIV RNA:

PATIENTS ON
PI MONOTHERAPY
WITH LPV/r FOR
AT LEAST 10 years

2 0 0 5 2 0 1 0 2 0 1 5
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
6 0 0
7 0 0
8 0 0
5 0
5 ,0 5 0
1 0 ,0 5 0
CD
4 c
ell
co
un
tV
L (c
op
ies
/mL
)
LPV + FTC /TDF
L P V /r
Vicente
2 0 0 4 2 0 0 6 2 0 0 8 2 0 1 0 2 0 1 2 2 0 1 4 2 0 1 6
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
6 0 0
7 0 0
0
5 0 ,0 0 0
1 0 0 ,0 0 0
1 5 0 ,0 0 0
2 0 0 ,0 0 0C
D4
ce
ll c
ou
nt
VL
(c
op
ies
/mL
)
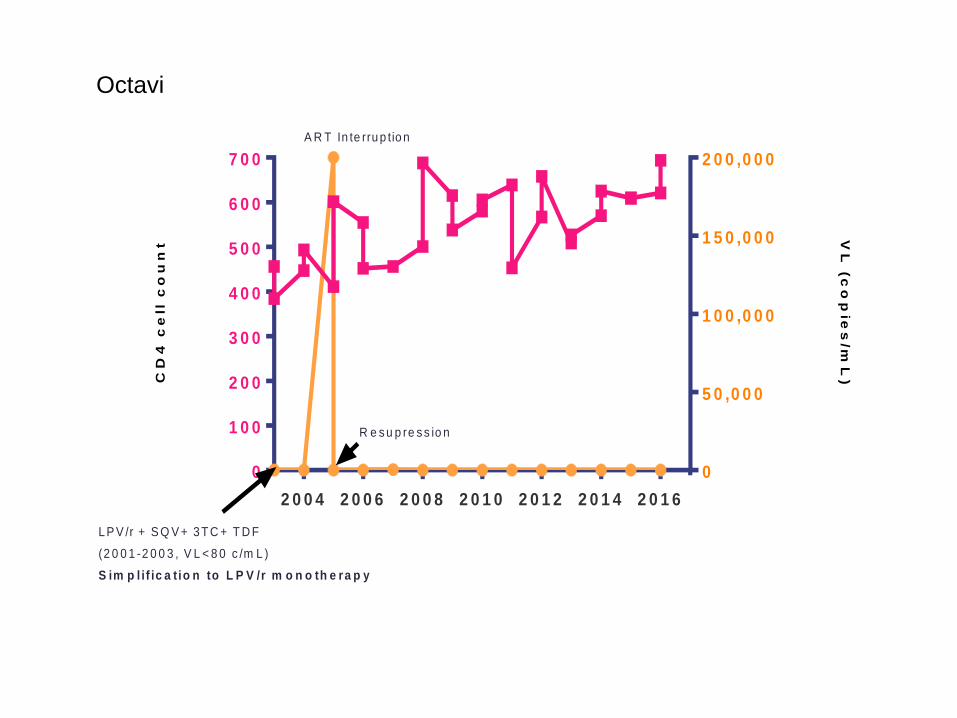
L P V /r + S Q V + 3 T C + T D F
(2 0 0 1 -2 0 0 3 , V L < 8 0 c /m L )
S im p l if ic a t io n to L P V /r m o n o th e ra p y
A R T In te rru p tio n
R e s u p re s s io n
Octavi
2 0 0 4 2 0 0 6 2 0 0 8 2 0 1 0 2 0 1 2 2 0 1 4 2 0 1 6
5 0 0
6 0 0
7 0 0
8 0 0
9 0 0
1 ,0 0 0
1 ,1 0 0
1 ,2 0 0
1 ,3 0 0
1 ,4 0 0
1 ,5 0 0
1 ,6 0 0
1 ,7 0 0
1 ,8 0 0
1 ,9 0 0
5 0
5 5 0
1 ,0 5 0
1 ,5 5 0
2 ,0 5 0
2 ,5 5 0
CD
4 c
ell
co
un
t
VL
(co
pie
s/m
L)
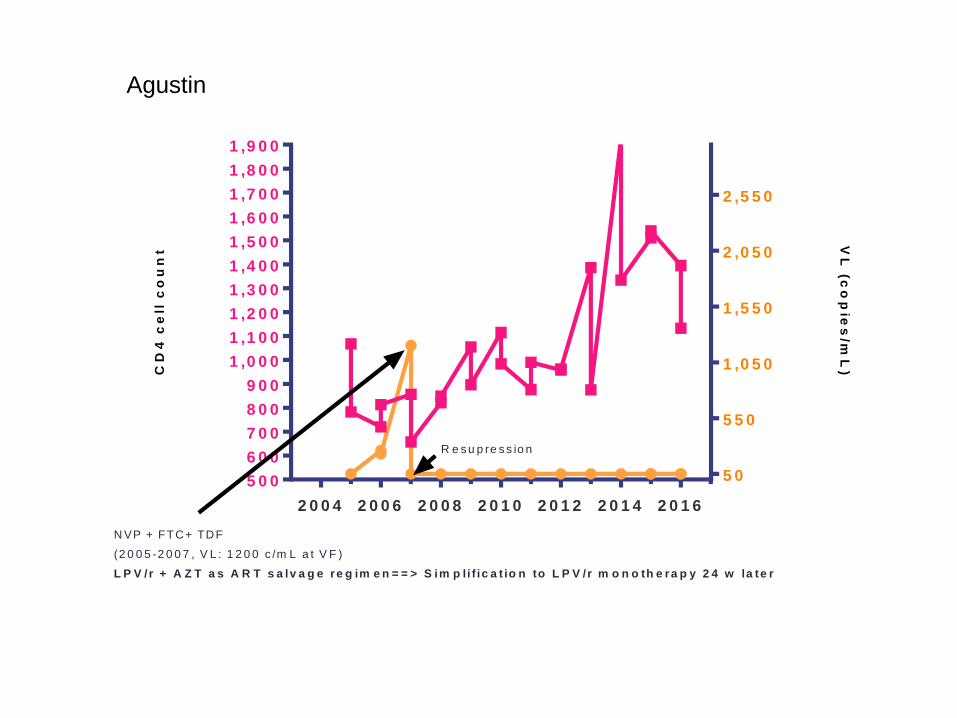
N VP + FTC+ TDF
(2 0 0 5 -2 0 0 7 , V L : 1 2 0 0 c /m L a t V F )
L P V /r + A Z T a s A R T s a lv a g e re g im e n = = > S im p li f ic a t io n to L P V /r m o n o th e ra p y 2 4 w la te r
R e s u p re s s io n
Agustin

2 0 0 2 2 0 0 4 2 0 0 6 2 0 0 8 2 0 1 0 2 0 1 2 2 0 1 4 2 0 1 6
4 0 0
5 0 0
6 0 0
7 0 0
8 0 0
9 0 0
1 ,0 0 0
1 ,1 0 0
1 ,2 0 0
1 ,3 0 0
1 ,4 0 0
1 ,5 0 0
5 0
1 ,0 5 0
2 ,0 5 0
3 ,0 5 0
CD
4 c
ell
co
un
t
VL
(co
pie
s/m
L)
N VP + dd I+ TDF
(2 0 0 1 -2 0 0 2 , V L : 3 9 0 0 c /m L a t V F )
L P V /r + 3 T C + T D F a s s a lv a g e re g im e n (2 0 0 2 )
R e s u p re s s io n
S im p lif ica tio n to L P V /r m o n o th e ra p y
Encarna