Embed Size (px)
Citation preview
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
Barbara F. Brandt, PhD Director, National Center for Interprofessional Practice and EducationAssociate Vice President for Education, Academic Health Center University of Minnesota Academic Health Center
Susan M. Meyer, PhDChair, National Center Nexus Learning System Advisory CommitteeCo-director, University of Pittsburgh Center for Interprofessional Practice and EducationAssociate Dean for Education and Professor, University of Pittsburgh School of Pharmacy
June 9, 2017 University of Texas - Houston
UTHealth Advances in Teaching and Learning Day
Welcome and Introductions
Barbara F. Brandt, PhD Director, National Center for Interprofessional Practice and EducationAssociate Vice President for Education, Academic Health Center University of Minnesota Academic Health Center
Susan M. Meyer, PhDChair, National Center Nexus Learning System Advisory CommitteeCo-director, University of Pittsburgh Center for Interprofessional Practice and EducationAssociate Dean for Education and Professor, University of Pittsburgh School of Pharmacy
2
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
Barbara F. Brandt, PhD Director, National Center for Interprofessional Practice and Education
June 9, 2017 University of Texas - Houston
The State of Interprofessional Practice and Education in Turbulent Times!
Topics
• Minding the gap of the current turbulent IPE environment
• How the National Center is working for you
• New Models of Care Require New Models of Learning: Tools you can use
4
Learning Partner Acknowledgement
Many thanks to all of our advisors, program participants, Nexus Innovations Network, funders, and many stakeholders from whom we learn every day.
Special thanks: National Advisory CouncilNexus Learning System Advisory Committee American Interprofessional Health CollaborativeAngela Willson, National Center Education & Training Manager“Conversation Café” Champions
5
Interprofessional Education and Collaborative PracticeThe “New IPE” – Interprofessional Practice and Education
6
Interprofessional education “occurs when two or moreprofessions learn with, about, and from each other toenable effective collaboration and improve healthoutcomes.”
Interprofessional, collaborative practice “occurs whenmultiple health workers and students and residents fromdifferent professional backgrounds provide comprehensivehealth services by working with patients, their families,carers (caregivers), and communities to deliver the highestquality of care across settings.”Adapted from:The Centre for the Advancement of Interprofessional Education, UK, 1987World Health Organization, Framework for Action on Interprofessional Education and Collaborative Practice, 2010.
What We Value:National Center Vision
7
We believe high-functioning teams can improve theexperience, outcomes and costs of health care.
National Center for Interprofessional Practice andEducation is studying and advancing the waystakeholders in health work and learn together.
National Center FundersHealth Resources and Services Administration CooperativeAgreement
Award No. UE5HP25067Robert Wood Johnson Foundation
Gordon and Betty Moore FoundationJosiah Macy Jr. Foundation
John A. Hartford Foundation
What We Value:National Center Vision
8
We believe high-functioning teams can improve theexperience, outcomes and costs of health care.
National Center for Interprofessional Practice andEducation is studying and advancing the waystakeholders in health work and learn together.
National Center FundersHealth Resources and Services Administration CooperativeAgreement
Award No. UE5HP25067Robert Wood Johnson Foundation
Gordon and Betty Moore FoundationJosiah Macy Jr. Foundation
John A. Hartford Foundation
The Nexus: Our Vision for Healthnexusipe.org
9
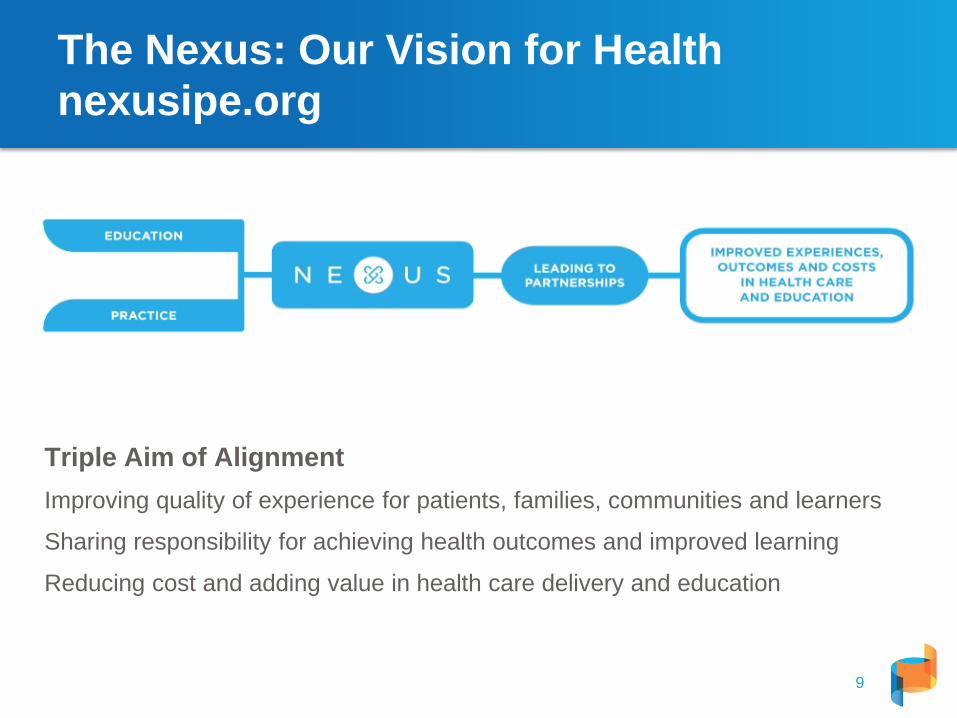
Triple Aim of AlignmentImproving quality of experience for patients, families, communities and learners
Sharing responsibility for achieving health outcomes and improved learning
Reducing cost and adding value in health care delivery and education
HRSA PrinciplesJune 1, 2012 Funding Opportunity Announcement
A coordinating center for interprofessionaleducation and collaborative practice will provide
leadership, scholarship, evidence, coordination, and national visibility to advance interprofessional education and
practice as a viable and efficient health care delivery model. (p.4)
“Unbiased, neutral convener”
10
11
The Nexus Focus
11
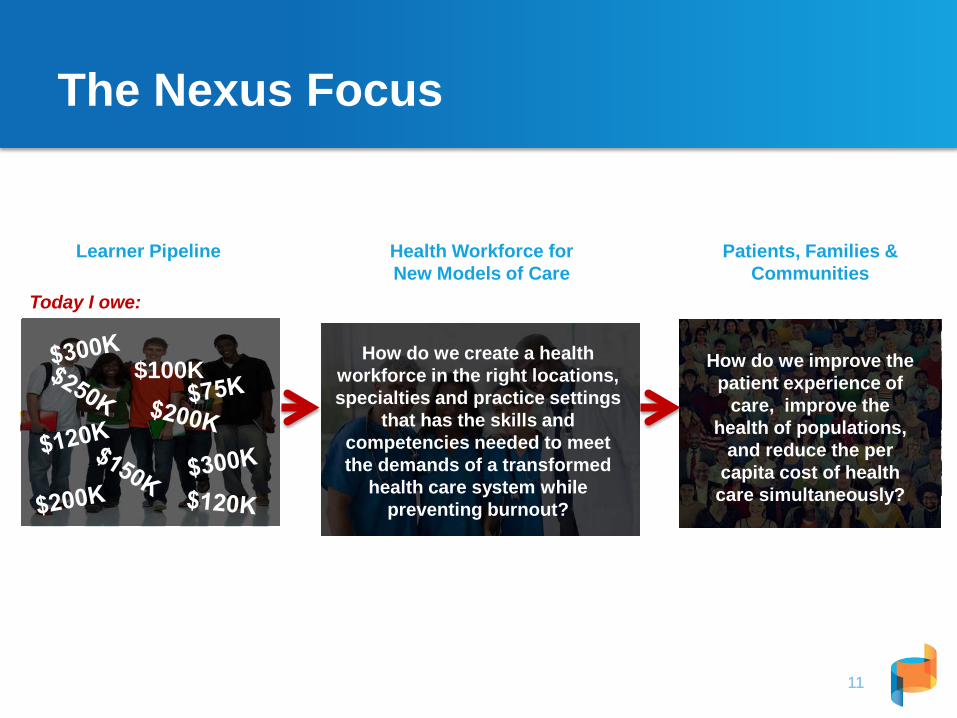
How do we improve the patient experience of
care, improve the health of populations,
and reduce the per capita cost of health care simultaneously?
Patients, Families & Communities
Health Workforce for New Models of Care
Learner Pipeline
How do we create a health workforce in the right locations, specialties and practice settings
that has the skills and competencies needed to meet the demands of a transformed
health care system while preventing burnout?
Today I owe:
How do we prepare the next generation of health
professionals for a transformed health care system while improving
experience and decreasing costs?
How do we prepare the next generation of health
professionals for a transformed health care system while improving
experience and decreasing costs?
$100K
Unbiased, Neutral Convener:“Calling the circle”
– Convenes groups and tees up “thorny IPE issues” topics for discussion and recommendations
– Works inter- and intra-professionally to promote dialogue and understanding
– Cannot favor one profession over the other– Cannot advocate for one model over the other– Collects data and information to make sense while
striving to be objective
12
Unbiased, Neutral Convener:“Calling the circle”
– Advances thinking about the field based upon evidence, experience and expertise
– Based upon evolving models of IPE, identifies partners to educate and train in specialized areas
– Advocates for our values, based upon what we are learning makes a difference
– Says what needs to be said. . .
13
A National Birdseye View: Themes and ObservationsSelect Presentations, Consultations, Partnerships and Contracts for Services
14
• 1199/SEIU Training Funds• 3M• Accreditation Council of Graduate Medical Education• American Assembly for Men in Nursing• American Interprofessional Health Collaborative• AMA – Accelerating Change in Medical Education• Association of Nurse Professional Development• American Association of Colleges of Nursing• American Association of College of Pharmacy• American Board of Medical Specialties• American Interprofessional Health Collaborative• American Medical Association• Association of Academic Health Centers• Association of Nursing Professional Development• Association of Schools and Programs of Public Health• American Physical Therapy Association • Association of Specialized and Professional Accreditors• Beyond Flexner Alliance• California Institute for Nursing and Health Care• Centers for Medicare and Medicaid Services • Council on Social Work Education• HRSA Nurse Education, Practice, Quality and Research
grantees• Indiana Center for Nursing• Joint Accreditors of Interprofessional Continuing Education• Josiah Macy Jr. Foundation• Institute for Healthcare Improvement (IHI)• Interprofessional Education Collaborative (IPEC)
• IOM Future of Nursing • IOM/NAM Global Forum on Innovations in Health Professions
Education• Macy T3 Faculty Development Program• National Advisory Council on Nurse Education and Practice • National Association of Community Health Centers• National Governors Association• National Health Policy Forum• National League of Nursing• National Nurse-lead Centers Consortium• National Quality Forum• Nursing Organizations Alliance• OptumHealth• Patient-Centered Primary Care Collaborative• Respiratory Nurses Society• University of North Carolina Cecil G. Shep Center• University of North Texas Health Sciences Center• University of Texas-Houston• VA Centers of Excellence in Primary Care• World Health Organization / Pan American Health
Organization• And more . . . . .
• Many team site visits -- scores of universities and practices• Many calls, emails. . . .
Satellite and Big Blue Marble
15
View from the Satellite:Interconnection of Organizations
16
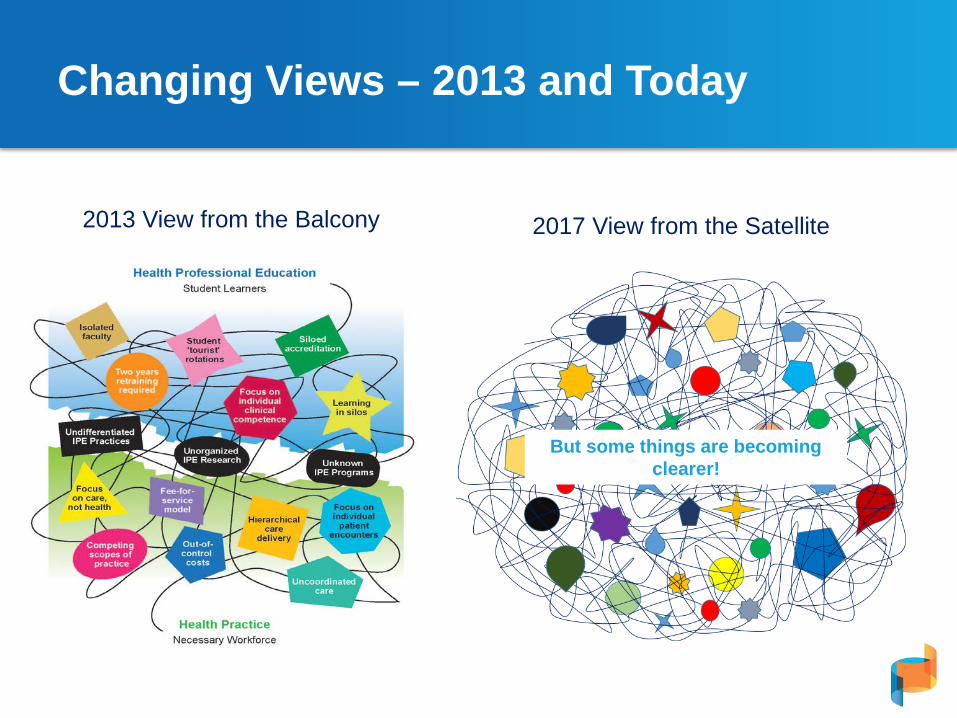
Changing Views – 2013 and Today
2013 View from the Balcony 2017 View from the Satellite
But some things are becoming clearer!
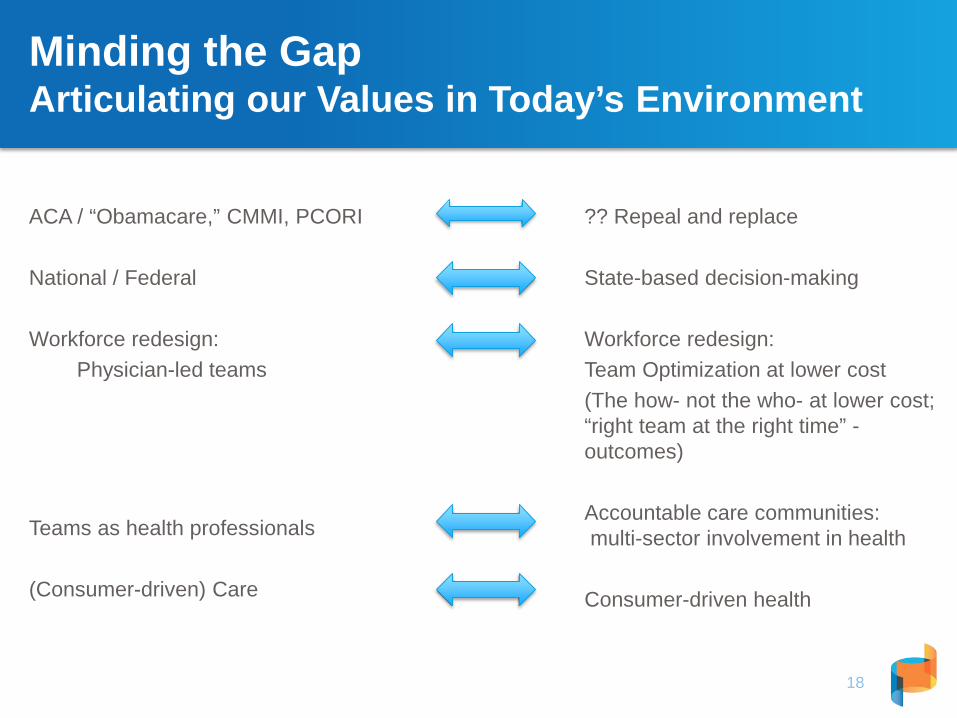
ACA / “Obamacare,” CMMI, PCORI
National / Federal
Workforce redesign:Physician-led teams
Teams as health professionals
(Consumer-driven) Care
?? Repeal and replace
State-based decision-making
Workforce redesign:Team Optimization at lower cost (The how- not the who- at lower cost; “right team at the right time” -outcomes)
Accountable care communities: multi-sector involvement in health
Consumer-driven health
Minding the GapArticulating our Values in Today’s Environment
18
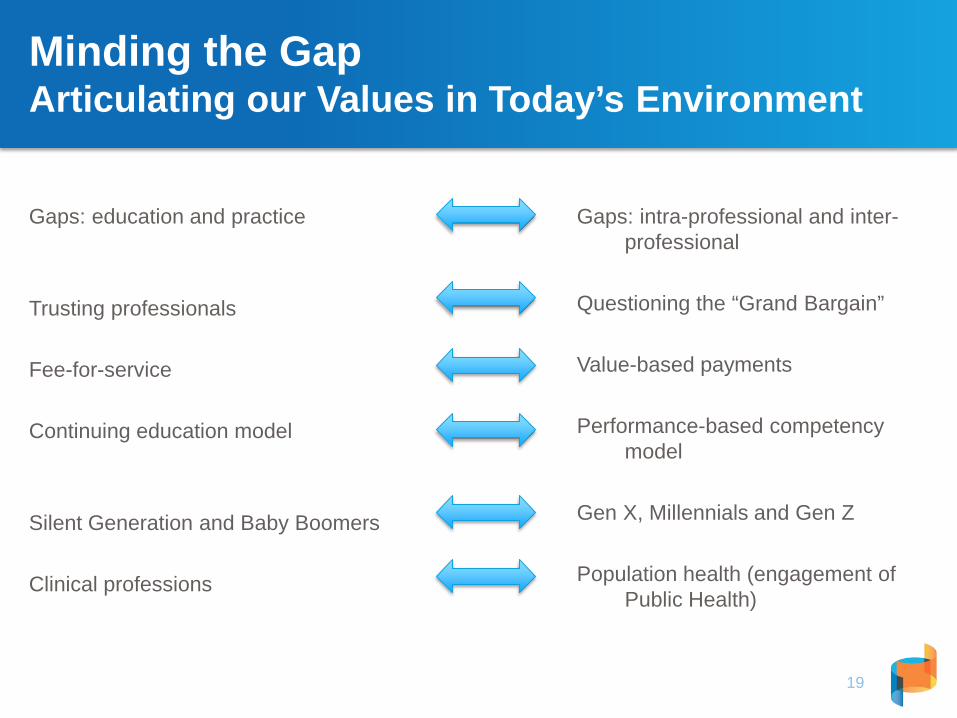
Minding the GapArticulating our Values in Today’s Environment
Gaps: education and practice
Trusting professionals
Fee-for-service
Continuing education model
Silent Generation and Baby Boomers
Clinical professions
Gaps: intra-professional and inter-professional
Questioning the “Grand Bargain”
Value-based payments
Performance-based competency model
Gen X, Millennials and Gen Z
Population health (engagement of Public Health)
19
“True North”: What Does it Mean?
• Commitment to interprofessional teams
• Value-based payment models
• “Consumer-driven” health care
20
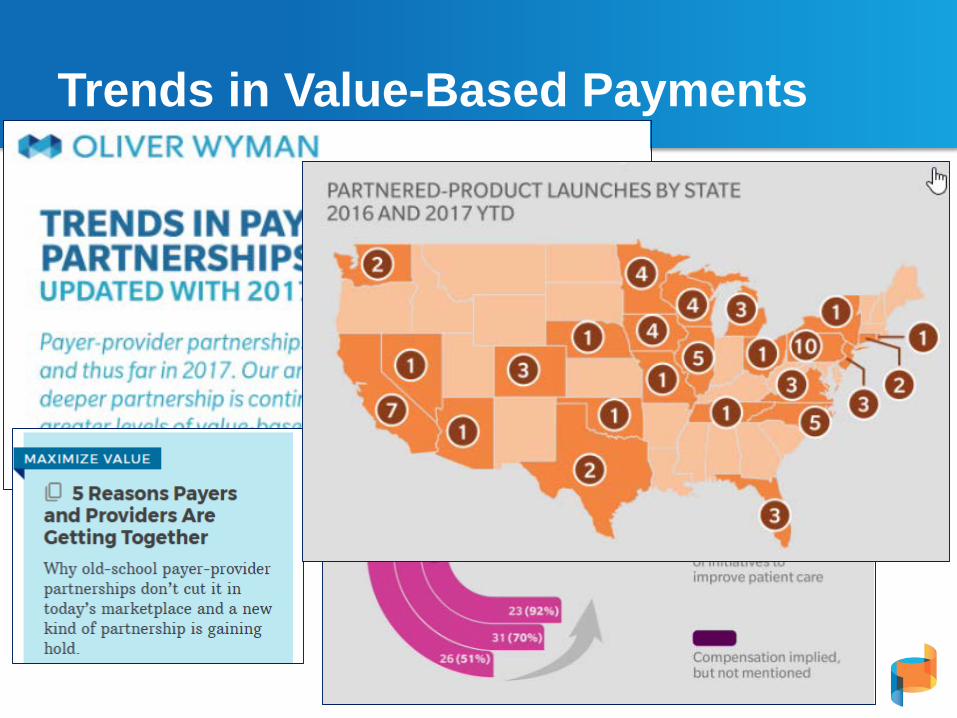
Trends in Value-Based Payments
21
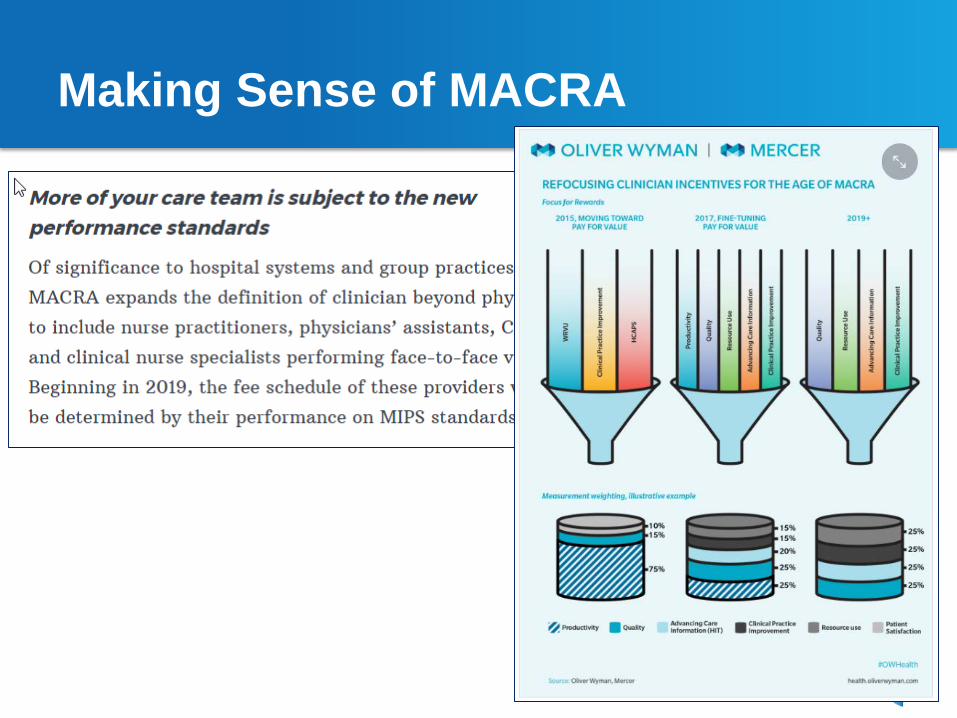
Making Sense of MACRA
22
The National Center: What’s in it for you?
23
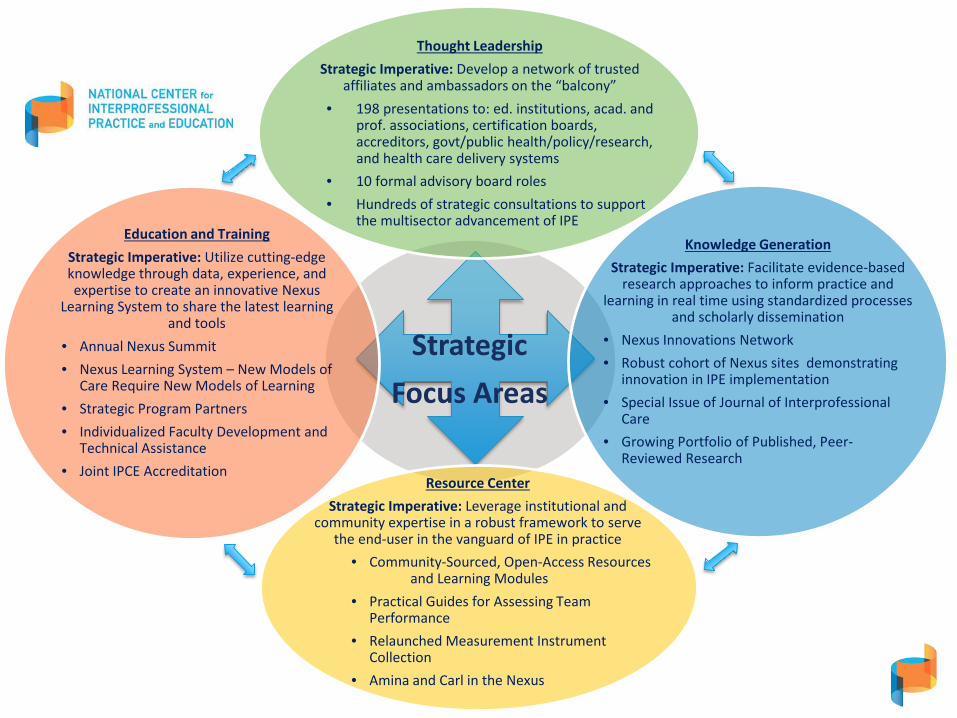
Strategic Focus Areas
Thought LeadershipStrategic Imperative: Develop a network of trusted
affiliates and ambassadors on the “balcony”• 198 presentations to: ed. institutions, acad. and
prof. associations, certification boards, accreditors, govt/public health/policy/research, and health care delivery systems
• 10 formal advisory board roles• Hundreds of strategic consultations to support
the multisector advancement of IPEKnowledge Generation
Strategic Imperative: Facilitate evidence-based research approaches to inform practice and
learning in real time using standardized processes and scholarly dissemination
• Nexus Innovations Network• Robust cohort of Nexus sites demonstrating
innovation in IPE implementation• Special Issue of Journal of Interprofessional
Care• Growing Portfolio of Published, Peer-
Reviewed Research
Resource CenterStrategic Imperative: Leverage institutional and
community expertise in a robust framework to serve the end-user in the vanguard of IPE in practice
• Community-Sourced, Open-Access Resources and Learning Modules
• Practical Guides for Assessing Team Performance
• Relaunched Measurement Instrument Collection
• Amina and Carl in the Nexus
Education and TrainingStrategic Imperative: Utilize cutting-edge knowledge through data, experience, and expertise to create an innovative Nexus
Learning System to share the latest learning and tools
• Annual Nexus Summit• Nexus Learning System – New Models of
Care Require New Models of Learning• Strategic Program Partners• Individualized Faculty Development and
Technical Assistance• Joint IPCE Accreditation
Thought Leadership
25

Expertise-formal and informal
advisory roles - leadership consults to
guide planning, investments
- customized resources to meet specific needs
Convener-facilitate “thorny IPE” dialogue
through unbiased lens- bring together diverse
perspectives to advance thinking- challenge traditional approaches
- invite innovation
Outreach-using findings in all
areas- facilitating learning and Nexus dialogue
-presenting at workshops, conferences
-utilizing affiliates to extend reach
26
Education and TrainingStrategic Imperative: Utilize
cutting-edge knowledge through data, experience, and expertise to
create an innovative Nexus Learning System to share the latest
learning and tools
Resource CenterStrategic Imperative: Leverage
institutional and community expertise in a robust framework to serve the end-user in the vanguard of IPE in
practice
Strategic Imperative: Develop a network of trusted affiliates and ambassadors on the “balcony”
Thought Leadership
Knowledge GenerationStrategic Imperative: Facilitate
evidence-based research approaches to inform practice and
learning in real time using standardized processes, scholarly
dissemination
Thought Leadership
Results: Annual Nexus Summit
27
2016 Summit
2017 Summit
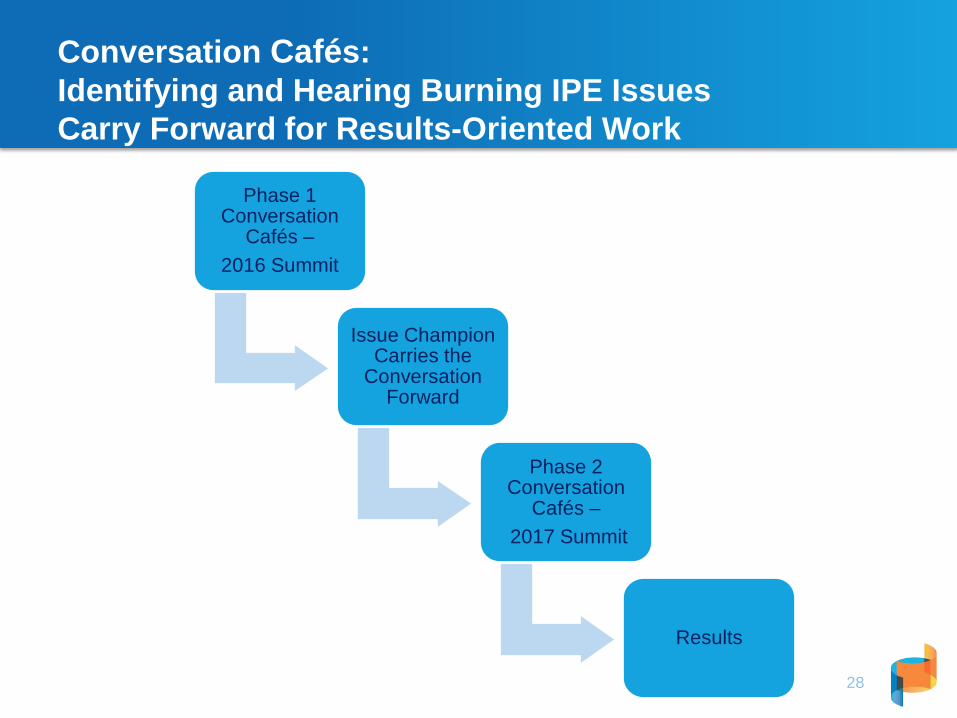
Conversation Cafés: Identifying and Hearing Burning IPE IssuesCarry Forward for Results-Oriented Work
28
Phase 1 Conversation
Cafés –2016 Summit
Issue Champion Carries the
Conversation Forward
Phase 2 Conversation
Cafés –2017 Summit
Results
Phase 1 (2016) and Phase 2 (2017)Conversations Cafés• Phase I to Phase II: Accreditation
– Focusing on new accreditation standards for IPE in pre-professional programs and interprofessional professional development, what criteria should be used to judge quality to promote new models of learning?
• Phase I to Phase II: The BIG Question– How do we help students, trainees, and practitioners gain the competencies to work in
new models of care when we are still practicing in traditional models?
• Phase I to Phase II: Organizational Models of IPE– What organizational models for aligning IPE and health care delivery will advance IPE
most effectively and efficiently?
• Phase I (2017): Team Optimization– What are the opportunities and unintended consequences of team optimization?
– What are the learning and education issues?
29
Phase I Cafe recommendations: Accreditation
• IPE is a recommendation that tends not to be effectively enforced.
• Different professions have different standards.
• Assessing IPE is challenging: Lack of clarity about what constitutes evidence of achievement of a standard.
• IPE needs to be purposefully incorporated into the curriculum.
• The IPE experience needs to be formalized.
• Outcomes need to be clearer.
30

Accreditation Conversation Café -Advancing the Dialogue in a 12 month cycle
31
During April 2017 ASPA convening, 23 accreditors signed on to work on a white paper about agreement on criteria for IPE
August 2016
September 2016
April 2017
August 2017
32
Knowledge Generation:What are we learning
33
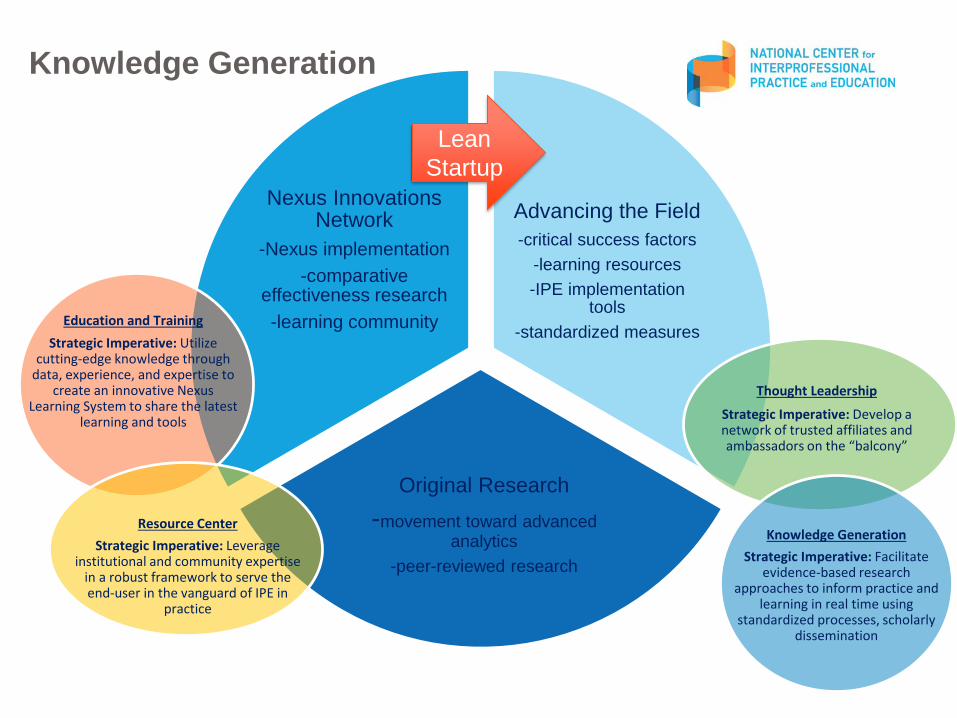
Advancing the Field-critical success factors
-learning resources-IPE implementation
tools-standardized measures
Original Research -movement toward advanced
analytics-peer-reviewed research
Nexus Innovations Network
-Nexus implementation-comparative
effectiveness research-learning community
34
Education and TrainingStrategic Imperative: Utilize
cutting-edge knowledge through data, experience, and expertise to
create an innovative Nexus Learning System to share the latest
learning and tools
Resource CenterStrategic Imperative: Leverage
institutional and community expertise in a robust framework to serve the end-user in the vanguard of IPE in
practice
Strategic Imperative: Develop a network of trusted affiliates and ambassadors on the “balcony”
Thought Leadership
Knowledge GenerationStrategic Imperative: Facilitate
evidence-based research approaches to inform practice and
learning in real time using standardized processes, scholarly
dissemination
Knowledge Generation
Lean Startup
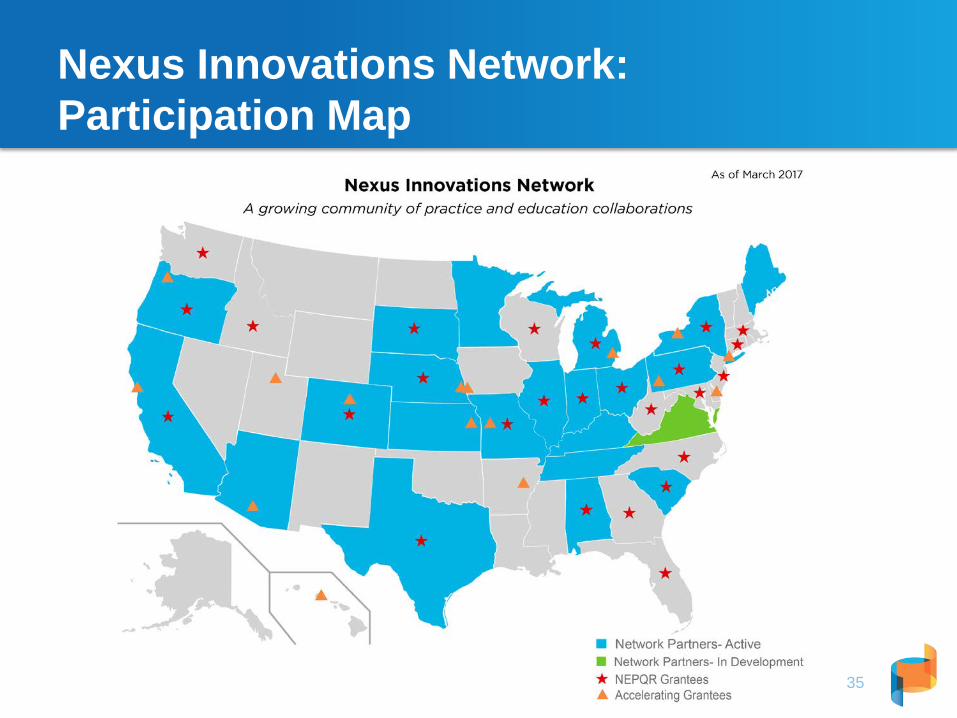
Nexus Innovations Network:Participation Map
35
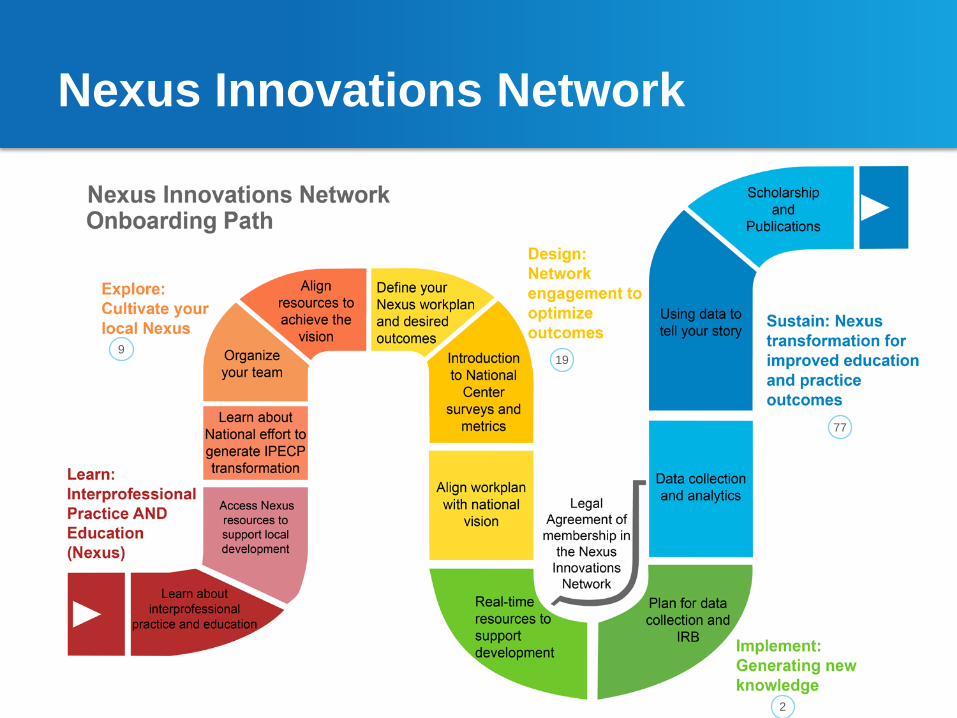
Nexus Innovations Network
• Onboarding path
36
199
2
77
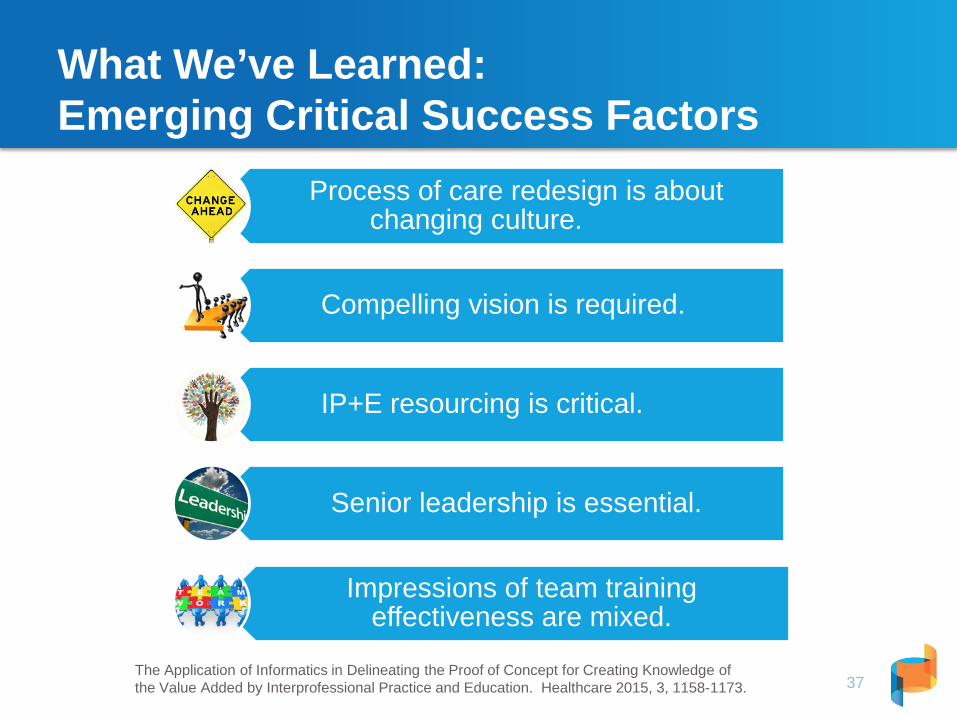
What We’ve Learned: Emerging Critical Success Factors
37
Process of care redesign is about changing culture.
Compelling vision is required.
IP+E resourcing is critical.
Senior leadership is essential.
Impressions of team training effectiveness are mixed.
The Application of Informatics in Delineating the Proof of Concept for Creating Knowledge of the Value Added by Interprofessional Practice and Education. Healthcare 2015, 3, 1158-1173.
Resource CenterNexusipe.org
38
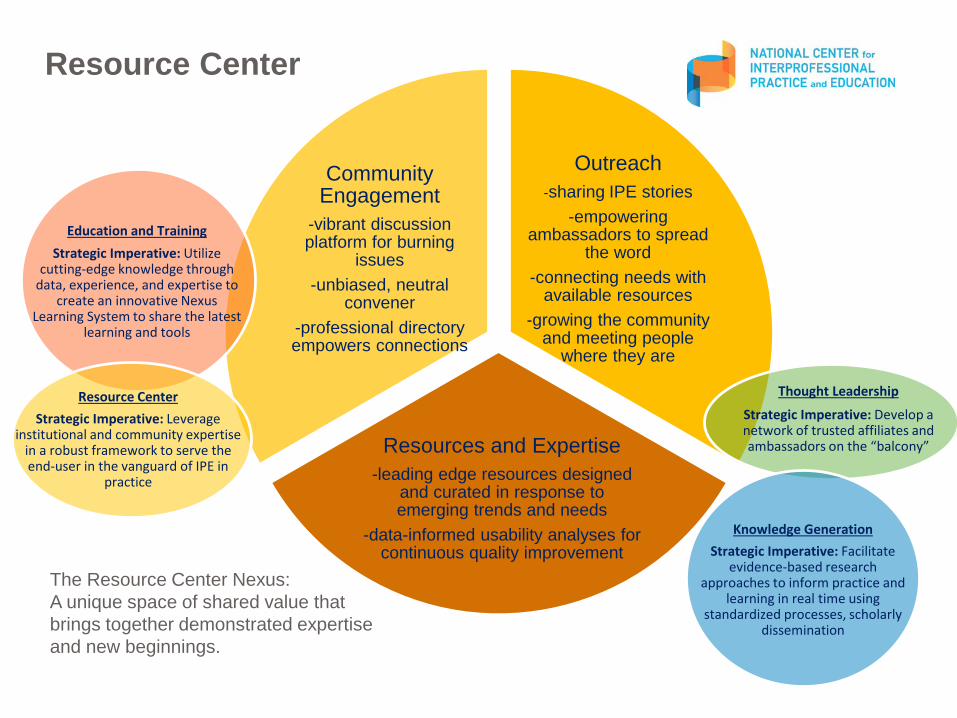
Outreach-sharing IPE stories
-empowering ambassadors to spread
the word-connecting needs with
available resources-growing the community
and meeting people where they are
Resources and Expertise-leading edge resources designed
and curated in response to emerging trends and needs
-data-informed usability analyses for continuous quality improvement
Community Engagement
-vibrant discussion platform for burning
issues-unbiased, neutral
convener-professional directory empowers connections
39
Education and TrainingStrategic Imperative: Utilize
cutting-edge knowledge through data, experience, and expertise to
create an innovative Nexus Learning System to share the latest
learning and tools
Resource CenterStrategic Imperative: Leverage
institutional and community expertise in a robust framework to serve the end-user in the vanguard of IPE in
practice
The Resource Center Nexus:A unique space of shared value that brings together demonstrated expertise and new beginnings.
Strategic Imperative: Develop a network of trusted affiliates and ambassadors on the “balcony”
Thought Leadership
Knowledge GenerationStrategic Imperative: Facilitate
evidence-based research approaches to inform practice and
learning in real time using standardized processes, scholarly
dissemination
Resource Center
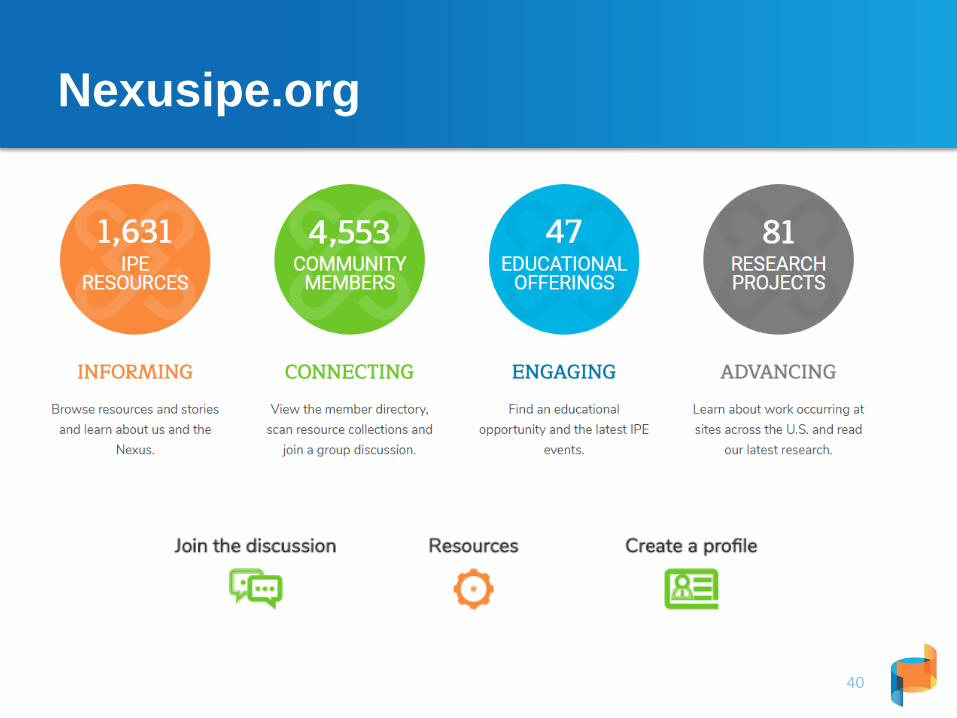
Nexusipe.org
40
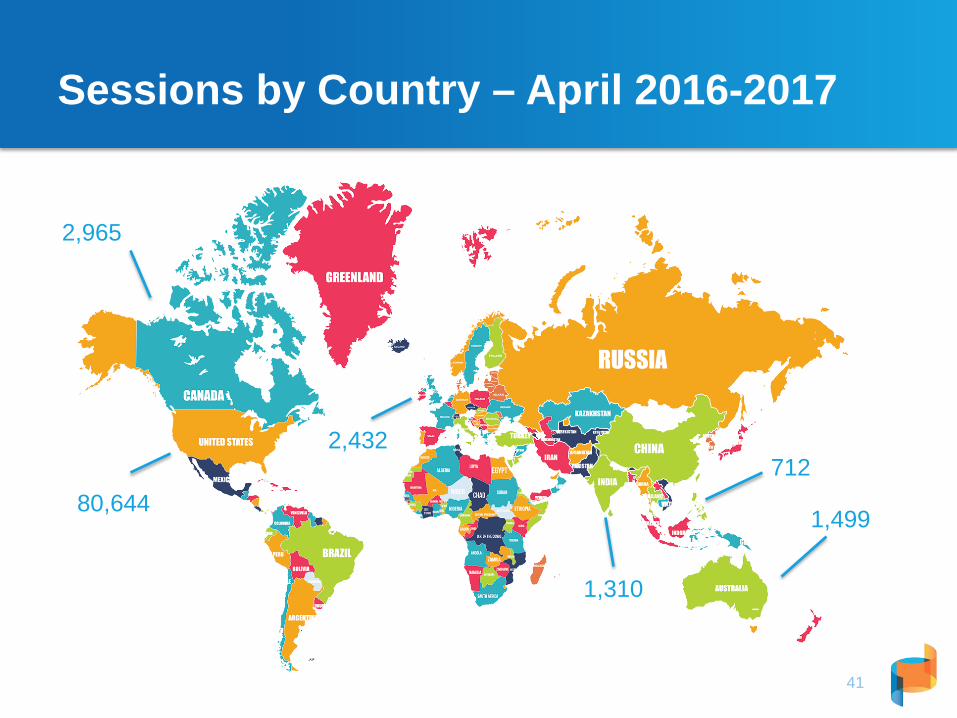
Sessions by Country – April 2016-2017
41
80,644
2,965
1,499
1,310
2,432712
Resource Center: Freely Available Institutional and Community Expertise
42
Resource Center: Amina and Carl in the Nexus
43
Number One Request: “Assessment”
• Evolution of the measurement collection• Importance of research on linkages between education,
practice, and Triple Aim (cost, quality, patient experience)
44
Community generatedopen source exchange
26 toolsin curated collection
Building community
capacity
2014 2017
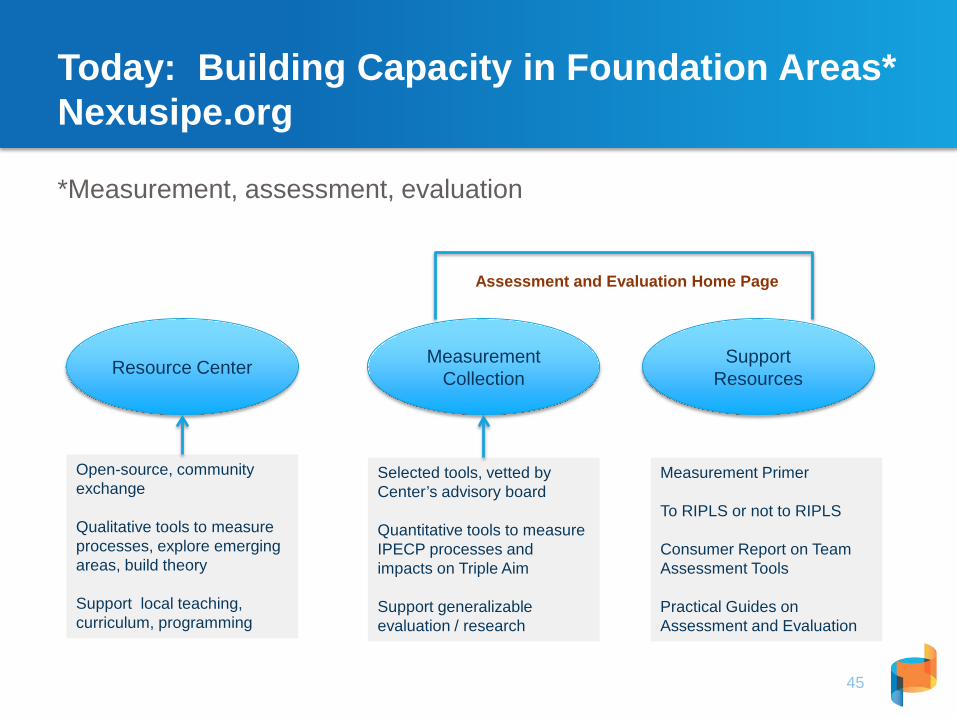
Today: Building Capacity in Foundation Areas*Nexusipe.org
*Measurement, assessment, evaluation
45
Measurement CollectionResource Center Support
Resources
Open-source, community exchange
Qualitative tools to measure processes, explore emerging areas, build theory
Support local teaching, curriculum, programming
Selected tools, vetted by Center’s advisory board
Quantitative tools to measure IPECP processes and impacts on Triple Aim
Support generalizable evaluation / research
Measurement Primer
To RIPLS or not to RIPLS
Consumer Report on Team Assessment Tools
Practical Guides on Assessment and Evaluation
Assessment and Evaluation Home Page
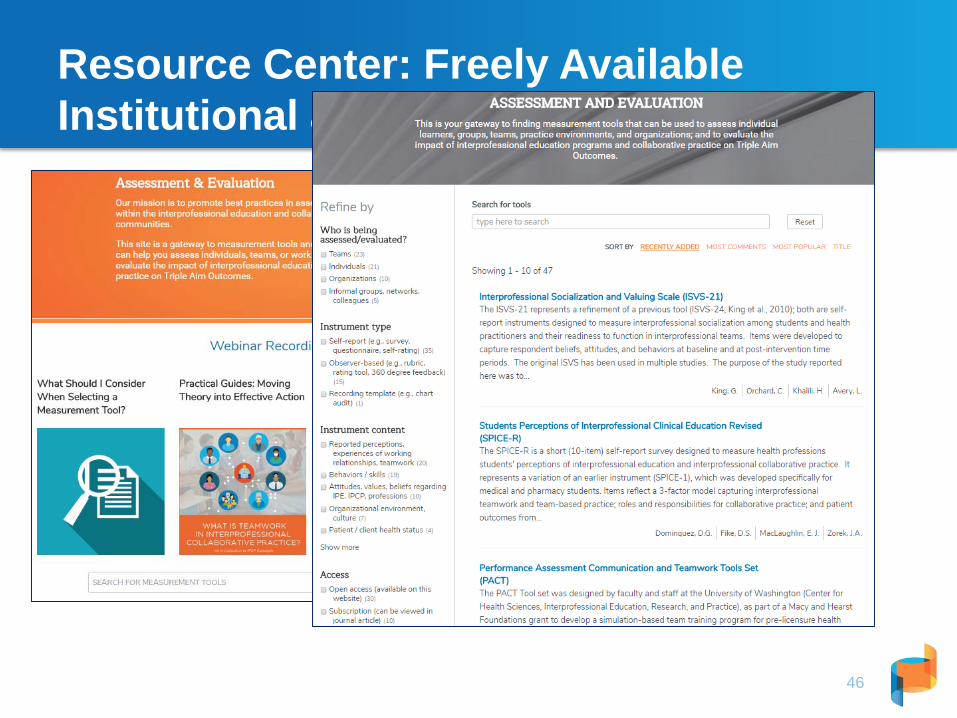
Resource Center: Freely Available Institutional and Community Expertise
46
Resource Center: Freely Available Institutional and Community Expertise
47
Resource Center: Freely Available Institutional and Community Expertise
48
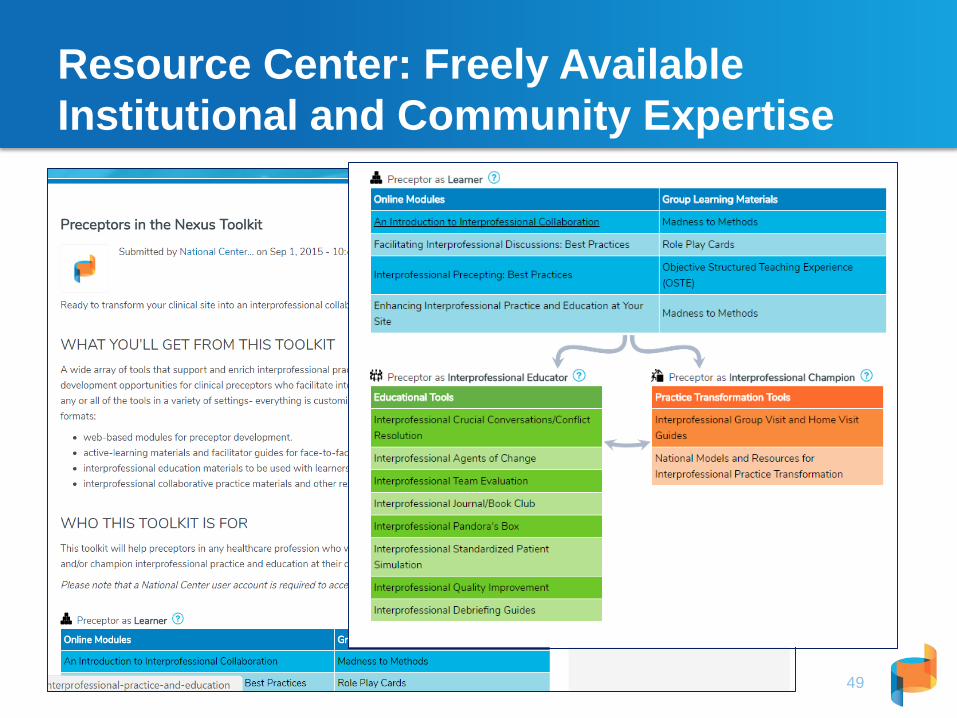
Resource Center: Freely Available Institutional and Community Expertise
49
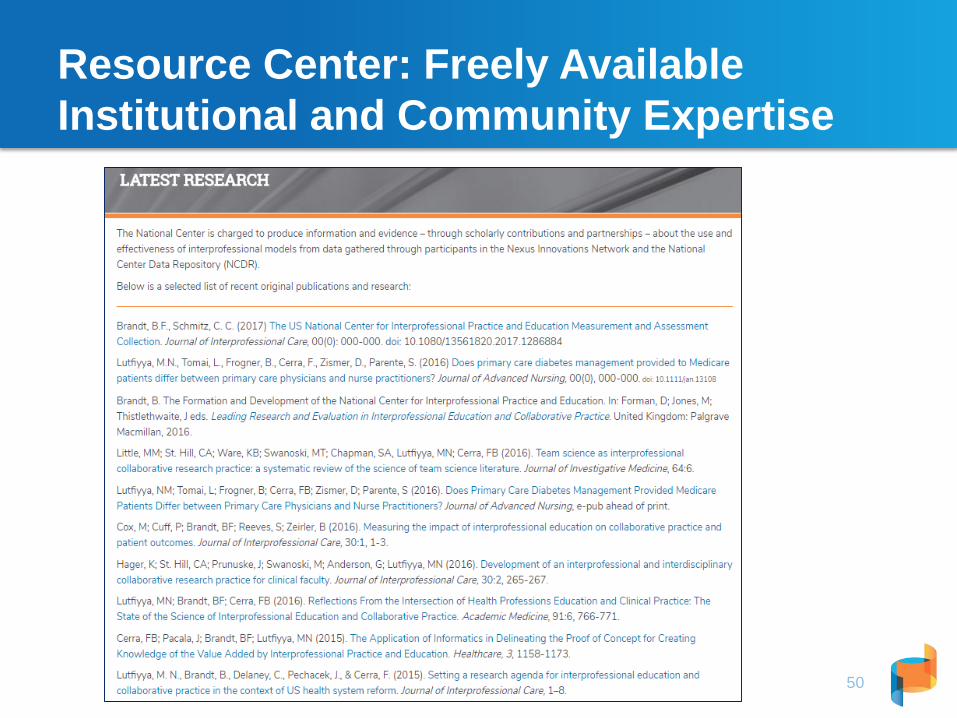
Resource Center: Freely Available Institutional and Community Expertise
50
Education and Training
51
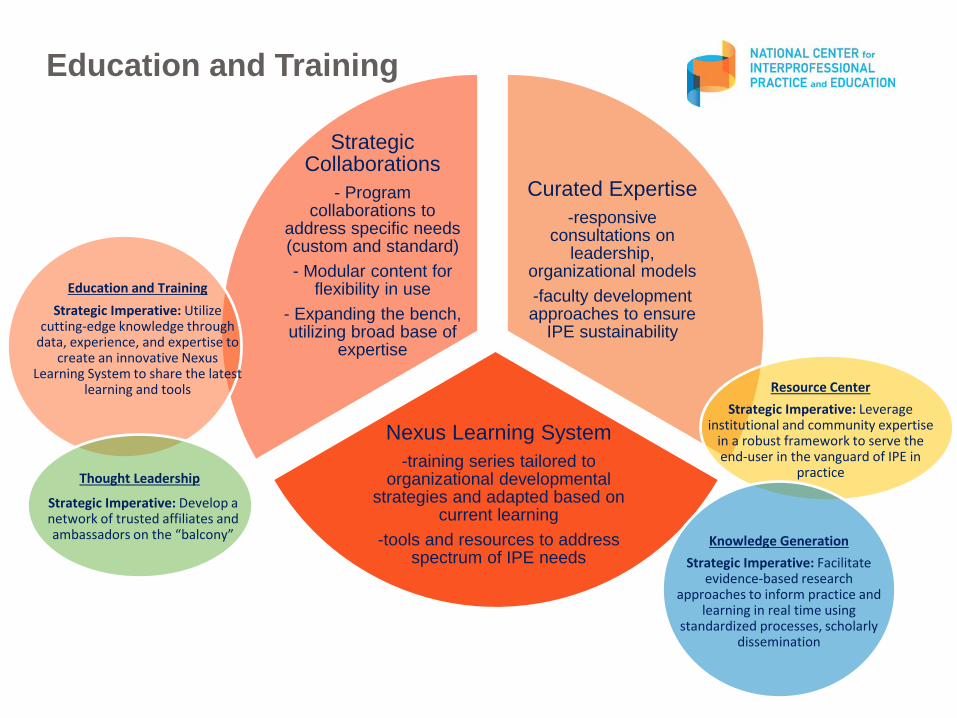
Curated Expertise-responsive
consultations on leadership,
organizational models-faculty development approaches to ensure
IPE sustainability
Nexus Learning System-training series tailored to
organizational developmental strategies and adapted based on
current learning-tools and resources to address
spectrum of IPE needs
Strategic Collaborations
- Program collaborations to
address specific needs (custom and standard)- Modular content for
flexibility in use- Expanding the bench, utilizing broad base of
expertise
52
Education and TrainingStrategic Imperative: Utilize
cutting-edge knowledge through data, experience, and expertise to
create an innovative Nexus Learning System to share the latest
learning and tools Resource CenterStrategic Imperative: Leverage
institutional and community expertise in a robust framework to serve the end-user in the vanguard of IPE in
practice
Strategic Imperative: Develop a network of trusted affiliates and ambassadors on the “balcony”
Thought Leadership
Knowledge GenerationStrategic Imperative: Facilitate
evidence-based research approaches to inform practice and
learning in real time using standardized processes, scholarly
dissemination
Education and Training
53
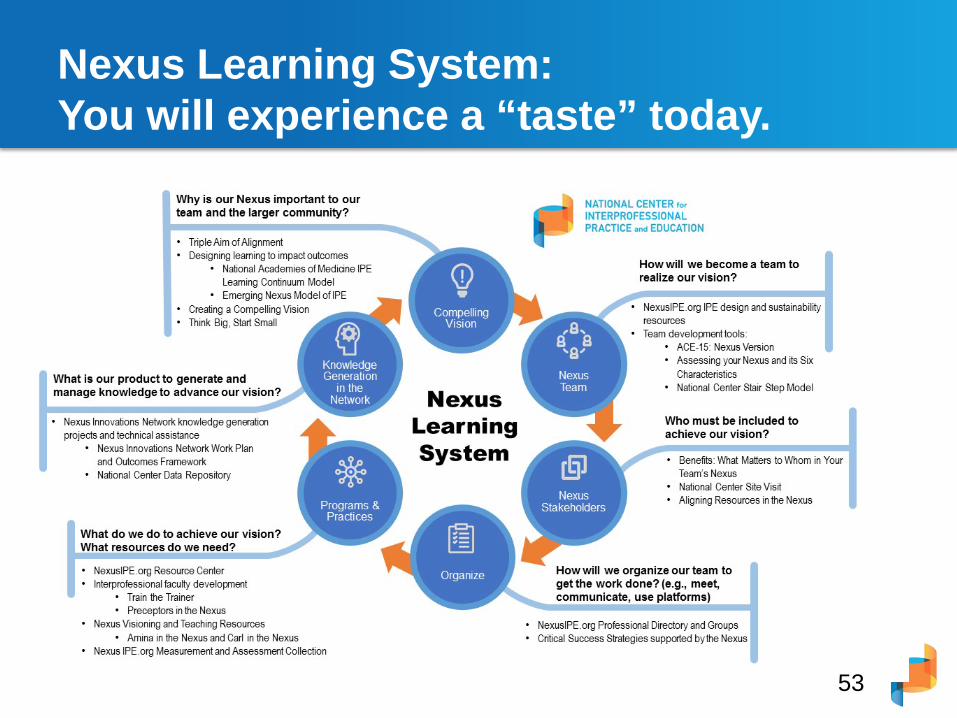
Nexus Learning System: You will experience a “taste” today.
National Center 2017 Learning Opportunities
54
Morning Break
55
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
Barbara F. Brandt, PhD Director, National Center for Interprofessional Practice and Education
Susan M. Meyer, PhDChair, Nexus Learning System Advisory Council
June 9, 2017 University of Texas - Houston
Aligning Interprofessional Education with Clinical Practice Redesign: What It Means for Amina and Carl

Amina in the Nexus
57Click here to watch Amina
Interviews to learn about the Nexus at the micro level: academic-clinical practice• Seven PCMHs selected by Patient-Centered Primary
Care Collaborative
• National Center participated in interviews to learn:• Presence of interprofessional education • “Nexus” – alignment of IPE with clinical practice redesign
• What are characteristics of sites that display both, as reported in the interviews?
• Articulate themes to inform new development
Characteristics of the Patient Centered Medical Home (PCMH)
A team-based health care delivery model
Continuous care to populations of patients with the goal of obtaining maximized health outcomes
An approach to providing comprehensive primary care for children, youth and adults
Shift care from acute to ambulatory / community settings
Care coordination – essential, requiring additional resources – health information technology – appropriately trained staff to provide coordinated care– workforce redesign
Reduce costs
Interprofessional Education and Collaborative PracticeThe “New IPE” – Interprofessional Practice and Education
60
Interprofessional education “occurs when two or moreprofessions learn with, about, and from each other toenable effective collaboration and improve healthoutcomes.”
Interprofessional, collaborative practice “occurs whenmultiple health workers and students and residents fromdifferent professional backgrounds provide comprehensivehealth services by working with patients, their families,carers (caregivers), and communities to deliver the highestquality of care across settings.”Adapted from:The Centre for the Advancement of Interprofessional Education, UK, 1987World Health Organization, Framework for Action on Interprofessional Education and Collaborative Practice, 2010.
The Nexus: Our Vision for Healthnexusipe.org
61
Triple Aim of AlignmentImproving quality of experience for patients, families, communities and learners
Sharing responsibility for achieving health outcomes and improved learning
Reducing cost and adding value in health care delivery and education
Elements of the “Nexus”
• integrate clinical practice and education in new ways,
• partner with patients, families, and communities,
• strive to achieve the Triple Aim in both health care and education (cost, quality, and populations),
• incorporate students and residents into the interprofessionalteam in meaningful ways,
• create a shared resource model to achieve goals, and
• encourage leadership in all aspect of the partnership.
Three Programs
• University of Oklahoma’s Family Medicine Center,
• San Francisco Veterans Administration Medical Center
• New Mexico State University Counseling Psychology Program
Refined Definition of the Nexus
“Clinical practices in transforming systems that partner with health professions education programs
think and act differently
learning organizations that support continuous professional development
while educating the next generation of health professionals”
Characteristics
• Sharing a vision
• The patient-centered curriculum
• Innovation for culture change
• Spontaneous team leaders
• Benefits of the Nexus to the practice
• Benefits of the Nexus to students and residents
Sharing a vision
• An extraordinary commitment to workforce development between PCMH and partner health professions education program
• Able to articulate common purpose and strategies to address significant barriers– Understand and meet each partner’s needs and
perspectives– Bridge culture to create new one – Significant face-to-face time, often unpaid – Builds relationships, trust and working appreciation
for one another
The patient-centered curriculum
Start with the patient in mind: not clinical practice or health professional education program
Being PCMH helps with relevant educational program
Successful strategies:• Needs of patient, then incorporate learner• Shared decision-making partnership with patients
explicitly role models the needs and wants of patients for all learners
Innovation for culture change
• Explicitly articulated:
– Essential role of site champions – A commitment to a fundamental cultural shift
away from a traditional, hierarchical to more innovative team-based approach
– Critical to transformation of clinical practice– Teaching / learning strategies to learn in practice
how to function in teams – Small changes add up
Spontaneous team leaders
• Shift to patient-centered curriculum
• Role of collaboration and conflict resolution skills
• Promotes leadership no matter which profession or whether clinician, student or resident
• Naturally learning new skills in practice
Benefits of the Nexus to the Practice
• Benefits to the whole site, including clinicians and staff
• Students and residents bring new ideas about interprofessional education and collaborative practice
• Students asking “tough questions” about efficient and effective patient care
Benefits of the Nexus to students and residents
• Intentionally trained in skills needed in practice
• More “collaboration-ready” and confident
• Marketable skills
• Prepared for practice in underserved areas
• Learn to address barriers to practice
Practical Take Homes
• Start with the patient in mind
• Design for practice and education model around principles of PCMH
• Significant commitment to develop a shared vision that benefits all
Resource Center: Freely Available Institutional and Community Expertise
73
Click here to watch Carl in the Nexus
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
Working Session 1:
Think BIG and Start SMALL: Using the National Academies of Medicine Interprofessional Learning Continuum Framework
Susan M. Meyer, PhDChair, National Center Nexus Learning System Advisory CommitteeCo-director, University of Pittsburgh Center for Interprofessional Practice and EducationAssociate Dean for Education and Professor, University of Pittsburgh School of Pharmacy
Friday, June 9, 2017
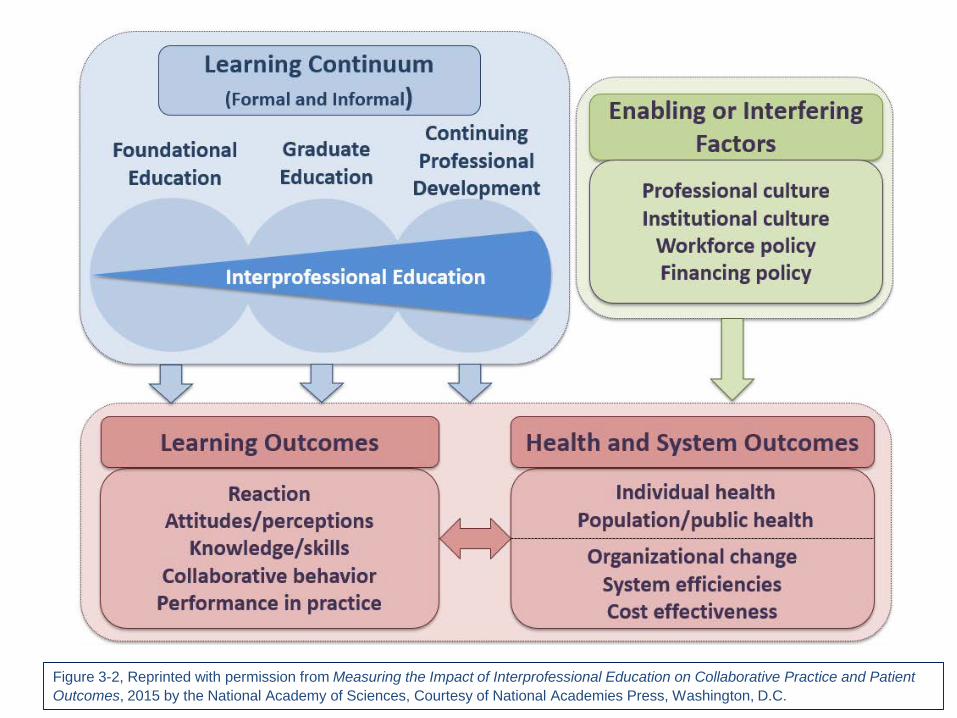
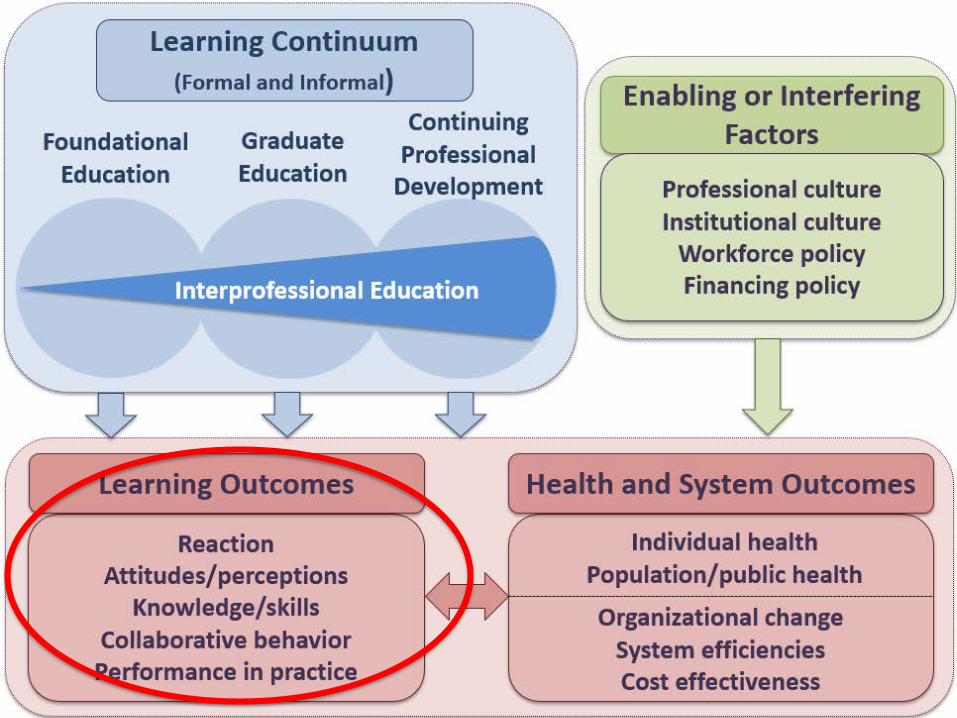
75Figure 3-2, Reprinted with permission from Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes, 2015 by the National Academy of Sciences, Courtesy of National Academies Press, Washington, D.C.
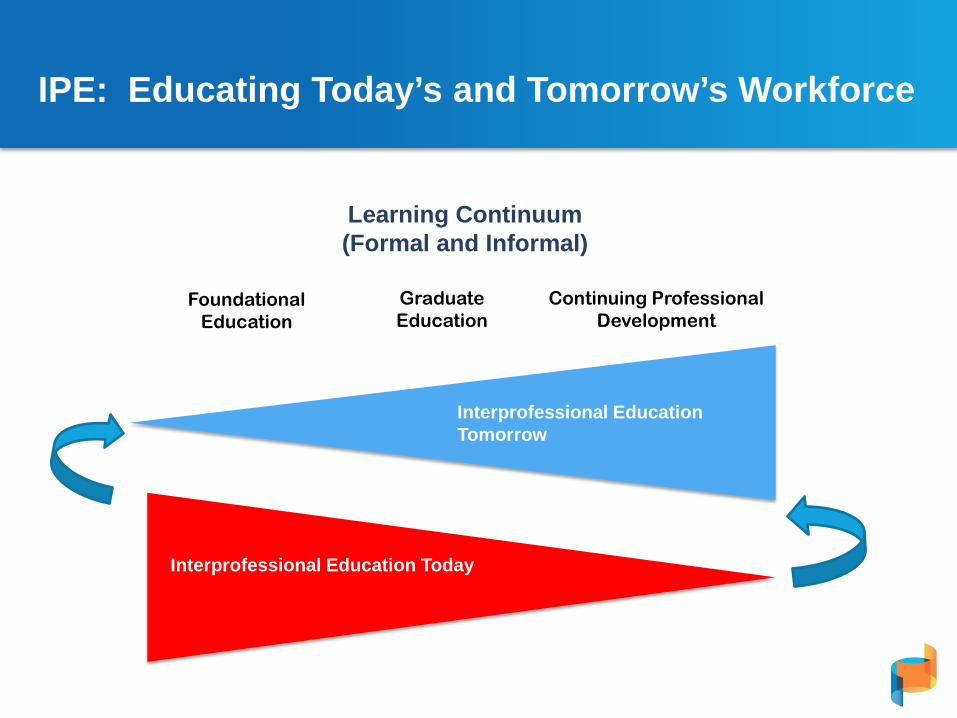
IPE: Educating Today’s and Tomorrow’s Workforce
Learning Continuum(Formal and Informal)
FoundationalEducation
GraduateEducation
Continuing Professional Development
Interprofessional Education Today
Interprofessional Education Tomorrow
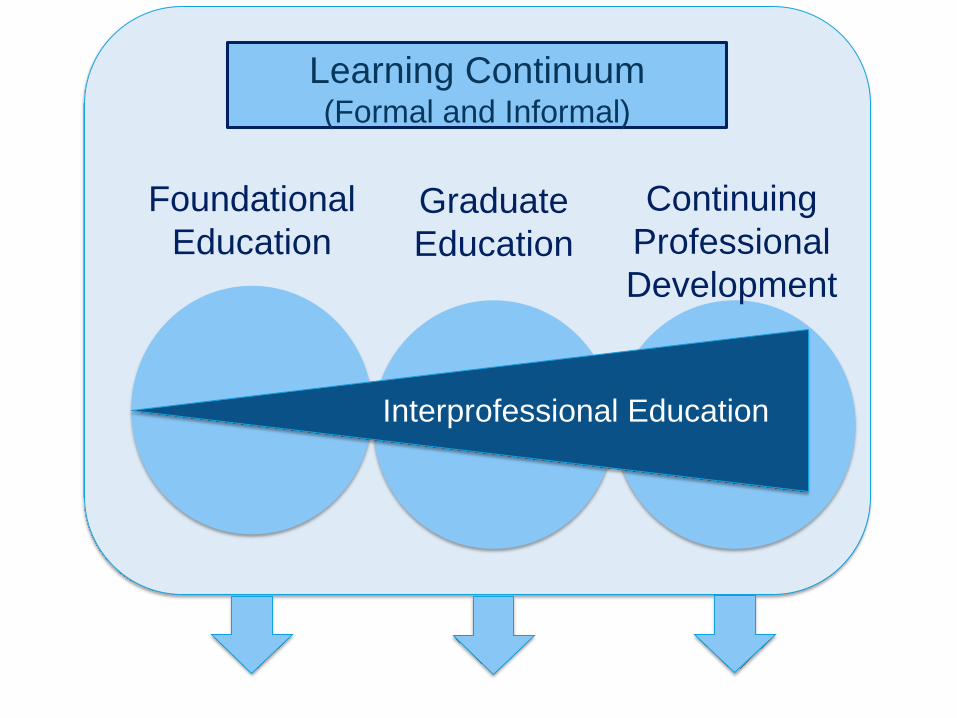
Learning Continuum(Formal and Informal)
Interprofessional Education
Foundational Education
Graduate Education
ContinuingProfessional Development
Where on the LEARNING CONTINUUM are your efforts focused?
What are defining features of your INTERPROFESSIONAL EDUCATION activities?
Who is/are the LEARNER(S)?
79
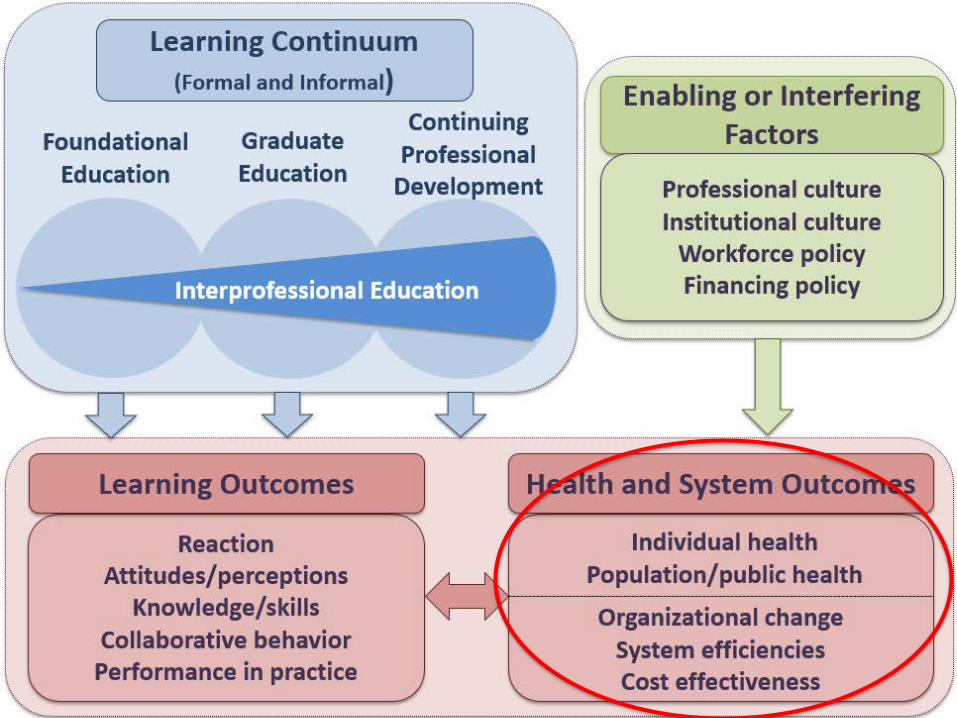
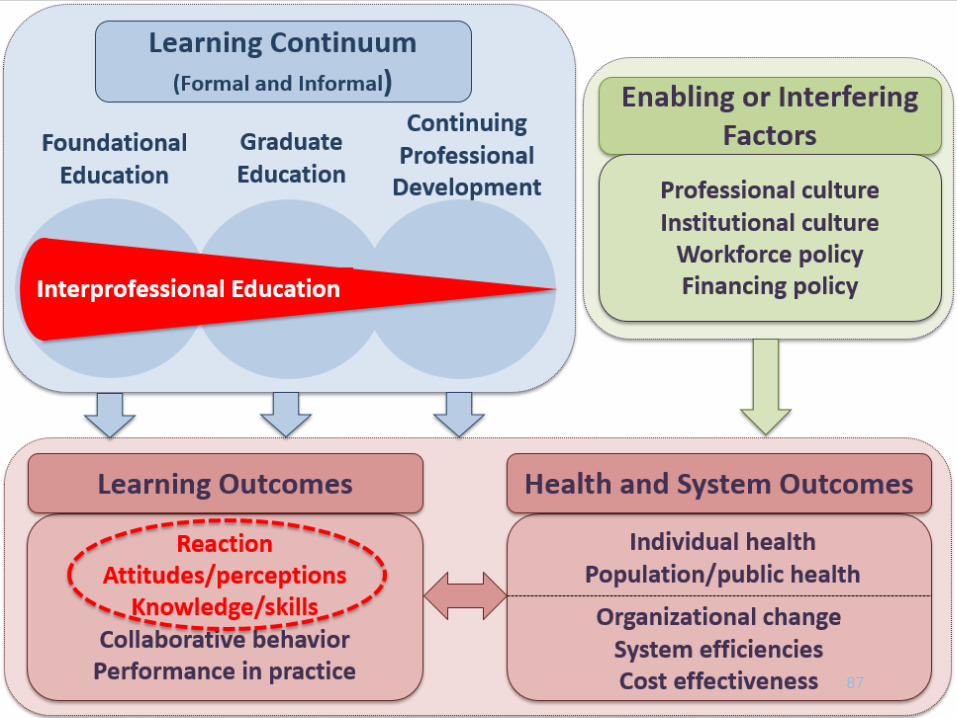
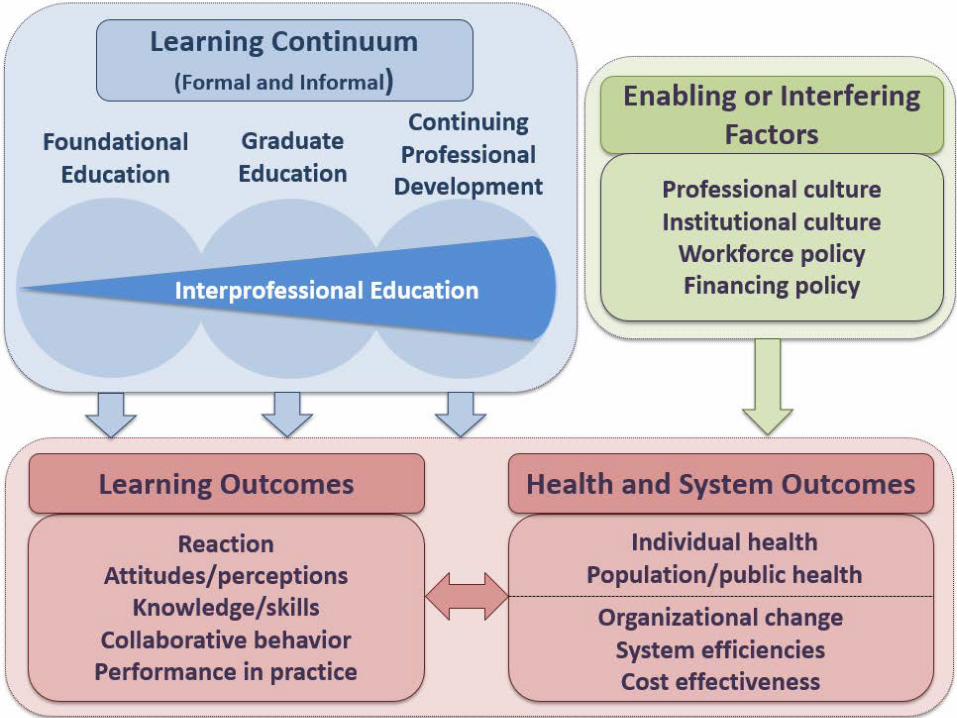
IOM (Institute of Medicine. 2015. Measure the impact of interprofessional education on collaborative practice and patient outcomes. Washington, DC: The National Academies Press.
FIGURE 3-2 The interprofessional learning continuum (IPLC) model.NOTE: For this model, “graduate education” encompasses any advanced formal or supervised health professions training taking place between completion of founda-tional education and entry into unsupervised practice.
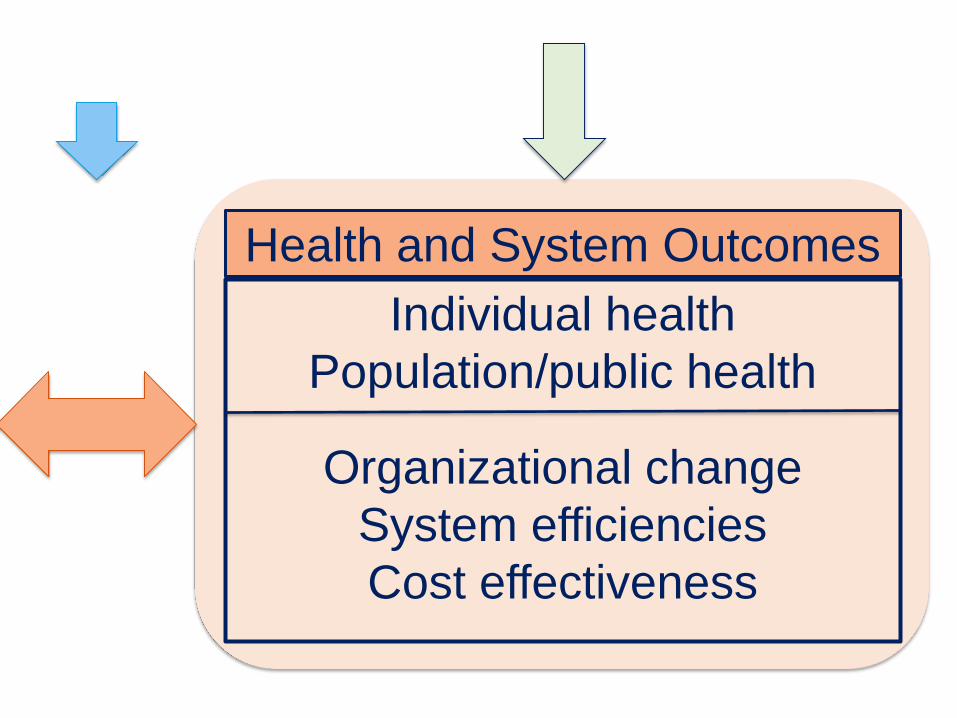
Health and System OutcomesIndividual health
Population/public health
Organizational changeSystem efficienciesCost effectiveness
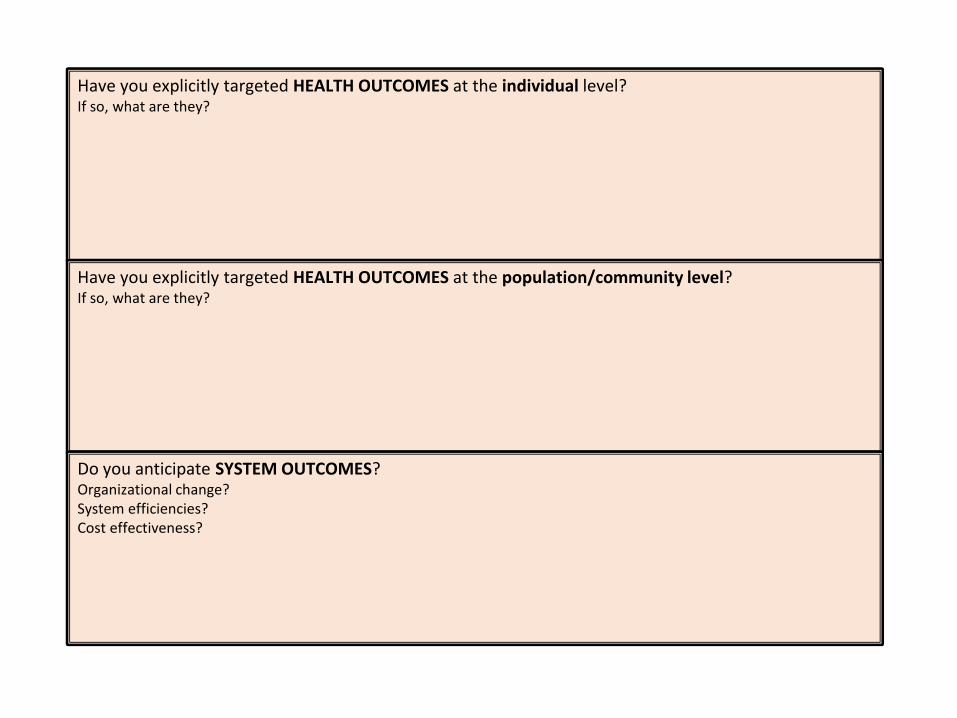
Have you explicitly targeted HEALTH OUTCOMES at the individual level?If so, what are they?
Have you explicitly targeted HEALTH OUTCOMES at the population/community level?If so, what are they?
Do you anticipate SYSTEM OUTCOMES?Organizational change?System efficiencies?Cost effectiveness?
82
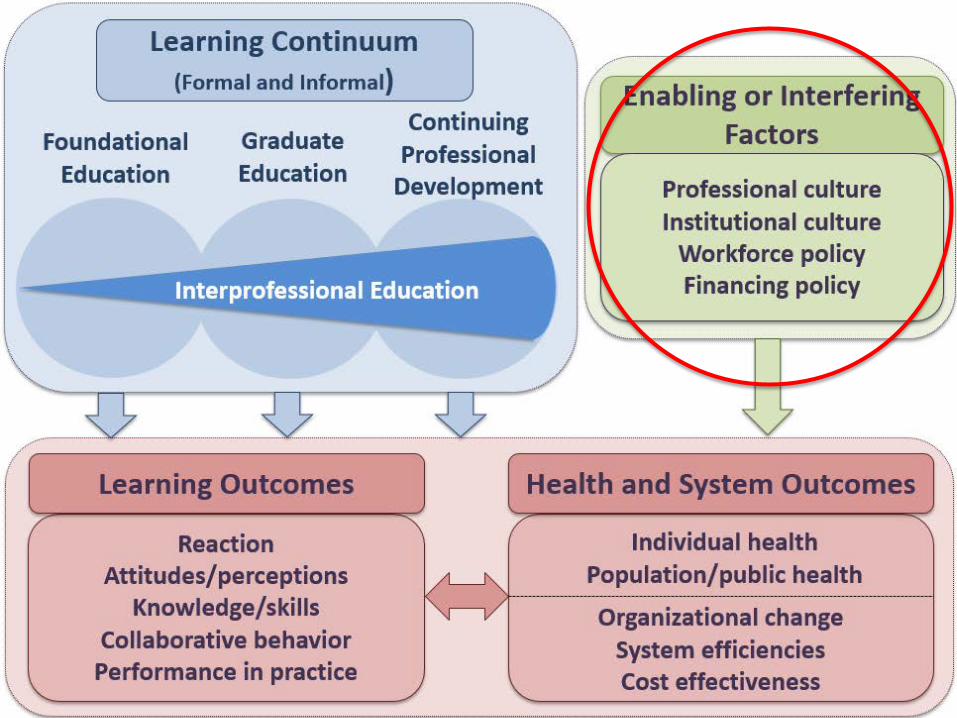
IOM (Institute of Medicine. 2015. Measure the impact of interprofessional education on collaborative practice and patient outcomes. Washington, DC: The National Academies Press.
FIGURE 3-2 The interprofessional learning continuum (IPLC) model.NOTE: For this model, “graduate education” encompasses any advanced formal or supervised health professions training taking place between completion of founda-tional education and entry into unsupervised practice.
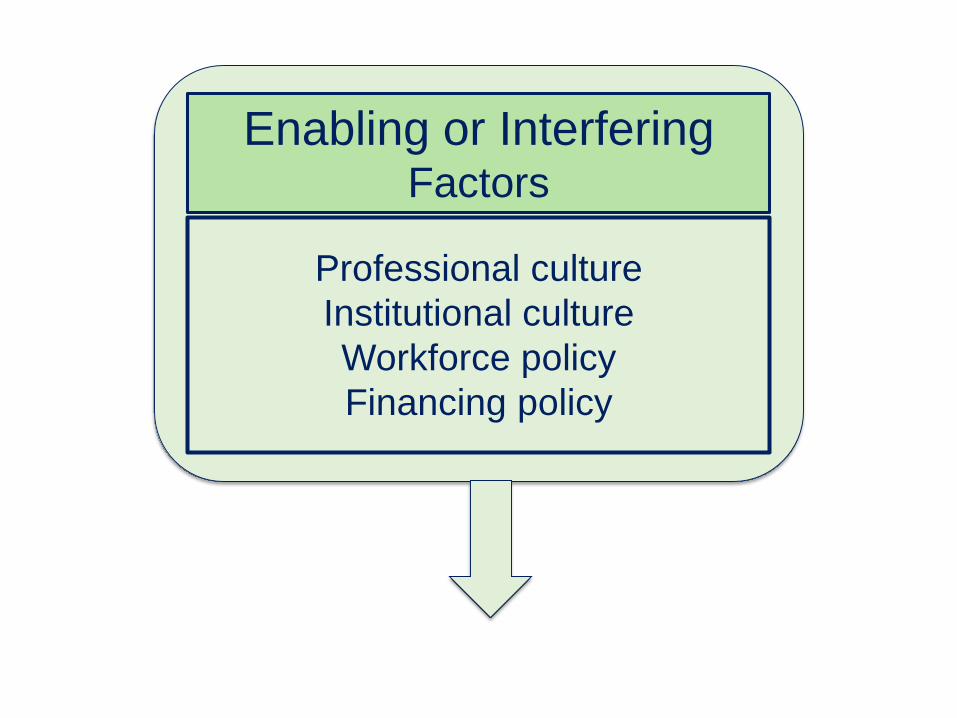
Enabling or InterferingFactors
Professional cultureInstitutional cultureWorkforce policyFinancing policy
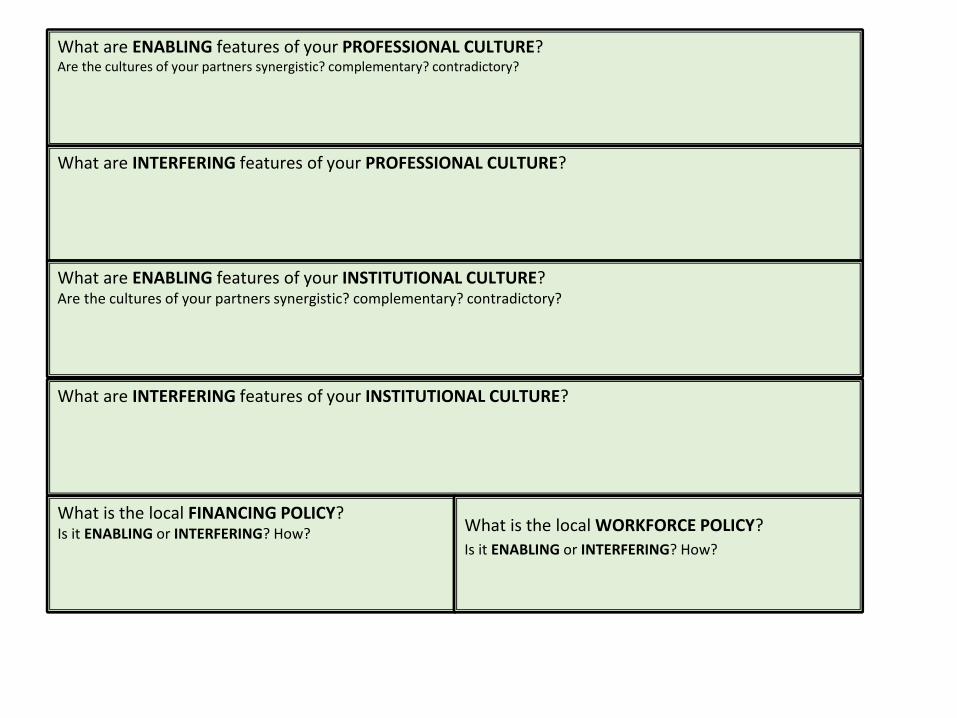
What are ENABLING features of your PROFESSIONAL CULTURE?Are the cultures of your partners synergistic? complementary? contradictory?
What are INTERFERING features of your PROFESSIONAL CULTURE?
What are ENABLING features of your INSTITUTIONAL CULTURE?Are the cultures of your partners synergistic? complementary? contradictory?
What are INTERFERING features of your INSTITUTIONAL CULTURE?
What is the local FINANCING POLICY? Is it ENABLING or INTERFERING? How? What is the local WORKFORCE POLICY?
Is it ENABLING or INTERFERING? How?
85
IOM (Institute of Medicine. 2015. Measure the impact of interprofessional education on collaborative practice and patient outcomes. Washington, DC: The National Academies Press.
FIGURE 3-2 The interprofessional learning continuum (IPLC) model.NOTE: For this model, “graduate education” encompasses any advanced formal or supervised health professions training taking place between completion of founda-tional education and entry into unsupervised practice.
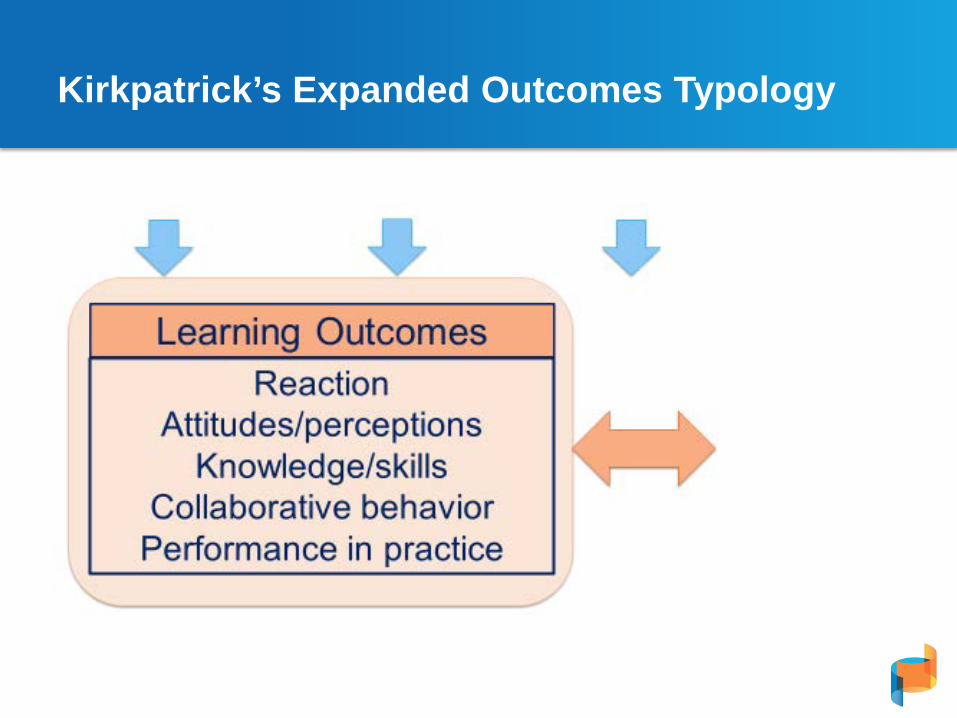
Kirkpatrick’s Expanded Outcomes Typology
87
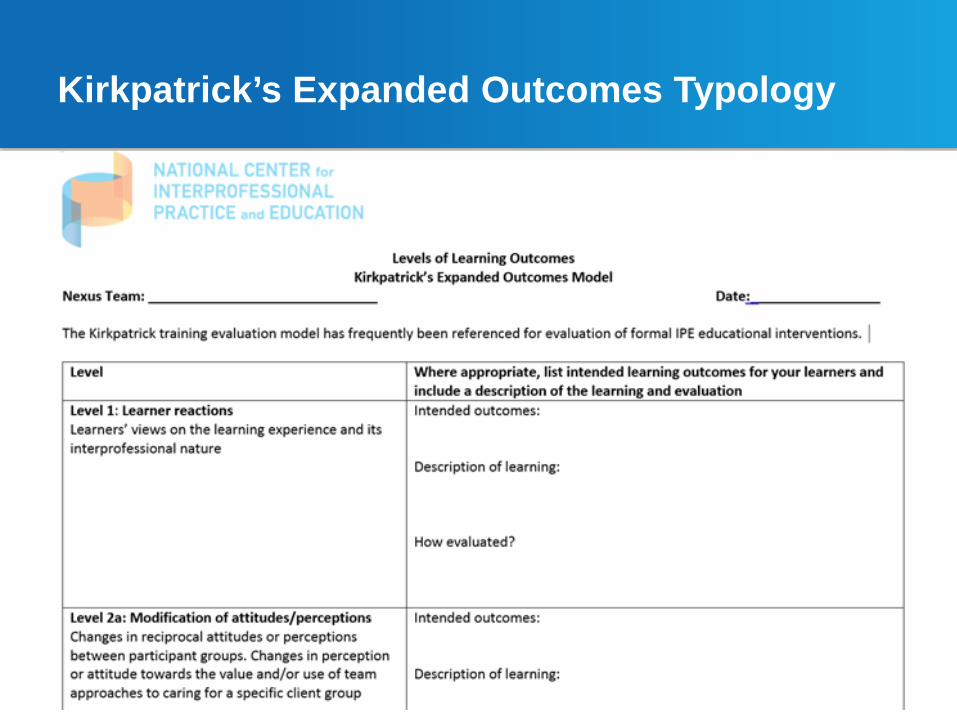
Kirkpatrick’s Expanded Outcomes Typology
89
Lunch
90
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
Working Session 2:
Designing Your Future - The “Stairstep” View of Nexus Developmental Stages- SOARR: Strengths and Assets, Opportunities, Aspirations and Results, ResourcesBarbara F. Brandt, PhD Director, National Center for Interprofessional Practice and Education
Susan M. Meyer, PhDChair, National Center Nexus Learning System Advisory Committee
June 9, 2017
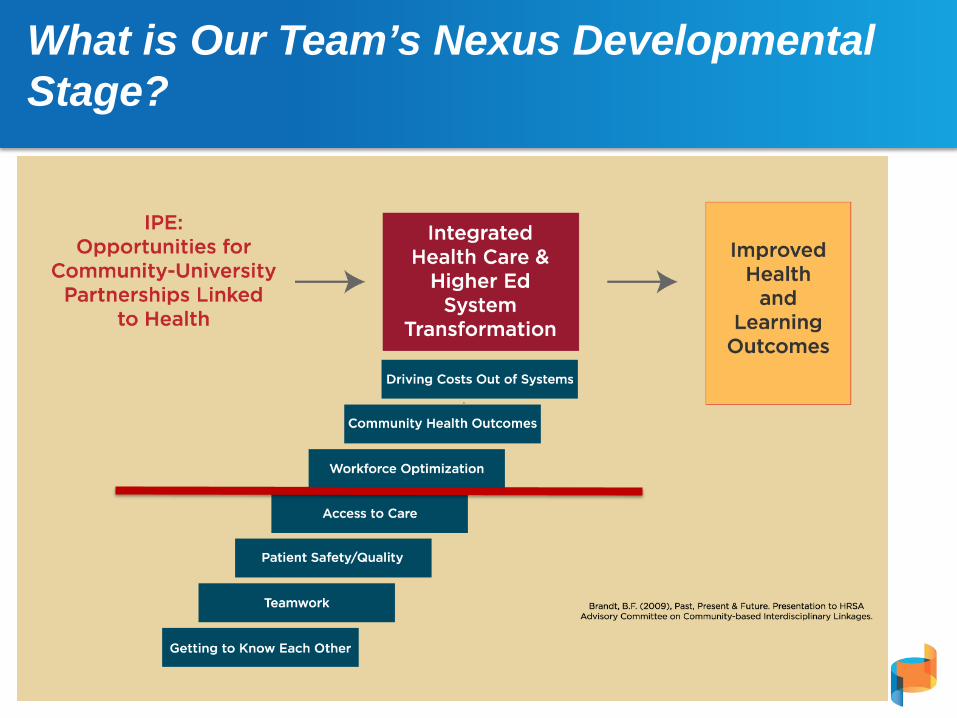
What is Our Team’s Nexus Developmental Stage?
92
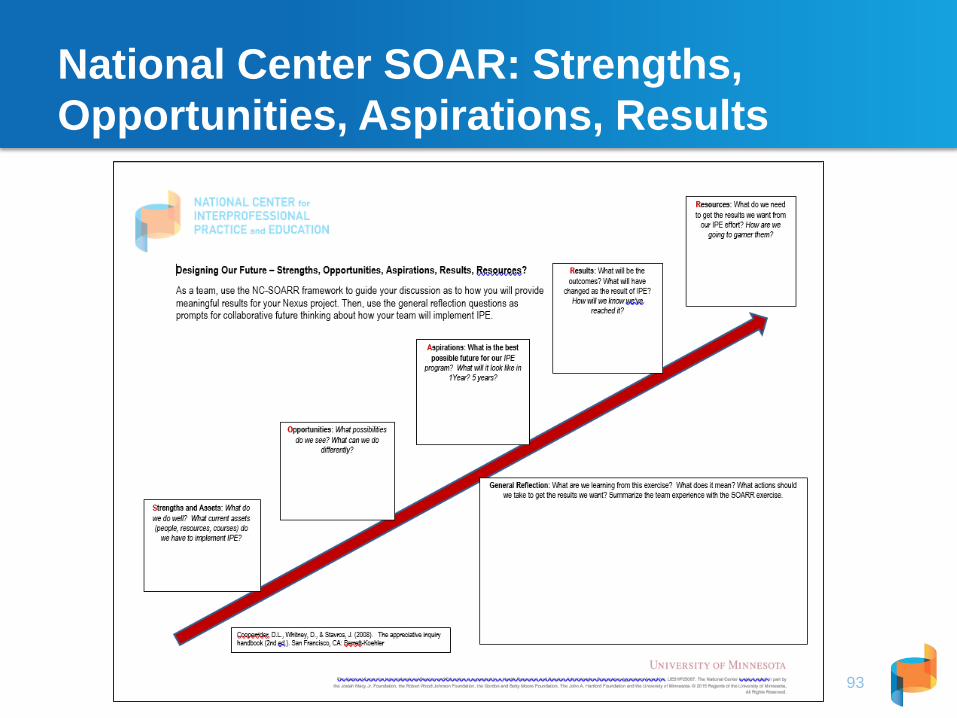
National Center SOAR: Strengths, Opportunities, Aspirations, Results
93
The National Center for Interprofessional Practice and Education is supported by a Health Resources and Services Administration Cooperative Agreement Award No. UE5HP25067. The National Center is also funded in part by the Josiah Macy Jr. Foundation, the Robert Wood Johnson Foundation, the Gordon and Betty Moore Foundation, The John A. Hartford Foundation and the University of Minnesota. © 2015 Regents of the University of Minnesota, All Rights Reserved.
https://nexusipe.org
https://www.facebook.com/nexusipe
https://twitter.com/nexusipe
https://www.linkedin.com/company/6382596