Embed Size (px)
Citation preview

R
Ut
Na
b
ARRAA
KTESAM
C
1
poiTmiPgcn
eA
1h
Ageing Research Reviews 12 (2013) 833– 839
Contents lists available at SciVerse ScienceDirect
Ageing Research Reviews
j ourna l h om epage: www.elsev ier .com/ locate /ar r
eview
sing memories to understand others: The role of episodic memory inheory of mind impairment in Alzheimer disease
oémie Moreaua,b,∗, Franc ois Vialleta,b, Maud Champagne-Lavaua
Aix-Marseille Université, CNRS, LPL UMR 7309, 5 Avenue Pasteur, 13604 Aix-en-Provence, FranceCentre hospitalier du Pays d’Aix, Department of Neurology, Avenue des Tamaris, 13616 Aix-en-Provence, France
a r t i c l e i n f o
rticle history:eceived 14 February 2013eceived in revised form 26 June 2013ccepted 27 June 2013vailable online xxx
a b s t r a c t
Theory of mind (TOM) refers to the ability to infer one’s own and other’s mental states. Growing evidencehighlighted the presence of impairment on the most complex TOM tasks in Alzheimer disease (AD). How-ever, how TOM deficit is related to other cognitive dysfunctions and more specifically to episodic memoryimpairment – the prominent feature of this disease – is still under debate. Recent neuroanatomical find-ings have shown that remembering past events and inferring others’ states of mind share the same
eywords:heory of mindpisodic memoryelf-projectionlzheimer disease
cerebral network suggesting the two abilities share a common process .This paper proposes to reviewemergent evidence of TOM impairment in AD patients and to discuss the evidence of a relationshipbetween TOM and episodic memory. We will discuss about AD patients’ deficit in TOM being possiblyrelated to their difficulties in recollecting memories of past social interactions.
© 2013 Elsevier B.V. All rights reserved.
ild cognitive impairmentontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8332. TOM impairment in AD and amnesic MCI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8343. Memory and theory of mind: Common cognitive processes?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8354. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 837
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 838References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 838
. Introduction
Alzheimer disease (AD) is clinically defined by an early androminent episodic memory impairment, associated with at leastne other cognitive dysfunction, and behavioural symptoms affect-ng autonomy in daily living activities (McKhann et al., 1984, 2011).he amnesic syndrome constitutes its core feature and is thus theost described symptom of this disease, even in prodromal stages,
.e., mild cognitive impairment (MCI) due to AD (Albert et al., 2011;
2010; Bertoux et al., 2012; Lough et al., 2006, 2001). This set ofstudies has led to the formulation of new neuropsychological crite-ria in the future publication of the DSM-5 manual of AmericanPsychiatric and Association (2013). Social cognition would take partin the DSM-5 classification for “Major Neurocognitive Disorders”,including frontotemporal and Alzheimer dementias. Such inclusionsuggests that deficit in social cognition would soon be considered asa hallmark of neuropsychological impairment in these diseases andwould have to be systematically assessed through cognitive evalu-ations. However, little is known about social cognition dysfunction
etersen, 2004). Recently, research on social cognition in neurode-enerative diseases, mainly in frontotemporal dementia, has grownonsiderably. Impaired social cognition was described as a promi-ent feature of frontotemporal lobar degeneration (Adenzato et al.,
∗ Corresponding author at: Service neurologie, CH Pays d’Aix, Laboratoire Parolet Langage, CNRS UMR 7309, Aix-Marseille Université, Avenue des Tamaris, 13616ix-en-Provence, Cedex 1, France. Tel.: +33 4 42 33 50 71; fax: +33 4 42 33 51 58.
E-mail addresses: [email protected], [email protected] (N. Moreau).
568-1637/$ – see front matter © 2013 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.arr.2013.06.005
in AD patients.Social cognition is defined as the capacity to interpret and
predict others’ behaviours according to their beliefs, intentions,emotions, and to decode social stimuli from the environment inorder to adapt one’s own behaviour in social situations (Adolphs,
2006). Mentalizing or theory of mind (TOM), is the abilitywhereby “an individual attributes mental states to himself and others”(Premack and Woodruff, 1978) and so constitutes a central aspectof social cognition. In other words, TOM refers to the capacity to
8 earch
ussc(w(mida
atearaa(
se2dhde
irtwnwbrsK“ci“
2
pe2idTop2ewt(tws
i
34 N. Moreau et al. / Ageing Res
nderstand that people’s behaviours are directed by their mentaltates, their intentions and beliefs about the world. Some authorsuggested that TOM would not be a specific module of humanognition but would rather rely on several different mechanismsSamson, 2009; Stone and Gerrans, 2006). More precisely, TOMould involve low bottom-up processes, also called “precursors”
i.e., face and emotion processing, eye gaze and body move-ent detection), in interaction with high top-down mechanisms
nvolved in meta-representational abilities and more cognitivelyemanding (i.e., executive functions, language, working memorynd episodic memory).
The question of an involvement of memory in mentalizingbility is raised, as many studies have not only shown correla-ions between episodic memory and TOM performances but alsovidenced that they would share a common pattern of brainctivity. This common cerebral network observed in fMRI foremembering and mentalizing indeed suggests common processesnd some authors put forward the hypothesis that these twoctivities would imply a mechanism referred to as self-projectionBuckner and Carroll, 2007; Spreng and Grady, 2010).
Research on TOM abilities in AD patients is restricted to eighttudies (Castelli et al., 2011; Cuerva et al., 2001; Fernandez-Duquet al., 2009; Gregory et al., 2002; Le Bouc et al., 2012; Verdon et al.,007; Zaitchik et al., 2006, 2004), and only one study was con-ucted in MCI individuals (Baglio et al., 2012). But, to date, theyave not provided enough evidence to clearly characterize TOMeficit and relate it or not to other cognitive disorders, especiallypisodic memory.
The aim of this paper is to review emergent evidence on TOMmpairment in AD patients and to discuss findings concerning theelationship between TOM and episodic memory. After reviewinghe results of the studies assessing TOM in AD and amnesic MCI,e will present data suggesting common processes supported by aeural substrate common to remembering and mentalizing. Then,e will discuss the issue of mentalizing deficits in AD patients
eing possibly related to their difficulties in recollecting memo-ies of past social interactions. This article is based on a MEDLINEurvey of the relevant literature published between 2001 and 2012.eyword searches were conducted using the following terms: (1)Alzheimer disease” or “mild cognitive impairment” and (2) “socialognition” or “theory of mind” or “mentalizing” or “mind read-ng” and (3) “autobiographical memory” or “episodic memory” orremembering”.
. TOM impairment in AD and amnesic MCI
The above-mentioned studies investigated TOM deficit in ADatients (Castelli et al., 2011; Cuerva et al., 2001; Fernandez-Duquet al., 2009; Gregory et al., 2002; Le Bouc et al., 2012; Verdon et al.,007; Zaitchik et al., 2006, 2004) and only one in amnesic MCI
ndividuals (Baglio et al., 2012). In AD, all these studies showed aeficit in high levels of TOM, even in the early stages of the disease.hey reported a significant decline in the performance on second-rder tasks, in which patients had to infer the mental state of aerson about another person (Castelli et al., 2011; Cuerva et al.,001; Fernandez-Duque et al., 2009; Gregory et al., 2002; Zaitchikt al., 2006). Similarly, patients were impaired on Faux-Pas tasks,hich require to detect that someone has done or said something
hat should not have been done or said in a particular situationGregory et al., 2002). They also had difficulties with Strange Storiesask (Happé, 1994) involving lies, double-bluffing or pretending, in
hich understanding the story depends on the character’s mentaltate (Castelli et al., 2011; Cuerva et al., 2001).The results are more contrasted concerning the tasks evaluat-
ng first-order TOM, in which patients had to infer someone else’s
Reviews 12 (2013) 833– 839
mental state, or in tasks assessing pragmatic abilities. Some studiesreported preserved first-order TOM abilities (Castelli et al., 2011;Fernandez-Duque et al., 2009; Gregory et al., 2002; Zaitchik et al.,2006, 2004) while one study showed impairment in AD patients onsuch tasks (Le Bouc et al., 2012). Moreover, some results demon-strated difficulties in eye gaze detection for AD patients (Castelliet al., 2011), attribution of an intention to a short comic strip char-acter or even in pragmatic abilities such as indirect requests orimplicit speech (Castelli et al., 2011; Cuerva et al., 2001). It wasalso demonstrated that AD patients had difficulties in perspectivetaking when they have to judge whether adjectives describe or nottheir personality, adopting theirs relatives’ point of view. In otherwords, they were impaired when they had to infer or imagine whattheir relatives could think about their personality trait (Ruby et al.,2009).
In the only work investigating TOM in amnesic MCI patients,results are similar to those found for AD patients. Participantsachieved worse performances on complex second-order taskcompared to healthy controls, while performances on StrangeStories task, eye gaze detection and first-order false belief taskswere similar to controls (Baglio et al., 2012). This suggests thatTOM impairment is already observed in patients with sparedgeneral cognitive functioning and whose deficits are more iso-lated than in AD. Unfortunately, in Baglio et al. (2012) TOMwas assessed only once whereas other functions where inves-tigated at baseline and 12–18 months later. Thus, despite thefollow-up in neuropsychological assessment, this study did notprovide any data about TOM deficit increasing as cognitive impair-ment worsens, especially in patients who had converted toAD.
Several authors hypothesized that mentalizing deficit in AD andMCI patients is secondary to other cognitive dysfunctions, espe-cially in executive and memory domains (Castelli et al., 2011;Cuerva et al., 2001; Fernandez-Duque et al., 2009; Zaitchik et al.,2004). However, findings on this issue differ. All the studies citedabove conducted neuropsychological evaluation in parallel to TOMassessment, except one in which patients just underwent MiniMental State Evaluation (MMSE) (Verdon et al., 2007). They allinvestigated executive functions such as abstraction, mental flexi-bility or inhibition. Nevertheless, the results did not provide enoughevidence of an executive involvement in TOM deficit. Indeed, somestudies showed correlations between impaired performances inone or several measures of executive functioning and TOM per-formances (Baglio et al., 2012; Castelli et al., 2011; Gregory et al.,2002; Le Bouc et al., 2012; Zaitchik et al., 2004), while another didnot find any correlation with executive tasks (Zaitchik et al., 2006).Concerning episodic memory, the central deficit in AD and amnesicMCI, only two studies reported positive correlations between mem-ory performances and TOM tasks (Castelli et al., 2011; Cuerva et al.,2001) whereas some did not find any correlation (Baglio et al.,2012; Fernandez-Duque et al., 2009). The remaining studies didnot explore memory function (Zaitchik et al., 2004), or did notconduct any correlation analyses between memory and TOM tasks(Gregory et al., 2002; Le Bouc et al., 2012; Zaitchik et al., 2006). Moreprecisely, Cuerva et al. (2001) compared their AD patients with“impaired TOM” to the AD patients with “preserved TOM”. Theyshowed that they differed only in their episodic and short-termmemory performances, assessed by Buschke Selective RemindingTest and digit span. This difference remained significant even aftercontrolling for general cognitive decline by matching MMSE scores.Castelli et al. (2011) showed various correlations between ver-bal and visual episodic memory measures and second-order false
belief tasks. These results only show correlations but they suggestthat performances on TOM and memory tasks may rely on com-mon mechanisms, which should be further explored using otherstatistical methods.
earch
tFteBfmtdcavatmwiic2bdwit2reocilttutdradmt
sEm2Rnt
3p
itR2aoawa
N. Moreau et al. / Ageing Res
Nevertheless, different methodological questions challengehese conclusions concerning TOM decline in AD and amnesic MCI.irst, some studies concerned restricted samples, sometimes of lesshan twenty patients (Baglio et al., 2012; Castelli et al., 2011; Cuervat al., 2001; Fernandez-Duque et al., 2009; Gregory et al., 2002; Leouc et al., 2012). Second, AD patients’ cognitive status is different
rom one study to another with considerable variations on MMSEeans and ranges. Variability at inclusion is a risk of misinterpre-
ation of the nature and extent of TOM deficit. Patients may haveifferent degrees of dementia and different cognitive deficits thatould explain variability on TOM performances. Moreover, in TOMssessment, tasks could be very complex. They usually consist inerbal stories which require efficient working or episodic memory,s well as efficient abstraction and meta-representational abilitieso realise inferences. They could generate a cognitive overload that
ight contribute to TOM deficit in AD. Indeed, given that patientsith AD show various impairments in several cognitive domains,
ncluding memory or executive functions (Weintraub et al., 2012),t may be difficult to tease out the respective roles of TOM andognitive impairment, as evaluated by these tasks (Apperly et al.,005; Bloom and German, 2000). To address this issue, it woulde necessary to design, in parallel to TOM conditions, control con-itions which do not require inferences about mental states buthich require inferences about physical conditions. Unfortunately,
n the studies reviewed above, control conditions were not sys-ematically proposed (Cuerva et al., 2001; Fernandez-Duque et al.,009; Le Bouc et al., 2012). When such a condition was designed,esults differ across studies. In Castelli et al. (2011) and Gregoryt al. (2002), AD patients performed as well as healthy subjectsn control conditions, whereas in Zaitchik et al. (2004, 2006) theontrol condition was failed by AD patients, even if task complex-ty was similar between TOM and control condition, in terms ofength and structures of the stories used. This control condition,hat did not imply mental state attribution, required participantso answer questions about pictorial representations, that is to say,nderstand that a picture can misrepresent reality and conflict withhe appearance of the current environment. This question of inci-ental TOM task demands, i.e., cognitive load associated to theesolution of mentalizing problems, must therefore be taken intoccount in assessing TOM decline in AD, and conclusions about thiseficit must be considered carefully. TOM should be assessed withore ecological materials, more adapted tasks, to better tease out
he role played by episodic memory impairment.Finally, in AD, the question of a decline in TOM capacity being
econdary to other cognitive dysfunctions remains to be answered.xecutive functions and TOM relationships were investigated inany studies with various populations (Aboulafia-Brakha et al.,
011) whereas episodic memory and TOM were less explored.ecent studies however showed that the latter shared a commoneuroanatomical substrate, suggesting a common mechanism forhese two activities.
. Memory and theory of mind: Common cognitiverocesses?
Recent studies supported that remembering the past and think-ng about others share a common brain network, suggesting thathey may rely on common processes (Buckner and Carroll, 2007;abin et al., 2010; Spreng and Grady, 2010; Spreng and Mar,012; Spreng et al., 2009). Episodic memory is dedicated to thecquisition, retention and retrieval of specific events in their phen-
menological context, which means spatial, temporal, emotionalnd perceptual information. More specifically, in this paragraph,e will focus on autobiographical memory (AM), which representssubsystem of episodic memory and is allocated to the storage
Reviews 12 (2013) 833– 839 835
of personal events. Remembering past personal memories impliesa mental time travel during which an individual consciously re-experiences previous events that happened in particular places andat particular times and associated with particular feelings, whichis also referred to autonoetic consciousness (Tulving, 2002, 1972).For some authors, this ability to mentally travel to other placesand times, also called self-projection, would constitute the processby which an individual can also imagine someone else’s inten-tions and feelings by projecting himself in “someone else’s shoes”(Buckner and Carroll, 2007; Cullen et al., 2011). This idea of self-projection represents the core process of the simulation theory ofTOM (Davies and Stone, 1998, 1995). This model states that weuse our own mental states to understand and predict others’ men-tal states. According to simulation theorists, to understand others’intentions or feelings, an individual must imagine what would behis own intentions and feelings and project them into someoneelse’s mind, putting himself “in the shoes” of that other person.Each individual therefore gets his own “tool” to understand other:his own mind, used as a model to simulate someone else’s mind(Gallese and Goldman, 1998). This idea of simulating or “mimick-ing” means that we may represent other’s minds from our ownmemories, and seems thus in favour of AM contribution to TOMfunctioning.
Moreover, understanding others supposes that we have to knowwhat kind of relationship we have with people to predict their reac-tions and intentions and so adapt our own behaviour. Behavingadequately towards a specific person in a specific situation meansthat we need to remember the past interactions we had together.Our behaviour is thus going to be different if we interact with awell-known person or with someone we do not know or have justmet once. For example, a communicative interaction with a per-son leads to the elaboration of a common ground of references, orshared knowledge, that will constitute a basis for future interac-tions (Clark, 1996; Jackendoff, 2002). In such a view, our attitudesand expectations towards a person would depend totally on thememories we have kept from our previous interactions, which helpus to understand the current interaction and anticipate their futurereactions and intentions.
Finally, TOM abilities would require memory, since pastevents would be necessary to understand current social scenarios(Corcoran and Frith, 2003). Accumulated memories of past inter-actions would indeed lead to the development of social scriptsand semantic constructs, which in turn guide our current socialbehaviour and help us to understand specific social situations(Spreng and Mar, 2012). In other words, TOM seems to rely onmemory since we have to remember which behaviour is usu-ally associated with specific thoughts, that is to say, rememberingepisodes in which particular behaviours were associated with spe-cific mental states.
Developmental evidence suggests a close emergence of men-talizing abilities and AM during childhood, at about the age offour (Perner, 2000; Perner et al., 2007; Saxe, 2007). Children withefficient TOM competences were shown to achieve better per-formances in tasks requiring re-experiencing an event (Perneret al., 2007). It was also demonstrated that children’s capacity tounderstand they had a false belief was related to their capacityto remember the source of their wrong knowledge (Naito, 2003).From these results, it was suggested that AM and TOM woulddevelop together, each contributing to the deployment of the other.Remembering would not just be recollection of past events butwould associate the reflection that past events are past events,known and personally experienced. Representing past events in
this way needs the capacity to think about one’s own mental states,that is to say, have a theory of one’s own mind (Perner, 2000;Saxe, 2007).This co-development of AM and TOM would in fact beunderpinned by the emergence of cognitive mechanisms such as
836 N. Moreau et al. / Ageing Research Reviews 12 (2013) 833– 839
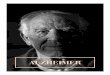
Fig. 1. (A) Autobiographical memory (light grey) and theory of mind (medium grey) cerebral networks. In dark grey are the regions activated by both activities (PCC andaMPFC). Adapted from Spreng and Grady (2010), Andrews-Hanna (2012). (B) AD histopathological stageing process from medial temporal lobe (1) to PCC, TPJ and mPFC (4).The gradual scales represent the proportion of neurofibrillary tangles in tissues. The first stage represented here corresponds to the condition of probable MCI and the lasts (1991a
ai2
amphhdrit(rrSbarseb
draTi(icjppo
tage represented corresponds to probable early AD. Adapted from Braak and Braaknd medial view of the right hemisphere.
utonoetic consciousness or source monitoring, i.e., the ability todentify the origins of one’s own knowledge and memories (Naito,003; Saxe, 2007).
AM and TOM were also related in behavioural studies in psychi-tric populations. In patients with schizophrenia, known to haveind reading impairment (Brune, 2005), one work showed a strong
ositive correlation between a hinting task, in which participantsad to infer the communicative intention of a character droppingints, and an AM task, in which they had to recollect events fromifferent periods of their lives (Corcoran and Frith, 2003). Theseesults were reproduced in a second study in which patients’ abil-ty to recall detailed and specific personal events was correlatedo their ability to infer intentions of characters in short moviesMehl et al., 2010). Corcoran and Frith (2003) suggested that theesolution of current social problems would depend on analogicaleasoning based on information issued from past social situations.imilar correlations were obtained in high-order autistic patients,etween an emotional inference task (Baron-Cohen et al., 2001) andn AM questionnaire (Adler et al., 2010). It is noteworthy that cor-elations were also shown in normal control participants in thesetudies, between the AM task and the Strange Stories task (Adlert al., 2010) and between the AM task and the second-order falseelief task (Mehl et al., 2010).
As mentioned earlier, recent functional imaging studies haveemonstrated the existence of a neuroanatomical overlap betweenemembering and mentalizing. Two meta-analyses, based on sep-rate group studies with participants performing either AM orOM tasks, showed that a common cerebral network was involvedn projecting oneself in past personal events or in other’s mindBuckner and Carroll, 2007; Spreng et al., 2009). This networkncluded the medial prefrontal cortex (mPFC), precuneus, posterioringulate (PCC), medial temporal lobe (MTL) and temporoparietal
unction (TPJ). Other fMRI studies directly compared same partici-ants performing both tasks, remembering a personal event fromhotographs or inferring the mental states of unknown personsn photographs (Rabin and Rosenbaum, 2012; Rabin et al., 2010;). Regional anatomic boundaries are approximate. The figure represents the lateral
Spreng and Grady, 2010). They confirmed the existence of a com-mon cerebral substrate activated during these two tasks includingmidline structures (i.e., mPFC, MTL, PCC, precuneus), and more lat-eralized regions (i.e., inferior frontal gyrus, the temporal poles andTPJ). PCC and mPFC were shown to be particularly activated duringboth tasks, while some regions seemed to be preferentially dedi-cated to AM or TOM (cf. Fig. 1; see also Andrews-Hanna, 2012).
These results reinforce the hypothesis of processes commonto remembering the past and inferring mental states, involvingspecific as well as common brain regions. It was argued that thiscerebral substrate may constitute a convergent zone “where infor-mation from autobiographical memory and mentalizing processesis synthesized and interact” (Spreng and Mar, 2012) and that pastexperiences may remain available, or “ready to use”, when we areengaged in social interactions.
The activation of this cerebral network common to AM andTOM seems however modulated according to the social situationsin which we are engaged. It was indeed shown that neural over-lap was stronger when participants had to infer mental states offamiliar persons on photographs or even when they had to ratethe intensity of an emotion associated to several events happen-ing to a fictional character sharing similarities with them (Perryet al., 2011; Rabin and Rosenbaum, 2012). More precisely, differentbrain patterns were involved during TOM tasks concerning familiarversus unfamiliar persons, suggesting different cognitive mech-anisms modulated by familiarity (Rabin and Rosenbaum, 2012).“Familiar” TOM involved in particular midline regions, as did theAM task, whereas “unfamiliar” TOM relied on more lateralizedregions, especially the temporal poles, usually involved in semanticmemory. These results show that inferring mental states of knownpersons would imply remembering specific past experiences, andso involves AM, whereas inferring unknown persons’ mental states
relies more on semantic social knowledge. The episodic and seman-tic aspects of memory seem therefore critical for TOM functioningbut their contribution would be modulated by familiarity, in sucha way that one would “dominate” according to the familiarity
earch
bsiis(cr
iblsawattopwowp
cacetorgtvtrotle(FsFiaoitc
4
eeoafddgee
N. Moreau et al. / Ageing Res
etween oneself and the target person. This dissociation betweenemantic or episodic memory involvements according to familiar-ty might explain why TOM was sometimes reported as preservedn amnesic individuals. Two patients with severe episodic amne-ia were indeed described with totally preserved TOM abilitiesRosenbaum et al., 2007) but in these observations, the TOM tasksoncerned unfamiliar persons and thus may involve other memoryesources, i.e., semantic knowledge, to solve TOM problems.
AM involvement in TOM may thus be modulated by the famil-arity we share with others, because we already know them orecause they share some similarity with us. Moreover, this modu-
ation would depend on the familiarity we have with the currentituation (Perry et al., 2011). Indeed, when participants had to judgen emotion felt by themselves or by “similar others” (i.e., peopleith personalities similar to theirs) in several scenarios, judgments
ppeared to be correlated between these two conditions only whenhe scenarios had already been experienced by the participants inhe past. This seems to indicate that we use past experiences ofur own thoughts and feelings to project them into the minds ofeople close to us in the current situation. In other words, whene think about others in specific situations, self-projection based
n AM will depend on how familiar we are with them, how similare feel to them and if we already experienced similar events in ourast (Perry et al., 2011; Rabin and Rosenbaum, 2012).
A lot of evidence reviewed here suggests that an efficient TOMapacity depends on the ability to remember past situations todapt our behaviour to the present social interaction. Memoryontribution may however be considered as larger than simple re-xperience of past events. Interactions we get with people lead tohe construction of specific representations and beliefs about eachne of them, which, in turn, help us to predict and understand theireactions. Beyond recollection therefore, past memories woulduide our behaviours, giving us clues about people we already meto understand current social interactions. Moreover, memory pro-ides us with semantic tools, or social scripts, to act adequatelyowards the people we meet. These social semantic constructs andules would be elaborated from accumulation and semantizationf specific social episodic memories. These social scripts would inurn help us to behave adequately and to tackle the social prob-ems in which we are engaged. This idea is further supported by thevidence of the activation of the temporal poles during TOM tasksfor reviews see Abu-Akel and Shamay-Tsoory, 2011; Gallagher andrith, 2003). They were shown to be related to knowledge aboutocial scenarios built on the basis of past experiences (Frith andrith, 2003; Ross and Olson, 2010), which is also in line with TOMmpairment reported in semantic dementia (Duval et al., 2012),
disease related to temporal pole degeneration. From this pointf view, the functional neuroanatomical network activated dur-ng remembering and mentalizing may finally be “critical for theransfer of information from experience to the formation of socialonceptual information” (Spreng and Mar, 2012).
. Discussion
As we reviewed in the previous section, recent studies in differ-nt domains highlighted that episodic memory, and more preciselypisodic AM, may be involved in TOM ability. This involvementf memory in TOM functioning raises the following questions: domnesic people have difficulties envisioning other minds? And aortiori, could the amnesic syndrome of AD account for their TOMeficits? Since AD patients suffer from primary episodic memory
isorders, we could indeed suppose that mentalizing abilities areoing to be impacted early in the disease. If TOM relies on thextraction of past memories, mentalizing deficit would thus appeararly in the pathological process. This is in fact what is suggested byReviews 12 (2013) 833– 839 837
the results described above in aMCI individuals which present TOMdeficits despite their spared general cognitive functioning (Baglioet al., 2012).These results suggest a precocious impairment of TOMin the AD pathological process, with a continuum between amnesicMCI individuals and AD patients.
In AD, it was demonstrated that patients present impaired TOMcapacity, and particularly on complex levels of mentalizing, usuallyassessed by second-order belief tasks. However, methodologicaldifferences, in terms of tasks used, number of patients included,or even their different cognitive status from one study to another,challenge conclusions regarding TOM decline and its relationshipswith other dysfunctions. In most studies, this deficit was describedas secondary to other cognitive disorders, but no clear conclusioncould be drawn as to whether they are independent or related,especially concerning episodic memory. Indeed, several studiesinvestigating TOM deficit in AD did not assess memory functionsystematically or did not conduct any statistical analyses betweenTOM and memory performances. In the few studies in which theseanalyses were done, correlations were observed between episodicmemory tasks and TOM deficit but additional statistical analysesare needed. No specific mechanism has been proposed to explainhow they are related to each other and the role that memory seemsto play in TOM impairment in AD patients.
To our knowledge, to date, no study has investigated morespecifically AM in relation with TOM difficulties in AD. Many studiesreported lower performances on AM tasks in AD patients comparedto healthy controls and particularly concerning the most recentperiod of life compared to remote memories (Donix et al., 2009;Irish et al., 2011; Leyhe et al., 2009; Meulenbroek et al., 2010).These difficulties in retrieving detailed memories were associatedwith an alteration of autonoetic consciousness, that is to say, anincapacity to relive episodes or to realise the mental time travelassociated with AM (Rauchs et al., 2007). In other words, even inthe early stages of the disease, patients present difficulties in pro-jecting themselves in the past, which, as a consequence, wouldbe associated with deficit to project in other’s mind, if we con-sider the self-projection hypothesis. This idea of a self-projectiondeficit is besides supported by the fact that AD patients were shownto present difficulties in simulating future personal events (Addiset al., 2009), that is to say, to project themselves in the future. Thus,if remembering and mentalizing rely on common processes, inves-tigating TOM deficit in relation with memory impairment appearstherefore relevant since amnesic patients would be “at-risk” todevelop mind reading incapacity.
One study could suggest such involvement of episodic mem-ory in TOM impairment in AD patients (Feyereisen et al., 2007).This work used a referential communication task, which is anecological paradigm assessing pragmatic skills. Champagne-Lavauet al. (2009) demonstrated that this referential communicationparadigm measured TOM ability as classical TOM tasks did but ina natural situation of conversation. In this paradigm, participantshave to describe a set of six tangrams (i.e., Chinese game) to a“blind” partner to help him reproduce the same order with his ownpictures. Through task repetition, healthy participants used moredefinite descriptions (the mountain), marking old, already knowninformation and less indefinite descriptions (a mountain) expectedto introduce new information. This reflects the construction of acommon ground between the two interlocutors. An increase incommunication efficiency is observed with a smaller number ofwords used. In Champagne-Lavau et al. (2009), this improvementof communication based on common references was observedwhatever the visual complexity of the tangrams used (very fig-
urative and easy to name or more abstract). This task relies onTOM processes since the participant must infer his interlocutor’sknowledge about the current interaction, that is to say, perform aninference about his mental state. On this task, AD patients did not
8 earch
bothtoribebHs
tsr2tetstaaiuooC
sa(e2wpm1hpgdtpweari
tpthmwiiuetne(
38 N. Moreau et al. / Ageing Res
enefit from repetition as they continued using the same numberf words or indefinite descriptions. Their decline in communica-ive effectiveness would in fact be explained by the difficulty theyave in taking into account their interlocutor’s knowledge, to usehe common ground they have built together in past interactions inrder to adapt their current speech (Feyereisen et al., 2007). Theseesults not only supported TOM deficit in AD but also supposed thenvolvement of episodic memory processes. Indeed, as suggestedy the authors, the re-use of definite markers and common refer-nces involves recollection of preceding exchanges, and thus coulde limited in AD patients because of their memory dysfunction.owever, this study did not explore memory function to confirm
uch hypothesis.From a neuroanatomical point of view, it was also demonstrated
hat AM and TOM activate a common cerebral network. This sub-trate was also involved in default mode network (DMN), whichefers to cerebral activity at rest (Buckner et al., 2008; Raichle et al.,001; Spreng and Grady, 2010; Spreng et al., 2009). It was suggestedhat DMN may support internalized simulation of different experi-nces and may finally correspond to the navigation of self in otherimes, in other places or in other persons’ minds. It would underlieelf-projection from current situations to alternative perspectives,hat is to say, remembering oneself in specific past situations ordopting other’s point of view (Buckner and Carroll, 2007; Sprengnd Grady, 2010). This projection into different perspectives maymply a mental elaboration based on internal-driven stimulus sim-lation, involving frontal structures for planning and constructionf different alternatives, as well as temporal regions for recollectionf specific past events related to the current situation (Buckner andarroll, 2007).
DMN was investigated in a large amount of functional imagerytudies in AD patients and MCI individuals. Early connectivitybnormalities in specific regions of DMN were widely reportedBai et al., 2012, 2009, 2008; Dickerson and Sperling, 2008; Gilit al., 2011; Greicius, 2004; Hafkemeijer et al., 2012; Petrella et al.,011), particularly in PCC, precuneus, hippocampus and mPFC,hich are key regions involved in TOM and AM functioning. Morerecisely, it was suggested that early histopathological changes inedial temporal lobe and hippocampus (cf. Fig. 1, Braak and Braak,
991) may underlie hypoconnectivity with PCC and may explainypometabolism in this region at the very early stage of AD. If DMNresents early dysfunctions in AD, this could, as a consequence, sug-est early deficits in AM and TOM (cf. Fig. 1). AM was shown to beisturbed in early AD, which could be hypothesized as secondaryo early dysfunctions in key cerebral regions. In the same way, arecocious mentalizing impairment could be expected since TOMould rely on DMN cerebral regions whose dysfunction has been
vidence in AD. The hypothesis of a parallel decline between AMnd TOM in AD appears relevant and must be considered further, inelation with functional neuroanatomical abnormalities observedn early stages.
To conclude, despite the small number of studies on that ques-ion, it was shown that AD patients are impaired on complex TOMrocesses whereas the question of a deficit on first-order TOMasks is still under debate. We reviewed evidence suggesting theypothesis of common processes between episodic memory, andore precisely episodic AM, and TOM, in such a way that memoryould support mental state attribution, providing precious tools
n various social situations to understand people with whom onenteracts. This hypothesis is particularly relevant in the AD pop-lation. AD patients’ TOM deficit could indeed be related to theirpisodic memory impairment, which constitutes the first step of
his disease. However, this hypothesis remains to be verified, sinceo study has proposed to consider TOM deficit in AD in relation topisodic AM impairment as a possible inability of self-projectionBuckner and Carroll, 2007). Therefore, future research shouldReviews 12 (2013) 833– 839
investigate TOM with adapted tasks (i.e., tasks having restrictedmemory charge, such as living interactions) to better tease out therole of memory dysfunction observed in AD. It would also be a greatoption to assess TOM in amnesic MCI condition, in which deficitis isolated on memory function. The results of such research willallow us to better characterize the cognitive mechanism specificallyinvolved in TOM impairment in AD.
Acknowledgements
We would like to express our sincere gratitude to LaurentMartinez-Almoyna and Laurent Renie for their help with themanuscript and their helpful comments. This work was supportedby the Agence Nationale de la Recherche (ANR-11-BSH2-006-01MINDPROGEST).
References
Aboulafia-Brakha, T., Christe, B., Martory, M.-D., Annoni, J.-M., 2011. Theory of mindtasks and executive functions: a systematic review of group studies in neurology.Journal of Neuropsychology 5, 39–55.
Abu-Akel, A., Shamay-Tsoory, S., 2011. Neuroanatomical and neurochemical basesof theory of mind. Neuropsychologia 49, 2971–2984.
Addis, D.R., Sacchetti, D.C., Ally, B.A., Budson, A.E., Schacter, D.L., 2009. Episodicsimulation of future events is impaired in mild Alzheimer’s disease. Neuropsy-chologia 47, 2660–2671.
Adenzato, M., Cavallo, M., Enrici, I., 2010. Theory of mind ability in the behaviouralvariant of frontotemporal dementia: an analysis of the neural, cognitive, andsocial levels. Neuropsychologia 48, 2–12.
Adler, N., Nadler, B., Eviatar, Z., Shamay-Tsoory, S.G., 2010. The relationship betweentheory of mind and autobiographical memory in high-functioning autism andAsperger syndrome. Psychiatry Research 178, 214–216.
Adolphs, R., 2006. How do we know the minds of others? Domain-specificity, sim-ulation, and enactive social cognition. Brain Research 1079, 25–35.
Albert, M.S., DeKosky, S.T., Dickson, D., Dubois, B., Feldman, H.H., Fox, N.C.,Gamst, A., Holtzman, D.M., Jagust, W.J., Petersen, R.C., Snyder, P.J., Carrillo,M.C., Thies, B., Phelps, C.H., 2011. The diagnosis of mild cognitive impair-ment due to Alzheimer’s disease: recommendations from the National Instituteon Aging–Alzheimer’s Association workgroups on diagnostic guidelines forAlzheimer’s disease. Alzheimers Dement 7, 270–279.
American Psychiatric Association, 2013. Diagnostic and statistical manual of mentaldisorders, (5th ed). Author, Washington, DC.
Andrews-Hanna, J.R., 2012. The brain’s default network and its adaptive role ininternal mentation. Neuroscientist.
Apperly, I.A., Samson, D., Humphreys, G.W., 2005. Domain-specificity and theory ofmind: evaluating neuropsychological evidence. Trends in Cognitive Sciences 9,572–577.
Baglio, F., Castelli, I., Alberoni, M., Blasi, V., Griffanti, L., Falini, A., Nemni, R., Marchetti,A., 2012. Theory of mind in amnestic mild cognitive impairment: an fMRI study.Journal of Alzheimer’s Disease 29, 25–37.
Bai, F., Shi, Y., Yuan, Y., Wang, Y., Yue, C., Teng, Y., Wu, D., Zhang, Z., Jia, J., Zhang,Z., 2012. Altered self-referential network in resting-state amnestic type mildcognitive impairment. Cortex 48, 604–613.
Bai, F., Watson, D.R., Yu, H., Shi, Y., Yuan, Y., Zhang, Z., 2009. Abnormal resting-state functional connectivity of posterior cingulate cortex in amnestic type mildcognitive impairment. Brain Research 1302, 167–174.
Bai, F., Zhang, Z., Yu, H., Shi, Y., Yuan, Y., Zhu, W., Zhang, X., Qian, Y., 2008. Default-mode network activity distinguishes amnestic type mild cognitive impairmentfrom healthy aging: a combined structural and resting-state functional MRIstudy. Neuroscience Letters 438, 111–115.
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., Plumb, I., 2001. The reading themind in the eyes test revised version: a study with normal adults, and adults withAsperger syndrome or high-functioning autism. Journal of Child Psychology andPsychiatry 42, 241–251.
Bertoux, M., Delavest, M., De Souza, L.C., Funkiewiez, A., Lépine, J.-P., Fossati, P.,Dubois, B., Sarazin, M., 2012. Social cognition and emotional assessment dif-ferentiates frontotemporal dementia from depression. Journal of Neurology,Neurosurgery, and Psychiatry.
Bloom, P., German, T.P., 2000. Two reasons to abandon the false belief task as a testof theory of mind. Cognition 77, B25–B31.
Braak, H., Braak, E., 1991. Neuropathological staging of Alzheimer-related changes.Acta Neuropathologica 82, 239–259.
Brune, M., 2005. Theory of mind in Schizophrenia: a review of the literature.Schizophrenia Bulletin 31, 21–42.
Buckner, R.L., Andrews-Hanna, J.R., Schacter, D.L., 2008. The brain’s default network:anatomy, function, and relevance to disease. Annals of the New York Academyof Sciences 1124, 1–38.
Buckner, R.L., Carroll, D.C., 2007. Self-projection and the brain. Trends in CognitiveSciences (Regul. Ed.) 11, 49–57.

earch
C
C
CC
C
C
DD
D
D
D
F
F
F
G
G
G
G
G
H
H
I
J
L
L
L
L
M
M
N. Moreau et al. / Ageing Res
astelli, I., Pini, A., Alberoni, M., Liverta-Sempio, O., Baglio, F., Massaro, D., Marchetti,A., Nemni, R., 2011. Mapping levels of theory of mind in Alzheimer’s disease: apreliminary study. Aging & Mental Health 15, 157–168.
hampagne-Lavau, M., Fossard, M., Martel, G., Chapdelaine, C., Blouin, G., Rodriguez,J.-P., Stip, E., 2009. Do patients with schizophrenia attribute mental states in areferential communication task? Cognitive Neuropsychiatry 14, 217–239.
lark, H.H., 1996. Using Language. Cambridge University press, New York.orcoran, R., Frith, C.D., 2003. Autobiographical memory and theory of mind: evi-
dence of a relationship in schizophrenia. Psychological Medicine 33, 897–905.uerva, A.G., Sabe, L., Kuzis, G., Tiberti, C., Dorrego, F., Starkstein, S.E., 2001. Theory of
mind and pragmatic abilities in dementia. Neuropsyehiatry, Neuropsychology,and Behavioral Neurology 14, 153–158.
ullen, J., Buda, M., Darby, G., Simons, J.S., 2011. Time-travelling and mind-travelling:examining individual differences in self-projection. Psychiatria Danubina 23(Suppl 1), S182–S186.
avies, M., Stone, T., 1995. Folk Psychology. Blackwell.avies, M., Stone, T., 1998. Folk psychology and mental simulation. Royal Institute
of Philosophy Supplement 43, 53–82.ickerson, B.C., Sperling, R.A., 2008. Functional abnormalities of the medial temporal
lobe memory system in mild cognitive impairment and Alzheimer’s disease:insights from functional MRI studies. Neuropsychologia 46, 1624–1635.
onix, M., Brons, C., Jurjanz, L., Poettrich, K., Winiecki, P., Holthoff, V.A., 2009. Overgenerality of autobiographical memory in people with amnestic mild cognitiveimpairment and early Alzheimer’s disease. Archives of Clinical Neuropsychology25, 22–27.
uval, C., Bejanin, A., Piolino, P., Laisney, M., De La Sayette, V., Belliard, S., Eustache,F., Desgranges, B., 2012. Theory of mind impairments in patients with semanticdementia. Brain 135, 228–241.
ernandez-Duque, D., Baird, J.A., Black, S.E., 2009. False-belief understanding infrontotemporal dementia and Alzheimer’s disease. Journal of Clinical and Exper-imental Neuropsychology 31, 489–497.
eyereisen, P., Berrewaerts, J., Hupet, M., 2007. Pragmatic skills in the early stages ofAlzheimer’s disease: an analysis by means of a referential communication task.International Journal of Language & Communication Disorders 42, 1–17.
rith, U., Frith, C.D., 2003. Development and neurophysiology of mentalizing. Philo-sophical Transactions of the Royal Society of London, Series B: Biological Sciences358, 459–473.
allagher, H.L., Frith, C.D., 2003. Functional imaging of theory of mind. Trends inCognitive Sciences (Regul. Ed.) 7, 77–83.
allese, V., Goldman, A., 1998. Mirror neurons and the simulation theory of mind-reading. Trends in Cognitive Sciences (Regul. Ed.) 2, 493–501.
ili, T., Cercignani, M., Serra, L., Perri, R., Giove, F., Maraviglia, B., Caltagirone, C.,Bozzali, M., 2011. Regional brain atrophy and functional disconnection acrossAlzheimer’s disease evolution. Journal of Neurology, Neurosurgery, and Psychi-atry 82, 58–66.
regory, C., Lough, S., Stone, V., Erzinclioglu, S., Martin, L., Baron-Cohen, S., Hodges,J.R., 2002. Theory of mind in patients with frontal variant frontotemporal demen-tia and Alzheimer’s disease: theoretical and practical implications. Brain 125,752–764.
reicius, M.D., 2004. Default-mode network activity distinguishes Alzheimer’s dis-ease from healthy aging: evidence from functional MRI. Proceedings of theNational Academy of Sciences of the United States of America 101, 4637–4642.
afkemeijer, A., Van der Grond, J., Rombouts, S.A.R.B., 2012. Imaging the defaultmode network in aging and dementia. Biochimica et Biophysica Acta 1822,431–441.
appé, F.G., 1994. An advanced test of theory of mind: understanding of storycharacters’ thoughts and feelings by able autistic, mentally handicapped, andnormal children and adults. Journal of Autism and Developmental Disorders 24,129–154.
rish, M., Lawlor, B.A., O’Mara, S.M., Coen, R.F., 2011. Impaired capacity for autonoeticreliving during autobiographical event recall in mild Alzheimer’s disease. Cortex47, 236–249.
ackendoff, R., 2002. Foundations of language. In: Brain, Meaning, Grammar, Evolu-tion. Oxford University Press, New York.
e Bouc, R., Lenfant, P., Delbeuck, X., Ravasi, L., Lebert, F., Semah, F., Pasquier, F.,2012. My belief or yours? Differential theory of mind deficits in frontotemporaldementia and Alzheimer’s disease. Brain 135, 3026–3038.
eyhe, T., Müller, S., Milian, M., Eschweiler, G.W., Saur, R., 2009. Impairment ofepisodic and semantic autobiographical memory in patients with mild cognitiveimpairment and early Alzheimer’s disease. Neuropsychologia 47, 2464–2469.
ough, S., Gregory, C., Hodges, J.R., 2001. Dissociation of social cognition and execu-tive function in frontal variant frontotemporal dementia. Neurocase 7, 123–130.
ough, S., Kipps, C.M., Treise, C., Watson, P., Blair, J.R., Hodges, J.R., 2006. Social rea-soning, emotion and empathy in frontotemporal dementia. Neuropsychologia44, 950–958.
cKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., Stadlan, E.M., 1984.
Clinical diagnosis of Alzheimer’s disease report of the NINCDS—ADRDA WorkGroup* under the auspices of Department of Health and Human Services TaskForce on Alzheimer’s disease. Neurology 34, 939-939.cKhann, G.M., Knopman, D.S., Chertkow, H., Hyman, B.T., Jack, C.R., Kawas, C.H.,Klunk, W.E., Koroshetz, W.J., Manly, J.J., Mayeux, R., Mohs, R.C., Morris, J.C.,
Reviews 12 (2013) 833– 839 839
Rossor, M.N., Scheltens, P., Carrillo, M.C., Thies, B., Weintraub, S., Phelps, C.H.,2011. The diagnosis of dementia due to Alzheimer’s disease: recommenda-tions from the National Institute on Aging–Alzheimer’s Association workgroupson diagnostic guidelines for Alzheimer’s disease. Alzheimer’s and Dementia 7,263–269.
Mehl, S., Rief, W., Mink, K., Lüllmann, E., Lincoln, T.M., 2010. Social performanceis more closely associated with theory of mind and autobiographical mem-ory than with psychopathological symptoms in clinically stable patients withschizophrenia-spectrum disorders. Psychiatry Research 178, 276–283.
Meulenbroek, O., Rijpkema, M., Kessels, R.P.C., Rikkert, M.G.M.O., Fernández, G.,2010. Autobiographical memory retrieval in patients with Alzheimer’s disease.NeuroImage 53, 331–340.
Naito, M., 2003. The relationship between theory of mind and episodic memory: evi-dence for the development of autonoetic consciousness. Journal of ExperimentalChild Psychology 85, 312–336.
Perner, J., 2000. Memory and theory of mind. In: The Oxford Handbook of Memory.New York., pp. 297–312.
Perner, J., Kloo, D., Gornik, E., 2007. Episodic memory development: theory of mindis part of re-experiencing experienced events. Infant and Child Development 16,471–490.
Perry, D., Hendler, T., Shamay-Tsoory, S.G., 2011. Projecting memories: the role ofthe hippocampus in emotional mentalizing. Neuroimage 54, 1669–1676.
Petersen, R.C., 2004. Mild cognitive impairment as a diagnostic entity. Journal ofGeneral Internal Medicine 256, 183–194.
Petrella, J.R., Sheldon, F.C., Prince, S.E., Calhoun, V.D., Doraiswamy, P.M., 2011. Defaultmode network connectivity in stable vs progressive mild cognitive impairment.Neurology 76, 511–517.
Premack, D., Woodruff, G., 1978. Does the chimpanzee have a theory of mind?Behavioral and Brain Sciences 4, 515–526.
Rabin, J.S., Gilboa, A., Stuss, D.T., Mar, R.A., Rosenbaum, R.S., 2010. Common andunique neural correlates of autobiographical memory and theory of mind. Jour-nal of Cognitive Neuroscience 22, 1095–1111.
Rabin, J.S., Rosenbaum, R.S., 2012. Familiarity modulates the functional relation-ship between theory of mind and autobiographical memory. NeuroImage 62,520–529.
Raichle, M.E., MacLeod, A.M., Snyder, A.Z., Powers, W.J., Gusnard, D.A., Shulman, G.L.,2001. A default mode of brain function. Proceedings of the National Academy ofSciences of the United States of America 98, 676–682.
Rauchs, G., Piolino, P., Mézenge, F., Landeau, B., Lalevée, C., Pélerin, A., Viader, F.,De la Sayette, V., Eustache, F., Desgranges, B., 2007. Autonoetic consciousnessin Alzheimer’s disease: neuropsychological and PET findings using an episodiclearning and recognition task. Neurobiology of Aging 28, 1410–1420.
Rosenbaum, R.S., Stuss, D.T., Levine, B., Tulving, E., 2007. Theory of mind is indepen-dent of episodic memory. Science 318, 1257.
Ross, L.A., Olson, I.R., 2010. Social cognition and the anterior temporal lobes. Neu-roImage 49, 3452–3462.
Ruby, P., Collette, F., D’Argembeau, A., Péters, F., Degueldre, C., Balteau, E., Luxen,A., Maquet, P., Salmon, E., 2009. Perspective taking to assess self-personality:what’s modified in Alzheimer’s disease? Neurobiology of Aging 30, 1637–1651.
Samson, D., 2009. Reading other people’s mind: insights from neuropsychology.Journal of Neuropsychology 3, 3–16.
Saxe, R., 2007. What was I thinking? Developmental and neural connections betweentheory of mind, memory and the self. In: Haggard, P., Rossetti, Y., Kawato, M.(Eds.), Attention and Performance, XXII. Oxford University Press, New-York, pp.619–636.
Spreng, R.N., Grady, C.L., 2010. Patterns of brain activity supporting autobiographicalmemory, prospection, and theory of mind, and their relationship to the defaultmode network. Journal of Cognitive Neuroscience 22, 1112–1123.
Spreng, R.N., Mar, R.A., 2012. I remember you: a role for memory in social cogni-tion and the functional neuroanatomy of their interaction. Brain Research 1428,43–50.
Spreng, R.N., Mar, R.A., Kim, A.S.N., 2009. The common neural basis of autobiograph-ical memory, prospection, navigation, theory of mind, and the default mode: aquantitative meta-analysis. Journal of Cognitive Neuroscience 21, 489–510.
Stone, V.E., Gerrans, P., 2006. What’s domain-specific about theory of mind? Societyfor Neuroscience 1, 309–319.
Tulving, E., 1972. Episodic and Semantic Memory. Organization of Memory, New-York, pp. 381–402.
Tulving, E., 2002. Episodic memory: from mind to brain. Annual Review of Psychol-ogy 53, 1–25.
Verdon, C.-M., Fossati, P., Verny, M., Dieudonné, B., Teillet, L., Nadel, J., 2007. Socialcognition: an early impairment in dementia of the Alzheimer type. AlzheimerDisease and Associated Disorders 21, 25–30.
Weintraub, S., Wicklund, A.H., Salmon, D.P., 2012. The neuropsychological profile ofAlzheimer disease. Cold Spring Harbor Perspectives in Medicine 2, a006171.
Zaitchik, D., Koff, E., Brownell, H., Winner, E., Albert, M., 2004. Inference of men-
tal states in patients with Alzheimer’s disease. Cognitive Neuropsychiatry 9,301–313.Zaitchik, D., Koff, E., Brownell, H., Winner, E., Albert, M., 2006. Inference ofbeliefs and emotions in patients with Alzheimer’s disease. Neuropsychology 20,11–20.