Embed Size (px)
Citation preview

Use of CRRT in ECMO: Is It Valuable?
James D. Fortenberry MD, FCCM, FAAPAssociate Professor of Pediatrics
Emory University School of MedicineDirector, Critical Care Medicine and
Pediatric ECMO/Advanced TechnologiesChildren’s Healthcare of Atlanta at Egleston

2
CRRT and ECMO
What are potential benefits? What is the experience? How do you do it? What are the risks? What more do we need to know?

3
CRRT on ECMO: Potential Benefits
Management of fluid balanceDecreasing fluid overloadRemoval of inflammatory mediatorsEnhanced nutritional supportControl of electrolyte abnormalitiesDecreased use of furosemide

4
Is Fluid Overload Bad?
Remember: fluid is good in resuscitation!
Early goal directed therapy outcome benefits
However, multiple studies (adults, pediatric) suggest survival benefit with decreased fluid overload in critical illness

5
Fluid Overload
Texas Children’s Hospital
21 pediatric ARF patients
Survival benefit remains even after adjusted for PRISM scores
0
5
10
15
20
25
30
35
Survivors Non-Survivors
Goldstein SL, et al: Pediatrics 107:1309-1312, 2001
Per
cen
t F
luid
Ove
rloa
d
*

6
Fluid Overload
Children’s Healthcare of Atlanta at Egleston
113 pediatric patients on CVVH
Multivariate analysis • Percent fluid overload
independently associated with survival in ≥ 3 organ MODS
0
2
4
6
8
10
12
14
16
Survivors Non-Survivors
-Foland JA, Fortenberry et al. Crit Care Med, 2004
*
Per
cen
t F
luid
Ove
rloa
d

7
Fluid Overload Decreased in 3 Organ MODS CRRT Survivors
-Foland JA et al. Crit Care Med, 2004

8
Fluid Overload and ECMO: Neonates
As weight gain decreases, ECMO flow decreases which comes first?
• As weight reduces, ECMO flow reduces
-Kelley RE, et al. J Pediatr Surg, 1991
111 cc/kg
97 cc/kg
73 cc/kg
30 cc/kg
9.1%
3.8%
2.0%
5.4%
0
20
40
60
80
100
120
25% 50% 75% 100%
Duration of ECMO
EC
MO
Flo
w (
cc
/kg
)
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
We
igh
t G
ain
(p
erc
en
t)

9
Fluid Overload and Outcome
Seattle Children’s Hospital 77 pediatric patients
• If pre-CRRT percent fluid overload >10% 3.02 times greater risk of mortality (95% CI 1.5-6.1,
p=0.002)
Gillespie RS, et al. Pediatr Nephrol 19:1394-1399, 2004

10
Fluid Overload/Oliguria is Common on ECMO
Children's Healthcare of Atlanta 30 consecutive neonates meeting ECMO
criteria – • 18 VV ECMO, 12 conventional management• Patients who went onto ECMO had:
Greater fluid overload Lower UOP Higher BUN Higher creatinine
-Roy BJ, Pediatrics 1995

11
ECMO and Urine Output
-Roy BJ, Pediatrics 1995

12
Blood
Black BileYellow Bile
Phlegm
Requisite Bad Humour Slide

13
Good Humours

CRRT/Plasma Exchange
CRRT/Plasma Exchange
Time
Time
SI RS/CARS
SI RS CARS SI RS CARS
I mmunohomeostasis
I mmunohomeostasis
Pro-inflammatoryMediators
Anti-inflammatoryMediators
IL-1TNF PAF
IL-10
Adapted f rom Ronco et al. Artificial Organs 27(9) 792-801, 2003

15
Hemofiltration Cytokine Clearance
Children’s Healthcare of Atlanta at Egleston 6 pediatric patients with culture proven
bacterial septic shock and ARF• 2 on ECMO
Compared to 3 ARF patients without septic shock• 1 on ECMO
-Paden M et al., submitted 2008

16
Absolute cytokine changes in septic shock/ARF patients
1
10
100
1000
10000
100000
IL-6 IL-10
Pre-CVVHEnd ofCVVH
Lo
g C
on
cen
trat
ion
(p
g/m
l)
p<0.02* p=0.04*
-Paden et al., submitted 2008

17
CVVH Associated With Decreased Cytokines in Children with Septic Shock
Cytokine Levels at the End of CVVH
-100
-80
-60
-40
-20
0
20
% D
ecre
ase
From
Bas
elin
e
IL-6
IL-8
IL-10
Septic ARF Patients Non-septic ARF Patients
*p<0.05
* *
-Paden et al., submitted 2008

18
Cytokine Results: Sample CVVH Patient-Nonseptic
Non-septic ARF Patient #3
0
10
20
30
40
50
60
70
80
90
Co
nc
en
tra
tio
n (
pg
/ml)
Human IL-10
Human IL-6
Human IL-8
Pre
-CV
VH
12 H
ours
24 H
ours
48 H
ours
En
d o
f C
VV
H
24 H
ours
off
C
VV
H
Note Scale

19
Cytokine Results in Sample CVVH Patient: Septic
Septic ARF Patient #5
0
200
400
600
800
1000
1200
1400
1600
1800
2000C
on
cen
trat
ion
(p
g/m
l)
Human IL-10
Human IL-6
Human IL-8
Pre
-CV
VH
12 H
ours
24 H
ours
48 H
ours
En
d o
f C
VV
H
24 H
ours
off
C
VV
H

20
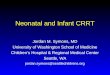
ECMO/CVVH Produces Cytokine Reduction
In vitro study –
• Increased cytokine levels overall due to ECMO membrane activation
• Adding a hemofiltration circuit significantly reduced : IL-1beta IL-1ra IL-6 IL-8
-Skogby M, et al. Scand Cardiovasc J. 2000

21 Skogby M, et al. Scand Cardiovasc J. 2000 Jun;34(3):315-20
IL – 8 Reduction with CRRT in ECMO

22
Is Avoiding Lasix Overuse Important?
Potential ototoxicity-particularly in neonates
Lasix use associated with worsened outcomes in adult renal failure

23
Diuretics and Critical Illness
4 University of California Hospitals 552 adults Use of diuretics increased risk of death or
renal non-recovery in adults with ARF• Overall 1.77 times greater risk
-Mehta RL, et al. JAMA 2002

24
CRRT and ECMO
What are potential benefits? What is the experience? How do you do it? What are the risks? What more do we need to know?

25
CRRT on ECMO: Published Experience with Use
Michigan• PICU• Cardiac surgery
Vanderbilt Atlanta Chile

26
CRRT/ECMO Experience: Michigan
U of M ECMO Database 35 neonatal and pediatric patients who
received ECMO + hemofiltration• 15 Survivors
Renal recovery in 14 of 15 (93%) survivors• One had Wegener’s as underlying cause of
renal failure-subsequently transplanted
-Meyer RJ, et al Pediatr Crit Care Med 2001

27
CRRT/ECMO Experience: Cardiac Surgery
University of Michigan 74 post-operative congenital heart disease
patients• Use of hemofiltration in 35%
5.01 times increased risk of death Use of hemofiltration indicative of longer
ECMO support time worse outcome was from duration, not hemofiltration
-Kolovos et al. Ann Thorac Surg 2003

28
CRRT/ECMO Experience: Cardiac Surgery
Vanderbilt University 84 post-operative congenital heart disease
patients• Temporary renal insufficiency in 41 patients
(48.9%)
CVVH NOT associated with :• Ability to wean off ECMO• Survival to discharge
-Shah SA et al. ASAIO J 2005

29
ECMO/CVVH Experience: Atlanta
Children’s at Egleston ECMO Database (11/97-12/05)
95 neonatal and pediatric patients who received ECMO + CVVH• 55 survivors• 14 came off ECMO on RRT (1 on prior to ECMO)• 1 needed RRT chronically• 1 with CRF but does not need RRT
Renal recovery in 53/55 (96%) survivors• Both CRF patients had primary vasculitis
-Paden et al., CCM 2007 (abstr)

30
Comparison of CVVH/ECMO vs. ECMO without CVVH
26/86 peds respiratory failure patients received CVVH for >24 hours
Case control comparison: 26 CVVH/ECMO pts. and 26 pts. receiving ECMO without CVVH
No difference in survival or vent days during or after ECMO
Significant differences in fluid balance Significant treatment differences
-Hoover et al., Intensive Care Medicine, in press 2008

31
Fluid Balance With CVVH/ECMO vs. No CVVH/ECMO
Flu
id B
alan
ce (
cc/k
g/d
ay)
-50
0
50
100
150 ECMO/non-CVVHECMO/CVVH ECMO/CVVH -CVVH days only
All Patients Survivors
* **
#
-Hoover et al., Intensive Care Medicine, in press 2008

32
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Lasixuse
Days todesiredcalories
CVVH/ECMO
ECMO alone
Comparison of CVVH/ECMO vs. ECMO without CVVH
-Hoover et al., Intensive Care Medicine, in press 2008
** *

33
CRRT/ECMO Experience in Infants: Chile
6 of 12 infants on ECMO received CRRT Observed complication: excessive
ultrafiltration Survival to discharge in 5 of 6 (83%) All with normal renal function at discharge
-Cavagnaro et al., Int J Artif Organs 2007

34
CRRT and ECMO
What are potential benefits? What is the experience? How do you do it? What are the risks? What more do we need to know?

35
CRRT on ECMO: How to Perform It
Options:• Parallel use of stand-alone CRRT devices
(Gambro, Braun) Pros Cons
• Use of inline hemofilter with syringe pumps Pros Cons

ECMO/CRRT Arrangement: The “Michigan Method”

37
Use of Standard CRRT Devices for Delivery on ECMO

38
CRRT and ECMO
What are potential benefits? What is the experience? How do you do it? What are the risks? What more do we need to know?

39
CVVH/ECMO: Are There Risks?
Complexity of machineryErrors due to replacement fluidsUnderestimation of fluid removal

40
Sometimes it gets a little crowded

41
CRRT Error Rate Increases with Increasing Flow/Pressure
-Sucosky, Paden et al., JMD, in press 2008

42
Error Rate in CRRT/ECMO Circuits
Potential error rate noted in stand-alone CVVH Ex vivo ECMO circuit Compared measured versus actual fluid removal
rates with inline hemofilter arrangement and with Braun Diapact for CVVH
Significant excess fluid removal over “expected” both for inline device and commercial device
-Paden et al., ppCRRT Conference 2008 (abstr)

43
Potential Solutions
Collaboration with GeorgiaTech
Paden, Sucosky Development of
fluid management/CRRT device
High accuracy in delivery
Patent pending

44
What Further Work Needs to be done?
Improved control of fluid management Randomized trial to compare CVVH/ECMO
to ECMO without routine CVVH Potential use of biomarkers for initiation?

45
Conclusions
CRRT on ECMO can potentially provide a variety of benefits
CRRT can be provided• without worsening renal insufficiency• with improved fluid balance• with decreased furosemide exposure
Potential risks of excessive fluid removal Further work to improve accuracy of fluid balance
and to determine if use translates into outcome benefit

46
MODS & 3 Organ Involvement
Effect SE OR 95% CI p
PRISM III 0.049 0.058 1.10 0.88, 1.39 0.4
% FO 0.058 0.023 1.78 1.13, 2.82 0.01
Pediatric Patients Receiving CVVH
Factors Associated with Mortality
- Foland, Fortenberry et al., CCM 2004

Pro-I nflammatoryMediators
Anti-I nflammatoryMediators (I nhibitors)
Pro/ Anti-I nflammatoryMediators
Activation Depression
Time
Time
Parallel
Serial
IL1TNF
PAF
IL10
IL6
Med
iato
r Le
vels
Med
iato
r Le
vels
Adapted f rom Ronco et al. Artifi cial Organs 27(9) 792-801, 2003