-
7/31/2019 Us Urinary System and Prostate
1/8
Ultrasound of the Urinary System
and ProstateAlain Giroux, DVM, MSc, DACVR
Introduction
Ultrasound is an excellent imaging modality to evaluate the
urinary tract. With ultrasonographicexamination the entire urinary
tract can be evaluated at one time and usually without the aid of
anesthesia.
The kidneys can be imaged using a 5.0-megahertz transducer;
however, for small dogs and cats, a 7.5-megahertz transducer is
ideal.
Normal Renal Anatomy
The kidneys are located in the retroperitoneal space, usually
between the caudal thoracic and 3rd lumbar
vertebrae. The kidneys are bean-shaped and are composed of the
renal capsule, renal cortex, renal medullaand the diverticuli. The
renal pelvis is located in the central portion of the kidneys and
is usually
surrounded by renal fat (Fig. 1K and Fig. 2K). Renal arteries
and veins can be identified at the hilus of the
kidneys. The ureter leaves the renal pelvis through the hilus of
the kidney. The normal ureter is not
usually identified ultrasonographically.
The left kidney is located caudal to the fundus of the stomach
and medial to the spleen. The right kidney is
caudal to the liver and is located in the renal fossa of the
caudate lobe of the liver. The right kidney is
further cranial than the left kidney, which makes visualizing
the right kidney more difficult.
The size of the kidneys varies depending on the size of the dog.
A normal canine kidney can vary from 4 to
9 cm in length and feline kidneys are usually 3.8 to 4.4 cm in
length.
1
Figure 1K: Kidney Anatomy Figure 2K: Kidney Anatomy at the
Pelvis
-
7/31/2019 Us Urinary System and Prostate
2/8
2
-
7/31/2019 Us Urinary System and Prostate
3/8
Ultrasonographic Renal Anatomy
The capsule of the kidney is a hyperechoic structure which is
identified surrounding the kidney. The renal
cortex is hyperechoic in relation to the medulla. There is good
distinction between the renal cortex and
renal medulla in the normal kidney (Fig. 3Ka,b and Fig. 4K). The
renal sinus (Fig.4K) usually contains fat
which can be seen as bright echoes and in some cases can result
in acoustic shadowing. The medulla of the
kidney is separated into sections by the diverticuli. The renal
cortex of the kidneys is usually lessechogenic than the spleen but
more echogenic than the renal medulla. The renal cortex can be
isoechoic tohypoechoic in relationship to the liver.
The renal artery and vein can usually be visualized entering the
kidney at the renal sinus. Renal vessels can
be recognized in the medulla. The arcuate and interlobar
arteries can sometimes be visualized at the
cortical medullary junction.
When evaluating the kidneys ultrasonographically, the patient is
usuallyplaced in dorsal recumbency. Thekidneys should be scanned in
both sagittal and transverse planes. The appearance of the renal
cortex and
renal medulla will depend on where the sagittal and transverse
images are obtained in relation to the
midline of the kidney. Renal pelvic dilatation may be best
visualized in the transverse plane (Fig. 5K andFig. 6K).
3
Figure 3Ka: Sagital View of Kidney:Centered on Hilus
Figure 4K: Transverse View of Kidney
Figure 3Kb: Sagital View of Kidney:Centered Off Hilus
-
7/31/2019 Us Urinary System and Prostate
4/8
Renal AbnormalitiesAs with other organs, diseases of the kidneys
are usually divided into focal and diffuse. The table 1K lists
examples of ultrasonographic changes in the kidney with possible
causes.
4
Ultrasonographic Appearance Diseases
Anechoic to hypoechoic lesions Renal cysts
Polycystic renal disease
Lymphosarcoma
Increased echogenecity Renal infarcts
InfectionNephrolithiasis
Renal calculi
Lymphosarcoma
Various echogenic appearances HematomasAbscesses
Neoplasia
Dilation of the renal pelvis Pyelonephritis
Hydronephrosis
Diuresis
Altered renal architecture Renal dysplasia
Neoplasia
End-stage renal disease
Anechoic fluid surrounding the kidneys Perinephrotic cyst
Perirenal hemorrhageExtravasation ofurine
Table 1K: Ultrasonographic Appearance of Common Renal
Diseases
Figure 5K:Renal pelvis Dilatation:
Sagital View
Figure 6K:Renal Pelvis Dilatation:
Transverse View
-
7/31/2019 Us Urinary System and Prostate
5/8
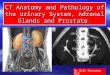
Urinary Bladder and Prostate Anatomy
The urinary bladder is a hollow organ which stores urine. The
size and location of the bladder is
divided into the neck and body with the neck directly toward the
pelvic canal and connected to the
urethra (Fig. 7K). The ureters enter the bladder on the
dorsocaudal aspect of the bladder just proximal tothe neck of the
bladder. The urinary bladder wall is composed of the serosa,
muscular layer and mucosa.
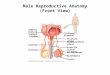
The prostate gland is located caudal to the urinary bladder. The
prostate gland in a castrated patient may
not be visualized. The prostate gland surrounds the pelvic
urethra beginning at the trigone region of the
urinary bladder. The prostate gland is a bi-lobe structure and
is surrounded by a capsule. The size and
position of the normal prostate gland varies with age, body size
and perhaps the breed of dog.
5
Figure 7K: Urinary Bladder and Prostate Anatomy:
Dorsal View
-
7/31/2019 Us Urinary System and Prostate
6/8
Ultrasonographic Urinary Bladder and Prostate Anatomy
The urinary bladder is identified as an anechoic structure in
the caudal aspect of the abdomen. The urinary
bladder is best evaluated when it is filled with urine. The
urinary bladder wall should be uniform in
thickness and the mucosal lining smooth in contour. Its wall
contains layers that can be seen in ideal
conditions as a double wall appearance (Fig. 9K).
The normal prostate gland has a homogeneous parenchymal pattern
with a medium to fine texture. Theechogenicity is variable from
hyperechoic to hypoechoic but should be uniform in
echogenicity.
Ultrasonographically, the individual lobes of the prostate gland
can be visualized in the transverse plane.
Ultrasonographic evaluation of the urinary bladder and prostate
gland is usually performed with the patient
in dorsal recumbency. A 7.5-megahertz transducer is ideal for
evaluating the urinarybladder andprostategland; however, in large
dogs, a 5-megahertz transducer can be used to evaluate the prostate
gland.
6
Figure 8K: Normal Urinary Bladder Figure 9K: Normal Urinary
Bladder:
Double Wall Appearance
Figure 10K: Normal Prostate:
Neutered Male
-
7/31/2019 Us Urinary System and Prostate
7/8
Urinary Bladder Abnormalities
Ultrasonographic abnormalities involving the urinary bladder
usually include thickening of the urinary
bladder wall which can be seen with cystitis or an infiltrative
process such as neoplasia. Neoplastic lesions
are most commonly identified in the trigone region and are
usually due to a transitional cell carcinoma (Fig.11K and 12K) but
can be present anywhere. Severe thickening of the urinary bladder
wall, especially in
cats, has been associated with neoplasia, such as lymphosarcoma.
The mucosal lining of the urinarybladder wall becomes irregular
with cystitis (Fig. 13K). Cystitis usually involves the
cranioventral aspect
of the urinary bladder. Cystic calculi (Fig. 14K) or blood clots
can be identified in the urinary bladder
lumen and usually gravitate to the dependent portion of the
urinary bladder wall. Evaluating the urinary
bladder with the patient in various positions would be necessary
to document that calculi or blood clots are
free floating within the lumen. Cystic calculi are usually
hyperechoic and result in acoustic shadowing
(Fig. 14K).
7
Figure 14K: Calculus and Cystitis
Figure 11K: Transitional Cell Carcinoma
Figure 13K: Severe Cystitis
Figure 12K: Transitional Cell Carcinoma
-
7/31/2019 Us Urinary System and Prostate
8/8
Prostate Abnormalities
Most of the disease processes involving the prostate gland
result in enlargement of the prostate gland.
Prostatic cysts appear as anechoic regions within the prostate
gland with acoustic enhancement and can be
of various sizes. Prostatic cysts (Fig 15K) must be separated
from prostatic abscesses (Fig 16K). Prostatic
abscesses usually contain echogenic material and are surrounded
by a capsule. Periprostatic cysts are also
associated with the prostate gland. Prostatic cysts or
periprostatic cysts may be congenital or developsecondary prostatic
hypertrophy or squamous metaplasia. Benign prostatic hyperplasia or
prostaticinfections can have a very similar appearance. Benign
prostate hyperplasia and infection usually result in
generalized enlargement of the prostate gland. Scattered
hyperechoic foci and small cysts can be
associated with prostatic hyperplasia; however, with prostatic
inflammation, the parenchyma is usually
heterogeneous with a mixed pattern of echogenicity. The prostate
gland may become hypoechoic with
infection. Mineralization is not usually associated with benign
prostatic hyperplasia; however, with
infection, hyperechoic areas secondary to fibrosis, gas or
mineralization can be visualized. The prostatic
capsule usually remains intact with both benign hyperplasia and
infection.
With prostatic neoplasia, the prostatic parenchyma has no
specific ultrasonographic changes to differentiate
neoplasia from infection or hyperplasia. Hyperechoic areas can
be present throughout the parenchymasuggesting mineralization;
however, caviar or cyst-like lesions can also be present.
Differentiation of
benign prostatic hyperplasia, prostatitis, or prostatic
adenocarcinoma can be difficult based on the
ultrasonographic appearance. A biopsy of the prostate gland may
be necessary to establish a definitive
diagnosis. With prostatic neoplasia, evaluation of the sublumbar
lymph nodes for changes to suggest
metastasis is recommended.
8
Figure 15K: Prostatic Cysts and HyperplasiaFigure 16K: Prostatic
Abscess