Embed Size (px)
Citation preview

Urological Trauma
Doc. MUDr. Robert Grill PhDr.
Urologická klinika 3. LF UK a FNKV

Renal trauma-aetiology and pathogenesis
Penetrating trauma ( stab wounds, gunshots
injuries)Blunt trauma ( 80-85% of all kidney´s
traumas) - direct blunt impact - deceleration
injuriesIatrogenic
(parenchymal injury during surgery , ESWL, percutan extraction of concrement )
a b
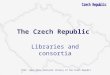
Mechanisms of renal injury a) direct blunt impact b) deceleration

Renal injury classification
AAST renal injury grading scale
Grade 1 - Contusion or non-expanding subcapsular haematoma, no laceration
Grade 2 - Non-expanding peri-renal haematoma, Cortical laceration < 1 cm deep without extravasation
Grade 3 - Cortical laceration > 1 cm without urinary extravasation
Grade 4 - Laceration through corticomedullary junction into collecting system or segmental renal artery or vein injury with contained haematoma, or partial vessel laceration, or vessel thrombosis
Grade 5 - shattered kidney or renal pedicle or avulsion.

Renal injury- symptomatology
Haematuria ( at 80-90% renal trauma)- no correlation between level of haematuria and degree of injury / 1/3 of wounded does not suffer by haematuria /
Abdominal tenderness extended during palpationAbdominal abrasionsRibs fractureNausea, vomiting, blockage of the intestine , acute
abdomen signsSymptoms of hypovolemic shock ( systolic pressure
< 90mm Hg, P > 90/min, decreased or no urine output, pale skin color, cool, clammy skin …..).

Diagnosis of renal injuries
Haemodynamic stability of patient is the fundamental criterion
History of accident - background of injury (rapid deceleration, direct blow to the flank, the size of the weapon in
stabbings…)
Patient´s medical history – focusing on pre-existing kidney dysfunctions and diseases
( hydronephrosis, nephrolithiasis, kidney cysts, kidney tumors, kidney surgeries )
Physical assessment - haematuria, flank abrassions, flank palpable pain, palpable mass in the kidney area, abdominal distension, acute abdomen signs, fractured ribs
Laboratory evaluation - urinalysis, regular haematocrit controlling, creatinine baseline

Diagnosis of renal injuries Imaging – criteria for radiographic assessment - gross or microscopic
haematuria and shock, associated major injuries Ultrasonography - provides a quick, non-invasive, low-cost means of
detecting peritoneal fluid collections, can detect degree of renal injury, eliminate solitary kidney, dopplers assessment of functional state of kidney, indication for other radiological examination
Standard IVP - offers basic information about kidney functionality, nowadays supplied by contrast CT examination. Unstable patients selected for immediate operative intervention / ,,one-shot“ IVP/ are exception for using Standard IVP.
Computed tomography – CT is a standard method used on stable patients. It is more sensitive and specific than IVP, USG and angiography. CT detects the location of injuries, evaluates details and functionality of kindneys, defines pre-existing abnormalities and associated traumas. Magnetic resonance imaging - MRI has no advantage in compare with CT, it requires a longer imaging time, increases the cost, and limits access to patients when they are in the magnet during the examination. MRI is therefore useful in renal trauma if patient suffers with iodine allergy or renal insuficience. Angiography - has been largely replaced by CT as the use of angiography is less specific, more time-consuming and more invasive. Angiography may be preferable when planning selective embolisation for the management of persistent or delayed haemorrhage from branching renal vessels .

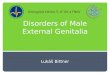
Renal injuries- Computed tomography
Grade 3 - Cortical laceration Grade 5 - shattered kidney/ arrow/

Treatment and prognosis in renal injuries
Non-operative therapy – choice for the majority stable patients with renal injuries grade 1-4 (bed-rest, hydration, antibiotics, continuous imaging examinations, hemostyptic therapy, monitoring of vital signs ).
Surgical management Indications – haemodynamic instability
- exploration for associated injuries - expanding or pulsatile peri-renal
haematoma identified during laparotomy - grade 5 injury - incidental finding of pre-existing renal
pathology requiring surgical therapy

Early and delayed complications at renal trauma
Early complications - occur within the first month after injury and can be bleeding, infection, peri-nephric abscess, sepsis, urinary fistula, hypertension, urinary extravasation, and
urinoma.
Delayed complications - include bleeding, hydronephrosis, calculus formation, chronic pyelonephritis, hypertension ( less than 5% patients ), arteriovenous fistulae, hydronephrosis and pseudoaneurysms.

Ureteral trauma-aetiology and pathogenesis
Very rare and accounts for only 1% of all urinary tract trauma.Blunt trauma 18%Penetrating trauma 7%Iatrogenic 75%
- gynecological 73% ( hysterectomy, ovarectomy, gynecologic laparoskopy surgery…)
- surgical 14% ( colorectal surgery, abdominal vascular surgery….)
- urological 14% ( ureteroscopy, insertion of ureteral catheter )

AAST ureteral injuries classification
• Grade 1: Haematoma only• Grade 2: Laceration < 50% of circumference• Grade 3: Laceration > 50% of circumference• Grade 4: Complete tear < 2 cm of devascularisation
• Grade 5: Complete tear > 2 cm of devascularisation

Ureteral trauma symptoms
Varies according to aetiology and difficulty of injury :
• Abdominal and flank pain• Haematuria in different levels• Faebrilia• Decreased urine output• Nausea, vomiting• Urosepsis• Acute abdomen signs

Diagnosis of ureteral trauma
Physical assessment Laboratory examination (urinalysis, blood
testing, renal functions ) Imaging - Ultrasonography (hydronephrosis,
hydroureter, extravasation of urine ) - Plain abdominal X-rays - IVP (delayed excretion, ureteral
dilatation, ureteral deviation, extravasation of radiological contrast material)
- CT scan (delayed excretion, ureteral dilatation, extravasation of radiological contrast material, urinoma)

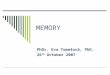
Ureteral trauma-IVP
Urinary extravasation from the middle third of the left ureter /after ureteroscopy/

Therapy of ureteral trauma
Treatment depends on the extent and the location of uretal trauma :
Grade 1 and 2 can be managed non-surgical with ureteral stenting or nephrostomy.
Grade 3 to 5 need a reconstructive repair. The type of reconstructive repair procedure depends on the nature and the site of the injury.
The options for repair of ureteral injuries - Uretero-ureterostomy - Ureterocalycostomy - Transuretero-ureterostomy - Boari flap and reimplantation - Ureterocystostomy - Psoas hitch - Ileal interposition

Complications at ureteral trauma
• Urinoma• Periureteral abscess• Fistula• Strictura

Bladder trauma - aetiology and pathogenesis
2% of all abdominal injuries, often associated with pelvic fracture
Blunt trauma - caused by direct impacts at the pelvic area or lower abdominal at patients with the full bladder, 80-100% of patiens suffer pelvic fractures at the same time
Penetrating trauma- gunshots, stub wounds
Iatrogenic trauma-1/2 of all bladder traumas (transuretral operation of prostatis, bladder, gynaecological operations, hernioplasty)

Bladder injury classification
Classification of bladder injury according to AAST
Grade 1 - Contusion Grade 2 - Intraperitoneal bladder
wall laceration Grade 3 – Intersticial injury Grade 4 - Extraperitoneal
bladder wall laceration - simple - complicated
Grade 5 – combination of injuries intraperitoneal and extraperitoneal
Extraperitoneal bladder wall laceration

Bladder trauma symptoms
Lower abdominal pain Gross haematuria most common signs
Nausea, vomiting Paralytic ileusPeritonitisInability to voidBruises over the suprapubic regionHaemoragic shock

Diagnosis of bladder traumas
Physical assessment – lower abdominal pain, crepitations and instability of pelvic ring, abrassions…..
Laboratory examination – urianalysis and blood examination Imaging
- Retrograde ureterocystography : standardly used method, sensitivity of 100%, it is neccessary to fill the bladder with a minimum of 350 ml of dilute contrast material
- CT cystography : this procedure should be performed using retrograde filling of the bladder with dilute contrast material
- IVP : is inadequate for evaluation of the bladder trauma ( dilution of the contrast material within the bladder, too low resting intravesical pressure to demonstrate a small tear )

Bladder trauma- Retrograde cystography
Extraperitoneal bladder wall laceration
Intra and extraperitoneal bladder wall laceration

Therapy of bladder traumas
Extraperitoneal bladder ruptures - managed by catheter drainage alone, ATB treatment
Indications for surgical repair : - intraperitoneal bladder ruptures - bladder neck injuries - the presence of bone fragments in the bladder wall - entrapment of the bladder wall by bone fragments - associated injuries that require surgical
intervention, are managed by interdisciplinary cooperation

Urethral trauma
Male urethral injury
The posterior urethra - prostatic and the membranous urethra.
The anterior urethra -
bulbar and penile urethra.

Urethral trauma – aetiology and pathogenesis
1. Posterior urethral injuriesMostly the result of pelvic fractures
/ height falls, traffic accidents /
2. Anterior urethral injuriesBlunt traumaPenetrating injuriesIatrogenic injuriesAutomutilation

Classification of urethral injuries
Classification of blunt anterior and posterior urethral injury
Grade 1 : Stretch injury. Elongation of the urethra without extravasation on urethrography
Grade 2 : Contusion. Blood at the urethral meatus, no extravasation on urethrography
Grade 3 : Partial disruption of anterior or posterior urethra. Extravasation of contrast at injury site with contrast visualised in the proximal urethra or bladder
Grade 4 : Complete disruption of anterior urethra. Extravasation of contrast at injury site without visualisation of proximal urethral or bladder
Grade 5 : Complete disruption of posterior urethra. Extravasation of contrast at injury site without visualisation of bladder
Grade 6 : Complete or partial disruption of posterior urethra with associated tear of the bladder neck or vagina

Symptoms of urethral trauma
• Lower abdominal pain
• Urethrorrhagia
• Inability to void
• Perineal haematoma

Urethral trauma diagnosis
Physical assessment – lower abdomen pain,urethrorrhagia, crepitations and instability of pelvic ring, ecchymosis, high-riding prostate, perineal haematoma
Laboratory examination – urinalysis and blood testing
Imaging - retrograde urethrography – gold standard for
evaluating urethral injury- CT and MRI : used in defining distorted pelvic
anatomy after severe injury and assessing associated injuries of other organs
- USG : useful in determining the position of pelvic haematomas, or the exact location of the bladder when a suprapubic catheter is indicated.

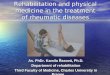
Urethral trauma- retrograde urethrography
Normal retrograde urethrography Disruption of posterior urethra

Therapy of urethral traumas
I. Anterior urethral injuries therapy Grade 1 – no treatment is neccessary Grade 2 and 3 - urethral catheterisation or suprapubic cystostomy More complicated injuries -suprapubic derivation, delayed optic
uretrotomy, urethral dilatation, longer defects of the anterior urethra should be repaired by an end-to-end anastomosis, defects over 1cm by flap urethroplasty
Open injuries - primary urethral suturing- defects of more than 1 cm in length a two-stage urethral repair
II. Posterior urethral injuries therapy Partial urethral rupture - suprapubic or urethral catheter. Complete urethral rupture - primary endoscopic realignment,
- immediate open urethroplasty , - delayed primary urethroplasty, - delayed formal urethroplasty, - delayed endoscopic incision

Female urethral injuries
Only the posterior urethra exists in the femaleRare injuries due to length and limited connection to
pubic boneMost often during the delivery, iatrogenic trauma,
pelvic fracture, fracture of ventral part of pelvic ring
Symptoms are similar to male urethral traumaIn diagnostic,urethroscopy is prefered to technically
hard performed urethrographyMost female urethral disruptions can be sutured
primarily either transvaginally or transvesically

Complications at urethral trauma
• Urinary incontinence• Erectile dysfunction• Urethral stricture• Fistulae or urethral pseudodiverticula

Genital trauma
• Penile trauma• Prostate and seminal vesicles trauma• Scrotal trauma

Penile trauma
Aetiology Blunt trauma – penile fracture, ischemic gangrene, thermal and
chemical injuries Penetrating trauma – gunshots wounds, stab, cuts Sympthoms Pain, haematoma, inability to void, bleedingDiagnosis Physical assessment /palpable tenderness, haematoma,
haematuria / USG, Retrograde urethrography / to eliminate an injury of urethra/Therapy In penile fracture- surgical intervention Reimplantation in case of total penile amputation In associated injury of urethra-epicystostomia, urethral
catheterisation

Prostate and seminal vesicles trauma
Aetiology Injury of the prostate and posterior urethra associated with pelvic
trauma Iatrogenic-prostate biopsySymptoms rectorrhagia Perineal pain Urethrorrhagia, hematuria Fever, septic shockDiagnosis Physical assessment -digital rectal examination/pain, oedema,
fluctuation / USG, NMR true Pelvis Therapy ATB, hemostyptic drugs, rectum tamponade, incision and
drainage of prostatic abscess

Scrotal trauma
Aetiology Blunt trauma Penetrating trauma / rare injuries / Iatrogenic traumaSymptomatology Depends on the extent of the injury / pain, bleeding, swollen /Diagnostic Physical assessment –inspection, palpation USG, CT, NMRTherapy Depends on the extent of the injury / from conservative
management to reconstruction of scrotum / Complications Post-traumatic testicular atrophy Testicular cancer

Adrenal trauma-aetiology
Vary in infants and adults
Blunt trauma
Penetrating trauma
Iatrogenic trauma
Infants post-delivery trauma

Adrenal trauma - symptoms
Haemoragic shock
Palpable resistance
Acute adrenal insufficiency /tachypnoe,
fever, petechiae and purpura, metabolic collapse, abdominal pain, vomiting and diarrhoea, spasm and cyanosis/ most common in infants with bilateral adrenal injury

Adrenal trauma-diagnosis
Physical assessment / palpable resistance, hypovolemic shock symptoms /
Abdominal X-ray /kidney dislocation, contour calcification/
IVPCT with urographyUmbilical Vein AngiographyNefroblastoma(Wilms`Tumor ) in differential
diagnosis

Adrenal trauma-therapy
Conservative management with blood loss compensation, corticoid substitute,
correction of metabolic interference
Surgical intervention in cases unable to treat non-operative – exploration,
nephroadrenalectomy

Literature
- Traumata urogenitální soustavy Doc. MUDr. Robert Grill, Ph.D.- Urologie 2009 Kawaciuk et kolektív- Všeobecná urologie 2006 Emil A. Tanagho, Jack W. McAninch- EAU Guidelines on urological trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, et kol.http://www.acssurgery.com/acssurgery/secured/figTabPopup.action?bookId=ACS&linkId=part07_ch11_fig3&type=fig-http://www.health-reply.com/urethral-injury-classification/-Teaching Atlas of Urologic Imaging Older / Bassignani
Thank you for your attention
![University Of Finance & Administration INTERNATIONAL BUSINESS [E_IB] PhDr. Karel Eliáš, CSc. 18303@mail.vsfs.cz](https://img.pdfslide.us/doc/110x75/56649d155503460f949e9f7c/university-of-finance-administration-international-business-eib-phdr.jpg)















![[INFORMATION INTERACTIONS 2016] - uniba.sk · INFORMATION INTERACTIONS 2016 DIGITAL SCHOLARSHIP, INFORMATION ETHICS ... Comenius University in Bratislava Program chair: Prof. PhDr](https://img.pdfslide.us/doc/110x75/5f0a9aad7e708231d42c72ce/information-interactions-2016-unibask-information-interactions-2016-digital.jpg)