Embed Size (px)
Citation preview
10/9/2015
1
Dana A. Brown, Pharm.D., BCPSAssistant Dean for Academics, Associate Professor of Pharmacy PracticePalm Beach Atlantic University
1. Explain the pathophysiology of benign prostatic hyperplasia (BPH), including factors which can worsen BPH
2. Recognize the clinical presentation of BPH, including common signs and symptoms
3. Provide appropriate non‐pharmacologic and pharmacologic recommendations for a given patient with BPH based on patient‐specific parameters
4. Counsel a given patient on the appropriate administration and potential adverse effects of various BPH treatment modalities
5. Compare and contrast BPH treatment modalities pwith regards to adverse effects, role in therapy, and drug‐drug interaction considerations
6. Explain patient characteristics that would make various BPH treatment modalities inappropriate (contraindications)
10/9/2015
2
Mr. JonesMr. Jones
71 yo WM
Chief Complaint “It feels like I have to pee all of the time. I get frustrated because I just end up dribbling until the urine comes out.”
Mr. Jones, cont’dMr. Jones, cont’d
History of Present Illness
‐1 year h/o difficulty urinating that has
worsened over the past month
Reports dribbling straining weak stream‐Reports dribbling, straining, weak stream,
nocturia X 3 episodes/night, occasional bed
wetting
‐Denies hematuria, loss of urine with activity
Mr. Jones, cont’dMr. Jones, cont’d
Past Medical History
‐Hypertension ‐Dyslipidemia
‐GERD ‐Allergies
‐Type 2 diabetes
Family History
‐Mother: ↓ age 69; + HTN, Type 2 DM
‐Father: ↓ age 88 from CHF; + HTN, Type 2 DM, dyslipidemia
‐Brother: ↑ age 69; + HTN, dyslipidemia

10/9/2015
3
Mr. Jones, cont’dMr. Jones, cont’d
Social History
‐Married X 49 years
‐1 daughter aged 42
R ti d t‐Retired carpenter
‐Drinks 1 beer each evening
‐Smokes 1 pack of cigarettes/day
‐No routine physical activity
Mr. Jones, cont’dMr. Jones, cont’d
Medications: Atenolol 100 mg PO Qdaily
Lisinopril 10 mg PO Qdaily
Pravastatin 40 mg PO HS
Famotidine 20 mg PO BID
Loratadine 5 mg/Pseudoephedrine 120 mg PO BID
Aspirin 325 mg PO Qdaily
Metformin 1000 mg PO BID
Glipizide XL 10 mg PO Qdaily
Amitriptyline 25 mg PO QHS
What is BPH?What is BPH?
Benign Prostatic Hyperplasia1,2
Enlargement of the prostate resulting in compression of the urethra ultimately leading to difficulty with urinationto difficulty with urination
American Urological Association definition1
“a histologic diagnosis that refers to the proliferation of smooth muscle and epithelial cells within the prostatic transition zone.”
Signs and symptoms may be regressive

10/9/2015
4
EpidemiologyEpidemiology22
~50% of men >60yo have microscopic findings consistent with BPH; ~90% at >85yo
~50% of men with microscopic changes will~50% of men with microscopic changes will develop an enlarged prostate gland and have difficulty emptying the bladder
~50% of symptomatic patients will require treatment
Functions of the Prostate GlandFunctions of the Prostate Gland22
Two major functions of the prostate gland:
1. To secrete liquefying components of semen q y g pwhich allow sperm to move freely
2. To produce secretions which have antibacterial effects because of high zinc concentrations
Prostate Gland Growth SpurtsProstate Gland Growth Spurts22
BirthProstate weighs
~ 1 g
~40sGrowth Spurt #2
Prostate doubles/triplesin size
AdolescenceGrowth Spurt #2
Prostate weighs ~15-20 g
Age 70-80Prostate continues
to grow until this age
10/9/2015
5
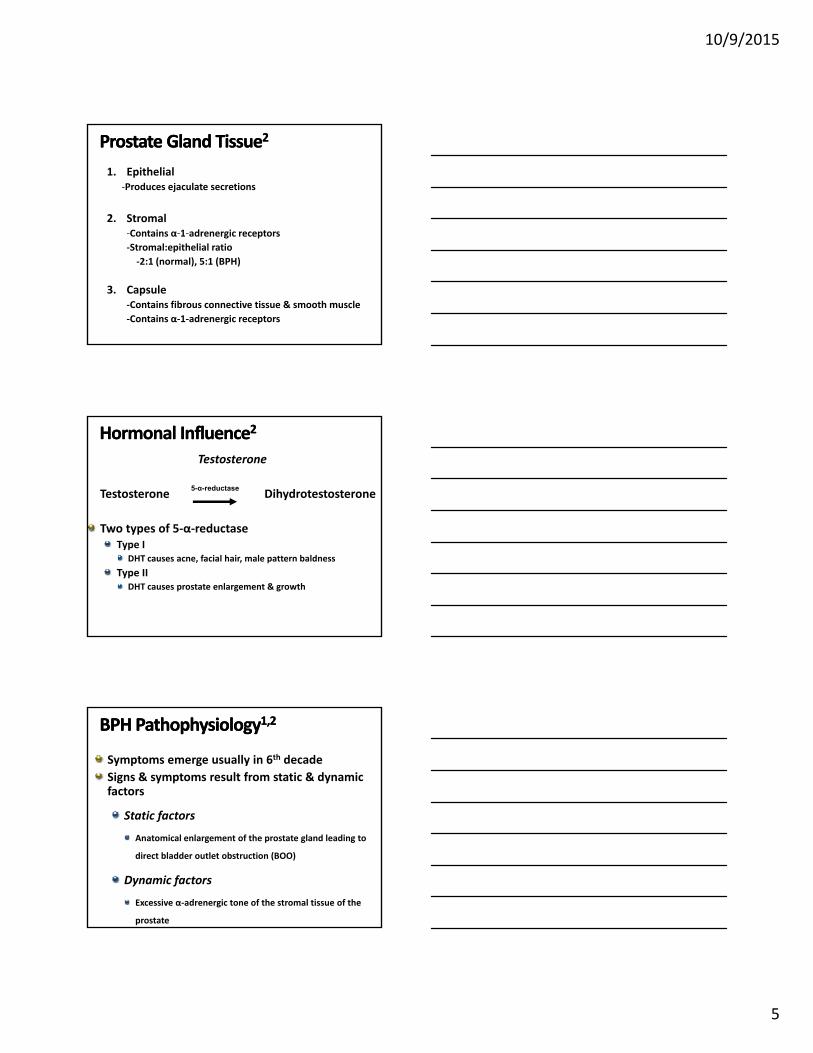
Prostate Gland TissueProstate Gland Tissue22
1. Epithelial‐Produces ejaculate secretions
2. Stromal‐Contains α‐1‐adrenergic receptorsContains α 1 adrenergic receptors
‐Stromal:epithelial ratio
‐2:1 (normal), 5:1 (BPH)
3. Capsule‐Contains fibrous connective tissue & smooth muscle
‐Contains α‐1‐adrenergic receptors
Hormonal InfluenceHormonal Influence22
Testosterone
Testosterone Dihydrotestosterone
T o t pes of 5 α red ctase
5-α-reductase
Two types of 5‐α‐reductaseType I
DHT causes acne, facial hair, male pattern baldness
Type IIDHT causes prostate enlargement & growth
BPH PathophysiologyBPH Pathophysiology1,21,2
Symptoms emerge usually in 6th decade
Signs & symptoms result from static & dynamic factors
Static factorsStatic factors
Anatomical enlargement of the prostate gland leading to
direct bladder outlet obstruction (BOO)
Dynamic factors
Excessive α‐adrenergic tone of the stromal tissue of the
prostate

10/9/2015
6
Lower Urinary Tract Symptoms (LUTS)Lower Urinary Tract Symptoms (LUTS)1,21,2
ObstructiveWeak urine stream
Urinary hesitancy
Straining
bbl
IrritativeUrinary frequency
Urgency
Nocturia
Dribbling
Incomplete bladder emptying (feeling of fullness after voiding)
Enuresis
Medications and Worsening of BPH Medications and Worsening of BPH SymptomsSymptoms1,21,2
Testosterone replacement regimens
More substrate to be converted to DHT
α‐adrenergic agonists (pseudoephedrine)
Stimulate α‐adrenergic receptors
Anticholinergic agents (antihistamines, phenothiazines, TCAs)
May ↓ bladder contractility
Quiz Question #1Quiz Question #1
Which of Mr. Jones’ medications could be contributing to his current clinical presentation?
A. Atenolol
B. Amitriptyline
C. Loratadine/pseudoephedrine
D. A & B
E. B & C

10/9/2015
7
Quiz Question #2Quiz Question #2
The 5‐α reductase enzyme converts dihydrotestosterone to testosterone.
A. True
B. False
Quiz Question #3Quiz Question #3
Mr. Jones’ complaints of nocturia and bed wetting are examples of what type of BPH symptoms?
A. Dynamic
B. Irritative
C. Obstructive
D. Static
Clinical Clinical AssessmentAssessment1,21,2
ALWAYS assess medications!!!
Other useful parametersProstate‐specific antigen (PSA)
Age PSA (ng/mL)40‐49 0‐2.5ng/mL
/
Not specific for BPH!
50‐59 0‐3.5ng/mL
60‐69 0‐4.5ng/mL
70‐79 0‐6.5ng/mL
Digital Rectal Exam (DRE)Helps determine size of prostate gland & assesses for prostate cancer
Harder but still somewhat soft on palpation (nose cartilage)
10/9/2015
8
Back to Mr. Jones…Back to Mr. Jones…
Vital Signs: BP 106/70, P 54, RR 22, Temp 98.5◦F, Pain 0/10, Wt 263 lbs
PE: All WNL exceptPE: All WNL except
GU: Normal scrotum; prostate round, mobile and firm on palpation; penis w/o discharge or curvature
Mr. Jones, cont’dMr. Jones, cont’dLaboratory/Diagnostic Findings
Chem 8 WNL
PSA: 7.9 ng/mL
U/S findings: PVR of 264 mL and prostate weight of approximately 51 g
U/A: ‐Color: yellow ‐Leukocyte esterase: (‐)
‐SG: 1.010 ‐Nitrites: (‐)
‐Glucose: (‐) ‐Ketones: (‐)
‐Blood: (‐)
Quiz Question #4Quiz Question #4
Mr. Jones’ PSA score of 7.9 ng/mL is considered elevated and likely indicates BPH.
A. True
B. False

10/9/2015
9
Complications of BPHComplications of BPH
BPH Management Options BPH Management Options 1,21,2
1. Watchful waiting
2. Pharmacotherapyα‐adrenergic antagonists5‐α‐reductase inhibitors
Type 5 phosphodiesterase inhibitorsType‐5 phosphodiesterase inhibitors Hormones (LHRH agonists & anti‐androgens)
Herbals/Complementary alternative medicine (CAM)
3. Minimally Invasive/Surgical InterventionsProstatectomy
Transurethral resection of the prostate (TURP)
Transurethral microwave thermotherapy (TUMT)
Watchful WaitingWatchful Waiting11
Indicated for patients with mild symptoms or who are asymptomatic
No specific treatment is indicated
Return for reassessment Q6‐12 months
10/9/2015
10
Patient EducationPatient Education11
Fluid restriction at bedtime
Avoid caffeine & alcohol intake
Li it lt i t kLimit salt intake
Frequent emptying of bladder
Avoid drugs that exacerbate symptoms
Categories of Drug OptionsCategories of Drug Options1,2,31,2,3
1. Interference with testosterone stimulatory effects on the prostate gland (↓ static factors)
‐5‐α‐reductase inhibitors
‐Hormones (LHRH agonists & anti‐androgens)
2. Relaxation of the prostatic smooth muscle (↓ dynamic factors)
‐ α‐adrenergic antagonists, PDE 5 inhibitors (?)
3. Combination therapy
‐ α‐adrenergic antagonist + 5‐α‐reductase inhibitor
Drug InitiationDrug Initiation2,32,3
Initiate with a single agent
α‐adrenergic antagonistFaster acting & more effective
Less sexual adverse effects
5‐α‐reductase inhibitor Prostates > 40g
Cannot tolerate the CV effects of α‐antagonists
PDE5 inhibitorFDA‐approved for BPH or BPH + ED
Combination therapy Prostates ≥50g + ↑ PSA levels

10/9/2015
11
αα‐‐Adrenergic AntagonistsAdrenergic Antagonists1,2,4,5,6,7,8,9,101,2,4,5,6,7,8,9,10
MOA: Relax prostatic smooth muscle by α1‐adrenergic receptor blockade (α1A [tamsulosin & silodosin])
Examples:First generation: phenoxybenzamine
Second generation: alfuzosin (Uroxatral®) doxazosinSecond generation: alfuzosin (Uroxatral®), doxazosin(Cardura®/Cardura XL®), terazosin (Hytrin®)
Third generation: Tamsulosin (Flomax®), silodosin (Rapaflo®)
↓ BPH symptoms but do not ↓ prostate size or volume
Do not affect PSA levels
TamsulosinTamsulosin v. Silodosinv. Silodosin1111
955 pts with t ti BPH
Silodosin 8 mg/dX 12 weeks
Tamsulosin 0.4 mg/dX 12 k
∆ from baseline in t t l f
Silodosin and tamsulosin significantly improved total scores of IPSS questionnaire, storage/voiding scores and QOL as compared to placebo
symptomatic BPH X 12 weeks
PlaceboX 12 weeks
total score ofIPSS questionnaire
TamsulosinTamsulosin v. v. SilodosinSilodosin, cont’d, cont’d1111
Only silodosin significantly ↓ nocturia v. placebo
Improvements in Qmax were noted in ALL t t ttreatment groups
A high placebo response
Most common ADR was absent or ↓ ejaculation
14% with silodosin, 2% with tamsulosin

10/9/2015
12
αα‐‐Adrenergic Adrenergic Antagonists, Antagonists, cont’dcont’d1,2,4,5,6,7,8,9,121,2,4,5,6,7,8,9,12
Relief of symptoms usually within 3 weeks of initiation
DosesAlfuzosin XR 10mg PO with same meal Qdaily
Doxazosin 1mg PO QHS, up to 4‐8mg/dayg Q , p g/ y
Doxazosin XL 4mg PO Qam w/breakfast, up to 8mg PO Qam over 3‐4 weeks
Terazosin 1mg PO QHS, up to 2‐10mg/day
Tamsulosin 0.4mg PO Qdaily, up to 0.8mg/day if no resolution of symptoms within 2 weeks of initiation; Take 30 min after the same meal
Silodosin 8mg PO with same meal Qdaily
αα‐‐Adrenergic Antagonists, cont’dAdrenergic Antagonists, cont’d99
Renal Dosage Adjustment for SilodosinCrCl > 50 ml/min: No dosage adjustment is needed.
CrCl 30—50 ml/min: 4 mg PO once daily.
CrCl < 30 ml/min: Not recommended.
αα‐‐Adrenergic Antagonists, cont’dAdrenergic Antagonists, cont’d1,2,4,5,6,7,8,91,2,4,5,6,7,8,9
Adverse EffectsOrthostatic hypotension (2nd generation)
Dizziness (2nd generation)
First dose syncope (2nd generation)
Fatig e (3rd generation)Fatigue (3rd generation)
Ejaculatory dysfunction (3rd generation)
Nasal congestion (3rd generation)
Flu‐like symptoms (3rd generation)
↑ risk for complications with cataract surgery (3rd generation)13

10/9/2015
13
αα‐‐Adrenergic Antagonists, cont’dAdrenergic Antagonists, cont’d1,2,4,5,6,7,8,91,2,4,5,6,7,8,9
Drug‐Drug InteractionsAlfuzosin is a substrate for CYP 3A4
Tamsulosin clearance is ↓ by cimetidine (avoid use)
Phosphodiesterase‐5 inhibitorsProduce systemic hypotension
Coadministration: stable dose of α‐adrenergic antagonist before initiation of PDE5 inhibitor
αα‐‐Adrenergic Antagonists, cont’dAdrenergic Antagonists, cont’d1,2,4,5,6,7,8,91,2,4,5,6,7,8,9
Avoid use:Hepatic insufficiency (no use in severe hepatic dysfunction)
Strong CYP 3A4 inhibitors (tamsulosin & silodosin)
CAD/angina
V l d l ti T l i &Volume depletion
Cardiac arrhythmias
Multiple antihypertensives
NOTE: Monotherapy with α‐adrenergic antagonists for the management of HTN in men with BPH is inappropriate therapy for HTN14
Tamsulosin & Silodosin arebetter options
αα‐‐Adrenergic Antagonists, cont’dAdrenergic Antagonists, cont’d1,8,91,8,9
Monitoring Parameters
Symptom improvement
BP and HR checks at every visit

10/9/2015
14
55‐‐αα‐‐ReductaseReductase InhibitorsInhibitors1,15,16,171,15,16,17
MOA: Blockade of 5‐α‐reductase enzyme to inhibit conversion of testosterone to DHT (finasteride – Type II only)
Examples:
Finasteride (Proscar®)
Dutasteride (Avodart®)
Best used in patients with LUTS and enlarged prostates (≥50 grams)
Adequate trial is 6‐12 months
55‐‐αα‐‐ReductaseReductase Inhibitors, cont’dInhibitors, cont’d1,15,16,171,15,16,17
DosesFinasteride 5mg PO Qdaily
Dutasteride 0.5mg PO Qdaily
Maximal reductions in prostate size seen ~12 monthsmonths
Adverse EffectsEjaculation disorders
Erectile dysfunction/↓ libido
Gynecomastia
Nausea, abdominal pain, flatulence
Rash (finasteride only)
55‐‐αα‐‐ReductaseReductase Inhibitors, cont’dInhibitors, cont’d1,15,16,171,15,16,17
Contraindications/PrecautionsHepatic dysfunction (caution)
Pregnancy Category XWomen of childbearing age or who are pregnant should NOT
Handle 5‐α‐reductase inhibitor tablets
Have contact with semen from men treated with 5‐α‐reductase inhibitors
Drug‐Drug InteractionsDutasteride only: cautious use with CYP 3A4 inhibitors/inducers
10/9/2015
15
55‐‐αα‐‐ReductaseReductase Inhibitors, cont’dInhibitors, cont’d1,15,16,171,15,16,17
Monitoring ParametersObtain baseline PSA & DRE
↓ PSA levels by 50%
Follow up with PSA in 6 months, then PSA & DRE annually
PDE5 InhibitorsPDE5 Inhibitors1188
MOA: Inhibition of PDE5 in prostate to cause vasodilation and prostatic and bladder neck relaxation
Example: Tadalafil (Cialis®)
FDA approved in Oct 2011
Approved for BPH as well as BPH + ED as studies show improvement in urinary symptoms
Dose5 mg PO Qdaily
Combination Combination TherapyTherapy19,2019,20
5‐α‐reductase inhibitor + α‐adrenergic antagonistJalyn® (0.5 mg dutasteride + 0.4 mg tamsulosin)
Ideal for patients with
Severe symptomsSevere symptoms
Enlarged prostates (>40 grams)
↑ PSA levels
Has been shown to prevent symptom progression & ↓ the risk for developing urinary retention, UTIs, & need for surgery

10/9/2015
16
Combination Therapy, cont’dCombination Therapy, cont’d1,19,201,19,20
↑ adverse effects and expensive
Can consider d/c’ing α‐blocker after 6‐9 mos
α‐adrenergic antagonist + anticholinergicConsidered for patients with BOO symptoms + symptoms of overactive bladder
Urinary frequency, urgency, enuresis
Quiz Question #5Quiz Question #5
Silodosin provides quick symptom relief in the management of BPH as well as reduces prostate size and volume.
A. True
B. False
Quiz Question #6Quiz Question #6
As part of the management of his BPH symptoms, Mr. Jones may be counseled to:
A. Avoid alcohol at bedtime
B. Discontinue using loratadine/pseudoephedrine
C. Limit fluid intake at bedtime
D. All of the above

10/9/2015
17
Quiz Question #7Quiz Question #7
A common adverse effect associated with terazosin therapy is:
A E il d f iA. Erectile dysfunction
B. Gynecomastia
C. Orthostatic hypotension
D. Rash
Quiz Question #8Quiz Question #8
Which of the following treatment options is appropriate for initiating today to manage Mr. Jones’ BPH symptoms?
A. Finasteride 5 mg PO Qdaily
B. Tadalafil 5 mg PO Qdaily
C. Tamsulosin 0.8 mg PO Qdaily
D. Terazosin 10 mg PO QHS
Herbals/CAM, cont’dHerbals/CAM, cont’d
Saw palmetto21,22,23Earlier evidence suggests modest efficacy on treated LUTS
Newer data fail to confirm a clinical important role in the management of BPH
AUA 2010 guidelines do not advocate recommending saw palmetto for BPH due to a lack of evidence1

10/9/2015
18
Zinc24High zinc levels found in normal prostate glands
Some men with BPH have low zinc t ticoncentrations
Better conclusions seen in men with prostate cancer
Adverse effects: Nausea, vomiting, abdominal cramps
Surgical InterventionSurgical Intervention11
Indications for surgeryUnresponsive to drug therapy
Refractory urinary retention or other BPH complications
Recurrent UTIs secondary to BPH
Individual preference
Prostatectomy
Transurethral resection of the prostate (TURP)
Transurethral microwave thermotherapy (TUMT)
Quiz Question #Quiz Question #99
Saw palmetto acts similar to tamsulosin to improve the symptoms of BPH.
A. True
B. False
10/9/2015
19
Quiz Question #10Quiz Question #10Mr. Jones has been receiving silodosin 8 mg PO Qdaily and dutasteride 0.5 mg PO Qdaily for 6 months now. His PSA is 3.3 ng/mL. He reports significant improvement in his symptoms and is mostly “symptom free”. Which of the following should occur?should occur?
A. He should continue both medications
B. He should D/C dutasteride and continue
silodosin
C. He should D/C silodosin and continue dutasteride
D. He should D/C both medications