Embed Size (px)
Citation preview
Urinary Symptoms as a Predictor forParticipation in Prostate Cancer Screening
Among African American Men
Sally P. Weinrich,1* Martin Weinrich,2 Curtis Mettlin,3William A. Reynolds Jr.,2 and John E. Wofford4
1College of Nursing, University of South Carolina, Columbia, South Carolina2School of Public Health, University of South Carolina, Columbia, South Carolina
3Roswell Park Cancer Institute, Buffalo, New York4Columbia Urological Associates, Columbia, South Carolina
BACKGROUND. There are minimal data on the influence of urinary symptoms and partici-pation in prostate cancer screening in African American men.METHODS. This correlational study examined the influence of urinary symptoms on 1)participation in a free prostate cancer screening program and 2) abnormal screening results.The 1,402 African American men in the South Carolina Prostate Cancer Project (SCPCP), meanage of 50 years, completed a survey that included self-reported urinary symptoms, partici-pated in a prostate cancer educational program, and received a free prostate cancer screeningconsisting of a digital rectal examination (DRE) and prostate-specific antigen (PSA) from theirpersonal physician.RESULTS. One in 5 men reported the presence of urinary symptoms. Over 60% of the 1,402men participated in the free CaP screening. Among the 852 men who participated in the freeprostate cancer screening, 73 (8.6%) had abnormal screening results as classified by abnormalDRE and/or PSA >4.0 ng/ml. Urinary symptoms were significant predictors, both of partici-pation in screening (OR = 1.30, CI = 1.00, 1.70) and of obtaining an abnormal screening result(OR = 1.78, CI = 1.17, 2.72).CONCLUSIONS. Prostate cancer health education needs to include the fact that prostatecancer, in its early stages, has no urinary symptoms. Prostate 37:215–222, 1998.© 1998 Wiley-Liss, Inc.
KEY WORDS: urinary symptoms; prostatic neoplasms; African American men; screen-ing
INTRODUCTION
Urinary symptoms that include frequency, ur-gency, weak urinary stream, dysuria, or hematuria areassociated with aging and can be symptomatic ofprostatism, benign prostatic hyperplasia (BPH), and/or prostate cancer [1–8]. In Olmsted County, Minne-sota, white men with urological symptoms were morelikely to seek medical care than men without urologi-cal symptoms [9]. However, there are minimal data onthe influence of urinary symptoms on participation inprostate cancer screening studies among AfricanAmerican men. This study examined the influence ofurinary symptoms on 1) participation in a free pros-
tate cancer screening program and 2) abnormalscreening results among men screened in a commu-nity-based cohort of 1,402 African American men.
The contents of this research are solely the responsibility of theauthors and do not necessarily represent the official views of theNational Cancer Institute.Contract grant sponsor: National Cancer Institute; Contract grantnumber: R01 CA60561-01.*Correspondence to: Sally P. Weinrich, College of Nursing, Univer-sity of South Carolina, Columbia, SC 29208. E-mail: [email protected] 5 January 1998; Accepted 17 June 1998
The Prostate 37:215–222 (1998)
© 1998 Wiley-Liss, Inc.

The prevalence of urinary symptoms reported incommunity-based screening programs varies widely.Forty-three percent of 1,105 African American menfrom community churches in Michigan had urinarysymptoms [10]. In contrast, most of the men (93%)reported urinary symptoms in the nationwide Pros-tate Cancer Awareness Week from 41 sites with1,000,000 men [11]. The 2,757 population-based whitemen in Olmsted County, Minnesota, reported urinarysymptoms that ranged from 5% (for pain or burning)to 40% (for dribbling) [1]. Fifty percent of men in twoother national prostate cancer screening studies reporturinary symptoms: half of the 1,695 men in the Ameri-can Cancer Society National Prostate Cancer DetectionProgram (ACS-NPCDP) [12,13], and 53% in a multi-center clinical trial with 6,630 men [14]. There is adirect relationship between age and urinary symp-toms, with an increase in urinary symptoms with in-creased age [2,11,15].
African American men have higher prostate cancerincidence rates than Caucasian men, i.e., 180.6 per100,000 African American men in comparison to 137.9per Caucasian 100,000 men, as well as higher mortalityrates, i.e., 53.7 per 100,000 African American men incomparison to 24.4 per 100,000 Caucasian men [16].Little is known about the reasons for participation inprostate cancer screening among African Americanmen due to the small percentage of African Americanmen who have participated in national prostate cancerscreening trials. Most prostate cancer studies includepredominately middle-income, educated Caucasianmen [17–21]. Less than 10% of the men participating inthe prostate, colorectal, lung, and ovarian cancerscreening (PLCO) trial of the National Cancer Institute[22] were African American.
MATERIALS AND METHODS
This correlational study examined the influence ofurinary symptoms on 1) participation in a free prostatecancer screening program and 2) abnormal screeningresults. It was part of a larger study, funded by the Na-tional Cancer Institute, to test educational interventionsfor recruitment of African American men into prostatecancer screening. Results concerning the educational hy-potheses are reported elsewhere [23].
Study Subjects
Prostate cancer educational programs were given at223 different community sites within 11 counties incentral South Carolina during 1994–1996. Communitysites, purposely selected based on their composition ofAfrican American and low-income men, includedwork sites, churches, housing projects, barber shops,
and National Association for Advancement of ColoredPeople (NAACP) meetings. A description of commu-nity recruitment strategies for the South CarolinaProstate Cancer Project (SCPCP) has been published[24].
Inclusion criteria were age of 40–70 years for Afri-can American men; no history of prostate cancer; nodiagnostic evaluation currently underway for prostatecancer; and informed consent. This study describes theimpact of urinary symptoms in 1,402 African Ameri-can men; 561 Caucasian men attended the communitysites but were deleted from the analyses due to thefocus on African American men and an insufficientnumber of men for race comparisons. Fifty-three menwho were seen at the community sites refused to par-ticipate in the study for reasons that ranged from‘‘routinely get prostate exam already’’ [8], to ‘‘no timefor exam’’ [3], to ‘‘refuse’’ [13]. A total of 1,406 AfricanAmerican men attended the community sites; 4 Afri-can American men were deleted from the analysesdue to incomplete data on income and self-reportedhealth status, leaving 1,402 African American men.
Data Collection and Analyses
After signing an informed consent, each man com-pleted a 20-min questionnaire. After completion of thequestionnaire, all men saw a slide-tape presentation onprostate cancer which covered statistics, risk factors,symptoms, and screening for prostate cancer, and whichcarried a positive message of, ‘‘If you don’t want to do itfor yourself, do it for the ones you love’’ [24]. The slide-tape show included the fact that urinary symptoms ofburning, frequency, and blood, and pain in back, groin,or testicles could be due to infection, benign prostatehyperplasia, or prostate cancer. It also stated that in theearly stages prostate cancer has no symptoms.
Each man was referred to his personal physician forprostate cancer screening that included a digital rectalexamination (DRE) and a prostate-specific antigen(PSA) test. Each physician was reimbursed $40 for per-forming the DRE and drawing blood for the PSA. AllPSAs were performed by a local laboratory using theHybritech Incorporated (Collegeville, PA) technique at acost of $12/PSA. Health providers for all men with ab-normal results were contacted to ensure that follow-up was obtained. Financial help for additional diag-nostic tests (i.e., ultrasound and biopsy) was obtainedfor low-income men who could not afford them [24].
The participants completed a self-administered,previously validated, 44-item questionnaire whichhad a readability level of grade 5 to aid in compre-hension. Questions that measured urinary symptoms,pain, demographics, previous prostate cancer screen-ing, and screening results are reported here. One ques-tion measured urinary symptoms: ‘‘Check all that you
216 Weinrich et al.

have had in the past 12 months: Problems with yoururine (for example, blood or pus in your urine, burn-ing with urination, get up often at night to urinate,urinate more often, or small stream of urine).’’ A sec-ond question measured pain: ‘‘Check all that you havehad in the past 12 months: Pain in lower back, hips,top part of legs, or in the area between the testicles andrectum.’’ If the participant indicated that he had any ofthese problems, the dichotomous prostate cancer(CaP) symptom variable was coded ‘‘yes.’’
The seven questions that measured demographics(age, ethnicity, education, income, marital status, andliving status) were adapted from an earlier study bythe first author [25]. The previous prostate cancerscreening variable was constructed from responses onwhether or not the participant had ever had a DREand/or PSA. All questions were asked before the ed-ucational program on prostate cancer screening wasgiven. The instrument for recording receipt of DREwas modified from the Prostate Cancer AwarenessWeek [26] and the National Prostate Cancer DetectionProgram [20]. Data on the DRE was sent to the Pros-tate Cancer Project by each individual physician. Proofof receipt of PSA and results were sent to the ProstateCancer Project by the laboratory company.
For all analyses, there were two outcomes: 1) par-ticipation in the free prostate cancer screening, and 2)normal or abnormal results among screened men. Theanswer (yes or no) to the self-reported urinary symp-toms was the primary independent variable. Covari-ates were age, education, income, marital status, self-reported health status, and previous prostate cancerscreening. Separate simple logistic regressions werefirst performed for each independent variable of inter-est, including age, in order to examine the relation-ships between urinary symptoms, the covariates, andeach of the two dependent variables (participation infree CaP screening and normal or abnormal resultsfrom screening). Multivariate multiple logistic regres-sion was then carried out using PROC CATMOD inthe SAS system [27]. This technique yields the sameresults as two separate ordinary multiple logistic re-gressions, plus an overall significance test to controlfor type I error. The independent variables included inthe univariate and multivariate models were urinarysymptoms and the covariates of age, education, in-come, marital status, self-reported health status, andprevious prostate cancer screening.
Odds ratios were estimated in the usual mannerfrom the logistic regression parameters [28]. An oddsratio (OR) of 1.00 indicates lack of association betweenthe independent variable and the outcome, and there-fore supports the null hypothesis. In contrast, an oddsratio statistically significantly greater than 1.00 sup-ports the hypothesis of increased risk of the outcome
(prostate cancer screening or abnormal screening re-sults), given the presence of the associated character-istic, which in this research is urinary symptoms.
RESULTS
Just over half (55%) of the 1,402 African Americanmen were age 40–49 years, about a third (31%) wereage 50–59 years, and the remaining 14% were age 60–70 years (Table I). They were evenly split among the
TABLE I. Description of African American Men,Prostate Cancer Project (n = 1,402)
Variables N %
DemographicsAge groups (mean age, 50 years)
40–49 years 767 54.750–59 years 443 31.660–70 years 192 13.7
EducationLess than high school graduate 439 31.3High school graduate 460 32.8Some college and above 503 35.9
Incomeø$9,600 per year 361 25.7ù$9,601 per year 1,041 74.3
Marital statusMarried 1,059 75.5Not married 343 24.5
Urinary symptomsYes 276 19.7No 1,126 80.3
Pain in back, groin, or upper thighsYes 428 30.5No 974 69.5
Previous CaP screeningPrevious DREYes 878 62.6No 524 37.4
Previous PSAYes 333 23.8No 1,069 76.2
Self-reported health statusExcellent 253 18.0Good 825 58.8Fair or poor 324 23.2
Participation in screeningYes 852 60.8No 550 39.2
Results of screeningNormal screen 779 91.4Abnormal screen
No follow-up 17 2.0Abnormal screen, follow-up, no cancer 37 4.4Prostate cancer diagnosis 19 2.2
Urinary Symptoms as a Predictor for Prostate Cancer Screening 217

three educational groups of less than high schoolgraduate, high school graduate, and some college andabove. Three fourths of the African American menwere married. One quarter (26%) had household in-comes of $9,600 per year or less.
As for previous history of prostate cancer screen-ing, 283 (33.2 %) of the men who were screened for thisstudy had never had prostate cancer screening (de-fined as DRE and/or PSA) in their lifetime. Amongthe men who did have previous history of screening,362 (63.6%) had not had CaP screening (defined as DREand/or PSA) within the last 12 months. Two hundredand ninety-eight (35.0 %) of the men who werescreened for this study had never had a DRE in theirlifetime. Among the men who did have previous his-tory of DRE screening, 365 (65.9%) had not had a DREwithin the last 12 months. Six hundred and fifty-eight(77.2 %) of the men who were screened for this studyhad never had a PSA in their lifetime. Among the menwho did have previous history of PSA screening, 110(56.7%) had not had a PSA within the last 12 months.
One in 5 subjects overall reported urinary symp-toms, and about 3 men in 10 reported back or hip pain(Table I). The percentage reporting urinary symptomsincreased with age, from 16.2% of men aged 40–49years, to 22.1% of men aged 50–59 years, and 28.1% ofmen aged 60–70 years. Self-reported health status was‘‘excellent’’ for just under 1 in 5, ‘‘good’’ for 3 in 5, and‘‘fair/poor’’ for a little more than 1 in 5 subjects. As forprevious prostate cancer screening, five eighths of themen had received a previous digital examination,though only about 1 in 4 reported a previous PSA test(Table I).
Over 60% of the men participated in the free CaPscreening (Table I). Abnormal screening results weredefined as men who had an abnormal DRE as definedby their personal physician and/or a PSA of 4.0 ng/mlor greater. There were 73 (8.6%) abnormal screeningresults out of 852 men screened. Twenty-three (31.5%)of these 73 men reported urinary symptoms, and 26(35.6%) reported pain symptoms. Twenty-eight(38.4%) out of the 73 men with abnormal screeningresults had a biopsy performed.
Diagnoses for men with abnormal screening resultsincluded 19 prostate cancers, 22 BPH, 6 prostatitis, and20 other diagnoses including elevated PSA. Six mencontinue to be followed. Among the 19 (2.2%) prostatecancers, 7 (36.8%) men reported urinary symptomsand 9 (47.4%) men reported pain symptoms.
Urinary Symptoms as a Predictor for Participationin Free CaP Screening and Abnormal Screening
Results
The univariate logistic regression results are shownin Table II. Urinary symptoms were significant pre-
dictors, both of participation in screening and of ob-taining an abnormal screening result. Pain in the back,groin, or upper thighs was not a significant predictorof either outcome.
Covariates that achieved significance in these uni-variate analyses for predicting participation wereolder age group (50–59 years), nonpoverty-levelhousehold income, being married, and having had aprevious DRE. There was a relationship between ageand participation in the free prostate cancer screening.Relative to the reference group (age 40–49 years), be-ing aged 50–59 years was statistically significantly as-sociated with greater participation (P < 0.05); beingaged 60–69 years was not.
For predicting an abnormal screen, significant vari-ates were age, educational level, and nonpoverty-levelincome. Men in the older age groups (both 50–59 and60–69 years) were more likely to have an abnormalscreen (P < 0.05). Men who reported an education ofsome college or higher were less likely to have anabnormal screen. In contrast, men with an income ofless than $9,600 per year were more likely to haveabnormal screening results. Previous PSA and self-reported health status were not significant predictorsfor either participation in the free prostate cancerscreening or abnormal screening results.
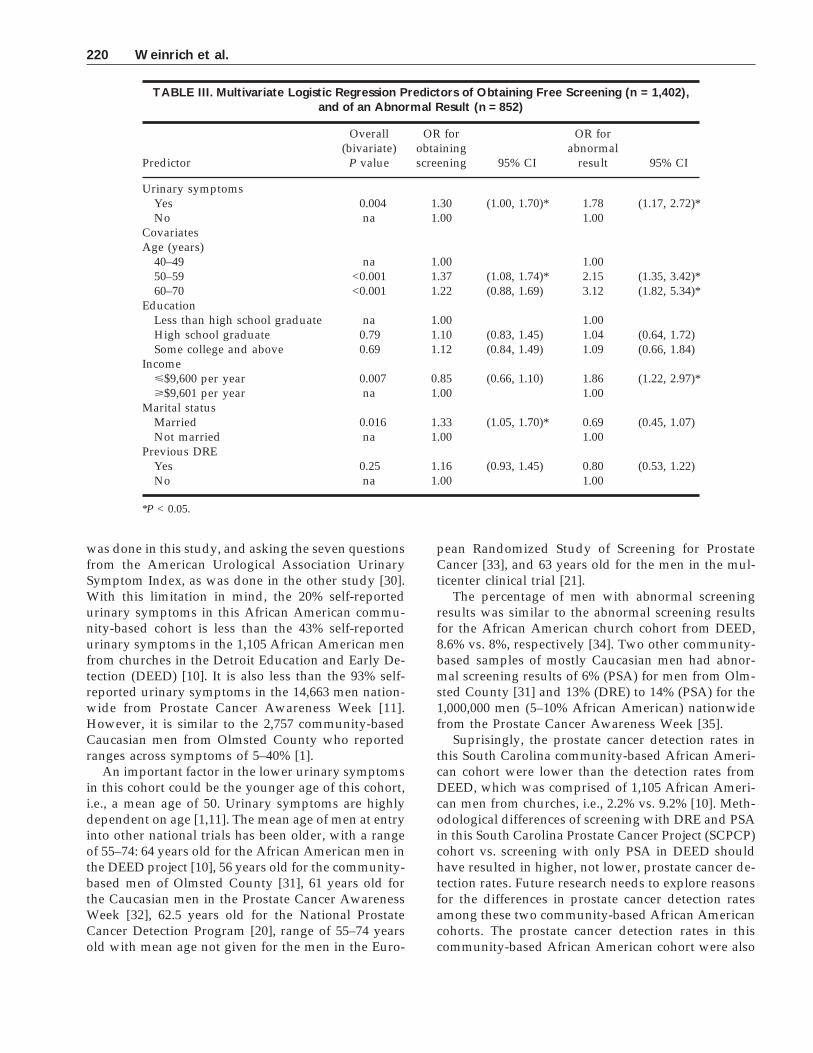
Results of the multivariate logistic regression areshown in Table III. The odds ratios and confidenceintervals (CIs) for urinary symptoms are consistentwith the results of the univariate analyses, i.e., pres-ence of urinary symptoms is associated with both par-ticipation in free CaP screening (OR = 1.30, CI = (1.00,1.70)) and with obtaining an abnormal screening result(OR = 1.78, CI = (1.17, 2.72)).
Comparisons of the odds ratios for screening par-ticipation associated with urinary symptoms in TablesII and III reveal that the introduction of the covariatescauses a modest reduction in the value of the oddsratio, from 1.46 to 1.30. Both values differ significantlyfrom the null value (1.00), and the length of the 95%confidence interval actually decreases in the presenceof the covariates. The odds ratio for abnormal screen-ing results actually increases from 1.73 to 1.78; whilethe length of the confidence interval increases, thelower confidence limit increases from 1.02 to 1.17(away from the null value).
For the covariates, the odds ratios for age, educa-tion, and income are all closer to the null value 1.00 inTable III (the multiple regression model) than theywere in Table II, where they were considered indi-vidually. Presumably, this is due to the multicollinear-ity of these variables. The pattern of statistically sig-nificant (P < 0.05) results is sparser than, but similar to,the pattern that was observed for the univariate analy-sis of the covariates. Age continues to be significant for
218 Weinrich et al.
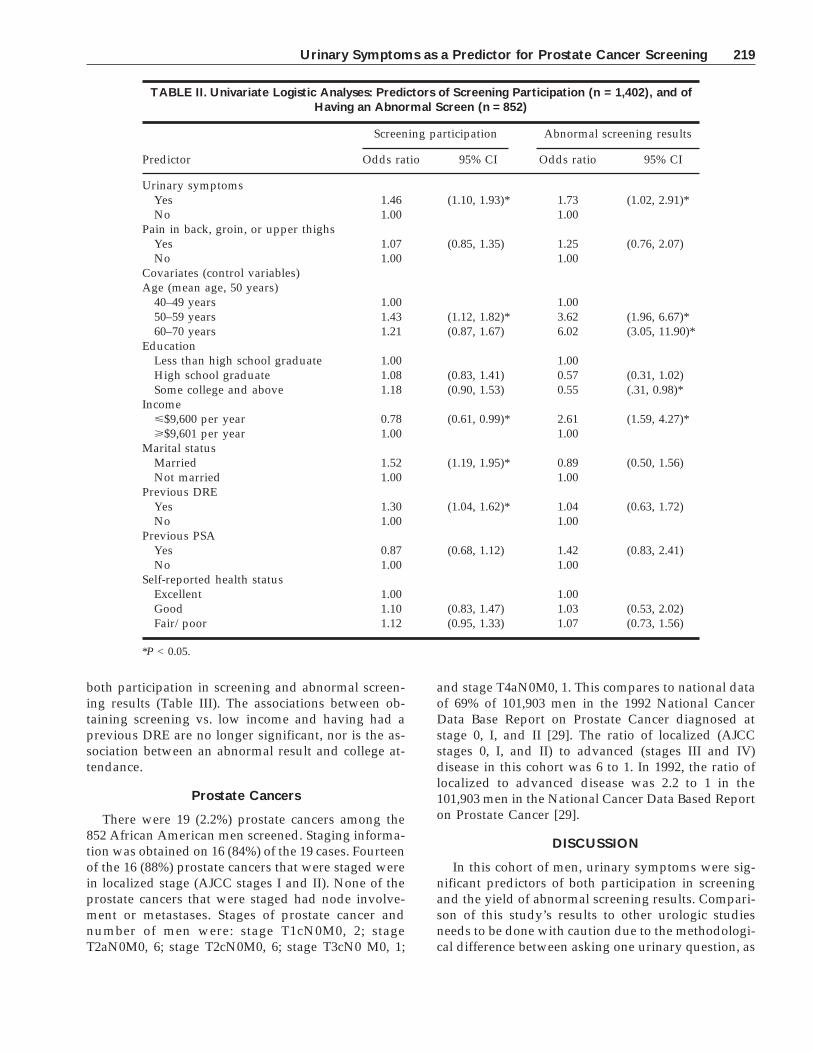
both participation in screening and abnormal screen-ing results (Table III). The associations between ob-taining screening vs. low income and having had aprevious DRE are no longer significant, nor is the as-sociation between an abnormal result and college at-tendance.
Prostate Cancers
There were 19 (2.2%) prostate cancers among the852 African American men screened. Staging informa-tion was obtained on 16 (84%) of the 19 cases. Fourteenof the 16 (88%) prostate cancers that were staged werein localized stage (AJCC stages I and II). None of theprostate cancers that were staged had node involve-ment or metastases. Stages of prostate cancer andnumber of men were: stage T1cN0M0, 2; stageT2aN0M0, 6; stage T2cN0M0, 6; stage T3cN0 M0, 1;
and stage T4aN0M0, 1. This compares to national dataof 69% of 101,903 men in the 1992 National CancerData Base Report on Prostate Cancer diagnosed atstage 0, I, and II [29]. The ratio of localized (AJCCstages 0, I, and II) to advanced (stages III and IV)disease in this cohort was 6 to 1. In 1992, the ratio oflocalized to advanced disease was 2.2 to 1 in the101,903 men in the National Cancer Data Based Reporton Prostate Cancer [29].
DISCUSSION
In this cohort of men, urinary symptoms were sig-nificant predictors of both participation in screeningand the yield of abnormal screening results. Compari-son of this study’s results to other urologic studiesneeds to be done with caution due to the methodologi-cal difference between asking one urinary question, as
TABLE II. Univariate Logistic Analyses: Predictors of Screening Participation (n = 1,402), and ofHaving an Abnormal Screen (n = 852)
Predictor
Screening participation Abnormal screening results
Odds ratio 95% CI Odds ratio 95% CI
Urinary symptomsYes 1.46 (1.10, 1.93)* 1.73 (1.02, 2.91)*No 1.00 1.00
Pain in back, groin, or upper thighsYes 1.07 (0.85, 1.35) 1.25 (0.76, 2.07)No 1.00 1.00
Covariates (control variables)Age (mean age, 50 years)
40–49 years 1.00 1.0050–59 years 1.43 (1.12, 1.82)* 3.62 (1.96, 6.67)*60–70 years 1.21 (0.87, 1.67) 6.02 (3.05, 11.90)*
EducationLess than high school graduate 1.00 1.00High school graduate 1.08 (0.83, 1.41) 0.57 (0.31, 1.02)Some college and above 1.18 (0.90, 1.53) 0.55 (.31, 0.98)*
Incomeø$9,600 per year 0.78 (0.61, 0.99)* 2.61 (1.59, 4.27)*ù$9,601 per year 1.00 1.00
Marital statusMarried 1.52 (1.19, 1.95)* 0.89 (0.50, 1.56)Not married 1.00 1.00
Previous DREYes 1.30 (1.04, 1.62)* 1.04 (0.63, 1.72)No 1.00 1.00
Previous PSAYes 0.87 (0.68, 1.12) 1.42 (0.83, 2.41)No 1.00 1.00
Self-reported health statusExcellent 1.00 1.00Good 1.10 (0.83, 1.47) 1.03 (0.53, 2.02)Fair/poor 1.12 (0.95, 1.33) 1.07 (0.73, 1.56)
*P < 0.05.
Urinary Symptoms as a Predictor for Prostate Cancer Screening 219
was done in this study, and asking the seven questionsfrom the American Urological Association UrinarySymptom Index, as was done in the other study [30].With this limitation in mind, the 20% self-reportedurinary symptoms in this African American commu-nity-based cohort is less than the 43% self-reportedurinary symptoms in the 1,105 African American menfrom churches in the Detroit Education and Early De-tection (DEED) [10]. It is also less than the 93% self-reported urinary symptoms in the 14,663 men nation-wide from Prostate Cancer Awareness Week [11].However, it is similar to the 2,757 community-basedCaucasian men from Olmsted County who reportedranges across symptoms of 5–40% [1].
An important factor in the lower urinary symptomsin this cohort could be the younger age of this cohort,i.e., a mean age of 50. Urinary symptoms are highlydependent on age [1,11]. The mean age of men at entryinto other national trials has been older, with a rangeof 55–74: 64 years old for the African American men inthe DEED project [10], 56 years old for the community-based men of Olmsted County [31], 61 years old forthe Caucasian men in the Prostate Cancer AwarenessWeek [32], 62.5 years old for the National ProstateCancer Detection Program [20], range of 55–74 yearsold with mean age not given for the men in the Euro-
pean Randomized Study of Screening for ProstateCancer [33], and 63 years old for the men in the mul-ticenter clinical trial [21].
The percentage of men with abnormal screeningresults was similar to the abnormal screening resultsfor the African American church cohort from DEED,8.6% vs. 8%, respectively [34]. Two other community-based samples of mostly Caucasian men had abnor-mal screening results of 6% (PSA) for men from Olm-sted County [31] and 13% (DRE) to 14% (PSA) for the1,000,000 men (5–10% African American) nationwidefrom the Prostate Cancer Awareness Week [35].
Suprisingly, the prostate cancer detection rates inthis South Carolina community-based African Ameri-can cohort were lower than the detection rates fromDEED, which was comprised of 1,105 African Ameri-can men from churches, i.e., 2.2% vs. 9.2% [10]. Meth-odological differences of screening with DRE and PSAin this South Carolina Prostate Cancer Project (SCPCP)cohort vs. screening with only PSA in DEED shouldhave resulted in higher, not lower, prostate cancer de-tection rates. Future research needs to explore reasonsfor the differences in prostate cancer detection ratesamong these two community-based African Americancohorts. The prostate cancer detection rates in thiscommunity-based African American cohort were also
TABLE III. Multivariate Logistic Regression Predictors of Obtaining Free Screening (n = 1,402),and of an Abnormal Result (n = 852)
Predictor
Overall(bivariate)
P value
OR forobtainingscreening 95% CI
OR forabnormal
result 95% CI
Urinary symptomsYes 0.004 1.30 (1.00, 1.70)* 1.78 (1.17, 2.72)*No na 1.00 1.00
CovariatesAge (years)
40–49 na 1.00 1.0050–59 <0.001 1.37 (1.08, 1.74)* 2.15 (1.35, 3.42)*60–70 <0.001 1.22 (0.88, 1.69) 3.12 (1.82, 5.34)*
EducationLess than high school graduate na 1.00 1.00High school graduate 0.79 1.10 (0.83, 1.45) 1.04 (0.64, 1.72)Some college and above 0.69 1.12 (0.84, 1.49) 1.09 (0.66, 1.84)
Incomeø$9,600 per year 0.007 0.85 (0.66, 1.10) 1.86 (1.22, 2.97)*ù$9,601 per year na 1.00 1.00
Marital statusMarried 0.016 1.33 (1.05, 1.70)* 0.69 (0.45, 1.07)Not married na 1.00 1.00
Previous DREYes 0.25 1.16 (0.93, 1.45) 0.80 (0.53, 1.22)No na 1.00 1.00
*P < 0.05.
220 Weinrich et al.

lower than the cancer detection rates in the 50,000community-based men nationwide from Prostate Can-cer Awareness Week, i.e., 2.2% vs. 4.7% [19]. Prostatecancer detection rates in other national trials rangefrom 3–10%: 5.4% (first year) or 8.9% (cumulative),ACS-NPCDP of 2,999 men with DRE, PSA, and TRUSscreening [36]; 3.2–3.6%, European Randomized Studyof Screening for Prostate Cancer of 18,595 men [33];5.8%, multicenter clinical trial of 6,630 men [21]; 2.6%for 1,249 men with PSA screening in Washington [17];and 5.7% for 1,002 men with PSA screening in Quebec[37].
The greatest percentage of prostate cancers was de-tected on the first or second screening in the nation-wide Prostate Cancer Awareness Week [19] as well asin the National Prostate Cancer Detection Program[36]. This South Carolina Prostate Cancer Project co-hort of men was comprised of 37% who had not had aDRE had in their lifetime and 76% who had not had aPSA in their lifetime. Among the men who had beenscreened previously, 63% had not had a DRE in thelast 12 months and 53% had not had a PSA in the last12 months.
Racial differences with higher prostate cancer ratesin African Americans have been attributed to socio-economic differences [38]. However, few low-incomeAfrican Americans are represented in published pros-tate cancer screening studies. A strength of the presentcohort is its representation of lower socioeconomiclevel African Americans. Thirty-one percent of themen had less than a high school graduation education,and 26% of the men had household incomes less than$9,600 per year.
CONCLUSIONS
Urinary symptoms were a predictor of both partici-pation in free prostate cancer screening and abnormalscreening results in this cohort of 1,402 community-based African American men. Two caveats regardingthis study need to be discussed: 1) Results can be gen-eralized only to Southern states with men who aresimilar to the African American men in this study. 2)Urinary symptoms were measured with only onequestion rather than the complete American Urologi-cal Association Symptom Index [30]. Our sample ofcommunity-based African American men is strength-ened by its inclusion of low-income men, and pro-vides valuable information.
Additional research on African American men andprostate cancer is needed [39]. Prostate cancer mortal-ity rates have shown a recent decline; however, thisdecline is less among African American men [39]. Fu-ture research needs to target African American men[40].
REFERENCES
1. Chute CG, Panser LA, Girman CJ, Oesterling JE, Guess HA,Jacobsen SJ, Lieber MM: The prevalence of prostatism: A popu-lation-based survey of urinary symptoms. J Urol 1993;150:85–89.
2. Girman CJ, Jacobsen SJ, Guess HA, Oesterling JE, Chute CG,Panser LA, Lieber MM: Natural history of prostatism: Relation-ship among systems, prostate volume and peak urinary flowrate. J Urol 1995;153:1510–1515.
3. Guess HA, Arrigihi HM, Metter EJ, Forzard JL: Cumulativeprevalence of prostatism matches the autopsy prevalence of be-nign prostatic hyperplasia. Prostate 1990;17:241–246.
4. Hunter DJ, Berra-Unamuno A, Martin-Gordo A: Prevalence ofurinary symptoms and other urological conditions in Spanishmen 50 years of age or older. J Urol 1996;155:1965–1970.
5. Moon TD, Brannan W, Stone NN, Ercole C, Crawford ED, Cho-dak G, Brawer M, Heisey D, Bruskewitz RC: Effect of age, ed-ucational status, ethnicity and geographic location on prostatesymptom scores. J Urol 1994;152:1498–1500.
6. Sagnier PP, MacFarlane G, Richard F, Botto H, Teillac P, BoyleP: Results of an epidemiological survey using a modifiedAmerican Urological Association Symptom Index for benignprostatic hyperplasia in France. J Urol 1994;151:1266–1270.
7. Sagnier PP, MacFarlane G, Teillac P, Botto H, Richard F, BoyleP: Impact of symptoms of prostatism on level of bother andquality of life in the French community. J Urol 1995;669–673.
8. Tsukamoto T, Kumamoto Y, Masumori, N, Miyake H, RhodesT, Girman CJ, Guess HA, Jacobsen SJ, Lieber MM: Prevalence ofprostatism in Japanese men in a community-based study withcomparison to a similar American study. J Urol 1995;51:391–395.
9. Jacobsen SJ, Girman CJ, Guess HA, Panser LA, Chute CG, Oes-terling JE, Lieber MM: Do prostate size and urinary flow ratespredict health care-seeking behavior for urinary symptoms inmen? Urology 1995;45:64–69.
10. Powell IJ, Heilbrun L, Litturp PL, Franklin A, Parzuchowski J,Gelfand D, Sakr W: Outcome of African American men screenedfor prostate cancer: The Detroit Education and Early DetectionStudy. J Urol 1997;158:146–149.
11. Stenner J, DeAntoni EP, O’Donnell C, Stone NN, McLeod DG,Crawford ED: Prevalence and natural history of urinary symp-toms in a longitudinal national prostate cancer screening (com-munity-based) study. Prostate Cancer Prostatic Dis, in press.
12. Kane R, Littrup P, Babaian R, Drago JR, Less F, Chesley A,Murphy GP, Mettlin C: Prostate-specific antigen levels in 1695men without evidence of prostate cancer. Cancer 1992;69:1201–1207.
13. Mettlin C, Murphy GP, Babian RJ, Chesley A, Kane RA, LittrupPJ, Mostofi FK, Ray PS, Shanberg AM, Toi A: The results of afive-year early prostate cancer detection intervention. Cancer1996;77:150–159.
14. Catalona W, Richie J, Ahmann F, Hudson MA, Scardino PT,Flanigan RC, deKernion JB, Ratliff TL, Kavoussi LR, Dalkin BL:Comparison of digital rectal examination and serum prostatespecific antigen in the early detection of prostate cancer: Resultsof a multicenter clinical trial of 6,630 men. J Urol 1994;151:1283–1290.
15. Richardson TD, Oesterling JE: Age-specific reference ranges forserum prostate specific antigen. Urol Clin North Am 1997;24:339–351.
16. Kosary CL, Reis LA, Miller BA, Hankey BF, Harras A, EdwardsBK: ‘‘SEER Cancer Statistics Review, 1973–1992: Tables andGraphs.’’ National Cancer Institute, 1995.
17. Brawer MK, Chetner MP, Beatie J, Buchner DM, Vessella RL,Lange PH: Screening for prostatic carcinoma with prostate spe-cific antigen. J Urol 1992;147:841–845.
Urinary Symptoms as a Predictor for Prostate Cancer Screening 221

18. Catalona WJ, Smith DJ, Ratliff T, Dodds KM, Coplen DE, YuanJJ, Petros JA, Andriole GL: Measurement of prostate-specificantigen in serum as a screening test for prostate cancer. N EnglJ Med 1991;324:1156–1161.
19. DeAntoni EP: Eight years of ‘‘Prostate Cancer AwarenessWeek.’’ Cancer 1997;80:1845–1851.
20. Mettlin C, Lee F, Drago J, Murphy GP: The American CancerSociety National Prostate Cancer Detection Project. Findings onthe detection of early prostate cancer in 2425 men. Cancer 1991;67:2949–2958.
21. Catalona W, Richie J, Ahmann F, Hudson MA, Scardino PT,Flanigan RC, deKernion JB, Ratliff TL, Kavoussi LR, Dalkin BL:Comparison of digital rectal examination and serum prostatespecific antigen in the early detection of prostate cancer: Resultsof a multicenter clinical trial of 6,630 men. J Urol 1994;151:1283–1290.
22. Gohagan JK, Prorok PC, Kramer BS, Hayes RB, Cornett JE: Theprostate, lung, colorectal, and ovarian screening trial of the Na-tional Cancer Institute. Cancer 1994;152:1905–1909.
23. Weinrich SP, Weinrich MC, Boyd MD, Mettlin C: Increasingprostate cancer screening in African American men with peereducator and client navigator educational interventions. J Can-cer Edu, in press.
24. Weinrich SP, Boyd MD, Bradford D, Mossa MS, Weinrich M:Recruitment of African-American men into prostate cancerscreening. Cancer Pract 1998;6:23–30.
25. Weinrich SP, Weinrich MC, Stromborg MF, Boyd MD, WeissHL: Using elderly educators to increase colorectal cancer screen-ing. Gerontologist 1993;33:491–496.
26. DeAntoni EP, Crawford ED: Prostate Cancer Awareness Week.Cancer Suppl 1995;75:1874-1879.
27. SAS Institute, Inc.: ‘‘SAS/STAT User’s Guide, Version 6, FourthEdition.’’ Cary, NC: SAS Institute, Inc., 1989.
28. Mausner J, Kramer S: ‘‘Mausner and Bahn Epidemiology—AnIntroductory Text.’’ Philadelphia: W.B. Saunders Company,1985.
29. Mettlin CJ, Murphy GP, McGinnis LS, Menck HR: The NationalCancer Data Base report on prostate cancer. American Collegeof Surgeons Commission on Cancer and the American CancerSociety. Cancer 1995;76:1104–1112.
30. Barry MJ, Fowler FJ Jr, O’Leary MP, Bruskewitz RC, HoltgreweHL, Mebust WK, Cockett AT: The American Urological Asso-ciation Symptom Index for benign prostatic hyperplasia. TheMeasurement Committee of the American Urological Associa-tion. J Urol 1992;148:1549–1557.
31. Oesterling JE, Jacobsen SJ, Chute CG, Guess HA, Girman CJ,Panser LA, Leiber MM: Serum prostate-specific antigen in acommunity-based population of healthy men. Establishment ofage-specific reference ranges. JAMA 1993;270:860–864.
32. DeAntoni EP, Crawford ED, Oesterling JE, Ross CA, Berger ER,McLeod DG, Staggers F, Stone NN: Age- and race-specific ref-erence ranges for prostate-specific antigen from a large commu-nity-based study. Urology 1996;48:234–239.
33. Schroder FH, Denis LJ, Kirkels W, deKoning HJ, Standaert B:European randomized study of screening for prostate cancer.Progress report of Antwerp and Rotterdam pilot studies. Cancer1995;76:129–134.
34. Powell IJ, Gelfand DE, Parzuchowski J, Heilburn L, Franklin A:A successful recruitment process of African American men forearly detection of prostate cancer. Cancer 1995;75:1880–1884.
35. Stone NN, DeAntoni EP, Crawford ED, Prostate Cancer Educa-tion Council: Screening for prostate cancer by digital rectal ex-amination and prostate-specific antigen: Results of ProstateCancer Awareness Week, 1989–1992. Urol Symp 1994;44:18–25.
36. Mettlin C: Early detection of prostate cancer following repeatedexaminations by multiple modalities: Results of the AmericanCancer Society National Prostate Cancer Detection Project. ClinInvest Med 1993;16:440–447.
37. Labrie F, Dupont A, Suburu R, Cusan L, Tremblay M, Gomez JL,Emond J: Serum prostate specific antigen as pre-screening testfor prostate cancer. J Urol 1992;147:846–852.
38. Vijayakumar S, Weichselbaum R, Vaida F, Dale W, Hellman S:Prostate-specific antigen levels in African Americans correlatewith insurance status as an indicator of socioeconomic status.Cancer J Sci Am 1996;2:225–233.
39. Mettlin C, Murphy G: Why is the U.S. prostate cancer death ratedeclining? Cancer 1998;82:249–251.
40. Eyre H, Feldman G: Status report on prostate cancer in AfricanAmericans: a national blueprint for action. CA 1998;48:315–319.
222 Weinrich et al.