Embed Size (px)
Citation preview

Urinalysis: A Comprehensive ReviewJEFF A. SIMERVILLE, M.D., WILLIAM C. MAXTED, M.D., and JOHN L PAHIRA, M.D.Georgetown Utiiversity School of Medicine, Washington, D.C.
A complete urinalysis includes physical, chemical, and microscopic examinations. Midstreamclean collection is acceptable in most situations, but tbe specimen sbould be examined withintwo hours of collection. Cloudy urine often is a result of precipitated phosphate crystals in alka-line urine, but pyuria also can be tbe cause. A strong odor may be the resuh of a concentratedspecimen rather than a urinary tract infection. Dipstick urinalysis is convenient, but false-posi-tive and false-negative results can occur. Specific gravity provides a reliable assessment of thepatient's hydration status. Microhematuria has a range of causes, from benign to life tbreatening.Glomerular, renal, and urologic causes of microbematuria often can be differentiated by otberelements of the urinalysis. Although transient proteijiuria typically is a henign condition, persis-tent proteinuria requires further work-up. Uncomplicated urinary tract infections diagnosed bypositive leukocyte esterase and nitrite tests can be treated without culture. {Am Fam Physician2005;71:1153-62. Copyright© 2005 American Academy of Family Physicians.)
Seepage 1046 forstrength-of-fecommenda-tion labels. Urinalysis is invaluable in the
diagnosis of urologic conditionssuch as calculi, urinary tractinfection (UTI), and malig-
nancy. It also can alert the physician to thepresence of systemic disease affecting thekidneys. Although urinalysis is not recom-mended as a routine screening tool exceptin women who may be pregnant, physiciansshould know how to interpret urinalysisresults correctly. This article reviews thecorrect method for performing urinalysisand the differential diagnosis for severalabnormal results.
Specimen CollectionA midstream clean-catch technique usuallyis adequate in men and women. Althoughprior cleansing of the external genitaliaoften is recommended in women, it has noproven benefit. In fact, a recent study' foundthat contamination rates were similar inspecimens obtained with and without priorcleansing (32 versus 29 percent). Urine mustbe refrigerated if it cannot be examinedpromptly; delays of more than two hoursbetween collection and examination oftencause unreliable results.^
Physical Properties: Color and OdorFoods, medications, metabolic products,and infection can cause abnormal urine col-
ors (Table 1).^ Cloudy urine often is a resultof precipitated phosphate crystals in alkalineurine, but pyuria also can be the cause.
The normal odor of urine is described asurinoid; this odor can be strong in concen-trated specimens but does not imply infec-tion. Diabetic ketoacidosis can cause urineto have a fruity or sweet odor, and alkalinefermentation can cause an ammoniacal odorafter prolonged bladder retention. Personswith UTIs often have urine with a pungentodor. Other causes of abnormal odors includegastrointestinal-bladder fistulas (associatedwith a fecal smell), cystine decomposition(associated with a sulfuric smell), and medi-cations and diet (e.g., asparagus).
Dipstick UrinalysisFalse-positive and false-negative results arenot unusual in dipstick urinalysis (Table 2).The accuracy of this test in detecting micro-scopic hematuria, significant proteinuria,and UTI is summarized in Table 3.'*"'̂
SPECIFIC GRAVITY
Urinary specific gravity (USG) correlateswith urine osmolality and gives importantinsight into the patient's hydration status. Italso reflects the concentrating ability of thekidneys. Normal USG can range from 1.003to 1.030; a value of less than 1.010 indicatesrelative hydration, and a value greater than
March 15, 2005 * Volume 71, Number 6 www.aafp.org/afp American Family Physician 1153

Strength of Recommendations
Key dinicai recommendation Label References
Patients with dipstick results of 3+ or greater may have significant proteinuria; further work-up isindicated.
Patients with microscopic hematuria (i.e., at least three red blood cells per high-power field in twoof three specimens) should be evaluated to exclude renal and urinary tract disease.
Exercise-induced hematuria is s relatively common, self-limited, and benign condition. Becauseresults of repeat urinalysis after 48 to 72 hours should be negative in patients with thiscondition, extended testing is not warranted.
A = cons/stent, good-quality patient-oriented evidence: B = inconsistent or limited-quality patient-oriented eviderxie: C = consensus, disease-orientedevidence, usual practice, opinion, or case series. Seepage 1046 for more information.
B
C
C
5
19,20
30
1.020 indicates relative dehydration.'* Increased USG isassociated with glycosuria and the syndrome of inappro-priate antidiuretic hormone; decreased USG is associatedwith diuretic use, diabetes insipidus, adrenal insuffi-ciency, aldosteronism, and impaired renal function.''* Inpatients with intrinsic renal insufficiency, USG is fixed at1.010—the specific gravity of the glomerular filtrate.
URINARY PH
Urinary pH can range from 4.5 to 8 but normally isslightly acidic (i.e., 5.5 to 6.5) because of metabolic activ-ity. Ingestion of proteins and acidic fruits (e.g., cranber-ries) can cause acidic urine, and diets high in citrate can
cause alkaline urine.'^ '̂ Urinary pH generally reflects theserum pH, except in patients with renal tubular acidosis(RTA). The inability to acidify urine to a pH of less than5.5 despite an overnight fast and administration of anacid load is the hallmark of RTA. In type I (distal) RTA,the serum is acidic but the urine is alkaline, secondaryto an inability to secrete protons into the urine. Type Ii(proximal) RTA is characterized by an inability to reab-sorb bicarbonate. This situation initially results in alkalineurine, but as the filtered load of bicarbonate decreases,the urine becomes more acidic.
Determination of urinary pH is useful in the diag-nosis and management of UTIs and calculi. Alkaline
TABLE 1
Common Causes of Abnormal Urine Coloration
Color Pathologic causes Food and drug causes
Cloudy
Brown
Orange
Red
Yellow
Phosphaturia, pyuria, chyluria, lipiduria,hyperoxaluria
Bite pigments, myoglobin
Brownish-black Bile pigments, melanin, mefhemoglobin
Green or blue Pseudomonal UTI, biliverdin
Bile pigments
Hematuria, hemoglobinuria, myoglobinuria,porphyria
Concentrated urine
Diet high in purine-rich foods (hyperuricosuria)
Fava beansLevodopa (Larodopa), metronidazole (Flagyl), nitrofurantoin
(Furadantin), some antimalarial agents
Cascara, levodopa, methyldopa (Aldomet), senna
Amitriptyline (Elavil), indigo carmine, IV cimetidine (Tagamet),IV promethazine (Phenergan), methylene blue, triamterene(Dyrenium)
Phenothiazines, phenazopyridine (Pyridium)
Beets, blackberries, rhubarbPhenolphthalein, rifampin (Rifadin)
CarrotsCascara
UTI = urinary tract infection; IV = intravenous.
Adapted with permission from Hanno PM, WeinAJ, Malkowicz SB. Clinical manual of urology. 3d ed. New York: McGraw-Hill, 2001:75
1 1 5 4 American Family Physician www.aafp.org/afp Volume 71, Number 6 • March 15, 2005

Urinalysis
TABLE 2
Causes of False-Positive and False-Negative Urinalysis Results
Dipstick test False positive False negative
Bilirubin Phenazopyridine (Pyridium)
Blood Dehydration, exercise, hemoglobinuria,menstrual blood, myoglobinuria
Glucose Ketones, levodopa (Larodopa)
Ketones Acidic urine, elevated specific gravity, mesna(Mesnex), phenolphthalein, some drug
metabolites (e.g., levodopa)Leukocyte Contamination
esterase
Nitrites Contamination, exposure of dipstick to air,phenazopyridine
Protein Alkaline or concentrated urine, phenazopyridine,
quaternary ammonia compounds
Specific gravity* Dextran solutions, IV radiopaque dyes, proteinuria
Urobilinogen Elevated nitrite levels, phenazopyridine
Chlorpromazine (Thorazine), selenium
Captoprii (Capoten), elevated specific gravity, pH < 5.1,proteinuria, vitamin C
Elevated specific gravity, uric acid, vitamin C
Delay in examination of urine
Elevated specific gravity, glycosuria, ketonuria, proteinuria,some oxidizing drugs (cephalexin [Keflex], nitrofurantoin[Furadantin], tetracycline, gentamicin), vitamin C
Elevated specific gravity, elevated urobilinogen levels,nitrate reductase-negative bacteria, pH < 6.0, vitamin C
Acidic or dilute urine, primary protein is not albumin
Alkaline urine
IV = intravenous.
*—False-positive results are caused by false elevation; false-negative results are caused by false depression.
TABLE 3
Accuracy of Urinalysis for Disease Detection
Condition
Microscopichematuria''
Significantproteinuria^
Culture-confirmedLJJ|6-73
Test
Dipstick
Dipstick
Dipstick
Micr05Copy
Results
a 1+ blood
2 3+ protein
Abnormal leukocyteesterase
Abnormal nitrites
Abnormal leukocyteesterase or nitrites
2 3+ protein
a 1+ blood
Any of the aboveabnormalities
> 5 WBCs per HPF
> 5 RBCs per HPF
Bacteria (any amount)
Sensitivity (%)
91 to 100
96
72 to 97
19 to 48
46 to 100
63 to 83
68 to 92
94 to 100
90 to 96
18 to 44
46 to 58
Specificity {%)
65 to 99
87
41 to 86
92 to 100
42 to 98
50 to 53
42 to 46
14 to 26
47 to 50
88 to 89
89 to 94
PPV
NA
NA
43 to 56
50 to 83
52 to 68
53
51
44
56 to 59
27
54 to 88
NPV
NA
NA
82 to 91
70 to 88
78 to 98
82
88
100
83 to 95
82
77 to 86
PPV = positive predictive value: NPV = negative predictive value; NA = not appiicable; UTI = urinary tract infection; WBCs = white biood cells;HPF = high-powered field; RBCs = red biood cells.
Information from references 4 through 13.
March !5, 2005 * Volume 71, Number 6 www.aafp.org/afp American Family Physician 1155

TABLE 4
Common Causes of Hematuria
Glomerular causes
Familial causes
Fabry's disease
Hereditary nephritis (Alport's syndrome)
Nail-patella syndrome
Thin basement-membrane disease
Primary glomeruionephritis
Focal segmental glomerulonephritis
Goodpasture's disease
Henoch-Schonlein purpura
IgA nephropathy (Berger's disease)
Mesangioproliferative glomeruionephritis
Postinfectious glomerulonephritis
Rapidly progressive glomerutonephritis
Secondary glomerulonephritis
Hemolytic-uremic syndrome
Systemic lupus nephritis
Thrombotic thrombocytopenic purpura
Vascutitis
Renal causes
Arteriovenous malformation
Hypercaiciuria
Hyperuricosuria
Loin pain-hematuria syndrome
Malignant hypertension
Medullary sponge kidney
Metabolic causes
Papillary necrosis
Polycystic kidney disease
Renal artery embolism
Renal vein thrombosis
Sickle cell disease or trait
Tubulointerstitiai causes
Vascular cause
Urologic causes
Benign prostatic hyperplasia
Cancer (kidney, ureteral, bladder.prostate, and urethral)
Cystitis/pyelonephritis
Nephrolithiasis
Prostatitis
Schistosoma haematobium infection
Tuberculosis
Other causes
Drugs (e.g., NSAIDs, heparin.
warfarin [Coumadin],cyclophosphamide [Cytoxan])
Trauma (e.g., contact sports,running, Foley catheter)
NSAIDs - nonsteroidal anti-inflammatory drugs.
Adapted with permission from Ahmed Z. Lee J. Asymptomatic urinary abnormalities. Hematuria and proteinuria. Med Clin North Am 7997,5/ 644.
urine in a patient with a UTI suggests the presence of aurea-splitting organism, which may be associated withmagnesium-ammonium phosphate crystals and canform staghorn calculi. Uric acid calculi are associatedwith acidic urine.
HEMATURIA
According to the American Urological Association, thepresence of three or more red blood cells (RBCs) perhigh-powered field (HPF) in two of three urine samplesis the generally accepted definition of hematuria.'^'" Thedipstick test for blood detects the peroxidase activityof erythrocytes. However, myoglobin and hemoglobinalso will catalyze this reaction, so a positive test resultmay indicate hematuria, myoglobinuria, or hemoglobin-uria. Visualization of intact erythrocytes on microscopicexamination of the urinary sediment can distinguishhematuria from other conditions. Microscopic exami-nation also may detect RBC casts or dysmorphic RBCs.Hematuria is divided into glomerular, renal (i.e., nonglo-merular), and urologic etiologies (Table 4).^^
Glomerular Hematuria. Glomerular hematuria typi-cally is associated with significant proteinuria, erythro-
cyte casts, and dysmorphic RBCs. However, 20 percentof patients with biopsy-proven glomerulonephritispresent with hematuria alone." IgA nephropathy (i.e.,Berger's disease) is the most common cause of glomeru-lar hematuria.
Renal (Nonglonierular) Hematuria. Nonglomerularhematuria is secondary to tubulointerstitiai, renovascu-lar, or metabolic disorders. Like glomerular hematuria, itoften is associated with significant proteinuria; however,there are no associated dysmorphic RBCs or erythrocytecasts. Further evaluation of patients with glomerularand nonglomerular hematuria should include determi-nation of renal function and 24-hour urinary protein orspot urinary protein-creatinine ratio.
Urologic Hematuria. Urologic causes of hematuriainclude tumors, calculi, and infections. Urologic hematu-ria is distinguished from other etiologies by the absenceof proteinuria, dysmorphic RBCs, and erythrocyte casts.Even significant hematuria will not elevate the proteinconcentration to the 2+ to 3+ range on the dipstick test.̂ ^Up to 20 percent of patients with gross hematuria haveurinary tract malignancy; a full work-up with cystoscopyand upper-tract imaging is indicated in patients with this
1156 American Family Physician www. aafp.org/a fp Volume 71 Number 6 * March 15, 2005

Urjnalysis
TABLE 5
Common Causes of Proteinuria
Transient proteinuria
Congestive heart failure
Dehydration
Emotionai stress
Exercise
Fever
Orthostatic (postural) proteinuria
Seizures
Persistent proteinuria
Primary glomerular causes
Focal segmental glomeruionephritis
IgA nephropathy (i.e., Berger's disease)
IgM nephropathy
Membranoproliferative glomeruionephritis
Membranous nephropathy
Minimal change disease
Secondary glomerular causes
Alport's syndrome
Amyloidosis
Collagen vascular diseases(e.g., systemic lupus erythematosus)
Diabetes mellitus
Drugs (e.g., NSAIDs, penicillamine[Cupriminel, gold, ACF inhibitors)
Fabry's disease
Infections (e.g., HIV, syphilis, hepatitis,post-streptococcal infection)
Malignancies (e.g., lymphoma, solidtumors)
Sarcoidosis
Sickle cell disease
Tubular causes
Aminoaciduria
Drugs (e.g., NSAIDs,antibiotics)
Fanconi syndrome
Heavy metal ingestion
Hypertensive nephrosclerosis
Interstitial nephritis
Overflow causes
Hemoglobinuria
Multiple myeloma
Myoglobinuria
NSAIDs = nonsteroidal anti-inflammatory drugs; ACE = ar]giotensin-converting enzyme; HIV = human immunodeficiency virus.
Adapted with permission from Ahmed Z. LeeJ. Asymptomatic urinary abnormalities. Hematuria and proteinuria. Med Clin North Am 1997;81:650.
condition.-'' In patients with asymptomatic microscopichematuria (without proteinuria or pyuria), 5 to 22 per-cent have serious urologic disease, and 0.5 to 5 percenthave a genitourinary malignancy.^^ ^̂
Exercise-induced hematuria is a relatively common,benign condition that often is associated with long-distance running. Results of repeat urinalysis after48 to 72 hours should be negative in patients with thiscondition.'"
PROTEINURIA
In healthy persons, the glomerular capillary wall is per-meable only to substances with a molecular weight ofless than 20,000 Daltons. Once filtered, low-molecuiar-weight proteins are reabsorbed and metabolized by theproximal tubule cells. Normal urinary proteins includealbumin, serum globulins, and proteins secreted bythe nephron. Proteinuria is defined as urinary proteinexcretion of more than 150 mg per day {10 to 20 mgper dL) and is the hallmark of renal disease. Microal-buminuria is defined as the excretion of 30 to 150 mgof protein per day and is a sign of early renal disease,particularly in diabetic patients.
The reagent on most dipstick tests is sensitive to albu-min but may not detect low concentrations of y-globu-lins and Bence Jones proteins. Dipstick tests for trace
amounts of protein yield positive results at concentra-tions of 5 to 10 mg per dL—lower than the threshold forclinically significant proteinuria.'"^ A result of 1+ cor-responds to approximately 30 mg of protein per dL andis considered positive; 2+ corresponds to 100 mg per dL,3+ to 300 mg per dL, and 4+ to 1,000 mg per dL.-*''̂ ^Dipstick urinalysis reliably can predict albuminuria withsensitivities and specificities of greater than 99 percent.''Asymptomatic proteinuria is associated with significantrenal disease in less than L5 percent of patients.*-^'
Proteinuria can be classified as transient or persistent(Table 5).-' In transient proteinuria, a temporary changein glomerular hemodynamics causes the protein excess;these conditions follow a benign, self-limited course.'''•^^Orthostatic (postural) proteinuria is a benign conditionthat can result from prolonged standing; it is confirmedby obtaining a negative urinalysis result after eight hoursof recumbency.
Persistent proteinuria is divided into three generalcategories: glomerular, tubular, and overflow. In glo-merular proteinuria, the most common type, albumin isthe primary urinary protein. Tubular proteinuria resultswhen malfunctioning tubule cells no longer metabolizeor reabsorb normally filtered protein. In this condi-tion, low-molecular-weight proteins predominate overalbumin and rarely exceed 2 g per day. In overflow pro-
March 15, 2005 * Volume 71, Number 6 www.aafp.org/afp American Family Physician 1 1 5 7

teinuria, low-molecular-weight proteins overwhelm theability ofthe tubules to reabsorb filtered proteins.
Further evaluation of persistent proteinuria usuallyincludes determination of 24-hour urinary protein excre-tion or spot urinary protein-creatinine ratio, microscopicexamination of the urinary sediment, urinary proteinelectrophoresis, and assessment of renal function.'-
GLYCOSURIA
Glucose normally is filtered by the glomerulus, but it isalmost completely reabsorbed in the proximal tubule.Glycosuria occurs when the filtered load of glucoseexceeds the ability of the tubule to reabsorb it (i.e., 180 to200 mg per dL). Etiologies include diabetes mellitus,Cushing's syndrome, liver and pancreatic disease, andFanconi's syndrome.
KETONURIA
Ketones, products of body fat metabolism, normally arenot found in urine. Dipstick reagents detect acetic acidthrough a reaction with sodium nitroprusside or nitro-ferricyanide and glycine. Ketonuria most commonly isassociated with uncontrolled diabetes, but it also canoccur during pregnancy, carbohydrate-free diets, andstarvation.
NITRITES
Nitrites normally are not found in urine but result whenbacteria reduce urinary nitrates to nitrites. Many gram-negative and some gram-positive organisms are capable ofthis conversion, and a positive dipstick nitrite test indicatesthat these organisms are present in significant numbers(i.e., more than 10,000 per mL). This test is specific but
The AuthorsJEFF A. 5IMFRVILLE, M.D-. is a fifth-year resident in urology atGeorgetown University Medical Center, Washington, D.C. Hereceived his medical degree from Georgetown University Schoolof Medicine.
WILLIAM C. MAXTED, M.D., is professor of urology at GeorgetownUniversity School of Medicine, where he received his medicaldegree and completed a residency in urology.
JOHN J. PAHIRA, M.D., is professor of urology at GeorgetownUniversity School of Medicine. He received his medical degreefrom Pennsylvania State University Milton S. Hershey MedicalCenter College of Medicine, Hershey, and a residency in urology atthe Hospital of the University of Pennsylvania, Philadelphia.
Address correspondence to Jeff A. Simerville, M. D., 6641 WakefieldDr., #411, Alexandria, VA 22307 (e-mail: [email protected]).Reprints are not available from the authors.
not highly sensitive. Thus, a positive result is helpful, but anegative result does not rule out UTL^ The nitrite dipstickreagent is sensitive to air exposure, so containers shouldbe closed immediately after removing a strip. After oneweek of exposure, one third of strips give false-positiveresults, and after two weeks, three fourths give false-posi-tive results.^^ Non-nit rate-reducing organisms also maycause false-negative results, and patients who consume alow-nitrate diet may have false-negative results.
LEUKOCYTE ESTERASE
Leukocyte esterase is produced by neutrophils and maysignal pyuria associated with UTI. To detect significantpyuria accurately, five minutes should be allowed for thedipstick reagent strip to change color. Leukocyte castsin the urinary sediment can help localize the area ofinflammation to the kidney.
Organisms such as Ghlamydia and Ureaplasma urea-lyticum should be considered in patients with pyuria andnegative cultures. Other causes of sterile pyuria includebalanitis, urethritis, tuberculosis, bladder tumors, viralinfections, nephrolithiasis, foreign bodies, exercise, glo-meruionephritis, and corticosteroid and cyclophospha-mide (Cytoxan) use.
BILIRUBIN AND UROBILINOGEN
Urine normally does not contain detectable amounts ofbilirubin. Unconjugated bilirubin is water insoluble andcannot pass through the glomerulus; conjugated bili-rubin is water soluble and indicates further evaluationfor liver dysfunction and biliary obstruction when it isdetected in the urine.
Normal urine contains only small amounts of urobi-linogen, the end product of conjugated bilirubin after ithas passed through the bile ducts and been metabolizedin the intestine. Urobilinogen is reabsorbed into the por-tal circulation, and a small amount eventually is filteredby the glomerulus. Hemolysis and hepatocellular diseasecan elevate urobilinogen levels, and antibiotic use and bileduct obstruction can decrease urobilinogen levels.
Microscopic UrinalysisMicroscopic examination is an indispensable part ofurinalysis; the identification of casts, cells, crystals, andbacteria aids in the diagnosis of a variety of conditions.To prepare a urine specimen for microscopic analysis, afresh sample of 10 to 15 mL of urine should be centri-fuged at 1,500 to 3,000 rpm for five minutes. The super-natant then is decanted and the sediment resuspendedin the remaining liquid.'^ A single drop is transferred toa clean glass slide, and a cover slip is applied.
1158 American Family Physician www.aafp.org/afp Volume 71, Number 6 • March 15, 2005

Urinalysis
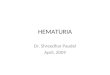
Figure 1. Squamous epithelial cells (arrows) and leukocytes(200 X).
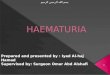
Figure 2. Convoluted renal tubule cells (200 X).
CELLS
Leukocytes may be seen under low- and high-powermagnification (Figure 1). Men normally have fewer thantwo white hiood cells (WBCs) per HPF; women nor-mally have fewer than five WBCs per HPF.
Epithelial ceils often are present in the urinary sedi-ment. Squamous epithelial cells are large and irregu-larly shaped, with a small nucleus and fine granularcytoplasm; their presence suggests contamination.The presence of transitional epithelial cells is normal.These cells are smaller and rounder than squamouscells, and they have larger nuclei. The presence ofrenal tuhule cells indicates significant renal pathol-ogy (Figure 2). Erythrocytes are best visualized underhigh-power magnification. Dysmorphic erythrocytes,which have odd shapes hecause of their passagethrough an abnormal glomerulus, suggest glomerulardisease.
TABLE 6
Urinary Casts and Associated PathologicConditions
Type of cast
Hyaline
Erythrocyte
Leukocyte
Epithelial
Granular
Waxy
Fatty
Broad
Composition
Mucoproteins
Red bloodcells
White bloodcells
Renal tubulecells
Various celltypes
Various celltypes
Lipid-ladenrenal tubulecells
Various celltypes
Information from reference 38.
Associated conditions
Pyelonephritis, chronic renaldisease
May be a normal finding
GlomerulonephritisMay be a normal finding in
patients who play contactsports
Pyelonephritis,glomerulonephritis.interstitial nephritis, renalinflammatory processes
Acute tubular necrosis,interstitial nephritis.eclampsia, nephriticsyndrome, allogrsftrejection, heavy metalingestion, renal disease
Advanced renal disease
Advanced renal disease
Nephrotic syndrome, renaldisease, hypothyroidism
End-stage renal disease
CASTS
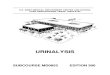
Casts in the urinary sediment may be used to localizedisease to a specific location in the genitourinary tract(Table 6).-'^^ Casts, which are a coagulum of Tamm-Horsfall mucoprotein and the trapped contents of tubulelumen, originate from the distal convoluted tubule orcollecting duct during periods of urinary concentrationor stasis, or when urinary pH is very low. Their cylindri-cal shape reflects the tuhule in which they were formedand is retained when the casts are washed away. The pre-dominant cellular elements determine the type of cast:hyaline, erythrocyte, leukocyte, epithelial, granular,waxy, fatty, or broad (Figure 3).
CRYSTALS
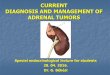
Crystals may be seen in the urinary sediment of healthypatients (Figure 4). Calcium oxalate crystals have arefractile square "envelope" shape that can vary in size.
March 15, 2005 * Volume 71, Number 6 www.aafp.org/afp American Family Physician 1 1 5 9

Figure 3. Urinary casts. (A) Hyaline cast (200 X); (B) erythrocyte cast (100 X); (C) leukocyte cast (100 X); (D) granular cast(100 X).
Uric acid crystals are yellow to orange-brown and maybe diamond- or barrel-shaped. Triple phosphate crystalsmay be normal but often are associated with alkalineurine and UTI (typically associated with Proteus spe-cies). These crystals are colorless and have a characteris-tic "coffin lid" appearance. Cystine crystals are colorless,have a hexagonal shape, and are present in acidic urine,which is diagnostic of cystinuria.
BACTERIURIA
Gram-negative streptococci and staphylococci can bedistinguished hy their characteristic appearance underhigh-powered magnification.
Gram staining can help guide antibiotic therapy, butit is not indicated in routine outpatient practice. Clean-catch specimens from female patients frequently arecontaminated hy vaginal flora. In these patients, fivebacteria per HPF represents roughly 100,000 colony-forming units (CFU) per mL, the classic diagnosticcriterion for asymptomatic bacteriuria and certainlycompatible with a UTI. In symptomatic patients, a col-
ony count as low as 100 CFU per mL suggests UTI, andantibiotics should be considered. The presence of bacte-ria in a properly collected male urine specimen is sug-gestive of infection, and a culture should be obtained.
The authors indicate that they do not have any conflicts of interest.Sources of funding; none reported.
Figures 1 through 4 reprinted from the National Institutes of HealthClinical Center Department of Laboratory Medicine, Bethesda, Md.
REFERENCES
1. Lifshit2 E, Kramer L. Outpatient urine culture, does collection techniquematter? Arch Intern Med 2O0O;160:2537-40.
2. Rabinovitch A, Urinalysis and collection, transportation, and preser-vation of urine specimens: approved guideiine, 2d ed. Wayne, Pa.:National Committee for Clinical Laboratory Standards, 2001. NCCLSdocument GP16-A2.
3. Hanno PM, Wein AJ, Malkowicz SB, Ciinical manual of urology. 3d ed.New York: McGraw-Hill, 2001,
4. Woolhandler 5, Pels RJ, Bor DH, Himmelstein DU, Lawrence RS. Dipstickurinalysis screening of asymptomatic adults for urinary tract disorders.I. Hematuria and proteinuria. JAMA 1989;262:1214-9
5. Agarwal R. Panesar A, Lewis RR. Dipstick proteinuria: can it guidehypertension management? Am J Kidney Dis 2002:39:1190-5
1160 American Family Physician www, aafp.org/afp Volume 71, Number 6 * March 15, 2005

Urinalysis
Orr,
Figure 4. Urinary crystals. (A) Calcium oxalate crystals (arrows; 100 X); (B) uric acid crystals (100 X); (C) triple phosphatecrystals with amorphous phosphates (400 X); (D) cystine crystals (100 X).
5 Pels RJ, Bor DH, Woolhandler S, Himmelstein DU, Lawrence RS. Dipstickurinalysis screening of asymptomatic adults for urinary tract disorders.II. Bacteriuria. JAMA 1989;262:1221-4.
7. Sultana RV, Zaistein S, Cameron P, Campbell D. Dipstick urinalysis andthe accuracy of the clinical diagnosis of urinary tract infection. J EmergMed 2001:20:13-9,
8. Smith P, Morris A, Reller LB, Predicting urine culture results by dipsticktesting and phase contrast microscopy. Pathology 2O03;35,161-5,
9. Van Nostrand JD, Junkins AD, Bartholdi RK. Poor predictive ability ofufinalysisand microscopic examination to detect urinary tract infection.Am J Clin Pathol 2000;113:709-13.
10. Eidelman Y, Raveh D, Yinnon AM, Ballin J, Rudensky B, Gottehrer NPReagent strip diagnosis of UTI in a high-risk population. Am J EmergMed20O2;20:112-3.
11. Lammers RL, Gibson S, Kovacs D, Sears W, Strachan G. Comparison oftest charactenstics of urine dipstick and urinalysis at various test cutoffpoints. Ann Emerg Med 2001;3S:505-12,
12. Semeniuk H, Church D. Evaluation of the leukocyte esterase and nitriteurine dipstick screening tests for detection of bacteriuria in womenwith suspected uncomplicated urinary tract infections, J Clin Microbiol1999:37:3051-2.
13. Leman P. Validity of urinalysis and microscopy for detecting urinary tractinfection in the emergency department, Eur J Emerg Med 2002:9:141-7
14. Kavouras SA, Assessing hydration status, Curr Opin Cltn Nutr MetabCare 2002:5:519-24.
15. Sheets C, Lyman JL. Urinalysis. Emerg Med Clin North Am 1986:4:263-80.
16. Kiel DP, Moskowitz MA. The urinalysis: a critical appraisal. Med ClinNorth Am 1987;71:607-24.
17. Benejam R, Narayana AS. Urinalysis: the physician's responsibility. AmEam Physician 1985:31:103-11.
18. Mariani AJ, Marian! MC, Macchioni C, Stams UK, Hariharan A, Monera A.The significance of adult hematuria: 1,000 hematuria evaluations includinga risk-benefit and cost-effectiveness analysis. J Urol 1989;141:350-5.
19. Grossfeld GD, Litwin MS, WoH JS, Hricak H, Shuler CL, Agerter DC, etal. Evaluation of asymptomatic microscopic hematuria in adults: theAmencan Urological Association best practice policy—part |- defini-tion, detection, prevalence, and etiology. Urology 2001;S7:B99-603.
20. Grossfeld GD, Litwin MS, Wolf JS Jr, Hncak H, Shuier CL, Agerter DC,et al. Evaluation of asymptomatic microscopic hematuria in adults: theAmerican Urological Association best practice policy—part II: patientevaluation, cytology, voided markers, imaging, cystoscopy, nephrologyevaluation, and follow-up. Urology 2001,57:604-10.
21. Ahmed Z, Lee J. Asymptomatic urinary abnormalities. Hematuria andproteinuria. Med Clin North Am 1997:81:641-52.
22. Fassett RG, Horgan BA, Mathew TH. Detection of glomerular bleedingby phase-contrast microscopy. Lancet 1982,1:1432-4.
23. Brendler, CB, Evaluation of the urologic patient: history, physical exami-nation and urinalysis. In: Campbell MF, Walsh PC. Campbell's Urology.7th ed, Philadelphia: Saunders, 1998:144-56,
March 15, 2005 * Volume 71, Number 6 www.aafp.org/afp American Family Physician 1161

Urinalysis
24, Sutton JM. Evaluation of hematuria in adults, JAMA 1990;263:2475-80.
25, Mohr DN, Offord KP, Owen RA, Melton t j 3d, A5ymptomatjc micro-hematurid and urologic disease. A population-based study. JAMA1986:256:224-9.
26, Khan MA, Shaw G, Paris AM, Is microscopic haematuria a urologicalemergency? BJU Int 2002;90.355-7,
27, Mohf DN, Offord KP, Melton U 3d, Isolated asymptomatic microhe-maturia: a cross-sectional analysis of test-positive and test-negativepatients, J Gen intern Med 1987;2:31S-24,
28, Messing EM, Young TB, Hunt VB, Emoto SE, Wehbie )M. The sig-nificance of asymptomatic microhematuria in men 50 or more yearsold: findings of a home screening study using urinary dipsticks, J Urol1987;137:919-22,
29, Khadra MH, Pickard RS, Charlton M, Powell PH, Neal DE A prospectiveanalysis of 1,930 patients with hematuria to evaluate current diagnosticpractice. J Urol 2000:153:524-7.
30, Siegei AJ, Hennekens CH, Solomon HS, Van Boeckel B, Exercise-related hematuria Findings in a group of marathon runners, JAMA1979,241:391-2,
31, House AA, Cattran DC. Nephrology 2 Evaluation cf asymptomatichematuria and proteinuria in adult primary care, CMAJ 2002:166:348-53,
32. Carroll MF, Temte JL, Proteinuria in adults: a diagnostic approach. AmFam Physician 2000:62:1333-40,
33. Von Bonsdorff M, Koskenvuo K, Salmi HA, Pasternack A. Prevalenceand causes of proteinuria in 20-year old Finnish men. Scand J UrolNephrol 1981,15:285-90.
34. Springberg PD, Garrett LE Jr, Thompson AL Jr, Collins NF, Lordon RE,Robin5on RR. Fixed and reproducible orthostatic proteinuria: results ofa 20-year foilow-up study, Ann Intern Med 1982:97.516-9.
35. Rytand DA, Spreiter S. Prognosis in postural (orthostatic) proteinuria:forty to fifty-year follow-up of six patients after diagnosis by ThomasAddis. N Engi J Med 1981;305:618-21.
36. Gallagher EJ, Schwartz E, Weinstein RS. Performance characteristicsof urine dipsticks stored In open containers. Am J Emerg Med 1990:8-,121-3,
37. Fogazzi GB, Garigali G. The dinicai art and science of urine microscopy,Curr Opin Nephrol Hypertens 2003:12:625-32.
38. Graham JC, Galloway A. ACP best practice no. 167: the laboratorydiagnosis of urinary tract infection, J Clin Pathol 2001,54:911-9,
1162 American Family Physician www.aafp.org/afp Volume 71, Number 6 * March 15, 2005