Embed Size (px)
Citation preview

Medullary Thyroid Cancer: From Diagnosis to SurveillanceJASON LEPSE, MS4UNIVERSITY OF KANSAS SCHOOL OF MEDICINE

Objectives• Case Presentation
• Overview of medullary thyroid cancer including workup, treatment and surveillance guidelines
• Ms. G’s course
• References

H&P• 49 yo female with previously discovered right thyroid nodule and multiple abnormal appearing lymph nodes on ultrasound
• CC: neck pain
• HPI• Nodule discovered by PCP; became painful 3-4 weeks ago• Endorses occasional odynophagia but denies dyspnea, dysphagia or voice change• No aggravating factors; pain medication helpful

H&P• PMH: cholelithiasis , hypothyroidism, iron deficiency anemia, menorrhagia, fibroid uterus
• Medications: sennokot
• Allergies: aspirin
• PSH: tubal ligation, laparoscopic cholecystectomy, C-section, D&C
• FH: diabetes in mother; no hx of thyroid or parathyroid disease, pheochromocytoma or mucosal neuromas
• SH: single; no cigarettes or EtOH
• ROS: denies fever, chills, night sweats, chest pain, shortness of breath, fainting or joint pain

H&P• Physical Exam
GEN: Alert and awake. No acute distress. Responds appropriately.
VOICE: Strong voice without hoarseness.
HEAD/FACE: Normocephalic, atraumatic. Face symmetric.
EYES: EOMI. Conjunctiva pink and moist
EARS: Able to hear at conversational levels. Normal pinna bilaterally.
NOSE: Midline dorsum and septum.
OC/OP: No mucosal lesions. Hard and soft palate normal. Tongue and FOM soft and clear. Oropharynx clear without erythema or exudate. NECK: Supple, palpable right cervical LAD; palpable right thyroid nodule, tenderness to palpation near lower border/insertion of right SCM/level 4. No fluctuance or overlying erythemaCARDIOVASCULAR: Pulses intact RESPIRATORY: Chest with normal symmetry, excursion, and respiratory effort. NEURO: Affect and mood normal. Alert and Oriented to Person, Place, Time, & Situation CN3-6, 7 (HB 1/6 BL), 9-12 grossly intact BLEXTREMITIES: Moving all extremities.

H&P• Physical Exam • Flexible Laryngoscopy: True Vocal Cords (TVCs) visualized without masses, symmetrically abduction-
adduction, and no persistent glottic gap noted
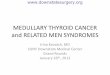
• DDX: Thyroid malignancy vs thyroiditis vs lymphoma• CT Neck Soft Tissue w/ IV Contrast had been performed in ED prior to admission and ENT consult

Axial CT Neck Soft Tissue with IV contrast










Coronal CT Neck Soft Tissue with IV contrast

Workup• FNA• “Atypia of undetermined significance”• Large atypical cells in a lymphoid background
• Excisional biopsy recommended
• Core biopsy of R lower cervical lymph node• Medullary thyroid cancer• Calcitonin stain: Positive
1

Overview• First characterized by Hazard and associates in 1959
• Cell of origin: Neural crest derived parafollicular C-cells• Calcitonin and CEA serum concentrations are directly related to C-
cell mass
• 1-2% of all thyroid malignancies• Lower than previous estimates due to rise in number of PTC cases
• Associated with mutations in RET proto-oncogene• 50% of sporadic cases have RET mutation• All MEN2A, MEN2B and FMTC cases have RET mutation

Prognosis• Ten-year survival rates 2 • Stage I: 100%• Stage II: 93%• Stage III: 71%• Stage IV: 21%
• 70% patients who present with palpable thyroid nodule have cervical metastases and 10% have distant metastases• Presenting with T1: 14% central neck disease, 11% lateral neck disease• Presenting with T4: 86% central neck disease, 93% had lateral neck disease 3
•Stage and age at diagnosis were found to be prognostic on multivariate analysis
• Post-operative calcitonin doubling time is independent predictor of survival

Workup Guidelines• All patients with FNA consistent with MTC should undergo: 4
• Physical Exam• Neck ultrasound• Calcitonin measurement• CEA measurement• RET genetic testing
• Systemic imaging indicated when calcitonin > 500 or patient has extensive neck disease• Octreoscan appears more sensitive than (18)FDG-PET for well-differentiated NETs, whereas (18)FDG-PET
demonstrates superior sensitivity for poorly-differentiated NETs 5

Further Workup• Calcitonin: 15,678 pg/mL
• CEA: 337.7 ng/mL
• Calcium and PTH within normal limits
• Plasma-free metanephrines within normal limits
• CT Chest: • Linear opacity in right middle lobe could be due to atelectasis or
mucoid impaction• Nonspecific 12 mm right hepatic hypodensity
• Presented at Tumor Board: T2N1bMx Medullary Thyroid Carcinoma• Recommendations: PET vs octreotide scan and surgery• Octreotide scan: No avid lesions in chest or liver

Treatment Guidelines• Total thyroidectomy• No neck disease• Level 6 neck dissection• Levels 2-5 neck dissection may be considered based on calcitonin level
• Neck disease• Level 6 neck dissection• Ipsilateral neck dissection levels 2-5• Contralateral neck dissection levels 2-5 if CTN>200
• Adjuvant EBRT should be considered in patients with residual disease, extra-thyroidal extension or extensive lymph node metastases
• Less aggressive surgery to preserve speech and swallow may be preferred in extensive regional or metastatic disease• EBRT or systemic chemotherapy should be considered

Treatment Guidelines• Vandetanib or cabozantinib can be used as single-agent first line chemotherapy in patients with advanced progressive MTC
• Not without side effects• Vandetanib trial: 12% dropped out and 35% required dose reduction • Cabozantinib trial: 16% dropped out and 79% required dose reduction
6 7

Surveillance• Key is serial physical exams, ultrasounds and labs• Draw first post-op calcitonin
and CEA 3 months after surgery
4

Surveillance• Doubling Times: should be calculated every 6 months for CEA and calcitonin• 4 data points over minimum of two years required• One retrospective study showed significant difference in 5 and 10 year survival in patients with doubling
times greater or less than 6 months 8
http://www.thyroid.org/professionals/calculators/thyroid-cancer-carcinoma/

Treatment• Total thyroidectomy with bilateral central and lateral compartment neck dissections
• Final pathology: pT2N1b medullary thyroid carcinoma• (+) extranodal extension• (-) angio-invasion or perineural spread
• ENT follow-up scheduled
• No adjuvant radiation per tumor board recommendations

References1: Litzky, L. Pulmonary Neuroendocrine Tumors. Surgical Pathology Clinics, 2010-03-01, Volume 3, Issue 1, Pages 27-592: Modigliani, Elisabeth, Regis Cohen, Jose-Marie Campos, Bernard Conte-Devolx, Beatrice Maes, Andree Boneu, Martin Schlumberger, Jean-Claude Bigorgne, Philippe Dumontier, Laurence Leclerc, Bernard Corcuff, and Isabelle Guilhem. "Prognostic Factors for Survival and for Biochemical Cure in Medullary Thyroid Carcinoma: Results in 899 Patients." Clin Endocrinol Clinical Endocrinology 48.3 (1998): 265-73.3: Quayle, Frank Jay, and Jeffrey Moley F. "Medullary Thyroid Carcinoma: Management of Lymph Node Metastases." Current Treatment Options in Oncology Curr. Treat. Options in Oncol. 6.4 (2005): 347-54.4:Wells, Samuel A., Sylvia Asa L., Henning Dralle, Rossella Elisei, Douglas Evans B., Robert Gagel F., Nancy Lee, Andreas Machens, Jeffrey Moley F., Furio Pacini, Friedhelm Raue, Karin Frank-Raue, Bruce Robinson, M. Rosenthal Sara, Massimo Santoro, Martin Schlumberger, Manisha Shah, and Steven Waguespack G. "Revised American Thyroid Association Guidelines for the Management of Medullary Thyroid Carcinoma." Thyroid 25.6 (2015): 567-610.5: Squires, Malcolm H., N. Adsay Volkan, David Schuster M., Maria Russell C., Kenneth Cardona, Keith Delman A., Joshua Winer H., Deniz Altinel, Juan Sarmiento M., Bassel El-Rayes, Natalyn Hawk, Charles Staley A., Shishir Maithel K., and David Kooby A. "Octreoscan Versus FDG-PET for Neuroendocrine Tumor Staging: A Biological Approach." Annals of Surgical Oncology Ann Surg Oncol 22.7 (2015): 2295-301. 6: Wells, S. A., B. Robinson G., R. Gagel F., H. Dralle, J. Fagin A., M. Santoro, E. Baudin, R. Elisei, B. Jarzab, J. Vasselli R., J. Read, P. Langmuir, A. Ryan J., and M. Schlumberger J. "Vandetanib in Patients With Locally Advanced or Metastatic Medullary Thyroid Cancer: A Randomized, Double-Blind Phase III Trial." Journal of Clinical Oncology 30.2 (2011): 134-41. Web. 7: Elisei, R., M. Schlumberger J., S. Muller P., P. Schoffski, M. Brose S., M. Shah H., L. Licitra, B. Jarzab, V. Medvedev, M. Kreissl C., B. Niederle, E. Cohen E. W., L. Wirth J., H. Ali, C. Hessel, Y. Yaron, D. Ball, B. Nelkin, and S. Sherman I. "Cabozantinib in Progressive Medullary Thyroid Cancer." Journal of Clinical Oncology 31.29 (2013): 3639-646. 8: Barbet, Jacques, Loïc Campion, Françoise Kraeber-Bodéré, and Jean-François Chatal. "Prognostic Impact of Serum Calcitonin and Carcinoembryonic Antigen Doubling-Times in Patients with Medullary Thyroid Carcinoma." The Journal of Clinical Endocrinology & Metabolism 90.11 (2005): 6077-084.















![Research Paper Thyroid transcription factor FOXE1 interacts ... 85949 ncotarget with non-medullary thyroid cancer risk including single nucleotide variants rs965513[A] (56 kb upstream](https://img.pdfslide.us/doc/110x75/613a50760051793c8c00f8ce/research-paper-thyroid-transcription-factor-foxe1-interacts-85949-ncotarget.jpg)