Embed Size (px)
Citation preview

Urgent and Emergency Care
Providing patients with better access to
services – a Vanguard programme
Health and social care organisations across Barking and Dagenham, Havering and Redbridge working together to improve the quality
of care, with better outcomes for our patients and public

Content
1. Purpose of this phase of the programme
2. Our local context
3. Our story so far
4. Approach taken
5. Telephone survey
6. Face to face engagement
7. Feedback from Stakeholder Event
8. Next Steps
Page number
1
2
4
11
12
18
27
36

Purpose of this phase of the programme
To ensure high quality engagement and consultation with local patients,
carers and the public on Urgent and Emergency Care to help us to
identify the following:
- The understanding of the urgent and emergency services available
locally
- How patients and the public currently use our services and what
drives behaviours
1

Our local context
Barking and Dagenham, Havering and Redbridge residents live in one
of the most challenged health and social care economies in the country.
2

Our local context
This variation and challenge
makes Barking and
Dagenham, Havering and
Redbridge an ideal test bed
for transforming urgent and
emergency care (UEC)
services.
Strong partnership in place
and a track record of
effective collaborative
working.
3

Our story so far
• Locally, as nationally, people are confused by the various urgent
and emergency care (UEC) options available to them
• We talked to local people, health and social care professionals,
and local organisations who represent patients and service users
(July 2015 conference)
• We wanted to know what people thought of services, how they
used them and what they found good – or bad – and what they felt
we could do to make it all work better
4

Our story so far
This is what you told us
Patients and staff told us they
are ‘confused’ by the number of
local services and settings
available to them and that care
is ‘fragmented’ and ‘inefficient’
That confusion and
fragmentation is one reason
why our local hospitals see
around 500 people per day in
A&E at busy times, with 40% or
more not needing to be there –
because they don’t have
emergency needs
5

Our story so far
The financial challenges
• The NHS and local authorities all face funding challenges
• If we continue as we are, we forecast a system wide budget gap of over £400million by 2020
• Spending on urgent and emergency care forecast to increase significantly over the next few years if nothing is done to change services.
We need to do things differently for our patients and for our staff
6

Our story so far
A ‘Vanguard’ programme
• Department of Health asked the NHS to look at new ways of doing things
• BHR partnership has a excellent reputation for working together to find new ways of delivering better care for local people
• BHR invited to describe our big idea for UEC care and bid for support
• Using your feedback, we made a bid and were successful. We are the only UEC Vanguard in London
• We now need to refine our idea – using your help and expertise
• “Vanguard” is just a word – describes a funding programme. This transformation of urgent and emergency care is already a priority for local health and social care partners
7

Our story so far
Our ambition
As a partnership of health and social care organisations, we want to:
• create a simple and streamlined urgent care system which delivers excellent care and patient experience – while achieving financial stability.
• provide services that gives patients better and personalised care through shared care records
• build on already successful schemes e.g. Community Treatment Team (CTT)
• deliver better care closer to your home when you need it
• break down the barriers between health and social care, and between different organisations
8

Our story so far
What does it mean for patients, carers and staff
We want to
• end confusion for our patients
• improve the co-ordination of urgent and emergency care services
• allow GPs to focus on patients who need their care e.g. long term conditions
• signpost patients and carers to other urgent care services, and allow A&E to focus on emergency care
• Patients and staff will co-design the new urgent and emergency care pathway, giving them a real say in what services look like and how they work for them
9

Our story so far
What our vision is – and isn’t
• We need to develop a new model of care that provides them with a
simple way of getting the right care, first time in the right place
• Focus is on providing better care, closer to your home
• Better signposting, advice and access for patient in need of urgent
care or advice
• We know there are local people who go to A&E when they could
choose to go to an alternative service.
• This is not about closing services or healthcare settings
• Vision for a smart digital platform that will recognise patients and
personalise the help they get as soon as they get in contact
• Helping people to self-care is a future priority
• Patients, carers and staff will be at the heart of what we do and will
help co-design the model of care, services, pathways and
information materials – whatever we all agree is important
10

Our approach to this phase of the programme
We want to build upon the work we have already carried out to co-design the new model
of care in Barking and Dagenham, Havering and Redbridge by carrying out extensive
research with our local populations through the following independently delivered
engagement activity:
1. Quantitative - telephone research (BMG Research)
2. Qualitative - face to face surveys and focus groups (Healthwatch partnership)
The purpose of the research was to explore the awareness of urgent and emergency
care services, provide information on how residents are currently navigating these
services and to get feedback that will help to start the co-design of urgent care services
across the three boroughs.
Both BMG Research and the Healthwatch partnership worked with us to co-design the
questions used for both the telephone and face to face surveys.
A stakeholder event was held on the 17th March 2016 to help us to understand the
findings, continue the co-design of the care model and start to shape the next steps of
the programme.11

Telephone survey
• BMG Research was commissioned in early February to deliver 3000 telephone interviews – 1000 per borough
• 3002 telephone interviews were conducted between the 2nd and 21st March, 2016
• The data has been weighted by age, gender, ethnicity and ward within borough and then by borough population. The objective of the weighting is to make the data representative by borough and overall.
• Weights are based on 2011 census data.
• The final report is attached at Appendix A
12

Telephone Survey
Key Findings – Service Awareness
• Only half (51%) of residents overall are
aware of NHS Choices as a source of
advice about urgent and emergency
care. Even among those who state that
they have internet access, this
proportion only rises to 55%. On this
basis it appears that there is potential to
increase awareness of this signposting
resource.
• While awareness of Walk In Centres is
high at 94% awareness of Urgent Care
Centres at 37% is 59-percentage points
lower than the awareness of A&E
departments (96%) despite these two
resources being co-located.
• Any focus on raising awareness of GP Hubs
and GP Out of Hour’s services should focus
on Barking and Dagenham and Redbridge.
Havering residents are more likely to be
aware of Out of Hours GP services (81%)
than residents of both Barking and Dagenham
(77%) and Redbridge (76%). Havering
residents are also more likely to be aware of
GP Hubs (51%).
• A&E users in the last 6 months do not have
significantly lower awareness of other urgent
and emergency care services than non-users.
Indeed, where significant variations do exist,
these show that A&E visitors have a higher
awareness of some of the other providers of
urgent and emergency care than non-users.
• On this basis, it would appear that it is not
simply the case of ignorance of other services
driving A&E attendance. The reality is likely to
be a more complex mix of awareness and
understanding of what each service can offer
and when these services can be accessed. 13

Telephone Survey
Key Findings – Service Usage
• In the last 6 months A&E is the third
most commonly used source of urgent
and emergency care after GPs and
chemists. Residents are most likely to
have used their Doctor/GP in the last six
months (72%), followed by a
chemist/pharmacy (69%). Accident and
Emergency was the third most
commonly used by respondents or their
households at 31%.
• Within this, 18% of A&E users within the
last 6 months only went on one
occasion, the highest proportion across
all of the listed services. The proportion
who visited A&E in the last 6 months is 8
times larger than the proportion that went
to an Urgent Care Centre (4%).
• The proportion of those who state that either
they, a household member, or someone they
care for has been to A&E in the last 6 months is
significantly higher among the 18-34 age group
(38%) and among those aged 35 to 54 (33%).
• Parents with children aged 0-5 (41%), those
with a long term illness or disability (35%) and
those with caring responsibilities (41%) are all
significantly more likely to have visited A&E than
those who do not have these roles/conditions.
14

Telephone Survey
Key Findings – Advice and Signposting
• Where NHS advice/signposting is sought
for health issues the advice received is
followed in the majority of cases. Among
those who visited A&E in the last 6
months and sought prior advice either
from an NHS information source such as
111 or NHS Choices or from a healthcare
professional 87% said that the advice
they received was to go to A&E. Similar
proportions are seen among Urgent Care
Centre visitors (91% of those who
sought NHS advice were advised to go
here), those who went to a Walk In
Centre (87%) and those who went to a
GP Hub (86%).
• When considering scenarios where advice and treatment would be required there is evidence of
younger residents being more likely to seek
information prior to treatment. For example, in a
scenario where someone with ongoing health
issues is experiencing breathlessness more
than twice as many 18-34 year olds (37%)
would suggest phoning NHS 111 than those
aged 65 and over (16%). This younger age
group are also most likely to suggest searching
for advice online (4%). Among older residents
(aged 65+) the most common suggestion is
calling a GP.
• Furthermore, among A&E visitors in the last 6
months, analysis by age shows that those aged
18-34 and 35-54 are most likely to have sought
advice from an NHS information source prior to
their attendance at A&E (26% and 24%
respectively).
15

Telephone Survey
Key Findings – Interest in personalised IT systems
• Looking to the future residents were
asked to state whether they would be
interested in a personalised IT solution to
help them access healthcare locally. All
were asked:
“If the local NHS had a website or app
which held all your health information,
where you could get advice, chat with a
doctor or nurse if necessary or book
yourself into appointments with your GP
or a clinic, do you think you would you
use it? “
• A clear majority of 79% express an interest in
such a solution, suggesting they would use it,
while 21% said they would not use it.
• Breaking these responses down further shows
that among those with access to the internet
84% would be interested in such a website or
app compared to 47% of those who do not have
internet access
16

Telephone Survey
Key Findings – Views on over-use of Accident and
Emergency
• When asked why they think that people
tend to go to A&E when they have non-
emergency issues the key themes that
emerge are:
• o Awareness of the alternatives;
o Resource/capacity issues with other
services; o Speed/convenience;
o Reassurance/trust issues;
o Personal circumstances or
characteristics;
o Uncertainty;
o Habit; and,
o Referrals.
• Within these comments there are two responses
that are particularly prevalent. The first is that
individuals cannot get an appointment with a GP
or other care services (33%). This includes
comments on GP appointments taking too long
to get, GP practice hours and GPs being
overworked. The second major suggestion is
that the public don't know of other services or
are not well informed (31%).
• The dominance of these two comments
suggests that future strategies will need to
assess both capacity issues in care provision
and information provision/signposting in relation
to urgent and emergency care.
• The other comments suggest that awareness
raising will need to develop trust in the
alternatives in terms of both the quality of care
and its availability.
17

Face to face engagement
A Healthwatch partnership from Barking and Dagenham, Redbridge
and Havering were commissioned to deliver face to face discussions
and focus groups across the three boroughs which included:
Redbridge Barking and Dagenham Havering
361 1:1 face to face discussions
298 1:1 face to face discussions
307 1:1 face to face discussions
3 Focus Groups 3 Focus Groups 4 Focus Groups/Workshops
Healthwatch from Barking & Dagenham, Havering & Redbridge
Urgent and Emergency Care Consultation Responses Barking and Dagenham, Havering and Redbridge CCGs Response Data from Healthwatch’s in Barking & Dagenham, Havering & Redbridge
The final report is attached at Appendix B
18

0
200
400
600
800
1000
Yes No
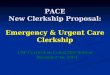
Face to face engagement
Key Findings – Service Awareness Have you heard of the following services where you can get help with treatment, or advice for urgent and emergency care?
19

Of the 774 people who have heard of walk-in Centres, 502 people knew the location.
Of the 301 people who have heard of Urgent Care Centres, 154 people knew the location.
0
100
200
300
400
500
600
Yes No
Do you know the location ofnearest WIC?
Do you know the location ofnearest UCC?
Face to face engagement
Key Findings – Service Awareness
20

0 20 40 60 80 100 120 140 160 180 200
NHS Choices website
Non-NHS health advice websites
NHS 111 telephone helpline
Chemist/Pharmacy
Your GP
Out of Hours GP Services
Mental Health Direct telephone helpline
GP Hubs
Walk in Centre
Urgent Care Centres (UCCs)
Accident and Emergency (A&E)
999 (London Ambulance Service)
Community Treatment Team
Emergency dentists
5 or more 4 3 2 1
How often have you or your household used the following health services for urgent or emergency care the last 6 months?
Number of visits
Face to face engagement
Key Findings – Service Usage
21

Of those who had made one or more visits to: A&E, and Urgent Care Centre, a
Walk-in Centre or a GP Hub 298 people sought advice on where to go before they
went from the following…
• 110 Yes - from an NHS information source such as 111/ NHS choices
• 134 Yes – from a healthcare professional such as a doctor, chemist
• 54 Yes - from a non-NHS source e.g. other website/friends family
• 297 No – I did not seek advice
• 60 I was taken to A&E by ambulance
Did the NHS advice suggest you go to this service?
Yes 171
No 147
Face to face engagement
Key Findings – Service Awareness
22

If the local NHS had a website or app which held all your health information, where you could get advice, chat with a doctor or nurse if necessary or book yourself into appointments with your GP or a clinic, do you think you would you use it?
0
100
200
300
400
500
600
700
Yes No
Face to face engagement
Key Findings – Interest in Personal IT systems
23

What do you think would be the main advantages of such a site or app?
0 50 100 150 200 250 300 350 400
Don’t know
Other (please state)
Single source of information
Personalised/responses based on myhealth records
Can be accessed anywhere
Available all the time/ outside of workinghours
Face to face engagement
Key Findings – Interest in Personal IT systems
24

Can you explain why you would be unlikely to use such a website or mobile phone app?
0 20 40 60 80 100 120
Don’t have internet access/computer/ smartphone
Don’t feel confident with technology/ would not know how to use
Data charges/cost to access
Concern about security of personal data/ health records
Would prefer to speak to someone in person
Use existing online GP booking systems
Other (please state)
Don’t know
Face to face engagement
Key Findings – Interest in Personal IT systems
25

NHS Accident and Emergency Departments commonly treat people whose injuries or
illnesses could be treated just as well elsewhere. Why do you think that people tend
to go to A&E when they have non-emergency issues?
• They do not have an understanding about other options
• Guaranteed that they will definitely be seen in A&E and have the problem
dealt with (Even if there is a long wait!)
• People thought it was the safest option
• Takes too long to see the GP. E.G No appointments for up to three weeks+
• No confidence in other services
• NHS 111 are not as competent as ambulance staff
Face to face engagement
Key Findings – Views on over-use of Accident and Emergency
26

Urgent and emergency careVanguard
Feedback from Stakeholder Event
17th March, 2016
27

Purpose of the event
To come together as a mixed group to help shape the next phase of
developing our urgent and emergency care services within Barking and
Dagenham, Havering and Redbridge by:
• Bringing everybody up to date on the story so far
• Provide feedback on the face to face and telephone engagement,
understand what it is telling us and agree whether there are any
gaps
• Start to shape the engagement activity for the next phase – co-
designing services
28

Attendees
• A mix of 40 people attended
including patients, carers,
clinicians and representatives
from Social Care, Healthwatch,
Voluntary Organisations and
NHS organisations operating
within the three boroughs
• A mix of people and
organisations from across the
three boroughs were present
and participated in three
workshops
29

Workshop 1 – What is the feedback telling us?
• What is interesting about the feedback?
• What is surprising?
• What questions does this raise?
These questions were discussed at six separate tables by a mixed group of attendees with a facilitator present
30

Summary of the feedback from Workshop 1 –what is the feedback telling us?
• Very complex system and therefore confusion for both patients and staff
• The language used for the different services is not easy to understand
• There is a need for simplicity ‘Clunk, click every trip’
• Rebadge services to reduce confusion
• There is a lack of awareness of some of the services available particularly the hubs and Mental Health Direct
• Should keep mental health on the radar and be clear on the services being provided
• Most of the awareness is where the services have been established the longest
• Need to explore the benefit of increasing awareness if the capacity doesn’t exist?
• Support clinicians to redirect to risk levels
• There are cultural nuances within the feedback and need to understand these
• We only advertise in English – should be advertising services in the main community languages and making best use of our community assets
• Need to understand the efficiency of community services
• More willingness to use online services than expected
• Maybe should consider Skype contact so patients can talk to someone
• Health Education, self care and prevention are important
• Ensure A&E message does not stop people accessing services
• We should be asking people what should we do?
31

Workshop 2 – Working together to shape the
services to meet the needs of local people
• What is missing from the research so far
• What else do we need to find out?
• How do we take this forward in the next phase?
These questions were discussed at six separate tables by a mixed group of attendees with a facilitator present
32

Summary of the feedback from Workshop 2 –
working together to shape the services to meet the
needs of local people• The engagement needs to be consistent
across the three boroughs
• Face to face versus non – experience of Learning/physical disabilities
• Missing questions from research which included:
– what does good look like?
– What would make it better?
– Why do people end up going to A&E when advised not to?
– What was the reason for the visit?
– Did the patient mean to go to A&E or just want a GP
• Data not collecting all equality groups and other groups within the community and therefore need to be much wider in engagement approach should be used to understand experiences “we are not hard to reach we are easy to ignore”
• Still focus on physical health need more focus on mental health
• Need to capture the experience of people using 999 services
• Understand reputation of services, good standards/quality
• Require different ways to cut the data to better understand the issues
• Look at data from 111 – are referrals appropriate?
• Education very important – need behaviour change – target schools and information and advice at surgery level
• Assumption about records being shared as an issue – how much would the community know about record sharing?
• Non English speakers – improve information and signposting to services
• Target the audiences likely to use the service – Physical disabilities/Learning Disabilities/Mental Health
– How do they access services
– What are the services doing to avoid A&E
admission?
• Access to GP/Primary Care is an issue
• Symbol recognition could be used to simplify the system
• Apps – growing use – potential – range of solutions (don’t assume age!)
• Need to explore how to support risk taking
• People need more confidence in services
33

Workshop 3
• Who do we need to talk to?
• How should we talk to people about it?
• What should we focus the discussions on?
• Can you help?
All individuals were given the opportunity to respond to these questions through the completion of post it notes placed on the relevant flip chart – facilitators were present to be able to help if required
34

Workshop 3
A huge response was received to each of the four questions and is
shown in detail at Appendix C.
35

Next steps
• The report of the engagement activity carried out in this phase will be made
publicly available
• The feedback from both the telephone research and face to face will be
analysed further and will help shape the next stage of activity to co-design
the urgent care services for Barking and Dagenham, Havering and
Redbridge.
36