Embed Size (px)
Citation preview

Tony Yates Digital SME
NHS England
Interoperability

High Level Architecture

Over 3 million ambulanceshave been dispatchedelectronically

Over
have been sentelectronically
10 million OOH messages

Most
has been sentelectronically
GP correspondence

All calls
right from thebeginning
traced against PDS

There is more to do!

MUCH MORE!

What isInteroperability?

Interoperability
Source: https://en.wikipedia.org/wiki/Conceptual_interoperability
• Not to be seen as just a “techie” concept• Its about how we get
• To achieve this, need to think on how we “deliver this in the service”
• Professional buy-in and prioritisation• Improving patient experience• System/vendor functionality• Levers and incentives
• Aligning with the wider NIB Interoperability strategy on enabling information sharing through open interfaces
the pertinent information tothe professional at the point of care where it adds value

Supporting the maturity of the estate
Source: https://en.wikipedia.org/wiki/Conceptual_interoperability
Structured APIs using
strategic terminology
(SNOMED and dm+d)
• View information
Structured APIs with existing coded
information
HTML View
• Automated prompting and alerting in all cases
• Automated clinical decision-support
• Consolidate information
• Pertinent information displayed
Sending System Receiving System
Sending systems moving up the maturity of information sharing
-> means that systems using this information can still move at different speeds without constraining innovation
Structured APIs using
strategic terminology
(SNOMED and dm+d)
Structured APIs with existing coded
information
HTML View

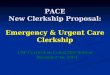
Interoperability Layers
Level 1•Technical Interoperability, means we have a way of electronic communication
•e.g. sms, messenger, skype etc.
Level 2•Syntactic Interoperability, common data structures are in place
•e.g. Email, Twitter API, Facebook etc.
Level 3• Semantic
Interoperability, the meaning of the data is shared
• e.g. Flight bookings, banking transactions etc.
Source: https://en.wikipedia.org/wiki/Conceptual_interoperability

Same at both sides? Not always!
Source: https://en.wikipedia.org/wiki/Conceptual_interoperability
Senders
•Semantic Senders (almost)
•Ensure we send the right thing
•Check the structure &
•Check the conformance
Receivers
• Syntactic Receivers
• Check the structure (CDA)
• Accept or reject
• Upgrades are value driven when they are needed

The Requirements• Sort out the PEM• Access to Records• Support clinical hub workflow across a range of skills• Open up repeat caller to 999, OOH, Clinical Hubs• Provide semantic codes flagged on SCR• Make the DOS API more flexible• Support other clinical content sets in ITK• Enable 999 to send into 111• NHS Number Tagging• Inter Clinical Hub transfers• Endpoint registry not dependent on the DOS• OOH Ambulance Dispatch• Booking In Hours, Out of Hours, Out of Area

Interoperability
Source: https://en.wikipedia.org/wiki/Conceptual_interoperability
Thinking about what this means for the patient

Start with the users

Observe what people do

Not what theysay

It’s not alwaysabout standards

How do we do this?

Together!