Embed Size (px)
Citation preview
UPDATES ON THE COVID – 19 VACCINE DEPLOYMENT AND IMPLEMENTATION
Maintained by the Disease Prevention and Control Bureau
Office of the Director III for Policy and Planning
(COVID 19 and Vaccine)
Strong
Leadership and Governance
NCA/IATF/NTF/DOH/DILG
Duterte Administration
Vaccine Roadmap
“Command and Control”
2
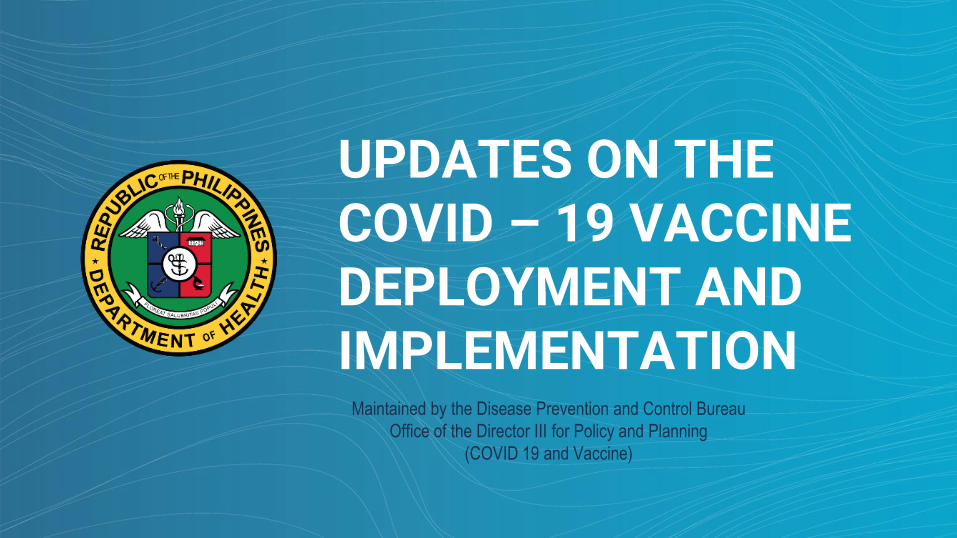
Whole-of-Government and Whole-of-Nation Approach
Engaged Government Agencies and Private
Sector
Supportive Academic Societies
Medical Experts
Highly Committed LGUs/LCEs
Adequately Informed Communities
Well-prepared Health Systems (HRs,
Funding, Information)
Massive Nationwide Vaccination Program
Tripartite AgreementDistribution and Deployment
Vaccine Administration
Tripartite AgreementPublic Uptake Communication
Supply Chain
Public Uptake Communication
ProcurementSupply Agreement
Implementation
CompliancePublic Uptake
Synchronized and Integrated Efforts

SPECIAL CHAPTER: GOVERNANCE
National Deployment and Vaccination Plan
● Establishment of a national level structure○ A robust system of
leadership, an accountable and transparent decision-making structure and process to protect national interests.

Protect the public and reduce morbidity
and mortality rates due to COVID-19
GOAL
To establish a sustainable immunization program
against COVID-19
MISSION
DOH Vision, Mission, and Goal
Strategic Plan for COVID-19 Vaccination
Safe, equitable, and cost-effective
immunization for all Filipinos by 2023
VISION
1. To provide equitable access to COVID-19 immunization services to priority groupsor at most, 50 to 70 million Filipinos if with enough global supply by 2021.
2. To increase demand for vaccination services through capacity and confidencebuilding measures;
3. To ensure safety in the immunization program and provide support to patientswith adverse reactions; and
4. To institute governance, regulatory, financing and performance accountabilitymeasures for COVID-19 immunization
DOH Objectives
Strategic Plan for COVID-19 Vaccination

● Complemented with
the activation of the
Incident Command
System at all levels
SPECIAL CHAPTER: GOVERNANCE
National Deployment and Vaccination Plan
National Deployment
& Vaccination Plan
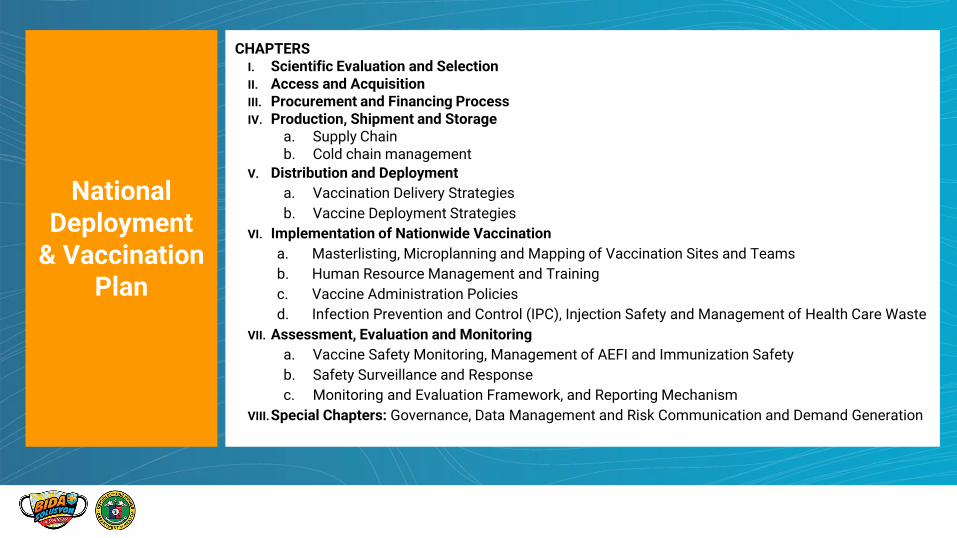
CHAPTERSI. Scientific Evaluation and SelectionII. Access and AcquisitionIII. Procurement and Financing ProcessIV. Production, Shipment and Storage
a. Supply Chain b. Cold chain management
V. Distribution and Deployment
a. Vaccination Delivery Strategies
b. Vaccine Deployment Strategies
VI. Implementation of Nationwide Vaccination
a. Masterlisting, Microplanning and Mapping of Vaccination Sites and Teams
b. Human Resource Management and Training
c. Vaccine Administration Policies
d. Infection Prevention and Control (IPC), Injection Safety and Management of Health Care Waste
VII. Assessment, Evaluation and Monitoring
a. Vaccine Safety Monitoring, Management of AEFI and Immunization Safety
b. Safety Surveillance and Response
c. Monitoring and Evaluation Framework, and Reporting Mechanism
VIII.Special Chapters: Governance, Data Management and Risk Communication and Demand Generation

Vaccination Delivery Strategies● Priority populations for COVID-19 vaccinations were identified based on the WHO Strategic Advisory
Group of Experts on Immunization (SAGE) values framework for the allocation and prioritization of
COVID-19 vaccination and reviewed by the National Immunization and Technical Advisory Group.
WHO SAGE Framework
Overarching Goal COVID-19 vaccines must be a global public good. The overarching goal is forCOVID-19 vaccines to contribute significantly to the equitable protection andpromotion of human well-being among all people of the world.
Principles Human Well-Being, Equal Respect, Global Equity, National Equity, Reciprocity,Legitimacy
National Deployment and Vaccination Plan
Chapter V: Distribution & Deployment
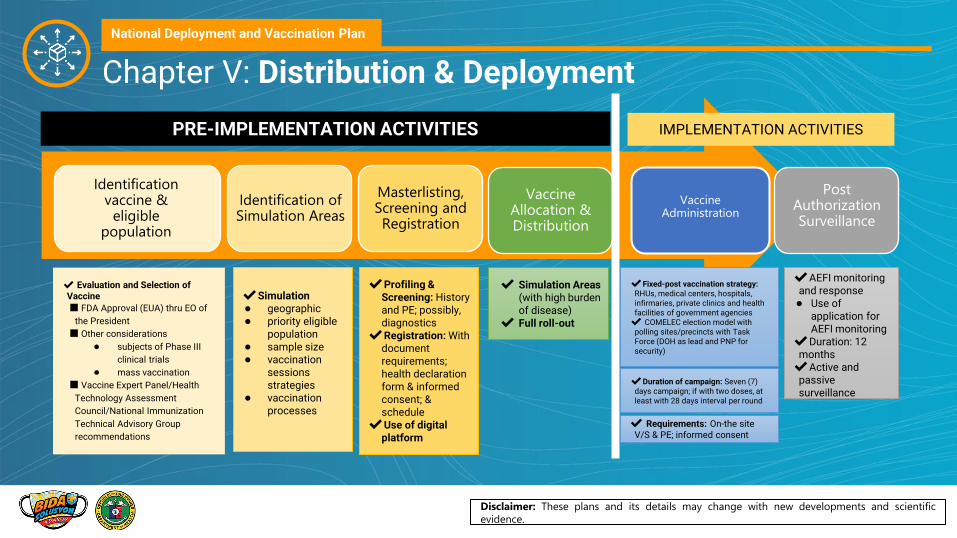
✔AEFI monitoring and response● Use of
application for AEFI monitoring
✔Duration: 12 months✔Active and
passive surveillance
✔ Evaluation and Selection of Vaccine
■ FDA Approval (EUA) thru EO of
the President
■ Other considerations
● subjects of Phase III
clinical trials
● mass vaccination
■ Vaccine Expert Panel/Health
Technology Assessment
Council/National Immunization
Technical Advisory Group
recommendations
✔ Simulation Areas (with high burden of disease)
✔ Full roll-out
✔Simulation● geographic● priority eligible
population● sample size● vaccination
sessions strategies
● vaccination processes
✔Duration of campaign: Seven (7) days campaign; if with two doses, at least with 28 days interval per round
Identification vaccine &
eligible population
Identification of Simulation Areas
Masterlisting, Screening and Registration
Vaccine Allocation & Distribution
Vaccine Administration
Post Authorization Surveillance
✔Fixed-post vaccination strategy: RHUs, medical centers, hospitals, infirmaries, private clinics and health facilities of government agencies✔ COMELEC election model with
polling sites/precincts with Task Force (DOH as lead and PNP for security)
PRE-IMPLEMENTATION ACTIVITIES
✔ Requirements: On-the site V/S & PE; informed consent
IMPLEMENTATION ACTIVITIES
National Deployment and Vaccination Plan
Chapter V: Distribution & Deployment
Disclaimer: These plans and its details may change with new developments and scientific
evidence.
Prioritization and
Allocation Framework

Prioritization in the context of scarcityObjectives: (a) reduce mortality and (b) preserve health system capacity
PRESENTED TO CHD ARDs & RESUS ON 2021-02-11
CRITERION 1 PRIORITY GROUPS
Group Priority Sectors
A 1: Workers in Frontline Health Services
2: All Senior Citizens
3: Persons with comorbidities
4: Frontline personnel in essential sectors
inc uniformed personnel
5: Indigent Population
B Other Frontline Workers and Special
Populations
C Remaining Population
CRITERION 2GEOGRAPHIC
LOCATIONCRITERION 3
SUB-PRIORITY
GROUPS
LGU and Supply
Chain
NEED CAPACITY
XEXPOSURE X MORTALITY RISK
For HCWs - by facility directly
providing care, Level 3 DOH
→ LGU → private, other
hospitals, community, stand
alone
For Senior citizenss -
institutionalized, then other
senior citizens
For indigents - in locality with
highest burden, with high
risk comorbidities, etc

Phase 2 - Priority Eligible B
B1 Teachers, Social Workers
B2 Other government workers
B3 Other essential workers
B4 Socio-demographic groups at significantly
higher risk other that senior citizens and poor
population based on the NHTS-PR
B5 Overseas Filipino Workers
B6 Other Remaining workforce
Phase 3 - Priority Eligible C: Rest of the Filipino
population not otherwise included in the above groups
Phase 1 - Priority Eligible A
A1 Frontline workers in health facilities both national
and local, private and government, health professionals and
non-professionals like students in health and allied professions
courses with clinical responsibilities, nursing aides, janitors,
barangay health workers, etc.
A2 Senior citizens aged 60 years old and above.
A3 Adults with comorbidities not otherwise
included in the preceding categories.
A4 Frontline personnel in essential sectors both in
public and private sectors, including uniformed personnel, and those in
working sectors identified by the IATF that are directly client facing and
cannot dutifully meet minimum public health standards.
A5 Poor population based on the National
Household Targeting system for Poverty
Reduction (NHTS-PR) not otherwise included
in the preceding categories.

Sub-prioritization: Priority Group A1
CRITERION 1 PRIORITY GROUPS
Group Priority Sectors
A 1: Workers in Frontline Health Services
2: All Senior Citizens
3: Persons with comorbidities
4: Frontline personnel in essential sectors
inc uniformed personnel
5: Indigent Population
B Other Frontline Workers and Special
Populations
C Remaining Population
Priority A1.1 COVID-19 referral hospitals designated by the DOH;
Priority A1.2Public and private hospitals and infirmaries providing COVID-19 care, as prioritized based on service capability, starting from level 3 hospitals, to level 2 hospitals to level 1 hospitals, and then infirmaries; Among hospitals with a common service capability, the order of priority shall be from facilities owned by the DOH, then facilities owned by LGUs, then facilities owned by private entities;
Priority A1.3Isolation and quarantine facilities such as temporary treatment and monitoring facilities and converted facilities (e.g. hotels, schools, etc) that cater to COVID-19 suspect, probable, and confirmed cases, close contacts, travellers in quarantine;
Priority A1.4 Remaining hospitals including facilities of uniformed services not catering to COVID-19 cases;
Priority A1.5Government owned primary care based facilities such as Urban Health Centers, Rural Health Units and Barangay Health Stations, birthing homes, and Local Health Offices to include members of BHERTS, contact tracers, social workers;
Priority A1.6Stand-alone facilities, clinics and diagnostic centers, and other facilities otherwise not specified (e.g. clinics, dialysis centers, dental clinics, and COVID-19 laboratories), dealing with COVID-19 cases, contacts, and specimens for research purposes, screening and case management coordinated through their respective local government units;
Priority A1.7 Closed institutions and settings such as, but not limited to, nursing homes, orphanages, jails, detention centers, correctional facilities, drug treatment and rehabilitation centers, and Bureau of Corrections.
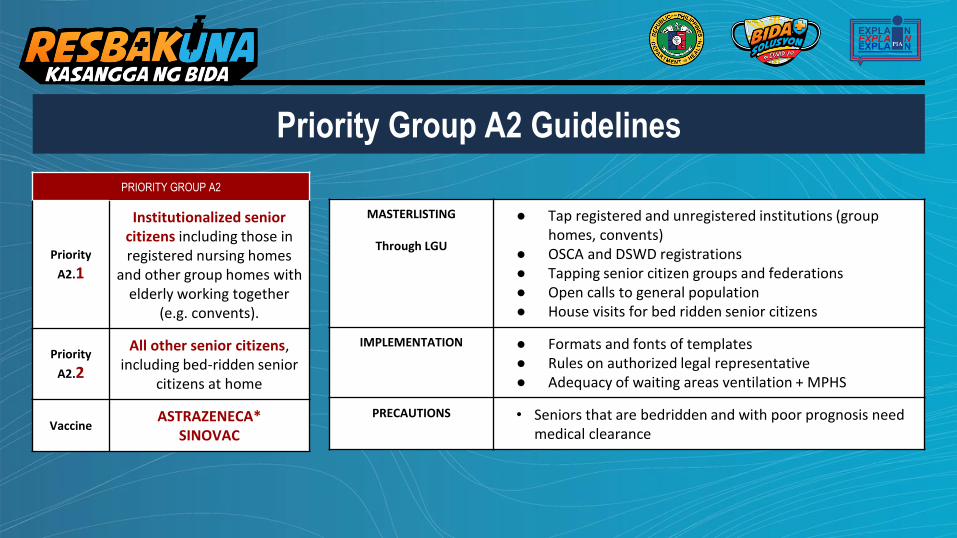
PRIORITY GROUP A2
Priority
A2.1
Institutionalized senior citizens including those in registered nursing homes
and other group homes with elderly working together
(e.g. convents).
Priority
A2.2
All other senior citizens, including bed-ridden senior
citizens at home
VaccineASTRAZENECA*
SINOVAC
Priority Group A2 Guidelines
MASTERLISTING
Through LGU
● Tap registered and unregistered institutions (group homes, convents)
● OSCA and DSWD registrations● Tapping senior citizen groups and federations● Open calls to general population● House visits for bed ridden senior citizens
IMPLEMENTATION ● Formats and fonts of templates● Rules on authorized legal representative● Adequacy of waiting areas ventilation + MPHS
PRECAUTIONS • Seniors that are bedridden and with poor prognosis need medical clearance

Priority Group A3 Guidelines
Priority Group A3: Adults with Comorbidities
Priority A3
Any non-senior adult between 18-59 years old with any clinically controlled comorbidity
Proofs of comorbidity shall include: ● Medical certificate from an attending physician
issued within the past 18 months● Prescription to medicines for the past 6 months ● Hospital records such as the discharge summary
and medical abstract● Surgical records and pathology reports
Vaccine SINOVAC
SUBPRIORITZATION ● By geographic burden of disease
MASTERLISTING ● LGU of hospital registries● Tap disease support groups, chapters● House visits by community workers● Open call for general population
IMPLEMENTATION ● Cannot be administered to those in active disease (uncontrolled or with symptoms)
PRECAUTIONS ● Those in immunodeficiency need medical clearance after dialogue with physician (Autoimmune
disease, Persons living with HIV, Persons with cancer or malignancy, transplant patients, persons using steroids)
● Controlled comorbidity and active disease to be screened during vaccination day
The vaccine recipient should be screened on the day of the vaccination. They are not in active disease OR they are stable/controlled if they:
1. Have no symptoms2. If vital signs are taken, have stable vital signs
(defer ONLY if hypertensive urgency > 180/90 mmHg)
1. Have had no attacks, admissions, or changes in medication for the past 3 months
2. Currently not hospitalized
VACCINE RECIPIENT - NOT IN ACTIVE DISEASE

Filipinos with the following diseases should be prioritized because they would have higher risk of having severe COVID-19 if infected. Other diseases not stated but fall in the general categories may also belong to Priority Group A3.
1. Chronic respiratory disease and infection such as asthma and respiratory allergies, Chronic Obstructive PulmonaryDisease, Interstitial Lung Diseases, Cystic Fibrosis, or Pulmonary Hypertension, Pulmonary Tuberculosis, Chronic bronchitis,Histoplasmosis, Bronchiectasis
2. Cardiovascular disease such as hypertension coronary heart diseases, cardiomyopathies, peripheral artery disease, aorticdiseases, rheumatic heart disease, congenital heart disease
3. Chronic kidney disease
4. Cerebrovascular disease such as stroke and transient ischemic attack
5. Cancer or malignancy
6. Diabetes Mellitus Type 1 and Type 2
7. Obesity
8. Neurologic disease such as dementia, Alzheimer’s Disease, Parkinson’s Disease, Epilepsy and Seizures, Bell’s palsy,Guillan-Barre Syndrome, or acute spinal cord injury
9. Chronic liver disease such as hepatitis cirrhosis, non-alcoholic fatty liver disease
10. Immunodeficiency state such as genetic immunodeficiencies, secondary or acquired immunodeficiencies (i.e. prolongeduse of corticosteroids), HIV infection, Solid organ or blood transplant patients
11. Other diseases such as sickle cell disease, Thalassemia or Down Syndrome
Who are part of Priority Group A3?

Frequently Asked Questions

WHERE WILL I MASTERLIST?
LGU of your permanent residence, current residence, or workplace
WHERE WILL I BE VACCINATED?
● In LGU-defined vaccination centers linked to appropriate health care provide networks for AEFI management
● Scheduled vaccination may be done on separate days or in:○ HIV treatment hubs, due to confidentiality considerations○ TB centers, esp for MDRTB wherein full vaccination team
will need to wear N95 masks
● At home through house-to-house vaccination, for those bed-ridden who have medical clearance for vaccination
LGUs to enable vaccination by having accessible vaccination sites and/or facilitating transportation of recipients, in compliance to minimum public health standards
On LGU-led Masterlisting and Vaccination

On vaccinating Senior Citizens
WHERE WILL SENIOR CITIZENS GET VACCINATED?
• They can be vaccinated at their assigned LGU sites• Those bed-ridden who have clearance can be vaccinated through
scheduled house-to-house teams or through LGU-facilitated transportation of senior citizens to vaccination centers via shuttles or allowing private transportation.
IS CLEARANCE NEEDED FOR SENIOR CITIZENS?
• Medical clearance is NOT needed prior to vaccination UNLESS they meet conditions needing clearance (Autoimmune disease, HIV, Cancer/ Malignancy, Transplant Patients, Undergoing steroid treatment, Patients with poor prognosis).
• However, they will still be screened for active disease during vaccination day.

WHO NEEDS MEDICAL CLEARANCE?
1. Autoimmune disease2. HIV3. Cancer/ Malignancy, if taking immunosuppressive drugs4. Transplant Patients5. Undergoing steroid treatment6. Patients with poor prognosis or bed-ridden
The objective of medical clearance is to have individual risk-benefit assessment depending onthe state of each patient. This may be done through:● Teleconsultation● Consultation at designated facilities or hubs, if applicable● Through RHU or other primary care centers designated by LGU
DO OTHER CONDITIONS NEED MEDICAL CLEARANCE PRIOR TO VACCINATION?
Other co-morbidities that do not fall under the above subgroups do NOT need medical clearance prior to vaccination.
Screening for active disease shall be done on vaccination day through interview in the health screening form and on-site physician assessment, if necessary.
On Medical Clearance
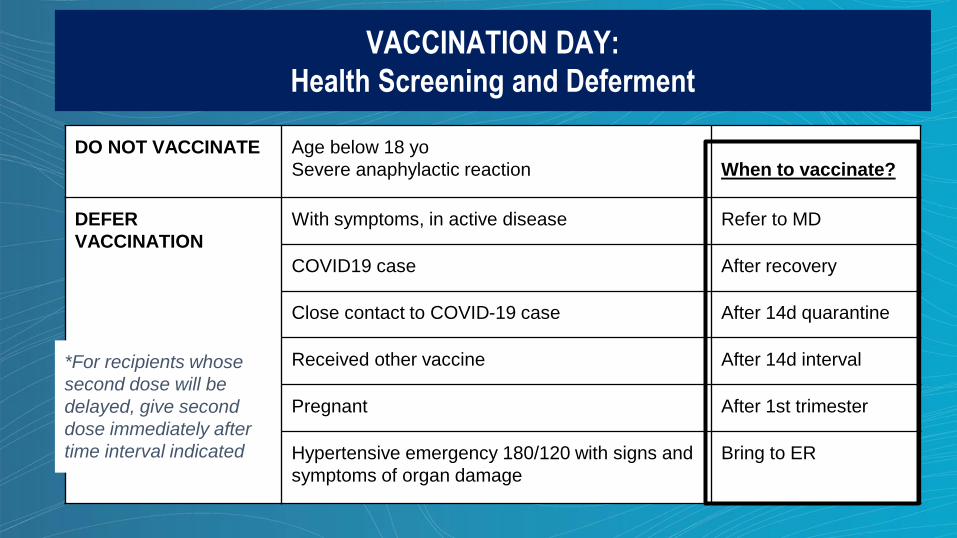
VACCINATION DAY:
Health Screening and Deferment
DO NOT VACCINATE Age below 18 yo
Severe anaphylactic reaction When to vaccinate?
DEFER
VACCINATION
With symptoms, in active disease Refer to MD
COVID19 case After recovery
Close contact to COVID-19 case After 14d quarantine
Received other vaccine After 14d interval
Pregnant After 1st trimester
Hypertensive emergency 180/120 with signs and
symptoms of organ damage
Bring to ER
*For recipients whose
second dose will be
delayed, give second
dose immediately after
time interval indicated

Updated Health Screening Form and Algorithm as of 12 April 2021
Templates and materials bit.ly/RESBAKUNAMaterials

● Informed consent shall only be taken ONCE, during the first dose. A separate informed consent form for the second dose is not necessary.
● Vaccination sites should ensure compliance to minimum public health standardsEspecially regarding maximum capacity, ventilation, engineering controls such as barriers and sectioning, availability of handwashing stations, wearing of face mask/shield
● Post-vaccination reminders and prompts to confirm presence of AEFI. Minimum frequency: one (1) week, two (2) weeks, one (1) month, three (3) months, six (6) months, twelve (12) months after the date of vaccination. LGUs may have more frequent interval of monitoring depending on their capacity and agreements with the vaccination sites.
Other Vaccination Day Reminders

The need to continuously implement minimum public health standards after vaccination including wearing of face masks and shields, maintaining physical distancing, hand hygiene, seeking consult and immediate quarantine or isolation if exposed or with symptoms, among others.
Second dose schedule and reminders
Mechanisms to report any adverse event after immunization to the vaccination site or the LGU
Initial treatment or management for common adverse events
Contact information or location for consultations or referrals
Post-Vaccination Instructions

PARALLEL ACTIVITIES IN THE VACCINATION SITE?
Parallel activities are allowed in the vaccination site provided that they are: A.) separate from the vaccination and monitoring area, B.) following minimum public health standards,C.) Done after vaccination, and not a pre-requisite to vaccination D.) Does not impact efficient operations of the vaccination program
Possible activities
PHILHEALTH - Membership updating- Registration to primary care provider- To enable financial coverage esp in case of AEFI or healthcare
after vaccination
LGU should coordinate with PhilHealth LHIO
NATIONAL ID/ PHILSYSLGU should coordinate with NEDA/PSA

Determining the Teams and Personnel RequiredOperational Guidelines: Vaccination Teams
● Vaccination Team composition (6)○ (2) Screening and Assessment: Physician/Nurse/Midwife ○ (1) Health educator: Allied Professionals/ Volunteers from partner
agencies (e.g. teachers, social workers, medical students, etc)○ (1) Vaccinator: Nurse/Midwife of RHU ○ (2) Documenter/Recorder and V/S taking: Midwife/BHW/Health
Staff / Volunteers from partner agencies (e.g. teachers, social workers, medical students, etc)
● One (1) supervisor, preferably a physician, for at least three (3) vaccination teams
● Other personnel needed in the implementing unit (fixed point strategy):○ Cold Chain Officers○ Local Officials (barangay captains)○ Security Personnel (PNP)○ Drivers○ Safety Officers (Barangay Tanods, among others)
● Personnel needed in the community/health facility (house-to-house strategy):○ Social mobilizers: BHWs○ Navigators/Transport: BHWS and Local Officials,
Health Facility Management
● AEFI Composite Team composition (2)○ (1) Monitor: Paramedic/Nurse/Midwife○ (1) Surveillance: Surveillance Officer/Nurse/Midwife /Pharmacist
● One (1) vaccination team = One (1) AEFI/AESI composite team
● One (1) vaccination team: 100 vaccinees/day
National Deployment and Vaccination Plan
Chapter VI: Implementation of a Nationwide Vaccination
Disclaimer: These plans and its details may change with new developments and scientific
evidence.

National Deployment and Vaccination Plan
Chapter VI: Implementation of a Nationwide Vaccination
Disclaimer: These plans and its details may change with new developments and scientific
evidence.
● Vaccination Implementing Units
○ Establishments authorized to conduct the vaccination activity
■ Medical centers, hospitals and infirmaries (private and public) i
■ Rural Health Units
■ Health facilities of other government agencies (e.g. AFP hospitals and facilities, 71
BJMP/BuCor health facilities, and DepEd clinics)
■ Private clinics
○ May have several vaccination sites/posts within its vicinity, e.g. a medical center can have
several vaccination sites/posts within its vicinity
● Vaccination sites/posts
○ Areas within the implementing units where the vaccination administration proper is
conducted
○ Interim Guidelines on the Identification and Utilization of COVID-19 Vaccination Sites
National Deployment and Vaccination Plan
Disclaimer: These plans and its details may change with new developments and scientific
evidence.
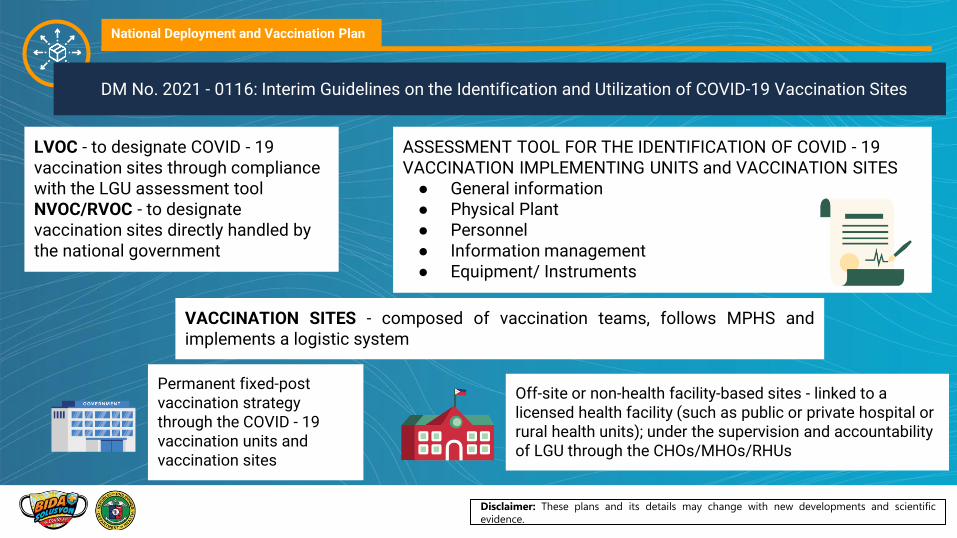
VACCINATION SITES - composed of vaccination teams, follows MPHS andimplements a logistic system
LVOC - to designate COVID - 19 vaccination sites through compliance with the LGU assessment toolNVOC/RVOC - to designate vaccination sites directly handled by the national government
ASSESSMENT TOOL FOR THE IDENTIFICATION OF COVID - 19 VACCINATION IMPLEMENTING UNITS and VACCINATION SITES● General information● Physical Plant● Personnel● Information management● Equipment/ Instruments
DM No. 2021 - 0116: Interim Guidelines on the Identification and Utilization of COVID-19 Vaccination Sites
Off-site or non-health facility-based sites - linked to a licensed health facility (such as public or private hospital or rural health units); under the supervision and accountability of LGU through the CHOs/MHOs/RHUs
Permanent fixed-post vaccination strategy through the COVID - 19 vaccination units and vaccination sites

National Deployment and Vaccination Plan
Chapter VI: Implementation of a Nationwide Vaccination
Disclaimer: These plans and its details may change with new developments and scientific
evidence.
✔ Scan QR code generated from Pre-registration
✔ Checklist of information
✔Document requirements
✔Health declaration form
✔ Informed consent
✔Utilize checklist before administering vaccination
✔Ensure proper vaccination technique
✔Encode the details in the immunization card and give to the vaccinee
✔Conduct History-taking and Physical Examination ✔Utilize Checklist
and Form
✔Utilize script and checklist✔Counsel patients by
batches✔Answer questions
about vaccine and possible side effects ✔Play Video on COVID-
19 Vaccine
✔Sign final consent form
VaccinationPost-vaccination Monitoring, Surveillance and Recording
COMPOSITE TEAM VACCINATION TEAM
Pre-vaccination Counselling and Final
ConsentRegistration Screening
✔ Observe the patient for 1 hour and watch out for any shortness of breath (SOB), syncope, anaphylactic reaction.
✔Monitor Vital Signs every 15 minutes. ✔ Utilize checklist✔ Respond and give first aid to patients
with AEFI.✔ Refer to hospital if further management
needed.

Disclaimer: These plans and its details may change with new developments and scientific
evidence.
Vaccine Administration Policies
Entrance Exit
RegistrationArea (2)
ScreeningArea (2)
Counselling and Final Consent
Area (1)
Vaccination Area (1)
Post-Vaccination Monitoring Area
(2)
QR and
Data
System
Waiting Area
QR and
Data
System
QR and
Data
System
Projector
or TVBP,
Temp, PE,
Present
Hx
VT1
VT2
VT3
BP,
Temp, PE,
Present
Hx
BP,
Temp, PE,
Present
Hx
Vaccine,
syringe,
SCB
BP, AEFI Kit,
Ambulance
Vaccine,
syringe,
SCB
Vaccine,
syringe,
SCB
S
A
S
A
S
A
S
A
S
A
S
A
S
A
S
A
S
A
S
A
S
A
Entrance ExitVaccination ProperPost - Vaccination
Area
Ave: 15 minutes/person 30 minutes - 1 hour/person
3-5 minutes 5 minutes 3-5 minutes 1-2 minutes SA - Sanitation Area
VT - Vaccination Team

National Deployment and Vaccination Plan
Ideas to Scale up the Vaccination Program
Disclaimer: These plans and its details may change with new developments and scientific
evidence.
1.Tap available support - private sector, military, other NGA
2.Lessen on-site processes by finishing most documents/ screening before
3.Larger vaccination sites for efficiency gains and reduce mass gatherings E.g. gym linked to health facility, engineering controls for minimum health standards
4.Other non-health cadres to perform functions that will reduce HCW administrative workload
5.Better business processes: marketing, organizing, manpower management, ICT tools and platforms,

AEFI Surveillance CycleWorld Health Organization, Guidance for establishing
AEFI surveillance systems AEFIC - Adverse Event
Following
Immunization
Committee
R/NAEFIC -
Regional/National
AEFIC
MOP - Manual of
Operations
ESR - Event-based
Surveillance and
Response
CRF - Case Report
Form
CIF - Case
Investigation Form
National level: national ratesSub-national level: line listing
5. Analysis
RAEFIC and NAEFIC
6. Causality Assessment
Reporting facilities stipulated in AO 2016-0006
1. AEFI Identification
AEFIC Resolutions, official statements
7. Feedback
ESR, CRF, CIFAEFI database
3. Reporting
Advisories, AO 2016-0006, AEFI MOP
4. Investigation
Minor AEFI cases- weeklySerious/ cluster- 24-48 hrs
2. Notification
National Deployment and Vaccination Plan
Chapter VII: Assessment, Evaluation and Monitoring
Disclaimer: These plans and its details may change with new developments and scientific
evidence.

Demand Generation
Communication & Community Engagement
Social Listening
Supply Side Demand Side
Develop and align
messages* & platforms
across public & private sector
Crisis Communication
Opinion-makers &
Influencers
Community Organizers
Activate Communities
Multiply champions
SPECIAL CHAPTER: Risk Communication and Community Engagement
National Deployment and Vaccination Plan

Significant Updates Procurement and Finance
No cost vaccines - COVAX Facility
15%Country's Population
(22 million Filipinos)
Significant Updates Procurement and Finance
148Million
Doses for 2021

Significant Updates Procurement and Finance
50-70Million
Filipinos will be vaccinated in 2021.

Indicative Timeline and Numbers of COVID - 19 Vaccine Arrival

REFERENCES:
National Deployment and Vaccination Plan
● For Demand Generation Playbook: tinyurl.com/DemGenPlaybook
● For standard templates, collaterals and FAQs: bit.ly/RESBAKUNAMaterials
● For LVOCs/LGUs/other local partners or groups bit.ly/COVIDVaccinesPHChampionsKit
● COVID-19 vaccination policies bit.ly/COVIDVaccinePolicies
● Information on COVID-19 vaccines https://doh.gov.ph/vaccines and covid19.gov.ph/vaccine

Maraming Salamat po!
Sama-sama tayo sa
RESBAKUNA: Kasangga ng BIDA