Embed Size (px)
Citation preview

Updated reviewCommon thyroid conditions
Thamer Alessa, MD, FACE, CCDEndocrinology, Diabetes & Metabolism
Jaber Al-Ahmad Hospital/Dasman Diabetes Institute

Case 1
• A 49-year-old woman presented to ER, with progressive lethargy and dyspnea (NYHA functional class IV)
• Has a 1-yr h/o weight gain, hair loss, dry skin, constipation, cold intolerance and leg swelling
• Vital signs:– Temp 31.1°C, BP 134/83 mmHg, HR
88 bpm, RR 18 breaths/min and O2
saturation 90% on room air
• Examination:– Cool, dry skin
– Pretibial, periorbital and bilateral lower extremity non-pitting edema
– Thyroid not palpable
– CV: muffled heart sounds, S3 and grade 2/6 systolic ejection murmur at the apex radiating to the left axilla
– Lung examination: rales bilaterally


Case 1
• Transthoracic echocardiography: showed a markedly dilated LV with a diastolic dimension of 5.7 cm, a severely depressed LVEF of 15–20%, severe diffuse hypokinesis, a moderate to severe degree of MR and a small pericardial effusion

Case 1 – Laboratory
• TSH 52 mIU/L (0.27-4.2 uIu/mL)
• FT4 2.3 pmol/L (7.8-16 pmol/L)
• TPO antibody titre 287 IU/mL (<40)

Case 1
• What is the most likely diagnosis?
Myxedema Coma

Myxedema Coma
• The most severe stage of hypothyroidism:– Impaired sensorium, hypoventilation, bradycardia, hypotension & hypothermia– Cardiovascular collapse and shock– Rare, high mortality rate (25-50%)
• Occurs usually in patients with long-standing, undiagnosed hypothyroidism.
• Precipitated by:– Infections– Trauma, surgery– Exposure to cold– Cardiovascular conditions (MI, stroke)– Drugs

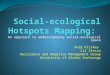
Diagnostic Criteria of Myxedema Coma
Adapted from Popoveniuc G, et al. Endocr Pract 2014; 11:1-36
Total score:• >60 highly suggestive/diagnostic
of myxedema coma• 25-59 supportive of diagnosis of
myxedema coma• <25 myxedema coma unlikely
Score 80

CV Complications of Untreated Hypothyroidism
• Dyslipidemia
• Atherosclerotic cardiovascular disease
• Congestive heart failure
• Reversible cardiomyopathy (severe hypothyroidism)
Modified from ATA 2014

Heart Failure Events by TSH
Gencer Circulation 2012; 126:1040
riskrisk

Hypothyroidism and CVS effectsTissue
ThermogenesisSystemic Vascular
Resistance
DiastolicBlood Pressure
AfterloadCardiac Chronotropy,Inotropy, & Lusiotropy
Cardiac Output
Preload
Renin/Angiotensin/Aldosterone
System
T4
T3
T3
T4
Based on Klein and Danzi, In: The Thyroid 2004

Hypothyroidism and CVS effectsTissue
ThermogenesisSystemic Vascular
Resistance
DiastolicBlood Pressure
AfterloadCardiac Chronotropy,Inotropy, & Lusiotropy
Cardiac Output
Preload
Renin/Angiotensin/Aldosterone
System
T4
T3
T3
T4
Based on Klein and Danzi, In: The Thyroid 2004

Other Manifestations of Myxedema Coma
• Neurologic– Patients might manifest variable degrees of altered consciousness– Brain function is affected by reduction in oxygen delivery and subsequent
consumption, decreased glucose utilization, reduced cerebral blood flow and hyponatremia
• Pulmonary– Hypoventilation is common, results from central depression of ventilatory drive
with decreased responsiveness to hypoxia and hypercapnia– Other contributing factors to hypoventilation:
• Respiratory muscle weakness, mechanical obstruction by a large tongue, and obesity-hypoventilation syndrome
– Fluid accumulation may cause pleural effusions and decreased diffusing capacity

Other Manifestations of Myxedema Coma
• Renal– Function may be compromised with reduced GFR due to low cardiac output and peripheral
vasoconstriction or rhabdomyolysis– Hyponatremia is common, caused by increased serum ADH and impaired water excretion
• Gastrointestinal– The GI tract can be marked by mucopolysaccharide infiltration and edema– Neuropathic changes can cause malabsorption, gastric atony, paralytic ileus, and megacolon– Ascites may occur due to increased capillary permeability or heart failure– GI bleeding secondary to an associated coagulopathy may occur
• Hematologic– Associated with coagulopathy (acquired von Willebrand syndrome type 1 and decreases in
factors V, VII, VIII, IX, and X) and anemia

Management
• Initial steps:
– Airway management
• Mechanical ventilation commonly required during the first 36-48 hours
• Some patients require prolonged respiratory support for as long as 2-3 weeks
– Thyroid hormone replacement
– Glucocorticoid therapy
– Supportive measures
• For hypothermia, hypoventilation, hyponatremia, volume depletion and hypoglycemia

Thyroid hormone replacementATA 2014
• Initial thyroid hormone replacement for myxedema coma should be levothyroxine and liothyronine given intravenously.
• Levothyroxine:– Loading dose of 200–400 µg– Daily replacement dose of 1.6 µg/kg body weight (reduced to 75% if given IV)– Oral therapy may be instituted after the patient improves clinically
• Liothyronine:– Loading dose of 5–20 µg, followed by a maintenance dose of 2.5–10 µg every 8
hours– Therapy can continue until the patient is clearly recovering

Glucocorticoid therapyATA 2014
• Empiric glucocorticoid coverage should be employed as part of the initial therapy for myxedema coma, with intravenous glucocorticoid administration, at doses appropriate for the stressed state, preceding levothyroxine administration.

Case 2
• A 53 year old retired housewife complains of progressive weight gain (7 kg in 1 yr) and fatigue, started 1.5 years ago
• Complains from poor sleep quality and lack of energy to workout
• Vital signs: Temp 36.1oC, pulse 58 bpm, BP 140/100 mmHg
• Physical exam:– Moderately obese with pale,
cool, dry skin
– Thyroid gland slightly enlarged, firm, not nodular, mobile, and not tender
– Deep tendon reflex delayed

Case 2 - Laboratory tests
• CBC and differential WBC are normal
• Free T4 9.8 pmol/L (7.8-16)
• TSH 7.2 uU/ml (0.27-4.2 uIu/mL)
• TPO Ab 150 IU/mL (<2.0)
• Total cholesterol is 7.1 mmol/l
• HDL-C 1.01 mmol/l
• TG 1.82 mmol/l
• LDL-C 5.2 mmol/L

Case 2
• What is the likely diagnosis?
Subclinical hypothyroidism

Case 2
• Most common causes of subclinical hypothyroidism:
– Autoimmune thyroid disease (Hashimoto's thyroiditis)
– Radioactive iodine therapy for hyperthyroidism
– Thyroidectomy
– External beam radiotherapy

Case 2
• Any additional tests required to help confirm the diagnosis?
No
Thyroid autoantibodies are arguably insensitive and the cost does not justify the benefit
Thyroid autoantibodies helpful to predict the risk of developing overt hypothyroidism in patients with subclinical hypothyroidism
ATA 2014

Case 2
• Is treatment with thyroid replacement therapy is indicated in this patient with subclinical hypothyroidism?
Depending on risk factors

Complications of Untreated Hypothyroidism
• Dyslipidemia
• Atherosclerotic cardiovascular disease
• Congestive heart failure
• Reversible cardiomyopathy (severe hypothyroidism)
ATA 2014

Hypothyroidism and dyslipidemia
• Laboratory abnormalities:
– Elevated total cholesterol
– Elevated LDL-C
– Elevated apolipoprotein B
– Elevated Lp (a) (thrombogenic and atherogenic)
– HDL2 (apo A1) increased
– Elevated triglycerides
– Raised homocysteine, CRP, urate, phosphate

Colorado hypothyroidism prevalence study. Canaris et al 2000
Hypothyroidism and dyslipidemia

Hypothyroidism and dyslipidemia
Elizabeth N. Pearce; The Journal of Clinical Endocrinology & Metabolism 2012, 97, 326-333
Thyroid hormone:• ↑ LDL receptor expression• ↑ CETP concentrations• ↑ hepatic lipase (HL) concentrations• ↑ hepatic cholesterol synthesis by inducing
HMG CoA reductase• ↓ intestinal cholesterol absorption an action
mediated by the Niemann-Pick C1-Like 1 (NPC1L1) protein
The reverse occurs in hypothyroidism

Biondi, Cooper Enocr Rev 2008 Feb;29(1):76-131
Subclinical Hypothyroidism Impact on IHD Events

Subclinical Hypothyroidism and CHD or Mortality
Ochs N, et al. Ann Intern Med. 2008 Jun 3;148(11):832-45.

Subclinical Hypothyroidism and CHD or Mortality
Ochs N, et al. Ann Intern Med. 2008 Jun 3;148(11):832-45.

Stratified Analysis of the Association of Subclinical Hypothyroidism with Risk for CHD
Ochs N, et al. Ann Intern Med. 2008 Jun 3;148(11):832-45.

HRs for CHD Events, CHD Mortality, and Total Mortality According to Elevated TSH Categories in Patients with Subclinical Hypothyroidism
Rodondi N et al. 2010 JAMA 304:1365-74
Data on 55,287 participants between 1972 and 2007 were supplied from 11 prospective cohorts in the United States, Europe, Australia, Brazil, and Japan

HTN risk in subclinical hypothyroidismMean SBP and DBP by categories of TSH in men (n = 8,014) and women (n = 14,721), adjusted for age
and smoking status
Asvold, B. O. et al. J Clin Endocrinol Metab 2007;92:841-845
SBP DBP

Correlation between weight and baseline TSH quartile
Fox, Archives Internal Medicine, 2008
Females Males

Subclinical hypothyroidism and CV risk
Does LT4 replacement improve the CV risk factors?

The effect of L-thyroxine vs. placebo on CV markers
Razvi S, et al. JCEM. 2007; 92:1715–1723
Randomized, double-blind, crossover study, with SCH (mean TSH 6.6 mIU/liter, mean age 53.8 yr) without previously treated thyroid or vascular disease, treated with 100 mcg L-thyroxine or placebo daily for 12 wks

IHD events and mortality in treated and untreated subclinical hypothyroid (The Whickham Survey)
Frequency and HRs for IHD events and mortality in treated and untreated subclinical hypothyroid (TSH 6.0-15 mIU/liter, mean age 49.9 yrs) participants over 20 yr of follow-up
Razvi S, el al. JCEM 2010, 95, 1734-1740.
Number of events (%) HRs (5–95% confidence intervals)

CV Treatment Outcome of Subclinical Hypothyroidism
Razvi S, et al. Arch Intern Med. 2012;172(10):811-817
40-70 years >70 years
(P = .02) (P = 0.56)
Retrospective analysis of UK General Practitioner Research Database to identify individuals with new SCH (TSH 5.01-10.0 mIU/L) recorded during 2001 with outcomes analyzed until March 2009, median follow up 7.6 years
IHD
Eve
nts
(fa
tal a
nd
no
n-f
atal
)
IHD
Eve
nts
(fa
tal a
nd
no
n-f
atal
)
aHR 0.61; 95% CI, 0.39-0.95 aHR, 0.99; 95% CI, 0.59-1.33

Time course of incident fatal plus nonfatal CV events & all-cause mortality in placebo and levothyroxine groups (intention to treat population)
Stott DJ, et al. NEJM. 2017; 376:2534-2544
Double-blind, randomized, placebo-controlled, parallel-group trial with 737 adults, ≥ 65 years of age with subclinical hypothyroidism (TSH 4.60-19.99 mIU/L and normal FT4), secondary outcome, study underpowered

Impact of Thyroid Hormone Therapy on Atherosclerosis in the Elderly With Subclinical Hypothyroidism
Double-blind RCT with 185 participants (mean age 74.1 yrs) with SCH and (TSH 4.60-19.99 mIU/L) randomized to receive levothyroxine vs placebo for median of 18.4 months
Blum MR , et al. JCEM. 2018 Aug 1;103(8):2988-2997

Is treating subclinical hypothyroidism beneficial?Who to treat?
When to treat?

Factors favoring L-thyroxine treatment in SCH
• Degree of TSH rise, and its progression
• Therapeutic trial for symptoms
• Age of the patient
• CV risk, or prevalent IHD
• Dyslipidemia
• Bipolar disorder, depression
• Pregnancy or intent of falling pregnant
• Infertility, ovulatory dysfunction
• Patient preference

Treatment of TSH between 5 and 10?Depends…
• Treatment should be considered particularly if they have symptoms suggestive of hypothyroidism, positive TPO antibodies or evidence of ASCVD, HF or have associated risk factors for these diseases.
• Evidence not fully generalizable to stated recommendation and there are no prospective, interventional studies.
Vanderpump MP et al. 1995 Clin Endo 43:55-68Vanderpump MP & Tunbridge WM 2002 Thyroid 12:839-47Hollowell JG et al. 2002 JCEM 87:489-99Huber G et al. 2002 JCEM 87:3221-26McQuade C et al. 2011 Thyroid 21:837-43Ochs N et al. 2008 Ann IM 148:832-45

Treatment of TSH levels > 10 is recommended
• Patients whose serum TSH levels exceed 10 mIU/L are at increased risk for HF and CV mortality, and should be considered for treatment with levothyroxin.
• Not generalizable and meta-analysis does not include prospective interventional studies.
– Hypothyroid patients treated with normalized TSH are still more likely to feel poorly (Saravan Clinical Endo 2002; Boeving Thyroid 2011)
Surks et al. 2004 JAMA 291:228-38Rodondi N et al. 2010 JAMA 304:1365-74Razvi S et al. 2010 JCEM 95:1734-40Gencer B et a.2012 Circulation Epub before print

Management
• Treatment of choice is levothyroxin
• Branded thyroxine and consistency is recommended (ATA 2014)
• No divided doses
• Check TSH level after 4-6 weeks to adjust the dose
• Not recommended for use:– Desiccated thyroid extract– Combination of thyroid hormones– T3 replacement except in Myxedema coma

Case 3
• Is treatment with levothyroxine therapy in this patient with subclinical hypothyroidism (TSH 7.2 uU/ml) is indicated?
• Recap:– Age 53– ? Symptomatic– Physical findings (pale, dry skin, deep tendon reflex delayed)– BP 140/100 mmHg– TG 1.82 mmol/l, LDL-C 5.2 mmol/L– TPO Ab 150 IU/mL (<2.0)
YES

Hypothyroidism during pregnancy
ATA 2017
ULRR, upper limit of the reference range

Hypothyroidism during pregnancy
• Women requiring levothyroxine replacement therapy, the dose should be titration to achieve a TSH concentration within the trimester-specific reference range.
• Serial TSH to be assessed every 4 weeks during the first half of pregnancy and reassessed during the second half of pregnancy.
• For women already taking levothyroxine, two additional doses per week of the current levothyroxine dose, given as one extra dose twice weekly with several days separation, may be started as soon as pregnancy is confirmed.
First trimester 0.1–2.5 mIU/L
Second trimester 0.2–3.0 mIU/L
Third trimester 0.3–3.0 mIU/L
ATA 2014

Case 3
• 73-year-old man is transported to the ER by ambulance for nausea, vomiting, diarrhea, weakness, palpitations and mild shortness of breath of three days’ duration
• PMH: T2DM, stage 3b chronic kidney disease, dyslipidemia, HTN and CAD
• Meds: Glargine, liraglutide, atorvastatin, lisinopril,
carvedilol, amlodipine and clopidogrel
• Exam: pulse 126 bpm, BP 154/88 mmHg, temp 36.8 °C, RR 18 breaths/min, PO2 98 mmHg, agitated, chest: rales, pedal edema
• ECG: A-fib• Chest x-ray and CT (without
contrast) of the head, chest, and abdomen within normal limits

Laboratory Tests
• TSH < 0.005 uIU/mL (0.27-4.2)
• Free T4 83 pmol/L (7.8-16)
• Free T3 14.97(2.3-4.2 pg/mL)
• Hemoglobin 11.2 g/dL
• Hematocrit 33%
• eGFR 39
• Glucose 10.0 mmol/L
• AST 94 U/L (15-37)
• ALT 94 IU/L (16-61)
• Alkaline phosphatase 78 U/L (45-117)
• Troponin I 0.10 ng/mL (0.00-0.50)
• Urinalysis WNL

Thyroid tests
• Thyroid-stimulating immunoglobulin: 309% (reference range, < 30%)
• Nuclear medicine thyroid scan with uptake: 6-hour uptake of 70.3% (10%-25%) and 24-hour uptake, 81.8% (15%-35%)
• Homogeneous radiotracer uptake within the thyroid gland: no evidence of hot or cold nodules
• Thyroid ultrasound: bilateral enlarged heterogeneous gland and multiple subcentimeter nodules

How should clinically or incidentally discovered thyrotoxicosis be evaluated and initially
managed?

Hyperthyroidism - Assessment of disease severityATA 2016
Assessment of thyrotoxic manifestations(CV and neuromuscular complications)
Cardiac evaluation may be necessary, especially in the older patient(Echo, ECG, Holter monitor, or myocardial perfusion studies)
Treatment may be needed for concomitant MI, CHF or atrial arrhythmias
Anticoagulation may be necessary in patients in AF
History and physical examination (PR, BP, RR, and body weight)
Thyroid size, tenderness, symmetry and nodularity
Peripheral edema, eye signs and pretibial myxedema

Is this patient at risk for complications and increased mortality?

Burch–Wartofsky Point Scale
? Thyroid storm Score 50

Thyroid Storm
• thyroid storm is a rare disorder characterized by multisystem involvement and mortality rates in the range of 8%–25%.
• Klein I, Danzi S 2007. Circulation 116:1725–1735
• Akamizu T, et al 2012 Thyroid 22:661–679
• Angell TE, et al 2015 JCEM 100:451–459
• Swee du S, et al 2015 Endocr Pract 21:182–189

How should thyroid storm be managed?

Thyroid Storm
• The diagnosis should be made clinically in a severely thyrotoxic patient with evidence of systemic decompensation
• Adjunctive use of a sensitive diagnostic system should be considered– Burch–Wartofsky Point Scale of ≥45 (or Japanese Thyroid Association) with
evidence of systemic decompensation require aggressive therapy
– The decision to use aggressive therapy in patients with a BWPS of 25–44 should be based on clinical judgment
• A multimodality treatment approach to patients with thyroid storm should be used

Precipitants of thyroid storm
• Abrupt cessation of ATDs
• Thyroidectomy
• Nonthyroidal surgery in a patient with unrecognized or inadequately treated thyrotoxicosis
• Acute illnesses unrelated to thyroid disease
• RAI therapy

Treatment strategy for thyroid storm
• Therapy directed against thyroid hormone secretion and synthesis
• Measures directed against the peripheral action of thyroid hormone at the tissue level
• Reversal of systemic decompensation
• Treatment of the precipitating event or intercurrent illness
• Definitive therapy

Reducing thyroid hormone secretion and synthesis
• Antithyroid medications– Methimazole/Carbimazole
• Initial daily dosing:– 5–10 mg if free T4 is 1–1.5 times the upper limit of normal– 10–20 mg for free T4 1.5–2 times the upper limit of normal– 30–40 mg for free T4 2–3 times the upper limit of normal
– PTU• Starting dose 50–150 mg three times daily
– AE: Agranulocytosis, Hepatotoxicity, pANCA-positive small vessel vasculitis
• Potassium iodide (KI)– The Wolff–Chaikoff Effect, blocks synthesis and release– Start after 1hr from antithyroid medications
ATA 2016

Decreasing T4-to-T3 conversion
• Preferential use of PTU over Methimazole/Carbimazole– T3 levels drops by 45% in the first 24 hours compared to 10%–15%
• Abuid J, Larsen PR 1974 J Clin Invest 54:201–208• Cooper DS, et al 1982. JCEM 54:101–107
• Glucocorticoid therapy• Chopra IJ, et al 1975 JCEM 41:911–920
• β-adrenergic blocking agents (propranolol), with selective ability to inhibit type 1 deiodinase
• Patients who respond poorly to traditional therapeutic measures:– Plasmapheresis/plasma exchange– Emergency surgery

Thyroid Storm: Drugs and DosesATA 2016

Reversal of systemic decompensation& Treatment of the precipitating event or intercurrent illness
• High flow O2
• Rapid cooling if markedly hyperthermic– Ice packs, cooling blanket, mist/fans, nasogastric tube lavage,
acetominophen
• IV fluid bolus if dehydrated– Inotropes and/or diuretics if in CHF
• IV diltiazem +/- digoxin for rate control for atrial fib
• Consider sedatives such as benzodiazepines (beta blockers are the mainstay of therapy)

Definitive therapy
• Radioactive iodine therapy
– Caution: Smoking with Graves’ orbitopathy
• Thyroidectomy

THANK YOU