Embed Size (px)
Citation preview

IMAGING IN RENAL TRAUMA
Presented by: Dr. Ajay P DsouzaSenior Specialist Radiologist Dasman Diabetes Institute.
Supervised by Dr. Abdelmohsen Bennakhi
FFR-RCSI FCSR-McMaster-Canada
FFR-RCSI Course Director-KIMSConsultant Radiologist-MAK Hospital
Presented at: Sabah Al Ahmed Urology Center
13.02.2014 Kuwait.

Learning objectives
Describe the mechanism of renal injuries
Indications for imaging in renal trauma.
Describe the spectrum of renal injuries.
Identify the key imaging features on CT.
Correlate the imaging findings with AAST grading.
Identify the distinguishing CT features according to the AAST
grading.
Update with modifications of AAST Renal Injury Grades.
Role of interventional radiology in the management of Renal injury

Mechanism of Renal trauma
Motor vehicle collision (MVC)
Fall from height, Direct blow to the
torso Sports injury
Deceleration injury

Imaging anatomy of Kidney

The anterior pararenal space (APRS) is located between the parietal peritoneum (PP) and the anterior renal fascia (ARF) and contains the pancreas (Pan),the ascending colon (AC), and the descending colon(DC).
The posterior pararenal space (PPRS) is located between the posterior renal fascia (PRF) and the transversalis fascia (TF).
The perirenal space (PRS) is located between the anterior renal fascia and the posterior renal fascia.
Ao = aorta, IVC = inferior vena cava, LCF = lateroconal fascia.

Indications for Imaging
Universally accepted indications for renal imaging in blunt trauma include Gross hematuria Microscopic hematuria and hypotension (systolic blood
pressure <90 mm Hg) or other associated injuries requiring CT evaluation
Blunt trauma with other injuries known to be associated with renal injury (e.g. rapid deceleration, fall from a height, direct contusion or hematoma of flank soft tissues, fractures of the lower ribs or thoracolumbarspine),regardless of the presence of
hematuria

Role of Imaging
Ultrasound
Quick, non invasive low cost way of detecting peritoneal fluid (FAST)
Can detect renal laceration but not accurate in depth and extent
No functional information like leakage and excretion
Can be better for the follow up and checking resolution of
hematomas
For triage of patients with blunt trauma.
Operator dependent

FAST Extension of physical examination of the trauma
patient Can be done during primary survey Primary goal of FAST is to identify intraabdominal
free fluid. Free fluid=Hemoperitoneum in unstable patients Free fluid found – solid organ injury in 80-90% Draw back:
Blood versus extravasated fluid /urine leakLow sensitivity for retroperitoneal blood.

Intravenous Pyelography
Replaced by CT
Recommended in places where only IVP is available
One shot intra-operative IVP
○ In unstable patients with signs of renal injury who
undergo immediate operative intervention it provides
important information for decision making as to the
function of the kidney and renal injury
○ Iodinated contrast of 2ml/kg body weight followed by
plain film after 10 minutes, it is safe and efficient.

Contrast Computed Tomography
Gold standard method
Most sensitive and specific than IVP
Detects all grades of injuries
Gives overview of the abdomen and pelvis
Superior anatomical detail and fast
Detects associated injuries
Urography phase gives functional details.
Missed renal injury on CT is common but minor and do not alter
clinical course

CECT technique Goal is largest amount of information in the shortest possible time
Initial nonenhanced study can be helpful in detecting acute bleeding or
intraparenchymal hematoma that may become isoattenuating relative to the
normal renal parenchyma at post contrast CT
Routine CT usually includes a portal venous phase; therefore, the kidneys will
be imaged during the late cortical or early nephrographic phase, which allows
identification of parenchymal injuries
Imaging should be performed during excretory phase (5min) to rule out leakage
of contrast-enhanced urine if renal pedicle injury or significant perinephric or
periureteral fluid is found, and whenever confusing findings requiring further
characterization are depicted during the portal venous phase
Delayed CT may also be useful in distinguishing between active bleeding and
pseudo aneurysms

BA
C D

MRI
Not used routinely
Longer imaging time
Used when CT not available/ iodine allergy
In few cases were CT findings are equivocal.
Technically demanding on patient and facility.

Angiography
Stable patients who are candidates for
radiological control of hemorrhage defined
on CT
More specific than CT in defining vascular
injury
Renal vein injury
Non enhancing Kidney on CT

Reporting terminology used in CT1. Contusions: is described as an ill-defined and poorly
marginated hypo dense area of decreased enhancement on the nephrographic phase that may show delayed or persistent enhancement.

2. Infarction
Infarcts are wedged shaped sharply marginated hypo dense area seen on the nephrographic phase and shows no delayed enhancement.
Infarcts can be confused with Contusions

3. Subcapsular Hematoma
Subcapsular hematomas are seen as cresentic or biconvex area of blood collection along the renal contour causing flattening or depression of the underlying renal surface

4.Perinephric hematoma Perinephric hematoma is confined between the
renal parenchyma and Gerota's Fascia It outlines renal contour extending over a wider area
with (when large) without flattening or depression of renal margins. It can displace the kidney.
It occurs following a laceration of the renal capsule

5.Laceration
Lacerations are irregular linear
hypo dense areas of
parenchymal defect reaching
up to surface causing
disruption of the parenchymal
continuity
It may be complex with
variable width of the clefts that
may be filled with blood clots
They also show no
enhancement

6.Shattered Kidney
Multiple lacerations causing gross disruption and fragmentation
of the renal parenchyma often associated with renal function
compromise, injury to the collecting system with urinary
extravasation, severe hemorrhage and active arterial bleeding.

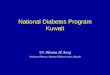
7.Pseudo aneurysm
Focal rounded well circumscribed lesion within the renal
parenchyma or in the lacerated segment that shows
intense enhancement similar to that of the attenuation of
the blood pool and wash out synchronous to blood pool
There is no expansion on the delayed scans
Pseudo aneurysm

FIGURE 1
Renal pseudoaneurysm after blunt renal trauma in a pediatric patient: management by angiographic embolization
S Halachmi, P Chait, J Hodapp, D.G Bgli, G.A McLorie, A.E Khoury and W Farhat Urology Volume 61, Issue 1, Page 224 (January 2003)

FIGURE 2
Source: Urology 2003; 61:224

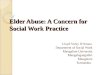
8. Active arterial extravasation
Focal ill defined areas of
contrast leak with different
configurations with high
attenuation values(85-370
HU) on early scans and will
appear as more hyper
attenuating than blood pool
and show spread and
expansion in to surrounding
tissue on a delayed scans

Active arterial haemorrhage in a patient in marginally unstable condition.
Harris A C et al. Radiographics 2001;21:S201-S214©2001 by Radiological Society of North America

Active haemorrhage
Dinkel H et al. Radiology 2002;223:723-730©2002 by Radiological Society of North America

Active haemorrhage in a 35-year-old man who sustained left flank penetrating trauma from a stab wound.
Alonso R C et al. Radiographics 2009;29:2033-2053©2009 by Radiological Society of North America

9.Devascularized kidney
Diffuse non-perfusion of kidney Most often from a clot that forms in an
incompletely torn renal artery

10.PUJ avulsion
Occurs due to sheering
injury at the fixation point
as it gets stretched over
the transverse process
Partial / complete
In complete avulsion no
ureter is opacified on
delayed images

Avulsion of the ureteropelvic junction in a 49-year-old man who had sustained blunt trauma.
Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America

AAST grading of the Renal Injury
Common consensus grading for
renal injuries between
radiologists and surgeons
Abdominal CT or direct renal
exploration is used to
accomplish injury classification
Now it is a standard method
adopted for radiological
reporting.

AAST Renal Injury Scale -1989

AAST Renal Injury Scale - 2011 Grades I, II, and III remain unchanged.
Grades IV and V are updated as follows:
Grade IV
○ Originally encompassed contained injuries to the main renal artery and vein, and
collecting system injuries.
○ Revision: adds segmental arterial and venous injury, and laceration to the renal
pelvis or ureteropelvic junction. Multiple lacerations into the collecting system used
to be considered a shattered kidney (Grade V), but now remains Grade IV.
Grade V
○ Originally included main renal artery or vein laceration or avulsion, and multiple
collecting system lacerations (shattered kidney).
○ Revised classification includes only vascular injury (arterial or venous) and
includes laceration, avulsion or thrombosis.
Revision of current American Association for the Surgery of Trauma renal injury grading system. J Trauma 70(1):35-37, 2011.

AAST: new versus old
2011
1989

Renal trauma management Interventional radiological perspective
CT Classification of Renal Trauma
Grade Usual management Remarks
Grade 1,2,3 Conservative Management
Intervention needed in presence of active hemorrhage with angio-
embolization/ Surgery in those with hemodynamic instability
Grade 4
Trial of conservative management provided the patient is
hemodynamically stable with no expanding hematoma
PCS injury managed with interventional radiology techniques
Grade 5
Complete PUJ disruption and renal pedicle avulsion needs surgical
repairPartial PUJ avulsion treated with
interventional radiology techniques
Renal artery thrombosis and devascularization -thrombolysis or
stenting within few hours

Follow up imaging
Needed to look for the resolution of injury
Usually not indicated for Grade 1-3 and grade 4 renal
injuries without urinary extravasation
Grade 4 injuries with urinary leak on previous scan
Grade 5 renal injuries who were managed conservatively
Patients with complications( fever, fall in HCT or clinical
instability)
Associated co-morbidity

Complications after renal trauma 3-10% of cases.
Early complications
Urinoma –most common
Delayed bleeding -1-2 weeks
Urinary fistula
Abscess and hypertension
Late complications
Hydronephrosis
Arteriovenous fistula
Pyelonephritis
Calculus formation
Delayed hypertension

Case 1
Grade 1 & 2 renal injury, Subcapsular hematoma. CT scan of the abdomen with intravenous contrast
in a patient after a motor vehicle collision shows cresentic high-density fluid collection around the left
kidney. Note the well-defined outer margin and the mild deformity of the renal parenchyma.

Case 2 Grade 2 renal injury,
subcapsular and perinephric
hematomas. Contrast-
enhanced CT scan of the
abdomen on a patient with
hematuria after a motor
vehicle collision shows an ill-
defined fluid collection in the
left perinephric space. There
is also a subcapsular
hematoma with deformity of
the renal parenchyma.

Case 3
Grade 2 renal
laceration. Contrast-
enhanced CT scan of
the abdomen after a
motor vehicle collision
shows a superficial
(less than 1 cm deep)
renal parenchymal
defect with a large
perinephric hematoma.

Case 4
Grade 3 renal laceration. CT scan of the abdomen after intravenous contrast administration shows irregular nonenhancing renal parenchymal defect with extension greater than 1 cm deep to near the renal pelvis.

Case 5
Renal infarction. Contrast-enhanced CT scan of the upper abdomen in another patient after a motor vehicle collision shows a segmental area of nonenhancement in the upper medial left kidney without associated renal laceration.

Case 6
Lacerations extending to the collecting system. Contrast-enhanced CT scan of the abdomen
in a patient with hematuria after a motor vehicle collision shows deep lacerations extending
into the collecting system of the right kidney. Extension into the collecting system is
confirmed by urinary contrast extravasation on delayed image through the kidney in
excretory phase. Grade 4 injury

Case 7
Shattered left kidney. Contrast-enhanced CT scan of the abdomen in a patient with
hematuria after a motor vehicle collision shows several deep lacerations extending into
the collecting system of the left kidney with separation of the fragments. Grade 4 injury

Case 8
Contrast-enhanced CT scan of the abdomen shows nonenhancement of left kidney
with non opacified left renal artery and hilar fat stranding suggesting renal artery
injury with thrombosis – Devascularization injury and associated left perinephric
hematoma- Grade 5 injury

Case 9
Fracture of the left lower pole of the kidney. Contrast-enhanced CT scan of the abdomen shows non
enhancement of the lower pole of left kidney. Extension into the collecting system is confirmed by urinary
contrast extravasasation on delayed image through the kidney in excretory phase Grade 4 Injury.

Case 10
Splenic laceration with perisplenic and perinephric hematoma and left partial
PUJ avulsion- Grade 4 injury


Case 11
Shattered right kidney with pseudo aneurysm formation. Right renal angiogram pre and
post embolization of the aneurysm. Spasm of the right proximal renal artery is noted

Case 12
Non enhancing right kidney, perinephric hematoma and right renal artery occlusion on selective angiogram – Grade 5 injury

Case 13 ?
Suspicious of Grade 4 injury – Needs a delayed excretory phase image

Multiple renal lacerations in a 9-year-old boy who had sustained blunt abdominal trauma and intra-abdominal injury. Grade 4 with active bleed
Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America
Case 14

FCT scan shows capsular rim nephrogram in the left kidney (arrows) after a renal infarction.
Harris A C et al. Radiographics 2001;21:S201-S214©2001 by Radiological Society of North America
Case 15

Alonso R C et al. Radiographics 2009;29:2033-2053©2009 by Radiological Society of North America
Case 16a

Alonso R C et al. Radiographics 2009;29:2033-2053©2009 by Radiological Society of North America
Case 16b

Partial tear of the left ureteropelvic junction (grade IV injury) in a 50-year-old woman who was involved in a motor vehicle accident.
Alonso R C et al. Radiographics 2009;29:2033-2053©2009 by Radiological Society of North America
Case 16c


Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America
Case 17a

Traumatic occlusion of the main renal artery in a 17-year-old boy who had sustained blunt abdominal trauma.
Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America
Case 17b

Traumatic occlusion of the main renal artery in a 38-year-old man who had sustained blunt abdominal trauma.
Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America
Case 17c

Laceration of the renal vein in an 18-year-old woman who had sustained blunt abdominal trauma. Grade 5 injury
Kawashima A et al. Radiographics 2001;21:557-574©2001 by Radiological Society of North America
Case 18

Case 19
Fractured kidney with PCS injury and urinoma

Case 20
Pseudo aneurysm of segmental renal artery


Conclusion Patient with hematuria after abdominal trauma should raise suspicion of
renal injury
Hematuria may not be present in patients with main renal artery thrombosis
or devascularized kidney
Radiology evaluation is needed to confirm and grade the injury
FAST is a rapid and well accepted tool for triage
CECT is the modality of choice to grade and look for complications.
Nephrographic phase and delayed excretory phase is needed, Be watchful
about the CT phases of contrast in kidney, ask for delayed when needed.
Most renal injury can be conservatively treated
Interventional techniques and minimally invasive procedures expand the
borders for conservative management and kidney salvage
Be familiar with new AAST grading,

Thank you