Embed Size (px)
Citation preview

Women’s health
AuthorsKatharine Gascoigne MRPharmsDr Sharmila Chauhan PhD MRPharmSDoreen Cochrane MRPharmS ▶Click here to continue

Women’s health
▶ Menstrual problems ● The changes caused during the menstrual cycle
● The treatments for menorrhagia available in the pharmacy
● The causes of amenorrhoea
● Common drugs that can interfere with the menstrual cycle
▶ Practical Approach 1What is SPD in pregnancy and how is it treated?
▶ Treating endometriosis● The incidence, prevalence and symptoms
of endometriosis
● How endometriosis is diagnosed and pain is managed
● The hormonal and surgical options available for treatment
● The answers to common questions on fertility
▶ Practical Approach 2Which LARC products will suit this patient?
▶ Management of lupus● The pattern of disease in lupus and the organs
commonly affected
● The key diagnostic signs you should know
● The different treatment options considered in lupus
● Lifestyle and management advice pharmacists can offer patients.
▶ Practical Approach 3Bleeding and depression with an IUD
Click here to continueThis toolkit is made up of three Update modules previously published in C+D magazine in August 2012 and online at chemistanddruggist.co.uk/update ▶
Contents Click on the green arrows to navigate directly to chapters or pages

Menstrual problemsKatharine Gascoigne MRPharmS
▶ ▶▶
Return to contents

▶ ▶▶
Return to contents
Asha Fowells MRPharms
Menstrual problems are one of the four most common reasons women of reproductive age visit their GP. This article gives an overview of the menstrual cycle, examining the roles played by the different hormones involved. It discusses three menstrual problems – menorrhagia (heavy periods), amenorrhoea (absent periods) and dysmenorrhoea (menstrual pain) – and how pharmacists can help sufferers manage their symptoms.
MenorrhagiaMenorrhagia is menstrual blood loss that interferes with a woman’s physical, emotional, social and material quality of life. It can occur alone or in combination with other symptoms. It is usually considered to be a monthly menstrual blood loss in excess of 80ml.
Around a third of women describe their periods as heavy, but only around 10 per cent are classed as having menorrhagia. In general, if the bleeding is such that the woman has to use tampons and towels together, is experiencing flooding, passing clots and is finding that the bleeding is impacting on her daily life, menorrhagia should be considered.
In 40 to 60 per cent of cases there is no obvious cause of the heavy bleeding; this is termed dysfunctional uterine bleeding. About 20 per cent of cases are associated with anovulatory cycles and menorrhagia is most common at the beginning and end of a woman’s reproductive life.
Other causes include:● fibroids● pelvic inflammatory disease● endometriosis● cervical or uterine polyps● polycystic ovary syndrome (PCOS)● hypothyroidism ● cancer.
A full blood count is usually performed to establish whether the woman is anaemic and, if necessary, iron tablets are prescribed.
Assuming there is no serious underlying cause, the first-line treatment for menorrhagia is the levonorgestrel-releasing intra-uterine system (LNG-IUS). It should be used for a minimum of 12 months and reduces blood loss by 71 to 96 per cent. Possible side effects are irregular bleeding for six months or more, breast tenderness, acne, headache and amenorrhoea.
If the LNG-IUS is not acceptable, for example because the woman does not want long-acting contraception, tranexamic acid can be prescribed, or is available as a P medicine for menorrhagia over several cycles in women with regular, 21 to 35-day cycles. It is a plasminogen-activator inhibitor, preventing the dissolution of thrombosis that leads to menstrual flow. It is taken for the three to four days of heaviest bleeding and can reduce blood loss by up to 58 per cent. Usually two tablets are taken three times a day for a maximum of four days,

▶ ▶▶
Return to contents
although the dose may be increased up to 4g daily for very heavy menstrual bleeding. Treatment should not be initiated until menstrual bleeding has started, and should be stopped if there is no improvement after three months.
NSAIDs are another choice: mefenamic acid, naproxen and ibuprofen are most commonly used and have been shown to reduce blood flow by 20 to 50 per cent. They should be taken throughout menstruation and work by reducing uterine prostaglandin levels. This also leads to a reduction in dysmenorrhoea but, if blood flow is not reduced within three months, treatment should be ceased.
The combined oral contraceptive (COC) is also used to treat menorrhagia, but has a number of significant side effects and is only an option if contraception is desired.
The third-line treatment for menorrhagia is norethisterone, at a dose of 5mg three times a day from day five to day 26 of the menstrual cycle. Side effects include weight-gain, bloating, headaches and acne. It works quickly and can stop heavy bleeding within 48 hours. Injected medroxyprogesterone acetate is also sometimes used.
If drug treatment is not effective, the next step is surgery according to whether the cause of menorrhagia is due to the presence of fibroids. There are no specific lifestyle changes that can reduce menorrhagia.
The menstrual cycleMenstruation is the shedding of the endometrium (lining of the uterus) accompanied by bleeding. It occurs roughly once a month throughout a woman’s reproductive life, except during pregnancy. Girls start to menstruate at an average age of 12 (at menarche) and continue until they reach menopause, usually between 50 to 55 years.
Each cycle normally lasts 25 to 36 days. Around 35 to 40ml of blood is typically lost over an average of five days.
The menstrual cycle is divided into three phases:
1. The follicular phase begins on day one of the menstrual cycle, classed as the first day of bleeding. At the beginning of this phase the endometrium is thick with fluids and nutrients, ready to receive a fertilised egg. If this does not happen, the levels of oestrogen and progesterone fall, causing the top layers of the endometrium to break down. As they are shed, menstrual bleeding occurs.
At this time the pituitary gland increases its production of follicle-stimulating hormone (FSH), which stimulates the growth of between three and 30 egg-containing follicles. The level of FSH then decreases, leaving just one follicle to continue to grow. This follicle starts to produce oestrogen and the other follicles break down.
This phase lasts an average of 13 to 14 days. It is the phase that varies most in length and tends to become shorter near menopause. The follicular phase ends when there is a surge in the level of luteinising hormone (LH).
2. The ovulatory phase then begins, lasting just 16 to 32 hours. It starts with a huge increase in the level of LH produced by the pituitary gland. LH stimulates the dominant follicle to bulge then rupture from the surface of the ovary, releasing the egg. The level of FSH also increases at this time. As the egg is released, the ovulatory phase ends.
3. The luteal phase begins after ovulation and lasts about 14 days. During this phase the ruptured follicle closes after releasing the egg and forms the corpus luteum. This structure produces increasing quantities of progesterone, which makes the endometrium thicken in preparation for receiving a fertilised egg. Progesterone also causes the mucus in the neck of the cervix to thicken and the body temperature to increase slightly. The level of oestrogen is high during this phase and also causes thickening of the endometrium.
If the egg is not fertilised, the corpus luteum degenerates after 14 days. Progesterone is no longer produced and levels of oestrogen decrease, resulting in the start of the next menstrual cycle.

▶ ▶▶
Return to contents
Asha Fowells MRPharms
AmenorrhoeaAmenorrhoea is the absence of menstruation and is classed as either primary or secondary.
Primary amenorrhoea is defined as the failure of menstruation by the age of 16 years in the presence of normal secondary sexual characteristics, or 14 years in the absence of other evidence of puberty. Primary amenorrhoea is not common, and the causes can range from delayed periods to abnormal development of the reproductive system.
Secondary amenorrhoea is defined as the absence of periods for at least six months in a woman who has previously had regular periods, or 12 months if she has previously had oligomenorrhoea (bleeds less frequently then six-weekly).
The prevalence of amenorrhoea not due to pregnancy, lactation or menopause is around 3 to 4 per cent in women of reproductive age and its treatment depends on the cause. Complications of amenorrhoea can include osteoporosis (prophylaxis may be required), cardiovascular disease, infertility and psychological distress, depending on its cause. One in three cases of secondary amenorrhoea is caused by PCOS, other symptoms of which include hirsutism, fertility problems and weight gain. Treatment options include:● weight loss and exercise● COC or anti-androgen therapy● metformin● clomifene and laparoscopic ovarian drilling.
Hypothalamic amenorrhoea can be caused by stress, excessive weight loss, excessive exercise or systemic illness and treating the cause should result in a restoration of menses; amenorrhoea due to hypothyroidism should cease after several months of treatment with levothyroxine.
Hyperprolactinaemia can cause amenorrhoea and can be drug-induced, in which case stopping the causative drug could be considered. Patients should be made aware that a small number of women with secondary amenorrhoea will become pregnant, so contraception should still be considered.
DysmenorrhoeaDysmenorrhoea is pain in the lower pelvis associated with menstruation. It is thought to be caused by prostaglandins and leukotrienes in the menstrual fluid creating vasoconstriction in the uterine vessels, leading to uterine contractions and pain. It is very common, affecting 40 to 70 per cent of women at some time. Risk factors for dysmenorrhoea include long duration of menses, early menarche, smoking, alcohol and obesity. Primary dysmenorrhoea occurs in adolescent girls with no underlying pathology. The pain often starts shortly before menstruation and lasts for up to 72 hours, improving as menses progresses. Nausea, vomiting, migraine, bloating and emotional symptoms may be experienced. ▶

▶ ▶▶
Return to contents
Secondary dysmenorrhoea is when menstrual pain – which often persists after menstruation has finished – appears after several years of painless periods and is associated with some forms of pelvic pathology. Causes of secondary dysmenorrhoea include:● fibroids● adenomyosis (uterine thickening caused by endometrial tissue moving into the outer muscular walls of the uterus)● endometriosis● pelvic inflammatory disease● cervical or uterine adhesions ● developmental abnormalities.
Having a hot bath or applying warmth to the area usually eases the discomfort of dysmenorrhoea, as does massage to the abdomen and/or back or lying down flat on the back. Acupuncture or the use of a TENS machine may be of benefit.
The most commonly used drugs for dysmenorrhoea are NSAIDs due to their inhibition of prostaglandin synthesis. If there is no benefit after three cycles, then a COC can be considered; these are thought to reduce prostaglandin release during menstruation.
Other treatments less commonly used include depo-medroxyprogesterone acetate, LNG-IUS, danazol and, rarely, leuprolide acetate.
Red flag menstrual symptoms ● Persistent bleeding outside menstruation● Post-coital bleeding● Pain during sexual intercourse● Rectal pain or bleeding
Drugs that can interfere with the menstrual cycle
● NSAIDs, if taken regularly, can interfere with ovulation.
● Steroids and immunosuppressants in high doses can prevent the pituitary gland from producing enough FSH and LH for ovulation to occur, resulting in irregular menstrual cycles.
● Some antipsychotics, antiepileptics and antidepressants (other than SSRIs) may cause hyperprolactinaemia, which can cause missed or irregular periods.
● Carbimazole and propylthiouracil can cause hypothyroidism, which in turn can cause amenorrhoea.
Further information● For women requesting advice on menstrual problems, the following websites are good sources of information and support: ▶ nhs.uk
▶ womens-health-concern.org
▶ pms.org.uk
▶ womens-health.co.uk
▶ endometriosis-uk.org

▶ ▶▶
Return to contentsReturn to contents
Tips for your CPD entry on menstrual problems
Refl ect What happens during the luteal phase of the menstrual cycle? What is the fi rst-line treatment for menorrhagia? What causes secondary amenorrhoea?
Plan This article gives an overview of the menstrual cycle and the roles played by hormones. It also discusses the causes, symptoms and treatment of menorrhagia, amenorrhoea and dysmenorrhoea.
Act Read the article and the suggested reading below then take the 5 Minute Test.
● Find out more about menorrhagia on the Patient UK website▶ tinyurl.com/menstrual11
● Read the brief decision aid about heavy menstrual bleeding management options▶ tinyurl.com/menstrual12
● Revise your knowledge of the OTC supply of tranexamic acid from Manx Healthcare▶ tinyurl.com/menstrual13
● Read more about amenorrhoea on the NHS Choices website▶ tinyurl.com/menstrual14
● Find out more about PCO▶ tinyurl.com/menstrual15
● Update your knowledge of dysmenorrhoea▶ tinyurl.com/menstrual16
Evaluate Are you now confi dent in your knowledge of the causes and symptoms of menorrhagia, amenorrhoea and dysmenorrhoea? Could you give advice to patients about their treatment?
Take the 5 Minute TestClick here to check what you’ve learnt by taking our short MCQ test and get a CPD log sheet if you pass
(Internet connection required)

▶ ▶▶
Return to contents
Practical Approach■ Test yourself and your team with this scenario based on pharmacy practice
A woman comes in the pharmacy, clutching her pregnancy notes and with tears running down her face.
Fearing the worst, you usher her into the consultation room so that she can have some privacy.
“I’ve just had my 24-week appointment with the midwife,” she says. “Everything is fine with the baby, but I’m having some pain when I walk and it’s starting to stop me doing things, like sitting on the floor to play with my four-year-old. “The midwife was running late so she didn’t say much, other than that it would get worse as I got bigger but it would go away once the baby comes. She told me it was pretty common and nothing to worry about, but it’s really uncomfortable.
“I’ve got months to go until the baby is born. What am I going to do?”
You glance at her pregnancy notes and next to today’s date see that the midwife has written “SPD”.
● What does SPD stand for?SPD stands for symphysis pubis dysfunction (also known as pelvic girdle pain, or PGP), and affects up to one in four pregnant women. There are various theories as to why it happens:● higher than normal levels of the hormone relaxin causing the pelvic ligaments to loosen too much and too early, causing movement in the normally stable pelvis● one of the three joints in the pelvis becoming stuck, causing asymmetric movements and leading to inflammation● separation of the symphysis joint in the pelvis.
continued ▶
What is SPD in pregnancy and how is it treated?

▶ ▶▶
Return to contents
Practical Approach
What is SPD in pregnancy and how is it treated? (continued)
● What are the symptoms?The condition can start at any point during pregnancy (usually in the second trimester) and is progressive due to the increasing weight of the growing baby. Pain, which often starts as a dull ache or an occasional stabbing sensation but rapidly worsens, can occur in the pubic region, the inside of the thighs, the hips and the buttocks. It can cause a clicking sensation or sound.
Any activity that puts strain on the pelvis can cause the pain to increase, including walking, climbing stairs, turning over in bed and lifting or pushing heavy objects. This means that the condition has a huge impact on everyday life, as well as causing sufferers to feel isolated and low.
● What are the possible treatment options, both in the pharmacy and from specialist teams?Getting help early can make a huge difference. A specialist obstetric physiotherapist will measure and
fit a pelvic support belt that limits the movement of the joint and keeps the pelvis aligned, and provide some hands-on treatment.
Suitable analgesia includes paracetamol, heat therapies and TENS. Resting and avoiding activities that trigger the pain can slow progression, but some women may need crutches or even a wheelchair as their pregnancy continues. Small adjustments can make a big difference, such as sitting on a carrier bag to make getting in and out of the car easier, going up the stairs on hands and knees, and sleeping with a pillow between the legs to keep the pelvis in line. However, the biggest difference will occur when the baby is born, hormones start to return to pre-pregnancy levels and the pressure on the pelvis is relieved.
● More information is available at: ▶ nhs.uk/conditions/pregnancy-and-baby/
pages/pelvic-pain-pregnant-spd.aspx
▶ pelvicpartnership.org.uk
If you identify a gap in your knowledge, consider making a CPD entry.

Treating endometriosisDr Sharmila Chauhan PhD MRPharmS
▶ ▶▶
Return to contents

▶ ▶▶
Return to contents
Endometriosis affects 10 to 15 per cent of all menstruating women aged 25 to 44 years. The condition can range from mild to severe and can be both physically and emotionally debilitating. Currently around 1.5 million women in the UK suffer from endometriosis and a significant number remain undiagnosed.1
Endometriosis is characterised by the presence of endometrial-like cells outside the uterus. These are most commonly found inside the pelvis, around the ovaries and fallopian tubes, on the ligaments, intestines, bladder, vagina and the rectum. In rarer cases, these ‘misplaced’ cells also grown into the muscle layer of the uterus (adenomyosis), the skin, eyes, spine, lungs and the brain.
The precise cause is unclear. Research has suggested a number of contributing factors, including endometrial cells travelling back up the fallopian tubes and onto the ovaries during menstruation, endometrial cells replacing other cells in tissues outside the uterus, transportation of endometrial cells to other parts of the body via the blood or lymphatic system, and immune dysfunction.
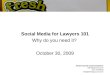
Abdominal wall
Intestines
Peritoneum
Appendix
Fallopian tubes and ovaries
Uterus
Cervix
Bladder
Rectum
Vulva
The organs inside a woman’s abdomen. Possible sites where endometriosis can develop are indicated in blue

▶ ▶▶
Return to contents
Endometriosis is an inherited condition and common in first-degree relatives of women with the condition. It is most common in menstruating women and generally becomes remissive after the menopause. It is more common in women who have: ● their first baby after age 30 years● never had a baby● short menstrual cycles (less than 27 days)● certain structural abnormalities of the uterus.
The condition is less common in women who have had several pregnancies, use low-dose oral contraceptives, or who exercise.
SymptomsLike their uterine counterparts, endometrial cells outside the uterus are also under the influence of sex hormones during menstruation, and will undergo proliferation and swelling under the influence of oestrogen before a period. However, since there is nowhere for them to be shed, they accumulate and cause inflammation, pain and, eventually, the formation of scar tissue. Bands of fibrous tissue (adhesions) may form between the structures in the abdominal cavity, causing neighbouring organs to stick together, leading to further complications.2,3
Typical symptoms include:2,3 ● severe dysmenorrhoea ● pain in lower abdomen between menstrual cycles (this may not be as painful as period pain but may be more constant)● painful sexual intercourse● menstrual irregularities● bowel or bladder symptoms (eg need to urinate frequently, pain during urination, constipation, rectal bleeding during menstruation).
Adhesions on the ovaries can form a cyst that bleeds
Patient questions on endometriosis1. Will I be able to have a baby? The majority (60 to 70 per cent) of women with endometriosis have no problems getting pregnant. If a woman wants conceive in the future, she should discuss this with her doctor, since this will play a role in the management of the condition. Pharmacological treatment for endometriosis should be avoided for women who are trying to conceive.3
2. What are the options if I want to have a baby and have difficulty conceiving?Data on the benefits of intrauterine insemination (IUI) in women with endometriosis are unclear, although IVF can be considered. Pregnancy rates, however, are lower in women with endometriosis than those with tubal infertility.3
3. Will having a baby ‘cure’ my endometriosis? Pregnancy is not a ‘cure’ for endometriosis, although some women may experience temporary benefit while pregnant. In most cases, symptoms return after giving birth and the menstrual cycle resumes.1
4. Can I use any alternative medicines? Systemic reviews indicate that a variety of alternative medications have been shown to relieve dysmenorrhoea, including: high frequency TENS, acupuncture, vitamin B1 and magnesium. One randomised controlled trial provided evidence that vitamin E may relieve primary dysmenorrhoea and reduce blood loss. The efficacy of these treatments in endometriosis-associated dysmenorrhoea is unclear.
into itself each month, often called a ‘chocolate cyst’. In severe cases of endometriosis, the adhesions may block the fallopian tubes, impairing fertility. Infertility has also been reported in women with mild cases of the disease but the mechanism by which this occurs is not understood. Between 25 and 50 per cent of women who are infertile have endometriosis.2,3
Endometriosis has a number of psychological effects and women with the condition may report depression, isolation and anxiety.

▶ ▶▶
Return to contents
DiagnosisDiagnosis of endometriosis cannot be made on symptoms alone, and in many women can be delayed by up to 12 years. This is because of a lack of awareness among women, lack of specialists, the asymptomatic nature of the condition and reluctance of women to ask for help until the condition is severe.
The diagnosis of endometriosis is all too often a consequence of a different medical investigation, for example, during investigation of fertility issues.1 Improved awareness of the condition together with provision of resources to enable diagnosis may help to improve prognosis of women with the condition. Diagnosis requires specialist investigation. Currently the gold standard is laparoscopy, which allows the pelvis to be visually inspected and the size and location of adhesions in the abdominal cavity to be assessed.
TreatmentManagement of endometriosis currently includes symptomatic treatment, hormonal intervention, and surgery.
First-line treatment usually includes non-steroidal anti-inflammatory drugs (NSAID), such as ibuprofen, naproxen, mefenamic acid, or diclofenac. These are usually prescribed to women who are experiencing a lot of pain, those who do not wish to use hormonal treatments, and those who are awaiting referral from their GP to a specialist. However, the Royal
College of Obstetricians and Gynaecologists (RCOG) states “that although NSAIDs may be effective in endometriosis-associated pain, there are too few randomised controlled trials to assess their effectiveness”.3
Patients who cannot take NSAIDs (eg those with stomach ulcers or asthma) can be prescribed paracetamol, and studies suggest regular use of the drug may be more effective than as-required use. In patients in whom adequate pain relief is not achieved, codeine may be added to paracetamol and/or an NSAID.
Hormone therapyHormonal treatments are used to interfere with oestrogen production and/or activity at its receptors, thereby shrinking the adhesion size. These treatments can also be used to treat the pain and bleeding disorders associated with endometriosis.
Combined oral contraceptives (COCs) are considered the first-line hormonal treatment, and may be taken continuously without a break, or in a tricycling (taking three packs without a break) regimen to control endometriosis. Women taking a COC may report beneficial effects such as lighter and less painful periods. Other symptoms such as painful sex and pain in the pelvic area may also improve.
Progesterone agents act by decidualisation
and atrophy of the endometrium. In studies, medroxyprogesterone has been shown to be effective in pain suppression. Adverse effects of this type of drug include weight gain, fluid retention, depression, and breakthrough bleeding.
Long-acting progesterones can be used in patients with compliance issues and also in women who are uncomfortable with a daily tablet intake. They may be more acceptable in patients who are familiar with depot or intrauterine devices for contraceptive use.
Women should be reassured that long-acting devices are effective and studies show that the levonorgestrel intrauterine system (LNG-IUS) can reduce endometriosis-associated pain and, if inserted during laparoscopic surgery, can reduce the recurrence of dysmenorrhea.
Androgens (eg danazol) act through an inhibition of the midcycle follicle-stimulating hormone (FSH) and luteinising hormone (LH) surges as well as prevention of steroidogenesis in the corpus luteum.
Although studies show danazol is as effective as the newer agents, its adverse effects reduce its acceptability. These include acne, oily skin, weight gain, deepening of the voice, and facial hirsutism. It also has a number of side effects related to low oestrogen levels: hot flushes, emotional lability, vaginal dryness, and reversible breast atrophy. The usual dose is 200 to 800mg daily in up to four

▶ ▶▶
Return to contents
divided doses, adjusted to achieve amenorrhoea, usually for three to six months. These can bring on an ‘artificial menopause’ as they reduce oestrogen and progesterone production.
GnRH analogues (eg buserelin, goserelin, nafarelin, leuprorelin, and triptorelin) inhibit pituitary gonadotrophin release. Preparations are taken as a nasal spray or injection. Goserelin and leuprorelin are the most commonly used agonists and have been shown in studies to reduce pain associated with endometriosis.
Reports suggest that as many as 85 to 100 per cent of women experience pain suppression following GnRH therapy and that these benefits may persist for between six to 12 months after treatment cessation. Research also shows GnRH treatment can also relieve the pain and bleeding associated with extrapelvic distant endometriosis.
Adverse effects of GnRH agonists include hot flushes, vaginal dryness, reduced sex drive, headaches, reduced bone density, insomnia and amenorrhoea, some of which disappear on cessation. Pharmacists should remind patients that they may experience flare up in symptoms during the first few days of treatment.
Manufacturers recommend a single course of six months duration, although some specialists may prescribe a repeated or extended course. There is limited data regarding the safety and efficacy of this approach. Alternatives include using a three-month
course or repeated shorter courses. The latter may offer sustained beneficial effect combined with lower impact on bone mineral density and fewer hypo-oestrogenic adverse effects.There is debate as to whether oestrogen/progesterone “add-back” therapy should be used to prevent osteoporosis and hypo-oestrogenic symptoms experienced by women receiving GnRH therapy for endometriosis. Low-dose hormone replacement therapy (HRT) has been shown to prevent loss in bone density and to relieve vasomotor symptoms without compromising the efficacy of GnRH regimens; these data suggest that inclusion may be beneficial for many women.
Surgical treatmentThe RCOG guidelines3 outline the ideal treatment of endometriosis as diagnosis followed by surgical removal of adhesions. There are three types of surgery: ● Conservative – reproductive potential is maintained● Semiconservative – reproductive ability is diminished but ovarian function is retained● Radical – when the uterus and ovaries are completely removed.
Surgery usually includes removal of adhesions and correction of any related anatomical distortions. The former are ablated using either laser energy or electrosurgical techniques.
Laparoscopic uterine nerve ablation (LUNA) involves the destruction of a small segment of ligament that
carries nerve fibres within the pelvis. However, it has not been shown to be efficacious and therefore is not advised for this patient group. When deciding on the type of surgery, the patient’s age, desire for children and their current quality of life should all be considered.
Dr Sharmila Chauhan is a pharmacist and medical writer with a PhD in clinical pharmacology
References1. Endometriosis UK Available at: http://www.endometriosis-uk.org/information/whatisit.html Accessed June 20122. Endometriosis Merck Manuals. Available at: http://www.merckmanuals.com/home/womens_health_issues/endometriosis/endometriosis.html. Accessed June 20123. The Investigation and Management of Endometriosis. Royal College of Obstetricians and Gynaecologists. 2006

▶ ▶▶
Return to contentsReturn to contents
For more information▶ fpa.org.uk/helpandadvice/contraception/
longactingreversiblecontraceptionlarc
▶ guidance.nice.org.uk/CG156
▶ fsrh.org/pages/clinical_guidance.as
● Endometriosis UK for women with endometriosis▶ endometriosis-uk.org
● Endometriosis SHE trust ▶ shetrust.org.uk
● RCOG ▶ rcog.org.uk/womens-health
● The Pain Society ▶ britishpainsociety.org

▶ ▶▶
Return to contentsReturn to contents
Refl ect What are the main symptoms of endometriosis? What are the adverse eff ects associated with GnRH analogues? How does endometriosis aff ect fertility?
Plan This article discusses endometriosis and includes information about causes, symptoms and diagnosis. It also describes the hormonal and surgical treatments available and answers common questions that patients with endometriosis might have about fertility.
Act Read the article and the suggested reading below then take the 5 Minute Test.
● Read more about endometriosis on the Patient UK website▶ tinyurl.com/endometriosis11
● Find out about the advice you could give to patients who are suff ering from long term pain on the NHS Choices website▶ tinyurl.com/endometriosis12
● Research self-help organisations and websites for women who suff er from endometriosis. Find out about local groups and print out any useful information leafl ets.
● Consider carrying out training with your pharmacy staff so that women who prefer to talk to a female or older or younger person can be made to feel more at ease.
Evaluate Are you now confi dent in your knowledge of the symptoms and treatment of endometriosis? Could you and your staff confi dently give advice to patients?
Tips for your CPD entry on treating endometriosis
Take the 5 Minute TestClick here to check what you’ve learnt by taking our short MCQ test and get a CPD log sheet if you pass
(Internet connection required)

▶ ▶▶
Return to contents
Practical Approach■ Test yourself and your team with this scenario based on pharmacy practice
Which LARC products will suit this patient?A young woman visits the pharmacy and requests a consultation for emergency hormonal contraception (EHC). You head into the consultation room and, after ensuring it is appropriate, decide to provide her with EHC.
As you come back, the woman looks anxious. “It’s really embarrassing, but this is the second time I’ve had to have this in the last few months,” she says. “My husband and I have two children and we really don’t want anymore. He’s thinking about having a vasectomy, but using condoms clearly isn’t working for us while he makes up his mind!”
You ask if she’s considered oral contraception.
“I don’t think that will work. I wasn’t very good at remembering to take the pill when I was younger, so is there something else I can do?”
● What are the four methods of long-acting reversible contraception? What are their effectiveness and benefits?There are four methods of long-acting reversible contraception (LARC), any of which may be suitable for this woman, and all of which are deemed by NICE to be more cost-effective than combined oral contraceptives even at one year of use and have more than 99 per cent effectiveness:
● The progesterone-based contraceptive injection needs administering every eight or 12 weeks depending on the product used. It is associated with menstrual disturbances and weight gain, and it can take up to a year for fertility to return once it is stopped.
● The implant also contains progesterone and works for three years, though it can be removed sooner if required. It has been associated with irregular menstrual bleeding, acne and discomfort on insertion and removal, and fertility returns to normal as soon as it is removed. ▶

▶ ▶▶
Return to contents
Practical Approach
Which LARC products will suit this patient?(continued)
● The intrauterine system (IUS) releases progesterone over five years (though it can be removed sooner at the woman’s request), and is more than 99 per cent effective. Disadvantages include discomfort on insertion and removal, and it can cause irregular bleeding, acne and mood changes, though many women enjoy the amenorrhoea it can cause. The risk of ectopic pregnancy is lower than if no contraception is being used, but if the woman becomes pregnant with the IUS in situ, the risk jumps to one in 20 (this is also the case for IUDs). Fertility returns to normal upon removal.
● Intrauterine devices (IUDs) containing copper have been widely superseded by the IUS but are still an option for woman who prefer a non-hormonal method of contraception. They need replacing every five to 10 years, though fertility returns to normal as soon as they are removed. The most common side effects are vaginal bleeding and pain, and pelvic inflammatory disease and uterine perforation are
much less common than perceived (and are the same as for the IUS).
This woman should be provided with information on all the options available and offered the opportunity to ask any questions she may have in order to choose a method that she will then be able to use effectively. Not all methods will be available from her GP surgery as some require specialist training, but she will be able to access her preferred contraception locally due to referral pathways.
If you identify a gap in your knowledge, consider making a CPD entry.

Management of lupusDoreen Cochrane MRPharmS
▶ ▶▶
Return to contents

▶ ▶▶
Return to contents
Lupus is an autoimmune rheumatic condition and about 90 per cent of cases are in women. The disease has peak onset during the child-bearing years. In the UK, lupus affects about one in 750 Caucasian women, rising to one in 250 Asian and African-Caribbean women. People from an Asian or African-Caribbean background tend to have severe forms. Pharmacists can help raise awareness of the condition, support patients with medicines and provide healthy lifestyle interventions to help prevent cardiovascular disease.
What is lupus? Lupus is a complex illness that can affect many organs, most commonly the muscles and joints or tendons; nervous system; lungs; heart; kidneys; serous membranes and components of the blood. In lupus the body’s immune system becomes hyperactive, forming antibodies that attack normal tissues and organs. It tends to be characterised by periods of illness – called flares or exacerbations – and periods of remission.
About 70 per cent of cases are catergorised as systemic lupus erythematosus (SLE), among which about half of patients have non-organ threatening
disease. These patients have normal life expectancy and it is unlikely they will develop major organ involvement after the first five years of developing lupus. If the disease affects the major organs (heart, lungs, kidneys or liver), it may become life threatening.
Drug-induced lupus, which accounts for about 10 per cent of all cases, is a side effect of long-term use of certain medications. It tends to be mild and is usually reversible when the medicine is stopped. Potential causative drugs include isoniazid, hydralazine and procainamide. A further 10 per cent of patients have cutaneous, or discoid, lupus.
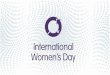
Systemic lupus erythematosus (SLE) rash on the skin of the face in a female patient, an autoimmune disease where the immune system attacks the body’s connective tissue, mainly in the skin, joints and kidneys.

▶ ▶▶
Return to contents
Some patients have a genetic predisposition to developing SLE. Many of the clinical manifestations of SLE are mediated by deposition of immune complexes in organs such as the kidney, resulting in lupus nephritis.
One or more environmental factors may trigger disease in genetically predisposed individuals. These factors include:● previous viral infections, especially with the Epstein-Barr virus● excessive ultraviolet light exposure● changes in the sex hormones, especially oestrogen.
Other environmental factors have been implicated in the pathogenesis of the disease. Autoantibodies may be present for many years before the clinical onset of lupus, and there may be increasing numbers of antibodies just before symptoms develop.
The development of clinical lupus results from abnormalities in B cells and T cells, defects in cell signalling, impairment of cell-surface protective mechanisms and failure in T-regulatory cells to prevent inflammation. If this process is interfered with chronically, this will result in tissue and organ damage. The prognosis from patients with lupus ultimately depends on the amount of permanent scarring or irreversible organ dysfunction accrued over the course of the illness. Treatment therefore aims to
eliminate inflammation and thrombosis, minimise organ damage and prevent cardiovascular disease.
DiagnosisExhaustion is one of the most common and persistent features of SLE. Lupus may start with flitting joint pains in the small joints of the hands and feet, and skin rashes – especially malar rash (a characteristic red or purple, mildly scaly facial rash) – which may be worse when exposed to strong sunlight. There may be swollen glands and mild hair loss. Raynaud’s phenomenon (whitening of the fingers) may occur. Depression is also an important symptom in lupus and patients may develop frequent mouth ulcers.
Patients presenting with these symptoms should be referred to their GP. A diagnosis of lupus or a related connective tissue disorder is often apparent after clinical assessment, urinalysis, and basic investigations such as full blood count (often showing anaemia or cytopenia), and renal and liver function tests; results indicating a high erythrocyte sedimentation rate (ESR) with a normal C reactive protein concentration are characteristic.
A blood test for anti-nuclear antibodies and anti-double-stranded DNA antibodies are the usual starting points when considering referral to specialist care. This will lead to more extensive testing, including detailed assessment of organ involvement and further autoantibody testing.
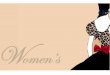
Raynaud’s phenomenon (whitening of the fingers) is one of the symptoms which may occurr.

▶ ▶▶
Return to contents
Treatment of lupus● Antimalarials such as chloroquine and hydroxychloroquine are effective in treating skin rashes, aches and pain and fatigue and reducing flares of the disease. They may protect against renal insufficiency and the occurrence of thrombotic events, diabetes, and reduced bone mineral density. They have a beneficial effect on lipid profiles, especially among patients treated with steroids. Hydroxychloroquine may be used alongside mycophenolate mofetil in the treatment of lupus nephritis.
The dose used at initiation of treatment with hydroxychloroquine for adults may be as high as 400-800mg daily, with an average maintenance dose of 200-400mg daily; the usual recommendation is for a daily dose of 1-3mg/kg daily to avoid retinal toxicity. Because of its long half-life, patients should be advised that it takes two to eight weeks to achieve effectiveness. Hydroxychloroquine is considered to be safe in pregnancy and breastfeeding.
● Immunosuppressants are commonly used to treat the condition. Azathioprine is widely used to suppress the immune response in SLE, but also affects other dividing cells – including white blood cells. It is often used if lupus is affecting the kidneys (lupus nephritis) and as a steroid-sparing agent. The usual dose is 1-2.5mg/kg body weight daily (usually 100-150mg daily). For most patients the drug is well tolerated but requires blood monitoring at least every three months. About five per cent
of patients cannot tolerate this medication due to immediate onset of nausea and altered liver function. Treatment with azathioprine should not be initiated during pregnancy but may be used during breastfeeding if its benefits outweigh the risks to the newborn.
Mycophenolate mofetil is an effective and safe alternative for many patients who cannot tolerate azathioprine. Initially mycophenolate was used in cases of lupus nephritis and to effect disease remission. It has now gained a place in other aspects of lupus including patients with muscle disease, low platelet counts and skin disease. The most common side effects are nausea and loose stools. It is not safe in pregnancy or breastfeeding and blood counts must be monitored monthly during treatment.
Methotrexate is used at a low dose, usually 7.5mg weekly, increasing if necessary depending on response and the side effects experienced by the patient. In view of the significant toxicity associated with methotrexate, patients should have a full blood count and renal and liver function tests checked before starting treatment, and at least every two to three months during maintenance therapy. Patients must be educated to report all signs and symptoms suggestive of infection and pulmonary toxicity immediately. ● Corticosteroids can be used, with the dose dependent on the severity of the patient’s illness. The most common side effects of corticosteroids are weight gain; ‘moon-face’; increased blood pressure;
osteoporosis; lowered resistance to infection and mood disturbances. Problems associated with the use of corticosteroids are minimised by using the lowest possible dose for the shortest period of time. Steroid-sparing drugs, such as azathioprine and mycophenalate mofetil, may be used to reduce the dose of corticosteroid. The patient’s blood pressure, glucose levels and lipid profile should be monitored during corticosteroid therapy, which is considered safe for use during pregnancy and breastfeeding.
Cyclophosphamide, cyclosporine, monoclonal antibodies and immunoregulators are used in the treatment of patients with severe disease.
Ongoing mananagement of lupusEducation is critical for patients, their carers and friends, and pharmacists can help them to access information about lupus and medicines used in its treatment to encourage concordance. Often, patients are concerned about the effects of the illness on their future physical mobility and employment. Because of the emotional and psychological consequences of the diagnosis and the role of depression in the illness, the hospital lupus team usually offers support from a specialist nurse counsellor. Patients are encouraged to alternate periods of activity with periods of rest to reduce symptoms of tiredness, and physiotherapists can support patients with a graduated exercise programme. ▶

▶ ▶▶
Return to contents
Pharmacists can help patients choose effective sun-blockers to reduce ultraviolet exposure. Patients should be advised to use a sunblock of factor 25 or greater, and that sunblock products are also available on prescription. Some OTC medications, such as sleep aids containing diphenhydramine, should be avoided by patients with thrombocytopenia due to haematological involvement. Many herbal treatments available in the pharmacy, including echinacea, are best avoided by patients with lupus.
In recent years, the treatment for lupus has broadened to include lifestyle factors, especially smoking cessation and reduction of cholesterol levels to prevent strokes and coronary artery disease; inflammation is associated with LDL lipoprotein levels. Management of related problems such as blood pressure, and prevention of conditions such as osteoporosis is important.
A balanced, healthy diet containing fish or fish oil supplements is encouraged. Alfalfa shoots, which are rich in the amino acid L-canavanine, trigger flares and should be avoided. Some patients avoid other foods which make their symptoms worse. The risks associated with live viral vaccinations must be individually assessed for all patients taking immunosuppressive medicines, and some patients can experience a flare of symptoms following vaccinations for illnesses such as influenza.Pregnancy presents particular challenges for the patient with lupus, especially if the mother has hypertension or reduced renal function. The
pregnancy should be planned well in advance wherever possible to minimise the risks to both the mother and foetus. Factors included in the pre-assessment for pregnancy in lupus include the manifestations of underlying disease, the past history of flares and past and current medications.
With proper management the majority of patients with lupus now lead full and active lives. Disparities continue to exist in the course of disease based on ethnicity and socioeconomic status and these are current areas of research.
Useful further information
▶ arthritisresearchuk.org
▶ lupus.org.uk
▶ thelupusinitiative.org
▶ sagepub.com Search for Lupus (An International Journal)

▶ ▶▶
Return to contentsReturn to contents
Refl ect In which ethnic groups is lupus likely to be more severe? Which treatments for lupus are safe for use in pregnancy and breastfeeding? What are the side eff ects of mycophenolate mofetil?
Plan This article describes the autoimmune rheumatic condition lupus and includes information about symptoms, diagnosis and treatment. Lifestyle advice and the challenges of lupus and pregnancy are also discussed.
Act Read the article and the suggested reading below, then take the 5 Minute Test. ● Read more about lupus on the NHS Choices website
tinyurl.com/lupus111 ● Find out more about discoid lupus erythematosus from the British Association of Dermatologists website
tinyurl.com/lupus112
● Read more about how lupus is diagnosed on the Arthritis Research UK website
tinyurl.com/lupus113
● Find out more about how lupus can aff ect the mouth on the Lupus UK website
tinyurl.com/lupus114
● For lifestyle advice you could give to patients with lupus, see the Arthritis Research UK website
tinyurl.com/lupus115
Evaluate Are you now confi dent in your knowledge of the symptoms and treatment of lupus? Could you give lifestyle advice to patients about this condition?
Tips for your CPD entry on managment of lupus
Take the 5 Minute TestClick here to check what you’ve learnt by taking our short MCQ test and get a CPD log sheet if you pass
(Internet connection required)

▶ ▶▶
Return to contents
Practical Approach■ Test yourself and your team with this scenario based on pharmacy practice
Bleeding and depression with an IUD1. Pamela Allen, a woman in her 30s asks to speak to pharmacist Verity Smith in private about two problems.
Verity leads her to the consultation room where the woman starts to explain.
“I had a Mirena coil fitted for contraceptive purposes after my daughter was born and it was brilliant,” she says. “The best thing of all was that it stopped my periods. When it ran out after five years, I had another one fitted straight away. That was four and a half years ago.
“In the past few months, I have started to get some spotting and in recent weeks. I seem to be bleeding all the time. My other problem is that I am feeling quite depressed for no reason. It’s just not like me. “Can being depressed give you periods? Or is the continual spotting making me depressed? The
two things seemed to happen about the same time.”
2. Pamela returns to the pharmacy about four weeks later, early on Saturday morning, and again asks to speak to the pharmacist in private. She is clearly in distress and Verity can see that she appears pale and is sweating.
She tells Verity that she saw her GP who believed that the Mirena had ‘run out’ even though the five years weren’t up. The GP said this wasn’t uncommon and could be causing Pamela’s problems. The GP took the coil out and Pamela opted to have it replaced at once. However, the procedure did not go smoothly. The doctor had great difficulty getting the replacement coil in, using Nitrolingual Pumpspray on Pamela’s cervix to facilitate the insertion. ▶

▶ ▶▶
Return to contents
Practical Approach
Bleeding and depression with an IUD (continued)
Pamela tells Verity that she was left feeling profoundly unwell and hadn’t really recovered. “I went into shock, which my GP said can happen if something comes into contact with your cervix like that.
“Anyway, that was four weeks ago and I’ve had problems ever since. Since then, I’ve been back to the practice and seen a different GP. “I told her I have been suffering from cystitis and soreness down below and she gave me antibiotics and some thrush cream, but it’s made no difference,” she says.
“Last night I started to get stomach ache, a horrid, disabling, cramping pain, which came and went, just like being in labour. I’m bleeding great clots and I feel sick and I’m sweaty and shivery.
“I took some paracetamol last night and it helped a bit, but I just don’t know what to do now.”
1. Can the intra-uterine device cause depression? What action should Verity take about the irregular bleeding?Verity looks at the BNF entry for Mirena and sees that depression (sometimes severe) is listed as a side effect and a history of depression is a caution for use of the device.
Irregular bleeding is common in the first six months of using an intra-uterine device, but is a sign for referral if it occurs after this time, as in Pamela’s case. Verity has no hesitation in referring Pamela to her GP. 2. What could be happening, and what should Verity do?Verity remembers that there can be some period-like pain early on after insertion, but she thinks this is more serious. She is concerned that Pamela may either have an ectopic pregnancy, that the coil is being expelled, or the insertion has perforated
Pamela’s womb. She rings the emergency doctor on Pamela’s behalf and Pamela’s partner drives her to the surgery.
Pamela returns to the pharmacy the following week, looking considerably better. The Mirena was indeed being expelled. Verity has discovered that this happens in about 6 per cent of Mirena users in the first year of use. Fortunately, there was no perforation (which occurs in about one in 1,000 women). The doctor removed the coil giving Pamela almost instant relief. She is going back to discuss possible future contraception in a week’s time.
If you identify a gap in your knowledge, consider making a CPD entry based on the article.

▶ ▶▶
Return to contents
C+D’s premium CPD package will give you 12 months’ access to a range of online learning and educational content, including:● popular courses such as Update● bite-sized learning such as Practical Approach and Ethical Dilemma● resource zone – apps for your mobile, key references, useful links, e-books
12 months access for £52+VAT (£62.40)
Find out more at chemistanddruggist.co.uk/update-plus
If you found this Update Toolkit useful, why not purchase one of our other CPD packages?
Update offers over 40 clinical and practice modules each year to choose from, any of which can be included in your ‘Plan and Record’ portfolio. It’s a flexible and cost-effective way to meet your continuing education requirements.
12 months’ access for £35+VAT (£42)
Find out more at chemistanddruggist.co.uk/update
C+D Training offers a range of courses for every role in pharmacy, from accredited courses for pharmacy staff, to pre-reg training and CPD packages for pharmacists and pharmacy technicians. All are competitively priced and delivered by C+D Training’s expert team, many of whom have previously worked in community pharmacies.
Find out more at chemistanddruggist.co.uk/training
▶ ▶ ▶